Asthma
1/12
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
13 Terms
Define asthma.
A recurrent and reversible (in the short term) obstruction to the airways in response to substances that aren’t necessarily noxious and normally do not affect non-asthmatic subject.
Give examples of stimuli that may cause an asthma attack.
Allergens, exercise, cold/dry air, respiratory infections, smoke, dust, environmental pollutants.
What is acute asthma (exacerbation)?
An acute airway obstruction caused by contraction of the airway smooth muscle. There is also mucus hypersecretion and thickening/plugging, alongside airway inflammation.
What are the symptoms of acute asthma?
Dyspnoea, wheezing, coughing.
Detail the symptoms that occur in the immediate phase (bronchospasm) of an asthma attack.
Bronchoconstriction, increased mucus production, vasodilation/increased vascular permeability, release of mediators of inflammation. This occurs in the first 1-4 hours.
Detail the symptoms that occur in the delayed phase (inflammatory reaction) of an asthma attack.
Recruitment of leukocytes and T cells by cytokines and chemokines produced by resident mast cells and epithelial cells. There is also a further release of mediators of inflammation. This occurs over 4 hours after the attack begins.
Detail the steps of airways remodelling in chronic asthma.
Increased mass of smooth muscle.
Accumulation of interstitial fluid (oedema).
Increased secretion of mucus.
Epithelial damage exposes sensory nerve endings, which contributes to increased sensitivity of the airways to bronchoconstrictor influences (bronchial hyperresponsiveness.
Airway narrowing by inflammation and bronchoconstriction increase airway resistance, decreasing FEV1 and PEFR.
How is asthma diagnosed?
Demonstration of an increase in airflow obstruction (spirometry and peak-flow test).
Pt reports difficulty with exhalation (wheezing in prolonged expiration).
Raised eosinophil count in blood test.
Do allergy test (skin pricking and blood test) to identify potential triggers.
How would COPD and asthma be differentiated between (diagnostically)?
Compared to a COPD patient, an asthmatic would have FEV1/FVC ratio return to normal with drug therapy. An asthmatic would also have a very large FEV1 response to bronchodilators or to 30mg prednisolone daily for 2 weeks. An asthmatics serial peak flow measurements would show 20% or greater day-to-day variability.
How would COPD and asthma be differentiated between (clinically)?
COPD patients are nearly all smokers/ex-smokers, whereas not all asthmatics have smoked.
Asthmatics often display symptoms under 35 y/o, for COPD patients this is rare.
Breathlessness is variable in asthma patients, but it is persistent and progressive in COPD patients.
Night time waking with breathlessness of wheeze is common in asthma patients, but uncommon with COPD.
There is a significant day-to-day variability of symptoms in asthma patients, but this is uncommon with COPD.
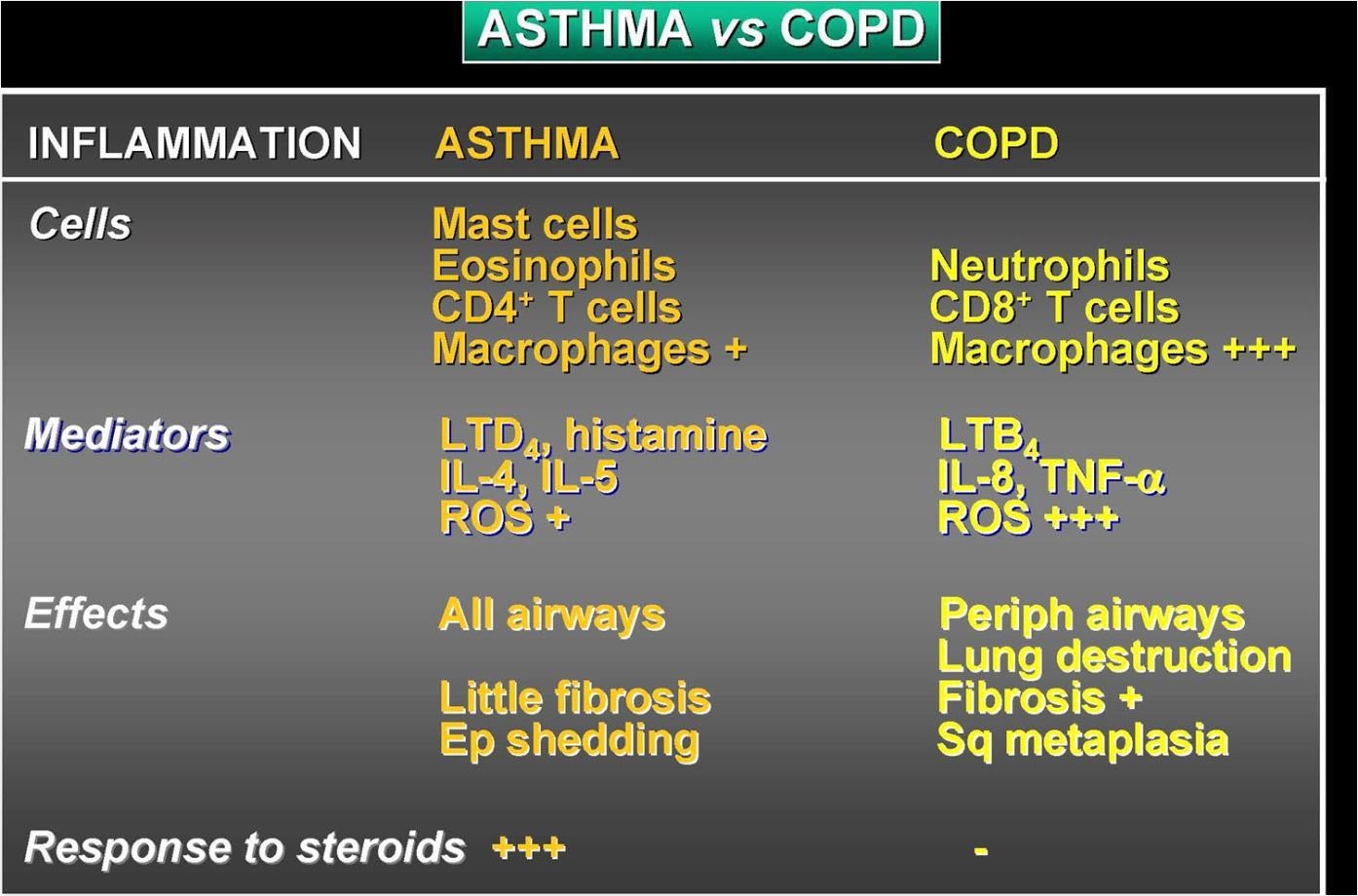
How would COPD and asthma be differentiated between (biomolecular pathogenesis)?
Which type of drug would be used to target the immediate bronchospasm phase of an asthma attack?
Bronchodilators (B2 agonists, muscarinic antagonists, xanthines).