pt 1 anatomy, embryology, physiology, and typical development
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
75 Terms
the most complex neuromuscular unit in the body
upper aerodigestive tract
serves as the shared pathway for the digestive, respiratory, and phonatory systems
upper aerodigestive tract
Normal Swallowing requires integration of the important functions of
breathing, eating, and speaking.
Understanding ______, ______, and ______ changes from infancy to adolescence is critical and informs diagnosis and treatment of pediatric feeding and swallowing disorders.
anatomy, physiology, and developmental
what structure is crucial for respiration, especially in neonates & infants (preferential breathing)
nose (nasal breathing)
nose functions:
cleans, warms, humidifies inspired air
the nose opens into nasopharynx via bilateral posterior nasal choanae—important for
speech resonance and airway
Lateral walls of the nose have nasal turbinates covered with _________
sensitive mucosa
nose is separated by
midline septum
Septal deviation at birth can cause ________ → feeding difficulties.
nasal obstruction
seals nasal cavity from oral cavity during swallowing.
soft palate elevation
Other causes of nose obstruction:
choanal atresia, encephalocele, rhinitis, etc.
what structure is involved in food ingestion, vocalization, and oral respiration.
mouth
Cheeks with _____ important for sucking in infants.
fat pads
______ affect sucking & swallowing
Anatomic defects
Food/liquid can lodge in __________ affecting bolus prep
anterior & lateral sulci
In infants, what structures blend?
nasopharynx and hypopharynx blend; no distinct oropharynx
Swallowing initiation is _____; completion is _____
voluntary; involuntary
Drains sinuses & middle ear
Resonator for speech
Sealed off during swallowing via soft palate elevation
nasopharynx
Includes:
Palatine tonsils (between tonsillar pillars)
Valleculae (wedge-shaped spaces at tongue base & epiglottis)
Lingual tonsil (at tongue base; enlargement may impair airway/swallowing, linked to GERD/EERD)
oropharynx
Part of the common airway-foodway intersection
hypopharynx
Key role in directing food to esophagus, away from airway
hypopharynx
Tonic contraction at rest—prevents reflux & air entry
Cricopharyngeus Muscle (UES) Upper Esophageal Sphincter
Cricopharyngeus Muscle (UES) Upper Esophageal Sphincter Relaxes only during:
Swallowing
Belching
Regurgitation
Primary Functions (in order of priority) of the larynx
Airway Protection
Respiration
Phonation
protective mechanisms of the larynx
Epiglottis: Directs food laterally into pyriform sinuses
Arytenoid cartilages + Aryepiglottic folds: Medial movement blocks laryngeal inlet
False vocal folds (ventricular): Expiratory control
True vocal folds: Prevent inspired foreign materia
Propels food from hypopharynx to stomach
esophagus
Upper Esophageal Sphincter (UES) → ______ muscle
Cricopharyngeus muscle
what structure of the esophagus: tonic contraction at rest; prevents air ingestion
UES
Lower Esophageal Sphincter (LES) →
Junction with stomach
what structure of the esophagus: Transient relaxation; prevents gastric reflux
LES
Help maintain an empty esophagus between swallows
LES
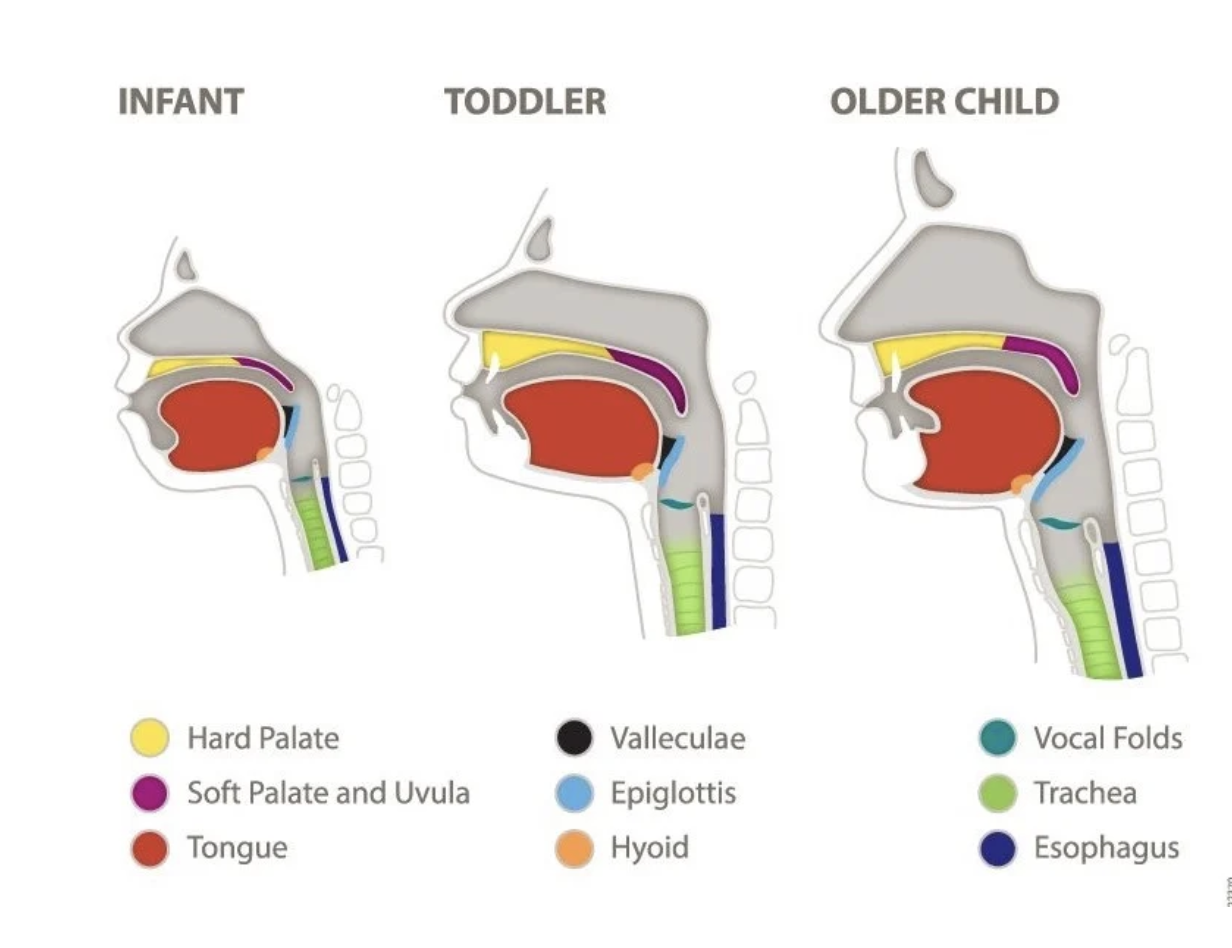
comparison of infant toddler and older adult
formation of 3 germ layers by week __
3
ectoderm
mesoderm
endoderm
CNS & cardiovascular system begin forming week ____
Week 3-4
All major organ systems develop at week ____
week 4-8
Embryo takes on human appearance by Week __
8
Rapid growth; face forms; limb development
week 9-12
Skeleton ossifies; movement felt by mother
weeks 13-20
Weight gain; lungs begin surfactant production weeks ____
weeks 21-25
Lungs can exchange air; eye opening; temperature control begins
weeks 26-29
Weeks ___: Pupillary reflex present; white fat → feeding readiness
weeks 30-34
Growth finalizes; ready for birth at ~38 weeks post-fertilization
weeks 35-40
Pharyngeal swallow appears by ____ weeks gestation
10–14
Swallowing observed in fetuses as early as ___ weeks
12.5
Non-nutritive sucking seen by __ weeks via ultrasound
15
Suckling (early feeding pattern) begins ___ weeks
18–24
Tongue moves forward & backward (more backward force)
suckling
Sucking (more mature pattern) emerges at ~________
4 months postnatal
Tongue moves up/down; lips more active
sucking
Consistent swallowing by ____ weeks
22-24
By ____ weeks, many fetuses can suckle and swallow adequately for oral feeding
32–34
why is understanding the development of the CNS important?
CNS regulates swallowing (buccal, lingual, pharyngeal)
Fetal facial expressions visible via 4D ultrasound by ____ weeks
20–24
The most critical period for brain development is from ____ weeks, however disruptions can occur after this period
3 to 16
four types of embryologic abnormalities
malformation, disruption, deformation, dysplasia
causes of embryologic abnormalities
genetic, environmental, or both; major cause of feeding/swallowing disorders
Teratogens (e.g., drugs, viruses) are most harmful ___ weeks gestation
3–16
Impact of embryologic abnormalities depends on
Critical developmental period
Dosage
Embryonic genotype
Injuries during early gestation cause greater long-term damage due to:
immature blood-brain barrier, development depends on integrity of early structures
Low birth weight and prematurity
Survival is rare <___ g or <____ weeks
CNS & respiratory system mature significantly by __ weeks
_______ abnormalities (CNS, airway, GI, etc.) may co-occur
500; 22–23
28
Multisystem
5 key phases of swallowing
Oral Preparatory Phase (Bolus Formation)
Oral Transit
Initiation of Pharyngeal Swallow
Pharyngeal Phase
Esophageal Transit
voluntary control
Oral preparatory & oral transit
mixed control
Pharyngeal phase
involuntary control
Esophageal phase
oral prep and oral transit includes:
Feeding (self or assisted)
Manipulation of food/liquid in the mouth
Bolus formation begins at what phase?
oral prep and transit
bolus prep for infants
latching and sucking (minimal bolus prep)
Food texture & oral skill level impact _____ of oral prep and transit
duration
structures involved in oral prep and transit
_______ is needed once material is in the mouth so that no liquid or food will be dribbled down the chin
The material is then held between the ______and ______
The ____________ help to generate suction in neonates and hold food between the teeth in older infants and children.
During this process, the _________ is in a lowered position and resting against the tongue base. This position helps to prevent a bolus from entering the pharynx before the swallow is produced.
The airway remains open and nasal breathing continues until a pharyngeal swallow is initiated
Lip closure
elevated tongue and hard palate
buccinator muscles
soft palate
initiation of pharyngeal swallow may occur at what structures for infants:
Anterior tonsillar pillars
Base of tongue
Valleculae
Pyriform sinuses
Essential for normal bolus formation and transit
pharyngeal swallow initiation
Sensory input of pharyngeal swallow drives motor modulation via ________
brainstem pathways
Types of Sensory Receptors for pharyngeal swallow initiation
Mechanoreceptors: touch, pressure (e.g., in tongue, palate, teeth)
Nociceptors: pain detection
Proprioceptors: sense shape, position
Chemoreceptors: detect chemical composition
Special receptors: for taste, smell, temperature
6 steps of pharyngeal swallow function
Elevation/retraction of soft palate (nasopharynx sealed)
UES opening (passive, via anterior laryngeal movement)
Laryngeal closure (vestibular level)
Tongue ramping/loading
Tongue propulsion
Pharyngeal clearance