Q1 - ICS - CAMBRA (Caries Management By Risk Assessment)
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
39 Terms
Factors of disease
xerostomia, diet, bacteria, genetics (pH)
erosion
smooth surface lesion, loss of surface contour
key teeth in erosion
occlusal surfaces of 1st molar and buccal surface of upper central incisor
attrition
flat noncupped incisal/occlusal surfaces, associated with cracked teeth and clenching habits
abrasion
pure, abrasion+toothpaste, abrasion+erosion
ETW
erosive tooth wear, acid from diet/stomach with physical forces, can affect single or multiple surfaces and plaque free teeth
caries
caries: bacteria produces acids/plaque, no physical component, affects single or multiple surfaces
ETW associated medical conditions
GERD (gastro-esophageal reflux disease), eating disorders, 65% population experiences intermittent reflus symptoms
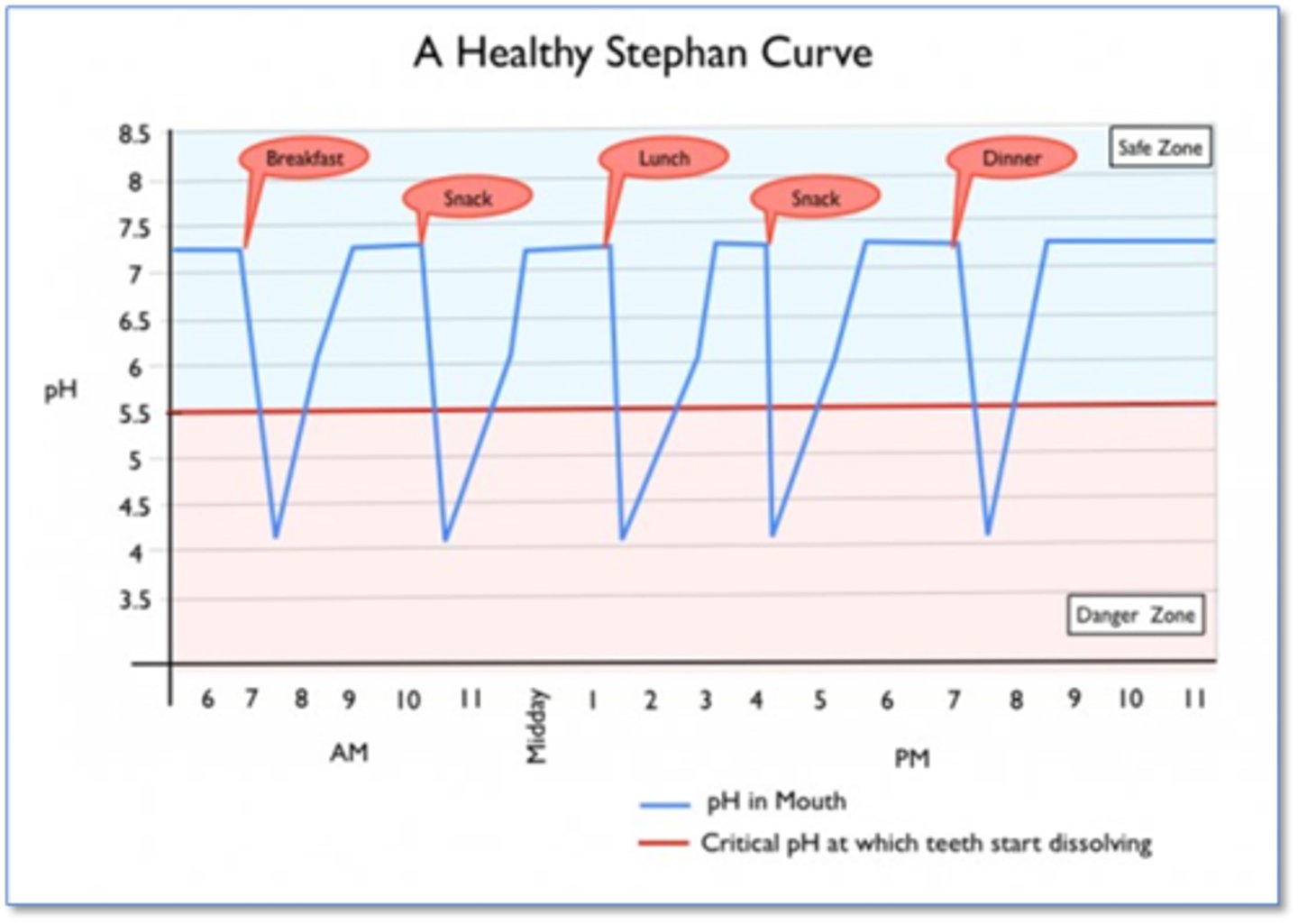
enamel dissolves at
pH 5.5
dentin dissolves at
pH 6.2
stephan curve
shows the pH levels in your mouth as time progresses
caries disease indicators (WREC)
white spots, restorations <3 years, enamel lesions, cavities/dentin
risk factors (BAD)
bad bacteria, xerostomia, destructive habits
protective factors (SAFER)
saliva and sealants, antibacterials, fluoride/Ca2+/PO3-4, effective habits, risk-based reassessment
carcinogenic bacteria + fermentable carbs (sucrose, glucose, fructose)
organic acids (penetrate enamel and dentin, dissolve tooth material)
common bacteria in plaque
s. mutans, lactobacillus
specifc plaque hypothesis
only a limited specied of bacteria in plaque can cause disease
cavitation importance
bad bacteria --> caries infection
but if bacteria doesn't get inside, then no need to restore
so, if subsurface is demineralized, it can be remineralized
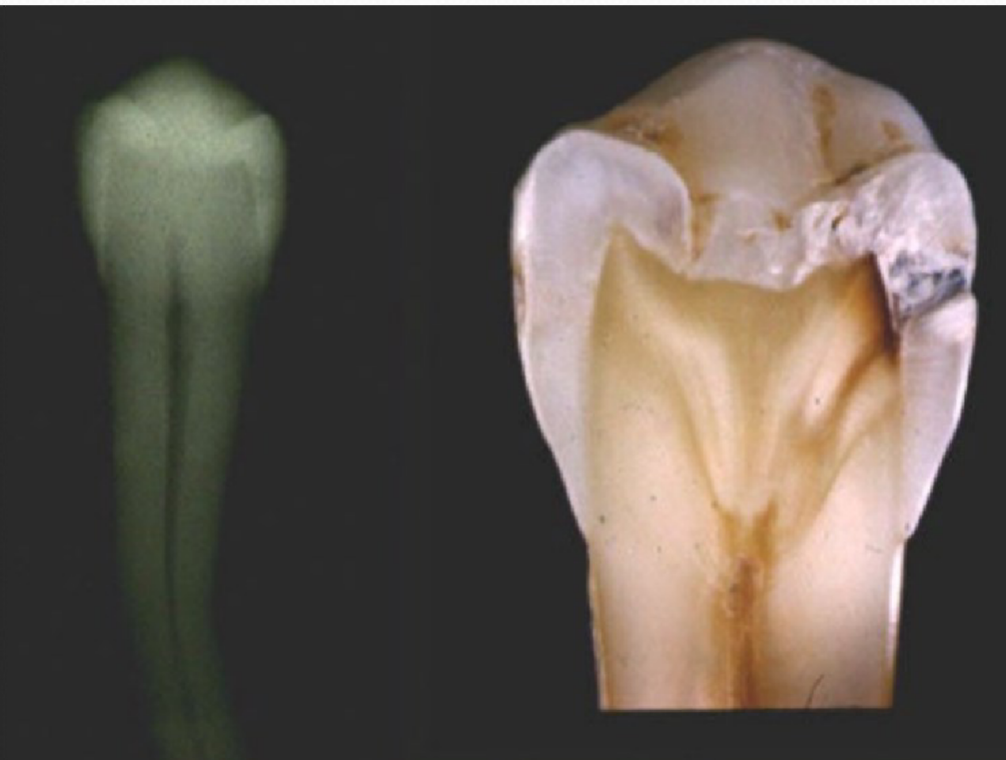
white spot lesion
earliest visible sign of subsurface demineralization
surface intact so prevents bacterial penetration
brown spot lesion
The previous white spot that is more porous and exogenous stain, can still be remineralized
pit and fissure lesions
occlusal surfaces of posterior teeth, lingual pits of maxillary incisors and buccal pits of mandibular molars
cavitated lesion
salivary glands
cleanse, buffer, lube, antimicrobial, remineralize, heal
unstimulated saliva
0.3-0.4 mL/min
stimulated saliva
>1 mL/min
medications that cause xerostomia
amphetamines, narcs, anti-inflammatories, antidepressants/anxiety/histamines/microbials/psychotics, asthma drugs, ACE inhibitors, Ca2+ channel blockers, gastric acid drugs, smoking cessation drugs
treatments and conditions that lead to poor salivary flow
sjogrens syndrome, head and neck radiation/surgical treatment
dentinogenesis imperfecta
poorly formed dentin
amelogenesis imperfecta
poorly formed enamel
mutated genes
malformed teeth susceptible to decay
taste gene mutation
prefer sweets —> prone to caries
saliva enzyme mutations
decrease production of protective enzymes —> decay
ATP test - CariScreen
measure bacterial load (correlates to risk level) ATP bioluminescence
low caries risk
no incipient/cavitated primary/secondary lesions in past 3 years and NO risk factors
moderate caries risk <6
no lesions in last 3 years but at least 1 risk factor
moderate caries risk >6
at least 1 lesion in the past 3 years or 1 risk factor
high caries risk <6
any lesion in past 3 years, multiple risk factors, low socioeconomic status, suboptimal fluoride exposure, xerostomia
high caries risk >6
3 or more lesion is past 3 years, multiple risk factors, suboptimal fluoride exposure, xerostomia
extreme risk
xerostomia