Failure of the Heart
1/73
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
74 Terms
Other names for heart failure
• Heart Failure
• Cardiac Failure
• Congestive Heart Failure (CHF)
• Cardiomyopathy
• LV dysfunction
Defn of heart failure
Inability of the heart:
– to pump blood at a sufficient cardiac output
– to maintain adequate perfusion of other organs
Cardiomyopathy defn
Any pathological process affecting the myocardium which results in a disturbance in myocardial function
- Refers to the actual underlying disease process
(Patient has the clincial syndrome of heart failure – “due to a dilated cardiomyopathy”)
Name 1 systolic dysfunction & 2 diastolic dysfunctions associated with HF
Systolic dysfunction: Reduced Contractility
Diastolic dysfunction: Impaired Relaxation & Increased Stiffness (stiffness e.g. increased thickness)
What effect would cause a rise/fall in the frank starling graph representing preload
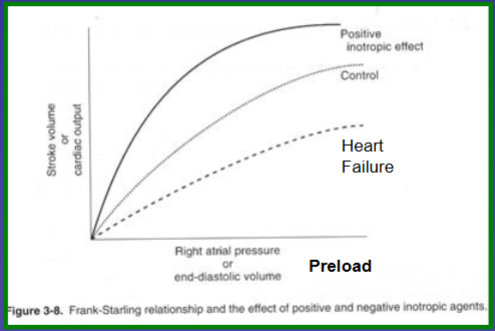
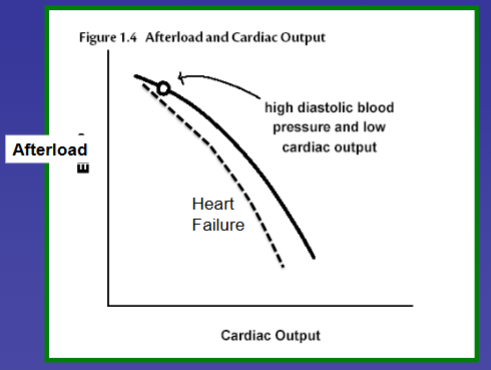
What effect would cause a rise/fall in the frank starling graph representing afterload
What is Ejection Fraction
Measure of heart function
• % emptying of the left ventricle
• Shows “systolic function”
Ejection Fraction normal %
Normal 55-60%
How is Ejection Fraction normally measured
Typically measured by echo (or MRI)
What are the 2 main types of heart failure
Heart Failure with reduced Ejection Fraction (HFrEF)
Heart Failure with preserved Ejection Fraction (HFpEF)
1 main problem & 2 resulting characteristics of HFrEF
Reduced LV ejection fraction (EF)
Reduced Stroke volume at rest and with exercise (Reduced “forward pressure”)
Increased intracardiac pressure (Increased “back pressure”)
1 main problem & 2 resulting characteristics of HFpEF
Diastolic dysfunction (Increased LV stiffness/Impaired relaxation)
• Reduced Stroke volume at rest and with exercise (Reduced “forward pressure”)
• Increased intracardiac pressure (Increased “back pressure”)
What are 2 resulting effects of Reduced stroke volume and cardiac output in HF
• Reduced “forward-pressure”
• Reduced organ perfusion
What are 2 resulting effects of elevated filling pressures and cardiac output in HF
• Increased “back-pressure”
• Fluid retention – affects oncotic pressure
What causes the Neuro-hormonal Response to HF
Stimulation of baroreceptors
Renal hypoperfusion (forward pressure)
Increased adrenaline & noradrenaline
Describe 2 counter-productive compensatory neuro-hormonal responses to HF
Activation of the Sympathetic System
Increases Heart Rate → Increases myocardial work
Increases contractility → Increases myocardial work
Vasoconstriction (improving BP) → but also increases afterload & myocardial work
RAAS activation
Increased Angiotensin II
Vasoconstriction (improves BP) → but increases afterload & myocardial work
Hyperaldosteronism
Sodium retention – enhances intravascular volume – maintains CO → but leads to volume overload
Explain the significance of the Law of Laplace in HF
Explains the progressive course of HF
LV dilates → Increased wall stress → LV becomes more spherical → Progressive dilatation
Heart gets progressively bigger!
2 functional issues in HF
Reduced cardiac output
Increased filling pressures
Symptoms of reduced CO in HF
1. Cool peripheries
2. Hypotension
3. Decreased renal perfusion
– Renal dysfunction
– Activation of RAAS
– Activation of sympathetic system
4. Fatigue
Symptoms of increased filling pressures in HF
1. Pulmonary venous congestion
– Dyspnoea
– Orthopnoea
– PND
– Pleural effusions
2. Right heart dysfunction
– Ankle oedema
– Elevated JVP
– Ascities
What are 2 possible causes of acute HF
Acute myocardial infarction
Cardiogenic shock
What would cause chronic HF
Chronic LV systolic or diastolic dysfunction
Causes of Hypertrophic Cardiomyopathy
• Hypertensive
• Hypertrophic (obstructive) cardiomyopathy (Rare Genetic Sarcomeric protein mutation - Subgroup at risk of sudden cardiac death)
• Metabolic storage diseases (e.g. Anderson Fabry)
• Obesity
What type of HF could Hypertrophic Cardiomyopathy cause
HFpEF
5 causes of HFrEF
1. Ischaemic cardiomyopathy (Ischaemic heart disease - IHD)
2. Non-ischaemic Dilated Cardiomyopathy
3. Hypertension – Usually HFpEF but can get “burnt out” hypertensive HF with reduced EF
4. Valvular Heart disease – AS; AI; MR
5. Tachycardia related – rate related
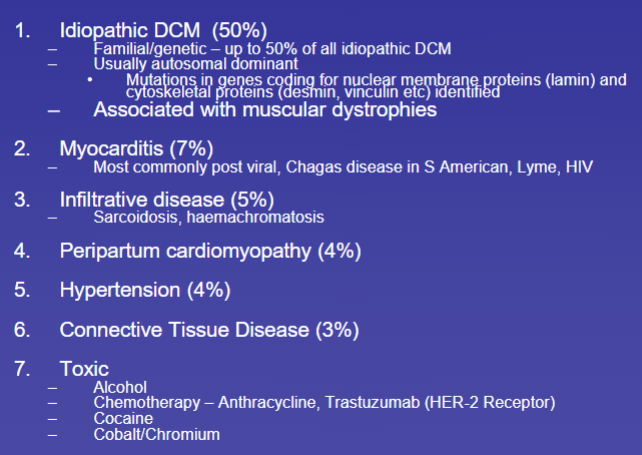
7 causes of Non-Ischaemic Dilated Cardiomyopathy
What % of HFrEF is caused by ischaemic cardiomyopathy
50-70%
Causes of HFpEF
1. Idiopathic/Familial
2. Infiltrative Processes
• Sarcoidosis
• Amyloidosis
3. Storage Diseases
• Haemochromatosis
• Genetic abnormalities
4. Endomyocardial Fibrosis
How does acute HF present
Acute pulmonary oedema
Dyspnoea
Pulmonary congestion
Implies extensive damage
New major acute insult - AMI
Often pale, listless, diaphoretic
How does chronic HF present
1. Dyspnoea on exertion
• NYHA class I to IV
2. Orthopnoea
• Increased venous return when recumbent
• Measure by number of pillows
3. PND
• Specific for heart failure
• Similar mechanism to orthopnoea
4. Pedal/lower limb oedema, anasarca,
• Dependent
• Worse in evening – resolves overnight
• Can get ascites, pleural effusions etc
• Cardiac oedema is pitting
5. Fatigue
Often pale, listless, diaphoretic
What is staging of HF based on
Dyspnoea on Exertion - New York Heart Association (NYHA) Classification
What are the 4 stages of HF
Class I: No symptoms
Class II: Dyspnoea on strenuous exertion
Class III: Dyspnoea on mild exertion
Class IV: Dyspnoea at rest
What would you find on a physical exam on a HF patient
• Often pale, listless, diaphoretic
• Tachycardic (Pulsus alternans – severe HF)
• BP can be normal, high or low (with advanced HF)
• Elevated JVP
• Oedema/ascites
What feature would you find when auscultating a HF patient’s lungs
Bilateral basal rales on chest auscultation
What feature would you find when auscultating a HF patient’s heart
Third heart sound
Gallop rhythm
MR murmur
What would be a sign of severe HF when taking someone’s pulse
Pulsus alternans (alternating strong and weak peripheral pulse)
What 4 features would you find on a CXR of a HF patient
– Cardiomegaly (CTR > 0.5)
– Pulmonary venous hypertension – upper lobe redistribution – enlarged pulmonary veins
– Interstitial oedema (increased interstitial lung markings) and Pulmonary oedema – pulmonary infiltrates
– Pleural effusions
What do we use an electrocardiogram (ECG) to find out
The cause of the HF:
Ischaemia
LBBB (Left bundle branch block)
What do we use an Echocardiography to find out
– Determine if systolic and/or diastolic dysfunction
– Quantify severity - estimated using LV ejection fraction
– Global vs regional dysfunction?
– Evaluate for any valvular pathology or LVH
– Quantify severity of diastolic dysfunction
What is considered: (EF%)
• Normal EF
• Mild LV dysfunction
• Moderate LV dysfunction
• Moderate/severe LV dysfunction
• Severe LV dysfunction
• Normal EF = > 50%
• Mild LV dysfunction = 40-45%
• Moderate LV dysfunction = 30-35%
• Moderate/severe LV dysfunction = 20-25%
• Severe LV dysfunction < 20%
What is Brain Naturetic Peptide - BNP
Released by stretch receptors in the LV in response to an increase in LV pressure/decrease in systolic function
Why do we measure brain naturetic peptide (BNP)? What does it tell us?
Useful to help differentiate cardiac dyspnoea (HF) from pulmonary dyspnoea
Good negative predictive value - Normal value makes HF very unlikely
What could be some other differential diagnoses of breathlessness?
• Pulmonary disease (looks very like HFpEF)
• Obesity
• Anaemia
• Other systemic disease
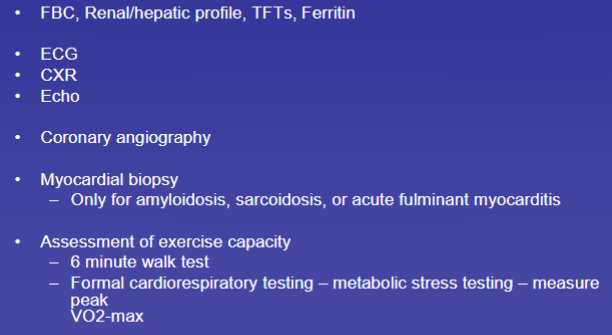
What are some test we run for HF evaluation
Prognosis of HF in class I-IV
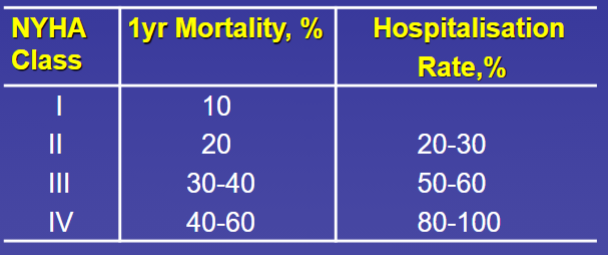
Prognosis of HF depends on stage & what other factors
Increasing age
Men worse prognosis
Ischaemic worse than non-ischaemic
Worse with lower ejection fraction
5 mechanisms of HF treatment
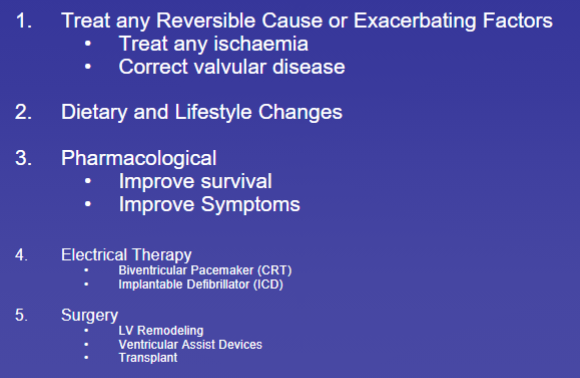
What are 7 lifestyle & dietary changes HF patients must make
1. Avoid harmful drugs (NSAIDs/Corticosteroids/Alcohol)
2. Dietary sodium restriction (< 2g/d)
3. Fluid restriction - < 2L/d
4. Weight reduction
5. Patient Education
6. Daily weights
7. Exercise programme
Name 5 drugs that improve survival in HFrEF
• ACE Inhibitors
• β-Blockers
• Aldosterone Antagonists
• (Angiotensin Receptor Blockers)
• Sacubitril/Valsartan
What are some drugs that don’t improve survival, but improve symptoms
Diuretics
Mineralocorticoid receptor antagonists
SGLT-2 inhibitors
What are 2 main types of diuretics used
Loop diuretics
Thiazide diuretics
Name 2 loop diuretics
Frusemide or bumetanide
AEs of loop diuretics
Hypokalaemia & hypomagnesaemia (due to electrolyte loss)
Muscle cramps
Exacerbate renal dysfunction
What 2 main things do ACEis have an effect on
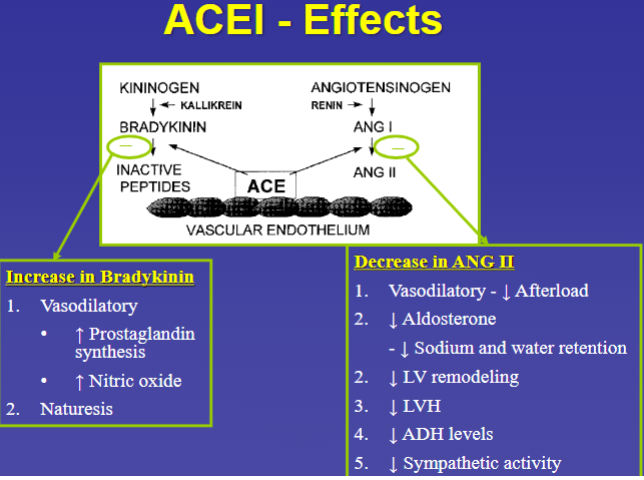
Effects of ACEis in HF
• Reduce Hospitalisations
• Improve Survival
• Reduce symptoms
• Improve exercise tolerance
• Improve EF
• Reduce LV dimensions (Remodeling)
• Improve haemodynamics
Side effects of ACEis
• Hypotension
• Cough (dry cough) – 10% - especially women
• Renal dysfunction
• Angio-oedema
• Taste disturbances
Effects of Beta Blockers
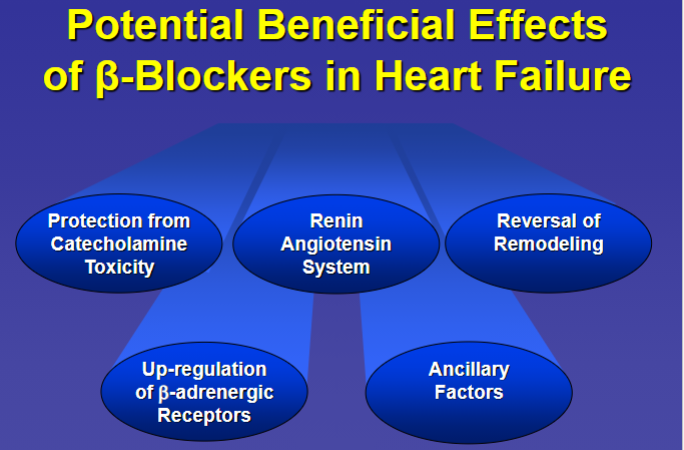
β-Blockers have a Biphasic Effect. What are the 2 acute effects
Decrease BP and CI
β-Blockers have a Biphasic Effect. What are the 5 chronic effects
• Improve EF
• Decrease HR – decrease arrhythmia risk
• Improve Sx - Takes up to 3 months
• Reduce hospitalisations
• Improve mortality (both progressive HF and SCD)
Name 2 Mineralocorticoid Receptor Antagonists (MRAs)
Spironolactone or Eplerenone
Mineralocorticoid Receptor Antagonists (MRAs) MoA & effects
Block sodium and water retention effects of Aldosterone (Weak diuretic) → Counteract the secondary hyperaldosteronism that occurs in heart failure
3 AEs of Mineralocorticoid Receptor Antagonists (MRAs)
Hyperkalaemia (esp. in renal impairment)
Gynaecomastia
(Breast pain)
Name 2 general treatments given to acute HF patients
Diuretic (IV)
Inotropes
Name 3 Inotropes used for acute HF patients
B1 agonists
Dobutamine
Dopamine
Are Inotropes used temporarily/long term
Temporary only
Effect of inotropes
Increase contractility
Name 5 treatments for chronic HF
• Diuretics
• ACE Inhibitors
• Betablockers
• Aldosterone antagonist
• Sacubitril/Valsartan (Entresto)
What are 2 options of Electrical Therapy for HF
• Implantable Cardioverter Defibrillator (ICD)
• Cardiac Resynchronisation Therapy (CRT)
Which of the 2 options of Electrical Therapy for HF is used for Biventricular pacing
Cardiac Resynchronisation Therapy (CRT)
Who would be given an ICD
Those with life-threatening arrhythmias
At risk of sudden death
High risk HF - (symptomatic & Poor LV function (EF < 30%))
Who would be given a Biventricular Pacemaker
People with a Left Bundle Branch Block
How does a LBBB cause Dyssyncrony
Left Bundle Branch Block → Delayed contraction of lateral wall → Septal wall is relaxing when lateral wall is contracting
(ineffective contraction)
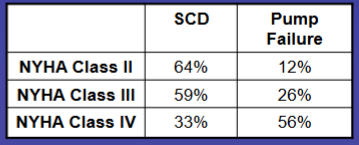
What is the main cause of death in HF NYHA Class II-IV
SCD = sudden death
Pump failure = CHF (Chronic heart failure)
3 types of Therapy for Advanced heart Failure
• Cardiac Transplantation
• Left ventricular assist devices (LVAD) (External pump)
• Surgery to correct for any evidence of ischaemia