Biomechanics of Amputees
1/19
Earn XP
Description and Tags
Biomechanics
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Biomechanics
the study of the forces and torques affecting movement and the description of the resulting movement
understanding and applying proper posture and the different types of levers that affect bodies from resistance training or daily activities
understand factors that affect human gait from walking or running in order to reduce or prevent accidents/injuries
Mechanics of the Knee Joint
the cruciate ligaments are able to pivot where they are attached to the bones because they are made of a non-rigid material
in a four-bar hinge the length of the four bars remains constant, but the angle between each bar can change so the lower leg can rotate
one important feature of the four-bar hinge is that the instantaneous centre of rotation approximately coincides with the cross-over point of the cruciate ligaments. this cross-over point moves as the joint opens and closes so that the knee does not have a fixed point of rotation, as does a simple pivot joint
the knee joint is a particularly sophisticated kind of four-bar hinge, because the cruciate ligaments are not rigid and have to be kept taut by the rolling action of the bones
Common Orthopedic Deformities of the Lower Extremity
varus and valgus hip
varus and valgus knee
varus and valgus ankle
Biomechanics Abnormality of the Lower Legs
limb length discrepancies can also develop into bowed legs or knock kneed
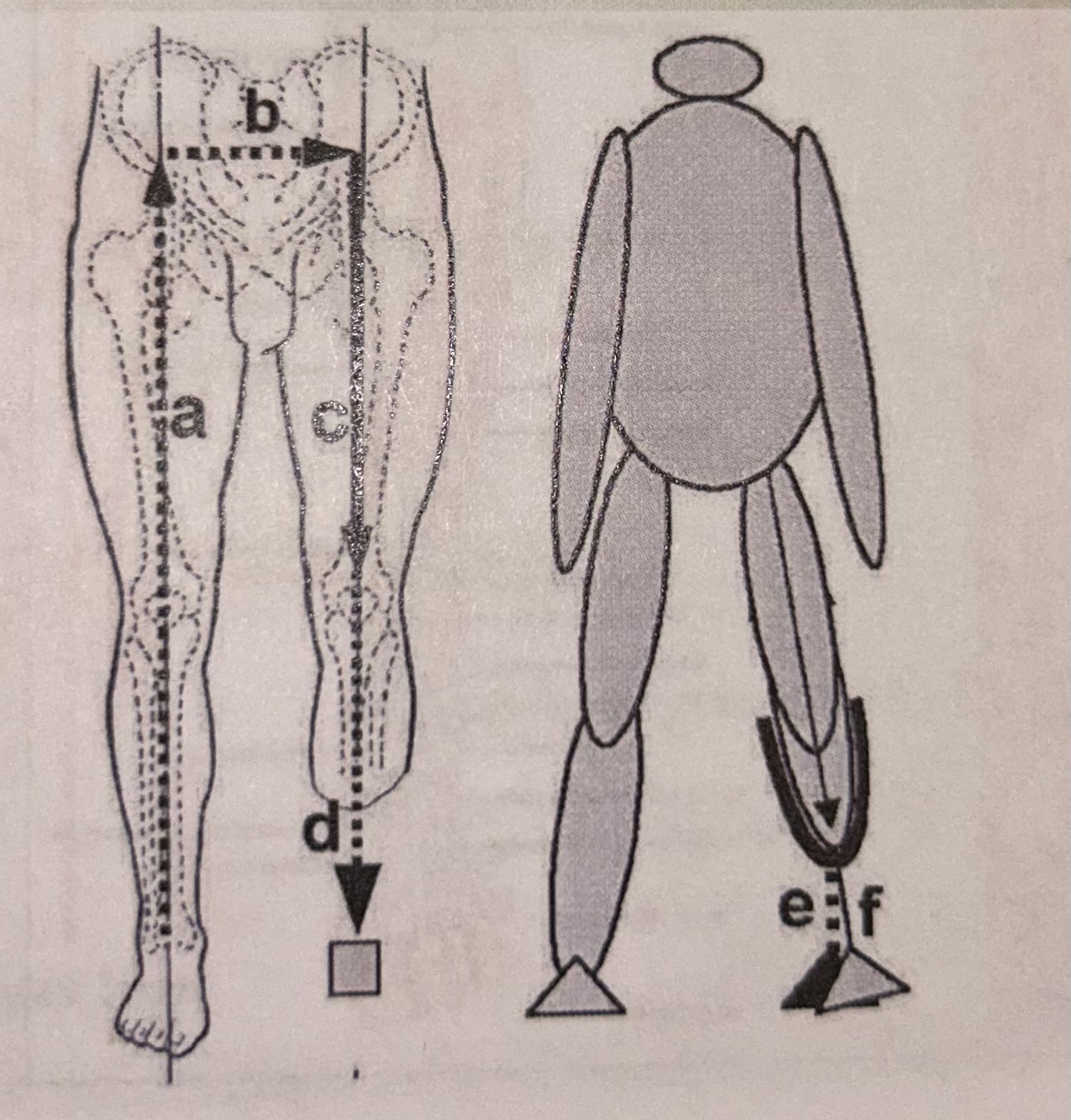
Ideal Alignment for Fitting BK Prosthesis
a: palpating the ASIS at the hip level then bisecting the unaffected limb
b: distance between the hip joints (equal to base of gait)
c: bisecting amputated limb
d: then connecting down to the prosthetic ankle
e, f: if knee adducted or abducted, causing prosthetic foot compensation - need to place prosthetic device with correct alignment
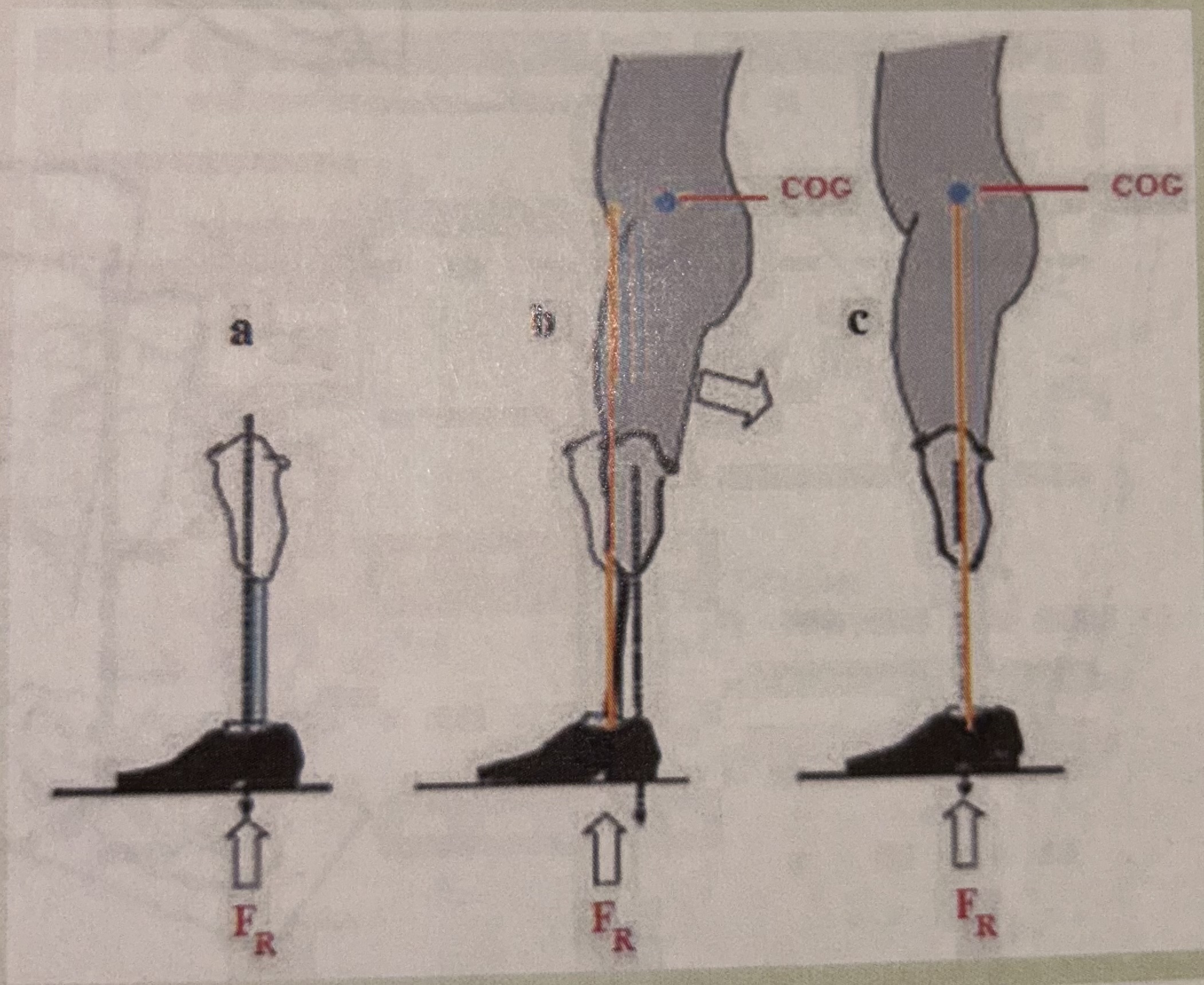
COG vs Lower Limb Axis
a: align the vertical axis of the limb - body weight should fall on the center of prosthetic ankle
b: unbalanced position
c: ideal/correct alignment
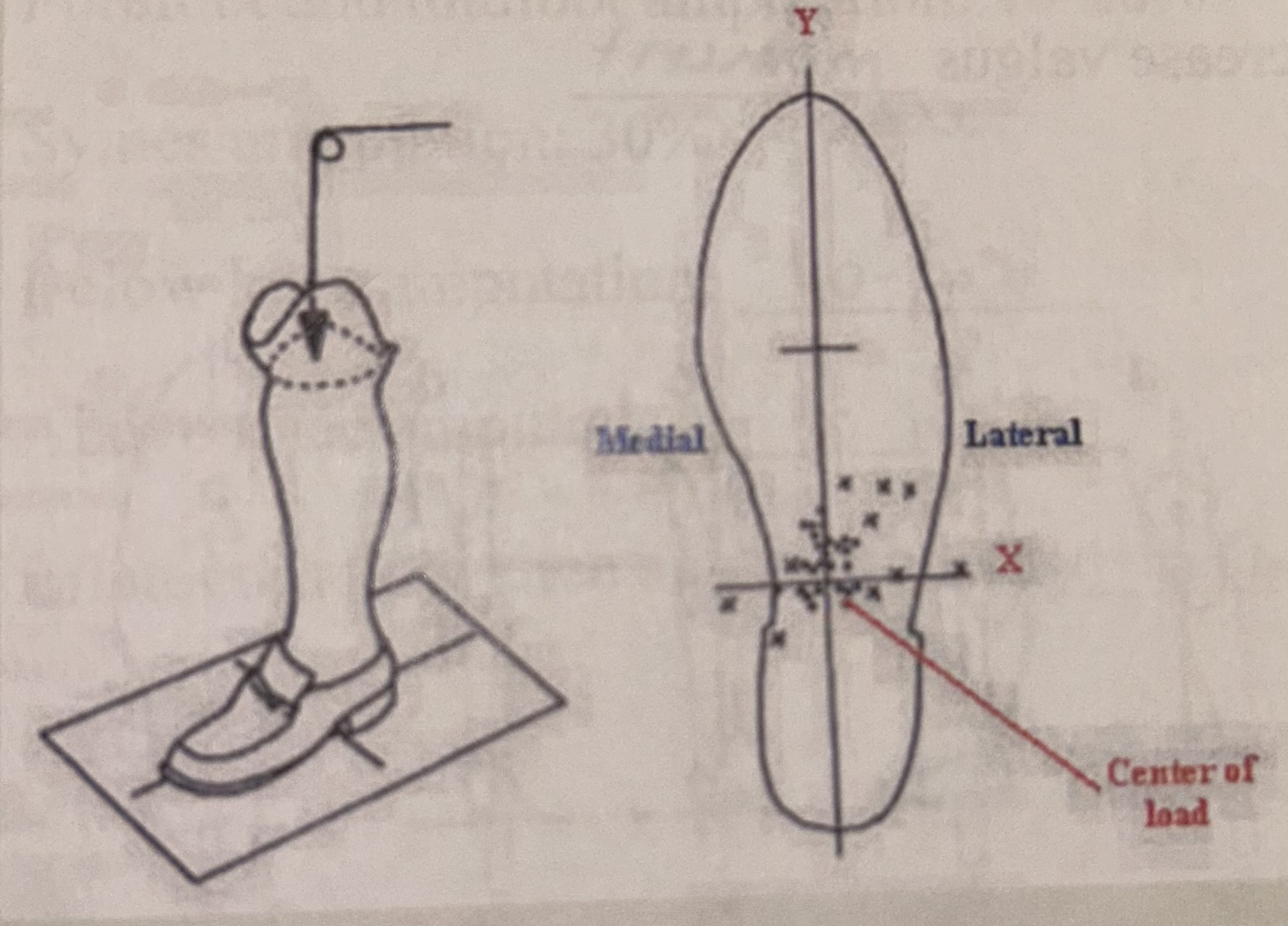
Ideal Center of Load (COL) on the Prosthetic Foot
COL of the body should project on the posterior 1/3 on Y axis, and medial 1/3 on X axis
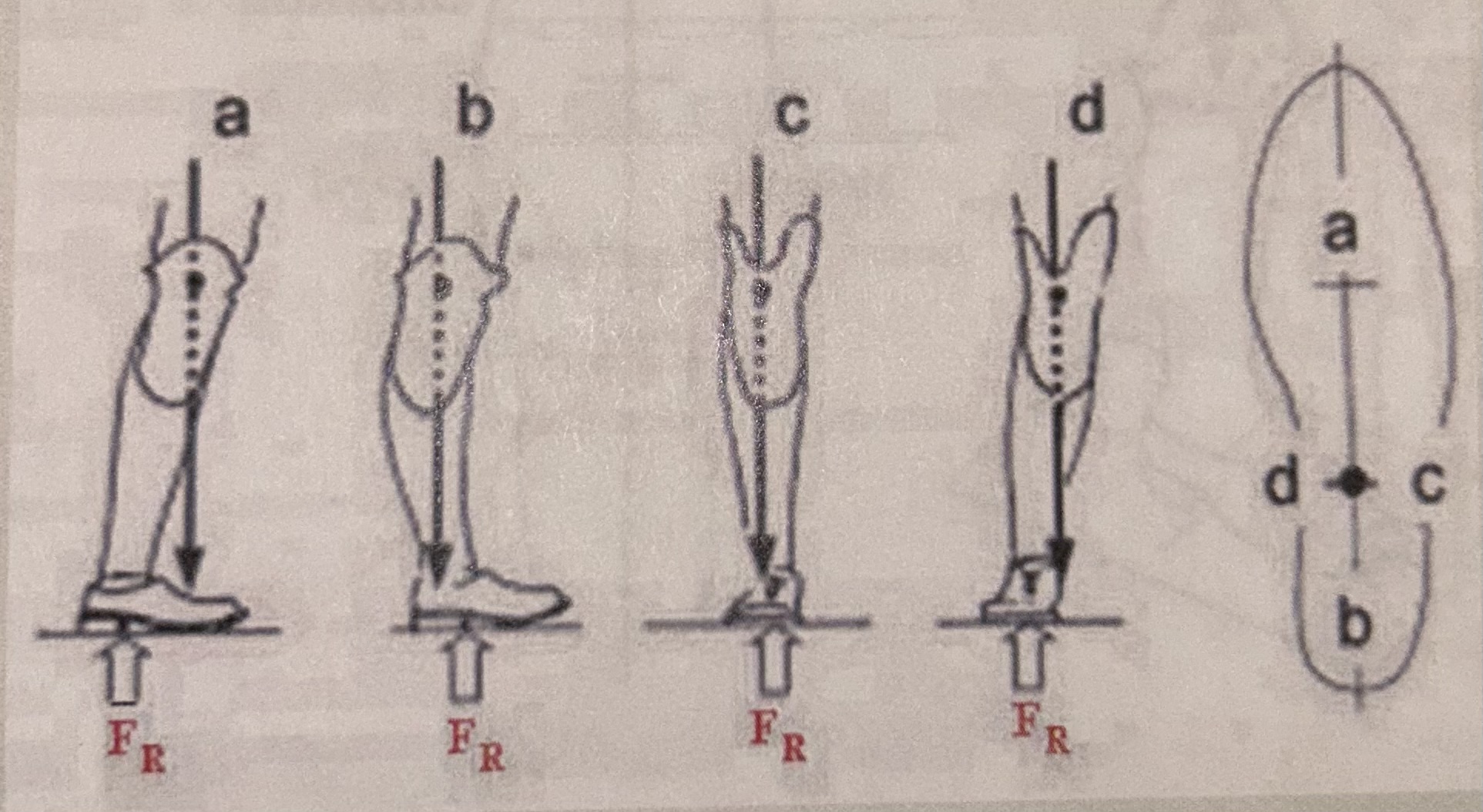
Gait Deviations and Projections of Socket Centers on the Shoe Tracing
a: excessive dorsiflexion
b: excessive plantarflexion
c: increase varus moment
d: increase valgus moment
A Common Transtibial Amputation Flap
overcorrection and under correction
Level of Muscle Energy Increase for Amputations
forefoot and mid foot amputation: 10-20%
symes amputation: 30%
below knee amputation: 40-50%
above knee amputation: 90-100%
bilateral below knee amputation: 60-100%
Research in Physics; Therapy Management of Lower Limb Amputations
Gertrude Mensch and Patricia M. Ellis, quoted studies that an amputee who walks the same distance as a non-amputee will have a higher level of oxygen consumption from the body
conclusion:
amputees with vascular deficiencies compared with non-amputees indicate an increase in oxygen consumption for:
BK from 9-20%
AK from 45-70%
bilateral AK up to 300%
A Common AK Amputation Flap
adductor flap
overcorrection and under correction
Alignment of Current Design Socket
perfect fit
cannot compensate for stump edema or vascular/blood pressure change
Mechanics of Ankle Complex
supination:
walk on outside of foot - inverted, plantar flexed, internal rotation
pronation:
walk on inside of foot - everted, dorsiflexed, external rotation
Perform Knee Mechanics
ROM and muscle strength:
test unilateral and bilateral to compare
frontal plane stability
ACL and PCL function
Check Hip Mechanics
have patient stand up
passive and active ROM of stump
muscle strength unilateral and bilateral (supine position or sit down on the chair)
compare bilaterally
Anisomelia (Leg Length Discrepancy)
Apparent method
measure from xiphoid process or umbilicus to medial malleolus
true method
measure from ASIS to medial malleolus
The Gait Cycle
the gait cycle is defined by the mechanics of walking or other forms of ambulation
three main phases: stance, toe-off, swing
FDA standards: 20 degrees of plantarflexion and 15 degrees of dorsiflexion
Complications of Wearing Artificial Limbs
gait is the major concern
physical activities
motion control (balance)
pain developing secondary to pressure from body load on the contact surface of the stump and the device
phantom pain
poor material selections for contact surface (materials can reduce friction, heat, and high oxygen permeability)
material allergies result in developing contact dermatitis
pressure sore/ulceration developing secondary from friction and pressure of body on materials
anesthetics
psychological concern
Phantom Pain
sensations felt by amputees: tingling, twisting, cramping, pins-and-needles, stabbing pains, pressure, a sense of fullness (as if the limb was still there, but slightly edema/swollen)
the ghost-limb sensations: a non-amputee feels when his/her foot has “fallen asleep” to the point of being numb, then sensation comes back painfully. the majority of amputees experience these sensations to some degree
an amputee may describe the sensation as being in a specific location, such as “on the bottom of the big toe” or “on the right side of the shin, right below the knee, going down in a straight line”
the phantom sensations are intermittent: come and go, unpredictable
causes - “brain re-organization”: after an amputation surgery, the brain loses input from the missing nerves. however, the neurons later become active again after the wound is healed, responding to input from the nerves that remain. consequently, pressure on the stump might trigger a response in the part of the brain that used to nerves in the missing limb, thus sensations are felt as if they were in the missing limb