Child and adolescent Midterm
1/168
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
169 Terms
adolescent period
12-18 years
Infancy period
0-2
Toddler period
1-3
middle childhood
6-12
Implies qualitative change, as in the change from being a child who can only think concretely (such as counting how many books on hw help are in the HW) to being an adult who can think abstractly.
Definition of Development
What occupational areas do people develop in?
· Vision (acuity, perceptual skills, visual motor skills)
· Gross Motor Coordination
· Cognitive/Language
· Social Emotional
- Play
· Fine Motor
· ADLS (Feeding, dressing, bathing, toileting, sleeping)
· IADLS (Meal prep, financial management, driving, personal care device management, home management, care of others)
What are the domains of human performance
Cognitive, affective, psychomotor
Cognitive Domain
Includes all aspects of thinking and language development, such as babbling in infancy, and learning the alphabet in preschool, as well as developing a greater attention span and acquiring a new language in school
What are the principles of development
Lifelong, sequential/predictable, multi-dimensional/directional, occurs in several domains at one, dynamic systems.
What are the directional principles of development
-cephalocaudal
-proximal to distal
-gross motor to fine motor
-undifferentiated to specific
What are the kinesiological areas of development?
-Antigravity movements
-mobility and stability
-asymmetry to symmetry
-rotation/ dissociation.
Occupational continuum
developing performance skills to perform occupations.
example: eating, feeding, mealtime preparation.
An infant is cared for, young child participates, an adolescent begins to have opinions and choices, and adult establishes a routine and expansion of occupation.
inferior pincer grasp to pincer grasp
What is the occupational contiunnum?
developing performance skills to occupations
ex. · Dependent or co-dependent on food, drink, and timing of meal Semi----> independent with food, drink, and timing of meal ---> Independent
Use the occupational continuum to define fine motor skills with grasp
Inferior pincer grasp to pincer grasp
Prenatal
before birth
What factors influence development during prenatal period?
Age of mom, stress/ cortisol/nutrition/ job demands, access to resources, exercise
What are the sensory foundations for baby while in utero
o Temperature
o Movement
o Sounds
o Positioning
o Vision/light
How does development impact labor and labor impact development
o The baby's development initiates birth, ex: Baby lung formation
o Labor has natural processes that are beneficial to bacterial/digestive development for the baby
o Different birth options and labor interventions can impact maternal and baby health outcomes.
o Stress can send mom into premature labor
o Vaginal birth provides bacteria to baby's gut and reflexes meant for them to assist in vaginal birth.
T/F First time moms may give birth past their due date
True
Gestational age is determined by?
Menstration time
Ultrasound and tape
Chronoligical age is considered?
Actual age since birth
today's date- DOB
Adjusted Age
Chronological age- # of weeks born prematurely.
pre-term birth age is calculated until the child is two years old
Eval: 7/28/23
DOB: 7/31/22
Premature: 9 weeks
CA= 1y/0m/27d
AA- 10m 20D
Perinatal complications
- Brachial plexus injury
- Hypoxic ischemic encephalopathy (cut off from O2, shortage of blood to the brain, damage)
- Cerebral palsy
- Brain bleed or cephalohematoma (bruise on head that can cause CP)
-General birth defects
-prematurity
What is a teratogen?
Any agent that may cause damage during the prenatal period
What period of development has the greatest structural abnormalities due to teratogens?
Embryonic
Teratogens examples
o -alcohol
o -viruses
o -stress
o -medications
o -chemicals
o BPA
o Caffeine greater than 200mg
Terratogens account for __ % of congential disorders
4-5%
Prematurity complications
o Hypoxia
o Low birth weight
o Respiratory stress disorder syndrome- undeveloped lungs
o Apnea
o Poor temp regulation- brain stem dysregulation
o Intraventricular hemorrhage
o Cardiac conditions
o Chronic lung disease
o Failure to thrive
o ROP- vision and perception issues
o Nutritional difficulties
Prematurity and death realtionships
o In the past it was a large cause of death/now it's a cause for disability, developmental delays, permanent medical conditions, slowed development, sensory processing difficulties, academic achievement challenges.
Critical period definiton
the times the body can be sensitive to damage cause by teratogens
Type and severity of teratiogen effect is directly related
Type of agent \n • Dose of agent \n • Time of exposure \n • Duration of exposure \n • Maternal and fetal susceptibility
The greates risk for defects occurs during?
The first trimester when important structures are developing, spine, head, arms, legs
What attempts to describe, explain, and predict behavior. Assists us with making sense of the world, provides a framework for observation and study, allows us to develop appropriate interventions
Theory
Developmental Theories/Multiple domains
Behaviorism
social learning theory
Eco Systems theory brofenbrenner
Behaviorism Theory of Learning
Who and what/ what type of theory
B.F. Skinner/developmetal/multidomain
-classical and operant conditioning,
-behavior is seen as a learned response to stimuli in the enviornment
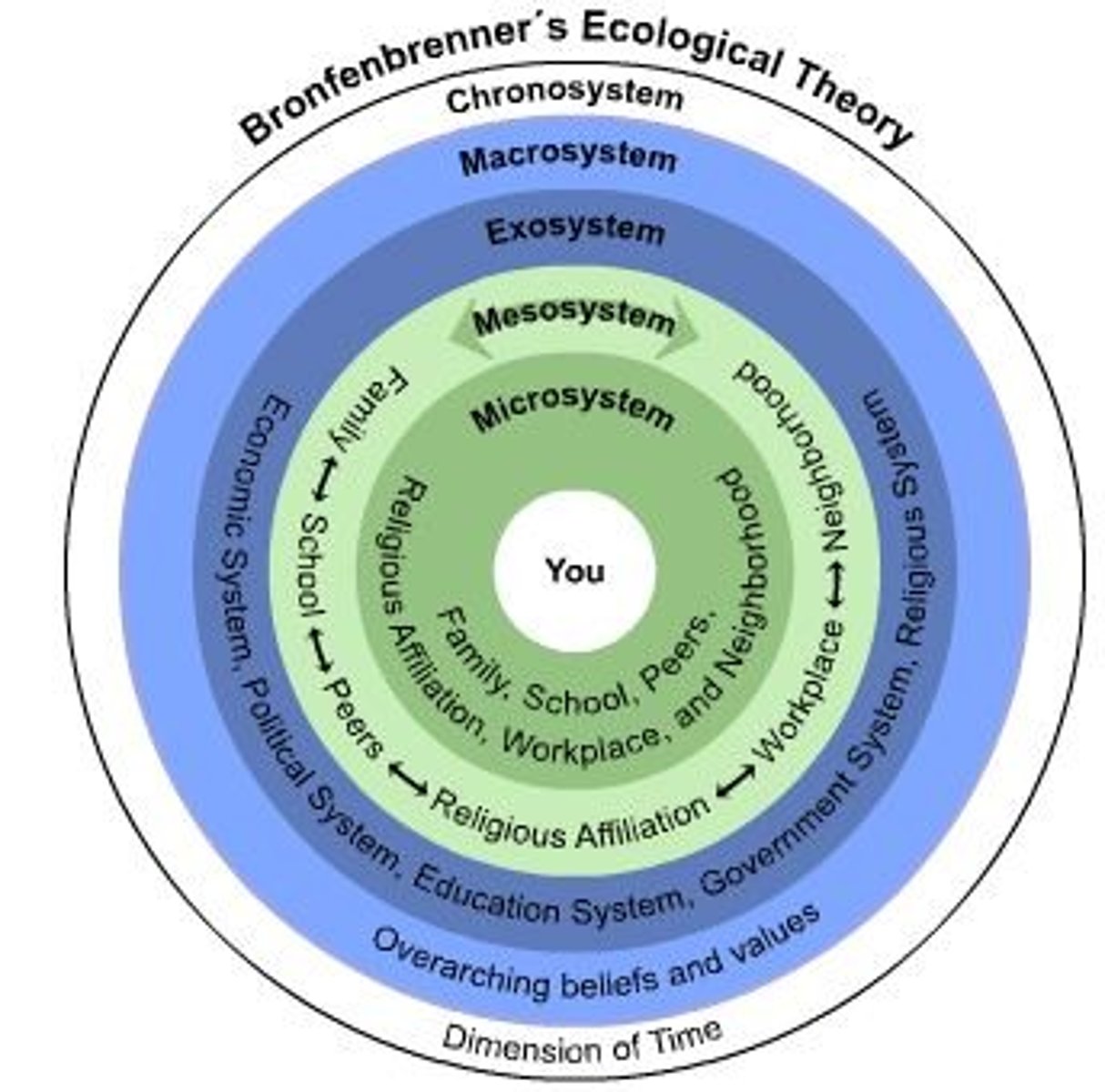
Ecological Systems Theory
Brofenbrenner developmental/mutlidomain
5 forces that impact our lives
-Microsystem- family, friends, that affect the child directly
-Mesosystem: forces connections of people together around the child, parents with teachers, teachers with peers
-Exosystem: Soical settings that do not directly involve the child, such as the father with his boss, teacher with principal
-Macrosystem: overarching culture, religion, and social norms that influence all
-Chronosystem: time which changes everything over the course of one's life (A childs prospect is not genetically predestined, but is the result of the larger enviornment a child is placed in.
this theory helped form the headstart program
Developmental theories: Psychomotor domain
Neuromaturational theory- gesell
dyanmical systems theory- esther
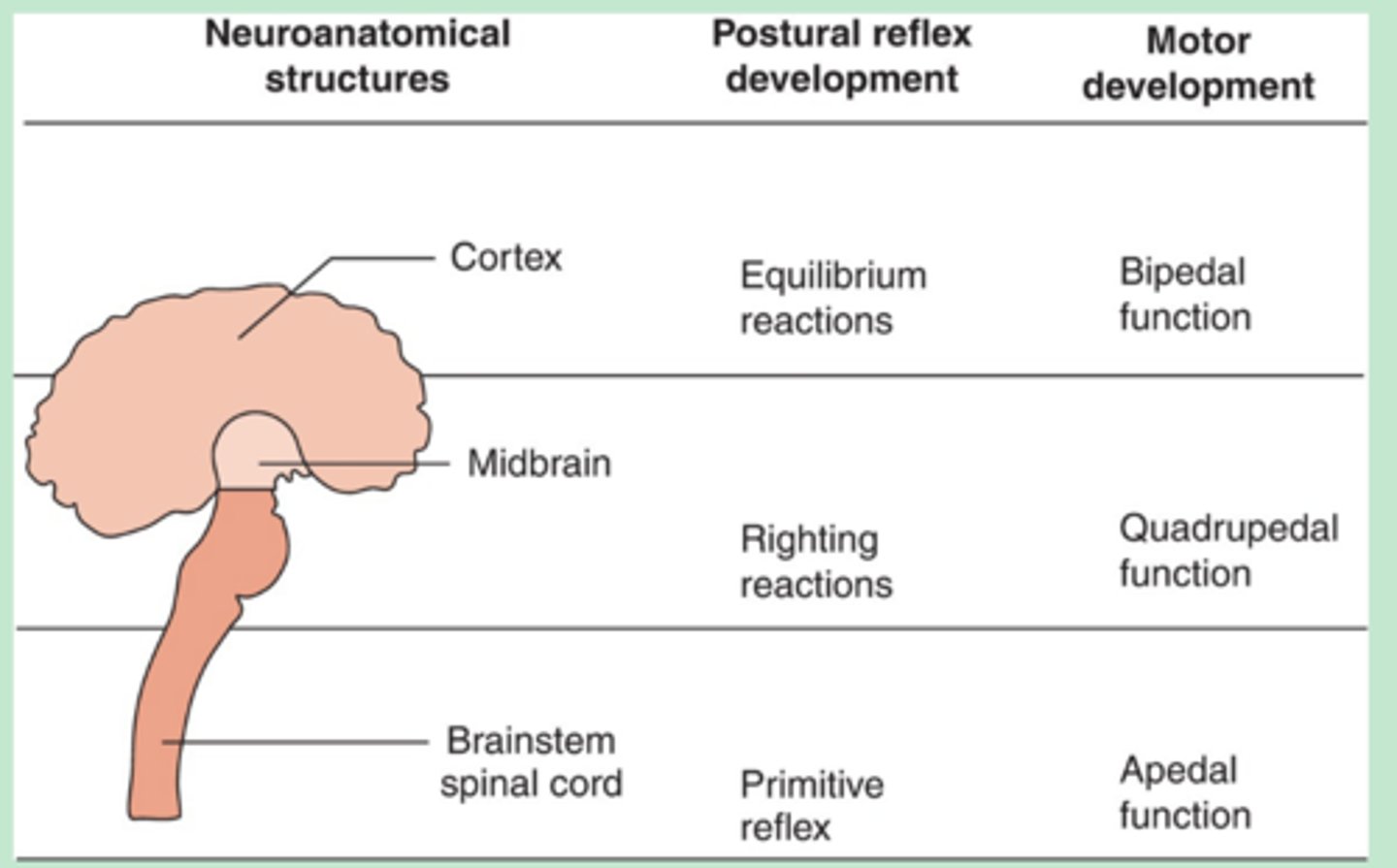
Neuromaturational theory
Gesell/developmenta; psychomotor
Motor skills develop based on CNS maturation
higher skills are contingent on development of lower level skills. (started from the bottom now we here)
reflex patters to coordinated motor control
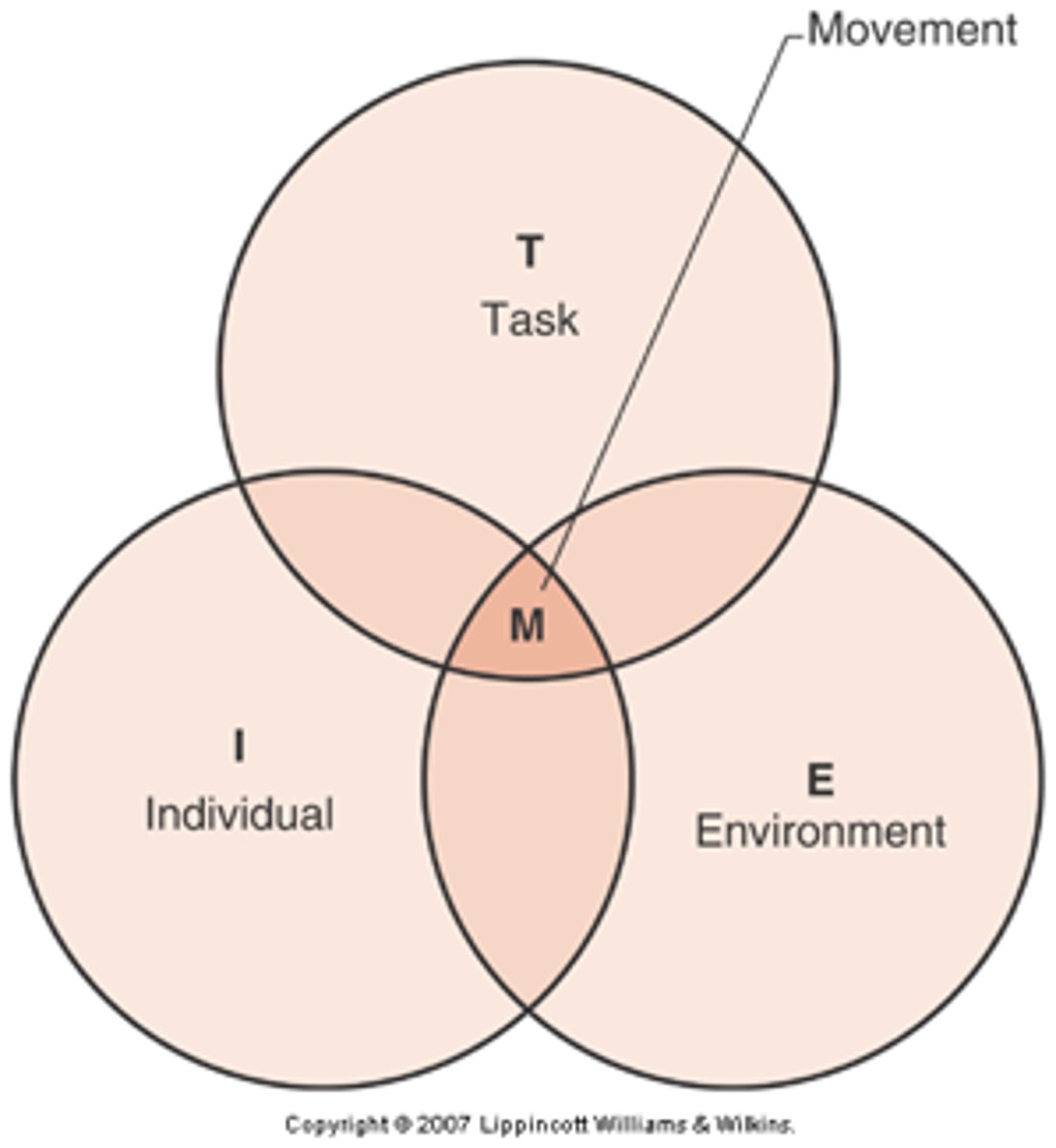
Dynamical Systems Theory
Esther thelen/psychomotor
· Development can only be understood as the multiple, mutual, and continuous interaction of all the levels of the developing system, from the molecular to the cultural.
Motor skills develop based on an interaction between
· multiple systems:
- Body
- Environment
- Task
Cognitive Developmental theory
Jean piaget/pshycomotor
- Cognitive development is a reorganization of mental processes rather as a result of nature and nurture
· Schemas are the basic building blocks of intelligent behavior
Sensorimotor: understands the world through senses- 0-2
preoperation: understands the world through langauage and mental images- 2-7
Concrete operational: Understands the world through logical thinking and catergories- 7-12
Formal Operational:
Understands world through hypothetical thinking and reasoning. Is able to predict consequences able to test own hypothesis -12 and up
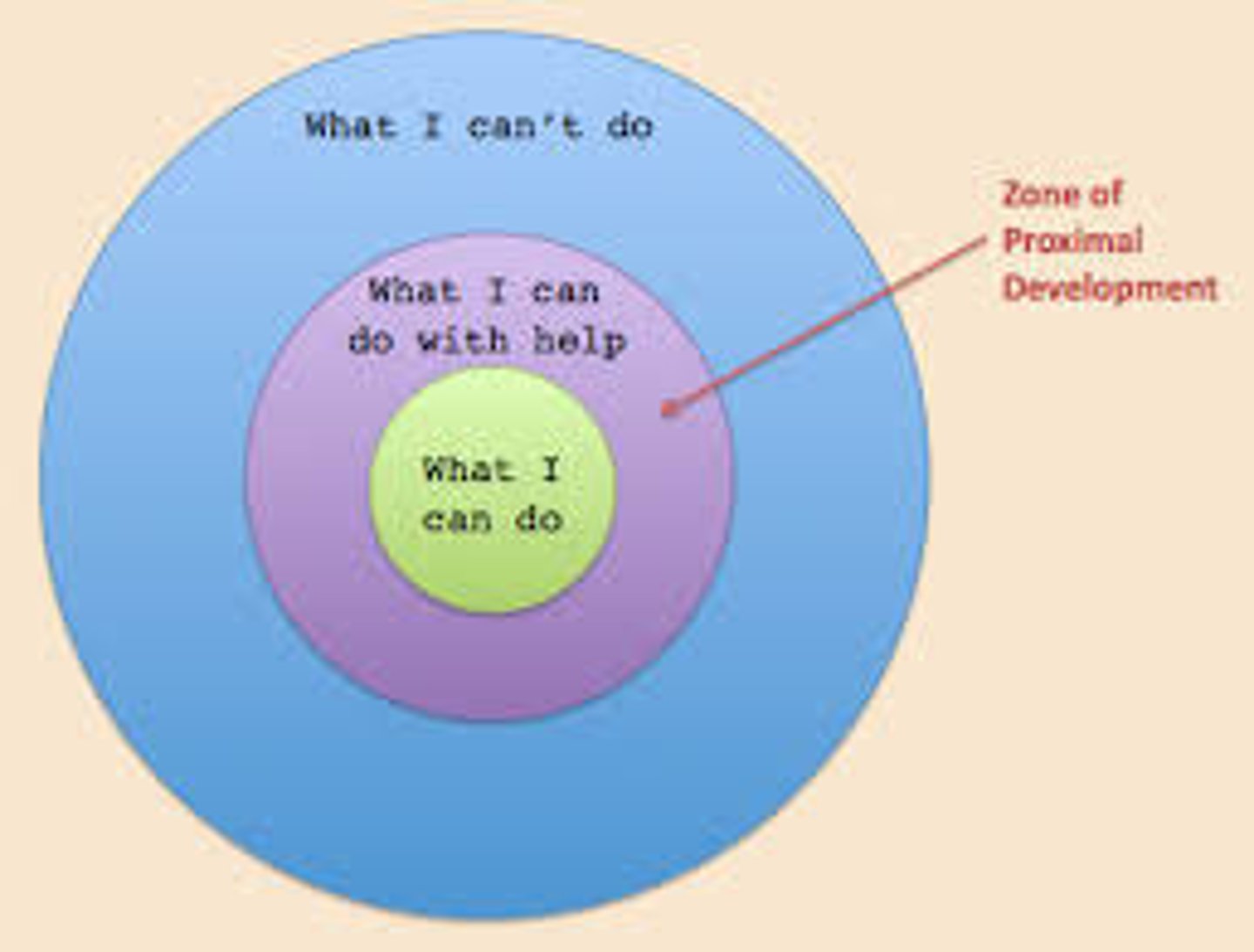
Sociocultural Theory
Vygotsky/psychomotor domain
According to Vygotsky's theory of cognitive development, children who are in the zone of proximal development for a particular task can almost perform the task independently, but not quite there yet. With a little help from other people, they'll be able to perform the task successfully.
· Zone of proximal development: According to Vygotsky's theory of cognitive development, children who are in the zone of proximal development for a particular task can almost perform the task independently, but not quite there yet. With a little help from other people, they'll be able to perform the task successfully.
· Scaffolding: Scaffolding refers to the temporary support given to a child by a More Knowledgeable Other that enables the child to perform a task until such time that the child can perform this task independently.
Developmental theories: affective domain
Hierarchy of needs- maslow
psychosocial theory
moral stages of development
temperament theory
theory of attatchment
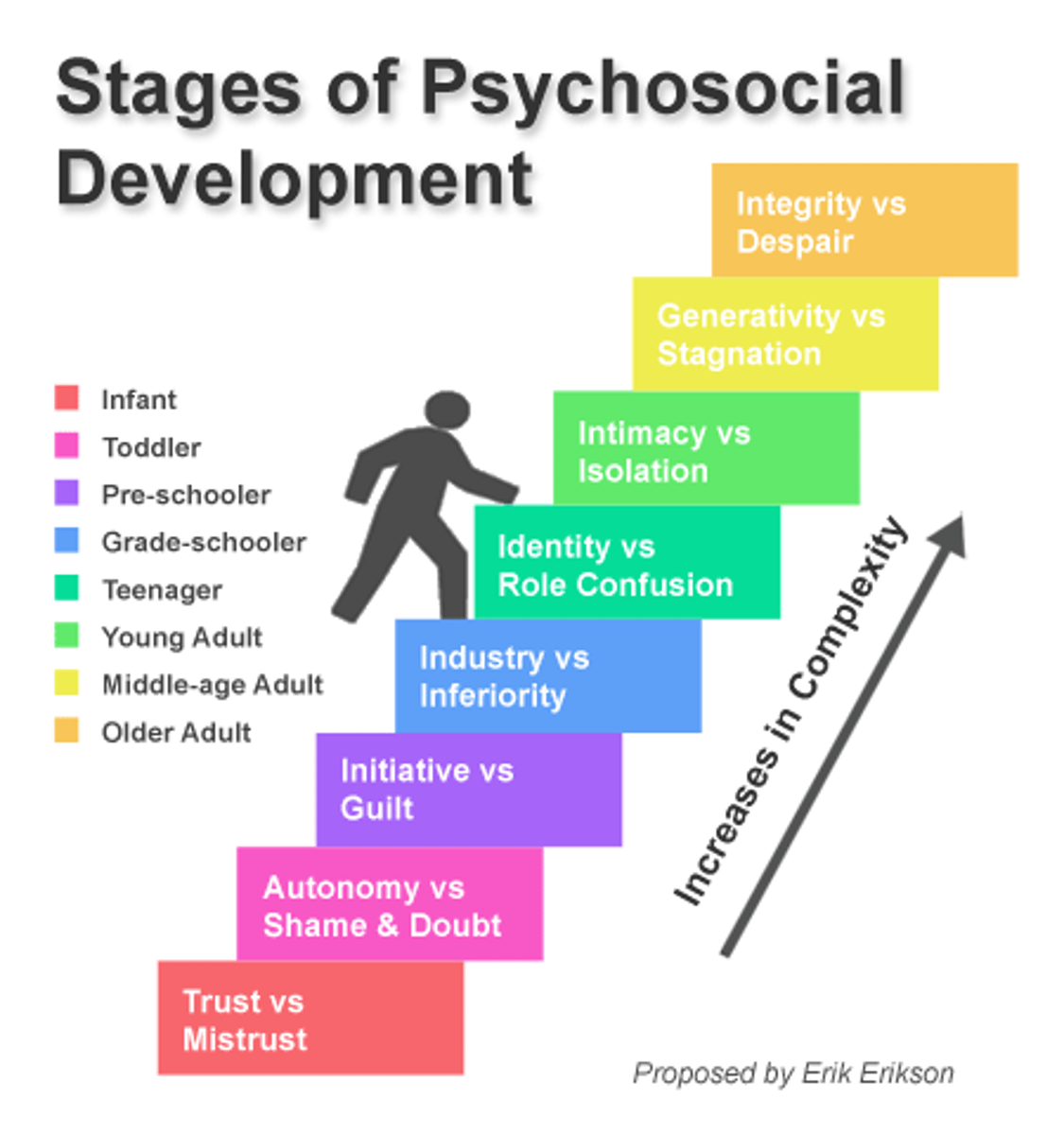
Psychosocial theory
Erikson/affective domain
· 8 psychosocial stages across the lifespan
· Each stage contains a stage-specific conflict
· Differences in personality can be explained by the way a conflict was or was not resolved
· Thinking becoming more complex
0-18 trust vs mistrust
18-3 autonomy vs shame & doubt
5-13 industry vs inferiority
13-21 indentiy vs role and confusion
21-39 intimacy vs isolation
40-65 generativity vs stagnation
65+ ego intergtiy and despair
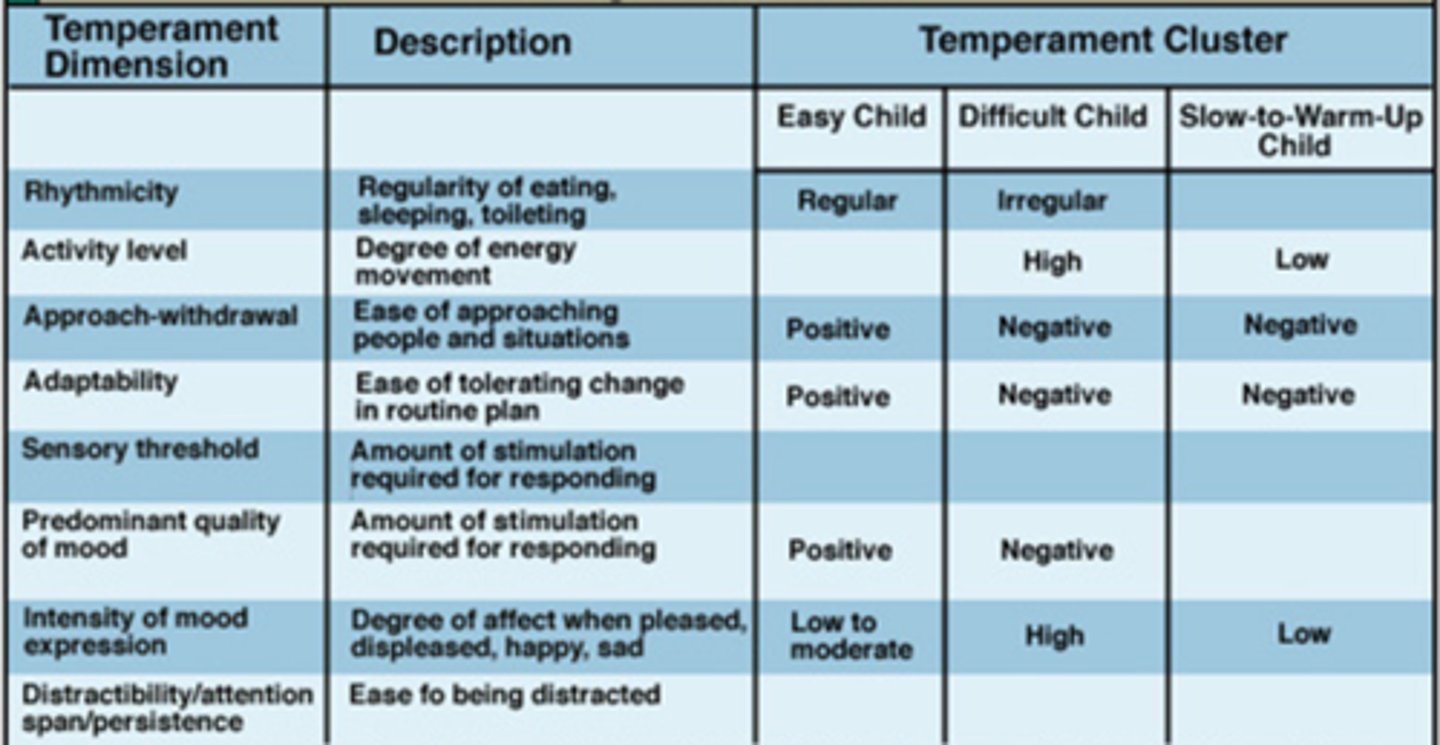
Temperament Theory (Thomas and Chess)
1. Activity level
2. Distractibility
3. Intensity of reaction
4. Biological rhythmicity
5. Threshold of responsiveness
6. Approach/withdrawal
7. Adaptability
8. Persistence/attention
9. Mood
Types of Temperament:
- Easy babies
- Difficult babies
- Slow to warm up babies
- Other not clearly defined
Developmental reflexes
· involuntary muscle response to a stimulus
· indicates neurological functioning
· age-specific
· serve a definite purpose
· controlled in the brain stem
· progresses from obligatory to inhibitory
-absence of a reflex- due to premature birth or other factors
-persistence of a reflex beyond age range
-response that it too weak or too strong (0-4)
Types of reflexes
primitive and postural
primitive reflexes
function to protect and nourish for survival
-develop in utero and are present at birth for full term babies
What are the primitive reflexes we have covered?
STNR, ATNR, Labryinthine, Neck Righting, Landau, Palmar, Suck, Moro, Startle, Plantar
Postural reflexes
Function to provide "practice" for future voluntary movements (motor development)
Emerge after birth, replacing primitive reflexes over time
What are the postural reflexes we have covered?
head/body righting, step, equilibrium reactions
Gross motor development 1-3 years
- Walking/navigating surface changes (12-18 months)
- Squatting (12-18) earlier when holding on
- Climbing
Steps
- Creeps (12-18 months)
- Non-reciprocal (24-30 months)
- Reciprocal (30-36 months)
Running (18-24 months)
Jumping
- Jumps off small obstacle (24-30 months)
- Jumps over objects with 2 feet (30-36 months)
- Hops on one foot (30-36 months)
Fine motor development (1-3)
· Hand movement and hands to mouth in utero
· Hands fisted at birth with reflexive grasp
· Hands open more by 3 months and functional grasps emerging around 4 months
· Ulnar to radial progression
· Pincer grasp appears around 10 months and becomes more refined, preparing for tool use
12-18 months: grasping and manipulating coloring utensils, holds with fist
24-30 months: separation of ulnar and radial sides of hand: snips with scissors
2-3: digial pronate grasp: holds pencil and utentsils
3-year-old: complementary hand use
Physical growth in the first year
· Length/height: one inch per month
· Weight: triple the birth weight
· Look at head circumference
· Growth slows after first year
· By 2: half adult height
· By 3: head size 90% of adult size
Neonate vision
· Legally blind
· High contrast
· Attracted to moving stimuli
· Preference for faces
· 8-10 range of focus
· Eyes and head move together
Reflexes important to feeding and eating
Reflexes are important to feeding and eating
- Rooting reflex
- Suck swallow breathe reflex
- Gag reflex
- Nutritive/nonnutritive sucking
- Transverse tongue reflex
- Phasic bit reflex
- Grasping reflex
Motor skills needed for feeding solid foods
Motor skills needed for feeding solid foods
- Good head and neck control/able to sit unassisted
- loss of tongue thrust reflex
- able to bring hands and toys to mouth
- developing a pincer grasp
- visual interest in food and mealtime routines
- Imitating motor patterns with mouth
Oral motor development reflexes
Suck reflex integrates at 6 months- purees
Rooting reflex integrates tongue thrust reduces- thicker purees
Phasic bite pattern, jaw stability increases (Reflexive sucking)- hard munchables
Tongue laterization (non reflexive sucking)- soft finger foods/ single solids
Graded bite- integration of two above - mixed textures
(all happens btw 6 to 12 months)
Physical development
includes all biological changes that occur from birth to adolescence. Includes increases in neuron connections within the brain during infancy and toddlerhood, growth of bones, as well as appearance of secondary sex characteristics during puberty.
Psychomotor Development
Development of human movement and factors that affect that development
Brain growth and development
- 100-200 billion neurons with few connections
- By Age 2 billion of established connections
Synaptic pruning
- Process of elimination of unused neurons
- Purpose is to increase efficacy of neutral connections
Congitive domain
Sensorimotor stage 0-2 Y
- Starts with reflexes
- Thinking is expressed through actions "pick me up"
- Sensorimotor actions occur by accident
- Explore the environment and begins to imitate other
- Interactions with objects are sought and how to use them (wanting to find the buttons to make the toys make noise)
- Mental representation begins
o Pretend play
Bandura: multidomain
- Cognitive (personal factors)
o Knowledge
o Expectations
o Attitudes
- Environmental
o Social norms
o Access in community
o Influences of others
- Behavioral
o Skills
o Practice
o Self-efficiency
congnitive development
- Infants communicate through crying
- 1-2 months: cooing, gurgling, and vocalizing
- 5-6 months: babbling begins
- 6 months: early object permanence
- 7-9 Months: clear vowel consonant: dada
- 11-12: first true word, object permanence, cause and effect
- 12-18: mastery of object perm, joint attention initiated, knows some body parts
- 18-24 m: deferred imitation, increased rate of word learning, putting words together
- 24-36 m: able to attend more than one thing/multitask
o Memorizes songs and rhymes
o Very interested in how things work
o Remembers past events
o Knows where you are going by landmarks
o Knows 1 color
o Demonstrates simple problem solving
Language development
Receptive: Understands:
- 2 step directions
- Simple concepts like hot and cold, go and stop
- Why questions
- New words quickly
Expressive
- Uses 2-3 words
- At least 50% of speech is understood by caregiver
- Has a word for most things
- Uses words like in, on, under
Development language Milestones
3 months: cooling/gurgling
6 months: babbling
12 months: first words
18 months: knows 5 to 40 words
2 years: 150-300 words, 2-3 word sentences
3 year: 900-1000 words, asks short questions
4 year: 2000 words, 5+ word sentences
5 year: identifies letters. Creates longer sentences
Autism screening
o Children are screened early for markers of autism
o Biomarker: head circumference > or = to 75%
o Social, communication, and behavioral differences
Early signs include:
o Very little eye contact
o Does not respond to caregiver's smile
o Does not point to objects/events to get attention
o Does not say a word until 16 months
o Does not start a convo or cannot continue it
o Rocks, spins, sways, walks on toes for long periods of time
o Over or under responsive to sensory stimuli
o Difficulty with transitions
Visual perceptive development
0-6: newborns look at faces and face like things
Discrimination based on high contrast
Stereopsis (depth perception) begins to develop around 4 months.
6 months - 1 year: visually explores objects in hands
Prefers geometric patterns
Differentiates faces
Begins to search for hidden objects
1.1.5 years: begins to discriminate and associate images with words
Can discriminate between similar objects
Starts to learn basic spatial concepts like in and out
1.5 -2 : turns picture right side up
Builds 6 cube tower
Completes a 3 piece puzzle
Begins to determine how far away something is/basic spatial reasoning
2-2.5: recognizes something from an outline only, stick figures like house
Stacks a few rings in size order after seeing it be done
Matches shapes after seeing it
Can identify when things are missing or out of place in images
2.5-3: completes simple inset puzzles of different items with 5 or more pieces
Begins to orient/turn items with greater independence
Begins to intimate from 3D designs
Eriksons affective domian
o Stage 1: Trust vs. Mistrust (0-18 months)
o Child learns "Can I trust the people around me?"
o Based on how fast needs are met when communicated (crying)
o Important event: feeding
o Feeling safe and secure
o Providing affection and comfort is essential
Stage 2: Autonomy vs. Shame & Doubt (18 months-3 years)
o Child learned increased independence with supportive encouragement
o Child wants to experiment and "do it myself"
o Increased independence with lead to increased self-esteem
o If child is not permitted to explore independence, they will develop feelings of embarrassment and doubt
Affective development
Early infancy (0-3m)
o Visual tracking not across midline
o Cries to communicate distress
o Temperament stable
o Calms to human voice and face
o Tells difference between mother and stranger
o Visual tracking at midline
o First smile
Middle infancy (4-6)
o Early play
o Shows delights
o Laughs
o Reciprocal social interaction
o Patty cake and peek a boo
o Clear preference for caregiver
o Begins to differentiate the emotions of others even if they don't understand yet
Late infancy (7-9 m)
o Shows anger and fear
o Caregiver attachment
o Separation protests; protests of caregiver leaves
o Initiates social interaction
o Emotional beings
o Reciprocal social interaction
o Patty cake and peek a boo
o Clear preference for caregiver
o Begins to differentiate the emotions of others even if they don't understand yet
Late infancy (7-9 m)
o Shows anger and fear
o Caregiver attachment
o Separation protests; protests of caregiver leaves
o Initiates social interaction
o Emotional beings
Transitional infancy (10-12 months)
o Shows clear attachment style
o Stanger/separation anxiety
o Greets others and shows regular affection
1-3 year olds
o Safe and secure in loving relationships
o Loves being the center of attention
o Recognize self in the mirror or photograph and makes faces
o Protests and says "No!"
o Likes to do things without help
o Has trouble sharing, may hit, push, and grab to keep toys
o Watches and copies others
o Shows wide range of emotions
o Begins to label emotions on self and others
o Shows affection and concern for others
Types of parenting
Authoritative: Clear expectations
o Definitive rules
o Supportive
o Authoritarian: high expectations
o Disciplined
o Unsupportive
Permissive:
o Low expectations
o Excessive responsiveness
o Uninvolved:
o No boundaries
o Little Support
types of parents:
Lawnmower parent: mow down all childrens challenges, discomforts and struggles
Helicopter parent: tend to hover and this can continue through college
Free-range parent: allow their kids to walk to school or a nearby playground alone
Attachment parent: use natural closeness rather than the clock to determine their babies needs
Tiger parent: known for putting excellence in academics and carefully chose extracirriculars above leisure time
Elephant parent: value encouragement over academic or athletic successes/
Sensory factors that impact infant and toddler regulation
o Proprioception
o Temperature
o Interoception: fatigue, hunger, thirst, feeling wet or soiled, feeling sick
o Overstimulation can be in any sensory system
o Lack of stimulation can lead to boredom and increase need for adult attention/interaction
Social participation and Play
unoccupied play 0-3m
solitary play 0-2y
onlooker play 2-21/2
parallel play 21/3-3y
Types of play
unoccupied, solitary, onlooker, parallel, associative, cooperative
Unoccupied play
0-3 m
child watches other in the envionrment at a distance
moves around to observe interesting things
Solitary play
0-2y
Plays by themself for long periods of time if interested in the activity
often does not notice others around them
not interested in engaging with peer
Onlooker play
2-2 ½ y
Child watches others play
stays close to other children to observe
child is content to watch without participating
Parallel play
2- ½ to 3
play in the presence of others
interested in what others are doing
may imitate peers and play with similar objects
Associative play
3-4 years
interested in peers and what they are doing
begins to play and share with others
develops friendships
Cooperative play
4-5 years
play becomes more rule-oriented
share materials duing play
take turns
have a common goal
"Non toy play"
Lining up toys, inspection/analyzing toys, feeling/touching toys repetition, engaging in various cause and effect actions
theres no thing as non toy play
Typical developmental occupations
o From co-dependent to semi-independent to independent
o From a co-occupation to an occupation
o From one occupation to another occupation to another
toddler occupations and co-occupations
o Eating and self-feeding
o Sleep and rest
o Beginning participation in dressing
o Beginning hygiene
o Beginning social participation
o Beginning education
o play
infancy co-occupations
eating
beginning self feeding
sleep
sensorimotor play
Attention as a factor of occupational development
attention span calculation
Average span per age can be calculated by doubling the age for the start range and then adding the age to the doubled number for the end range
- 4 years old= 8- 12 minutes
-8 years old = 16-24 minutes
Occupational continuum
Codependent for food, drink, and timing of meals—→ semi-independent with food, ——> drink, and timing of meals, independent
eating —→ feeding —→ meal prep
Personal Hygeine developmental considerations
o Washing hands is less complex than drying
o Nighttime bowel control, daytime bladder control and nighttime bladder control
*By 12 months*: may indicate when diaper needs changing
18-24 months: holds out hands to be washed, rubs hands together
- Opens mouth for teeth to be brushed
24 months: shows interest in potty training
- Flushes toilet independently
Toileting and personal hygeine
Readiness
- Has 2-hour periods with dry diapers
- Interest in toileting
- Most children in the U.S begin and master physiological function between 2 1/2 and 3 ½
- Accidents continue to happen
Wide variety of culturally-normed toilet training practices
- Ages, views of feces and urine, diaper availabilitly and access, caregiving practices
- Animation communication
Uses:
- Pull ups
- Toilet seats
- Stand-alone potties
Expectations:
- Caregivers: others around them
- Life demands
- Cost
Daycare centers:
- Requirements for admission
Society:
- Potty training experts
- Well-child visits
Dressing considerations
unbuttoning before buttoning/taking off less complex than putting on*
12 months: unsnaps front snap, pulls off clothes by “accident” for fun
18-24 months: takes off socks on request, puts on shoes halfway
24-30 months: puts on shoes
30 months: unbuttons large button
36 months: unsnaps back snap, buttons large button, zips and unzips, dones socks with assistance of heel
Teeth/face/hand hygeine considerations
First teeth appear 6-12 months
- Children need assistance to brush teeth through first grade and through elementary school
- 12-18m: wash face or some body parts with modeling
- 2-3 years: able to wash hands with modeling/prompting
Bathing considerations
dependent 0-3 years due to risk of drowning, but is great time for imitation and sensory exposure to water on head.
What is occupational justice? How does it apply to age ranges?
equity, laws, policies, inclusion, socioeconomic levelness
How are occupations learned?
Ethel vs other kids may have affordances vs barriers
AAP sleep considerations
- Supine for sleep "back to sleep"
- Firm, flat, non-inclined sleep surface
- Feeding of human milk
- Sleep in care-giver's room, close to the bed but a separate surface for at least the first 6 months
- No soft objects like toys pillows blankets
- Offer a pacifier at nap and bedtime
- Avoid overheating and head covering
6 parenting styles
lawnmower- mow down childrens challenges, discomforts or struggles
helicopter
free-range- lets kids walk to school or wherever
attatchement- uses closeness rather than determining needs
tiger- excellence in academics and extracircculars
elephant- academics over athletic success
SUID Prevention and plagiocephaly
Increased incidence of:
- Positional plagiocephaly: flat head due to repeated pressure on one part of the head
- Torticollis- Tightening of neck muscles on one side, affects balance, feeding, breathing, vision- improved through craniosacral therapy
- Delayed motor development
Contexts
environmental factors and personal factors, ecological systems theory
peformance patterns
habits
roles
routines
rituals
Performance skills
motor skills, process skills, social interaction skills
Client factors
Values, beliefs, and spirituality
Body functions
Body structures