Looks like no one added any tags here yet for you.
What is sepsis?
What is septic shock?
How does treatment differ?
Sepsis: Life threatening organ dysfunction caused by dysregulated host response to infection.
Shock: Sepsis with metabolic/circulatory abnormalities.
Treated similarly but shock requires vasopressors.
Sepsis/Septic Shock: Etiology (3)
1) Pneumonia (MCC)
2) Intra-abdominal
3) GU infections
Sepsis/Septic Shock: Etiology
Gram Positive (2)
Gram Negative (3)
Positive: S. aureus and S. pneumoniae (nasopharynx)
Negative: E. coli, Klebsiella, Pseudomonas aeruginosa (GU/GI)
Sepsis/Septic Shock: Risk Factors (2)
1) Chronic Disease (HIV/COPD/Cancer)
2) Immunosuppression
What are the 3 defining characteristics of septic shock?
1) Sepsis
2) Need for vasopressors to keep MAP >65
3) Lactate >2 even with fluids
3 factors for progressing from infection to organ dysfunction?
1) Load/virulence of infection
2) Comorbidities
3) Genetics (ability to respond)
Pro-inflammatory reactions in sepsis cause what? What about anti-inflammatory reactions?
Pro-Inflammatory: Tissue damage
Anti-Inflammatory: Susceptibility to 2nd infection
Sepsis/Septic Shock: Clinical Presentation
Cardiovascular
Respiratory
BP: Hypotension (High SVR)
O2: Hypoxemia
Sepsis/Septic Shock: Clinical Presentation (SVR/CO)
Early Shock
Post-Volume
Early Shock: High SVR, low CO
Post-Volume: Low SVR, high CO
How does a patient in septic shock respond to volume resuscitation?
Remain hypotensive.
Sepsis/Septic Shock: Clinical Presentation
Renal
CNS
Renal: Oliguria, azotemia (high BUN)
CNS: Delirium (due to inflammation)
What might be a necessary treatment due to chronic renal issues in septic shock?
Hemodialysis.
What two studies will you want to order if you see delirium or CNS issues in septic shock? What do you expect if CNS issues are due to sepsis?
CT: No focal lesions
EEG: No encephalopathy
Sepsis/Septic Shock: Dx
CBC (WBC/Platelets)
Lactate
Bilirubin
BUN/Cr
CBC: Thrombocytopenia, leukocytosis/penia with left shift
Lactate: Elevated >2.0
Bilirubin: Elevated
BUN/Cr: Elevated
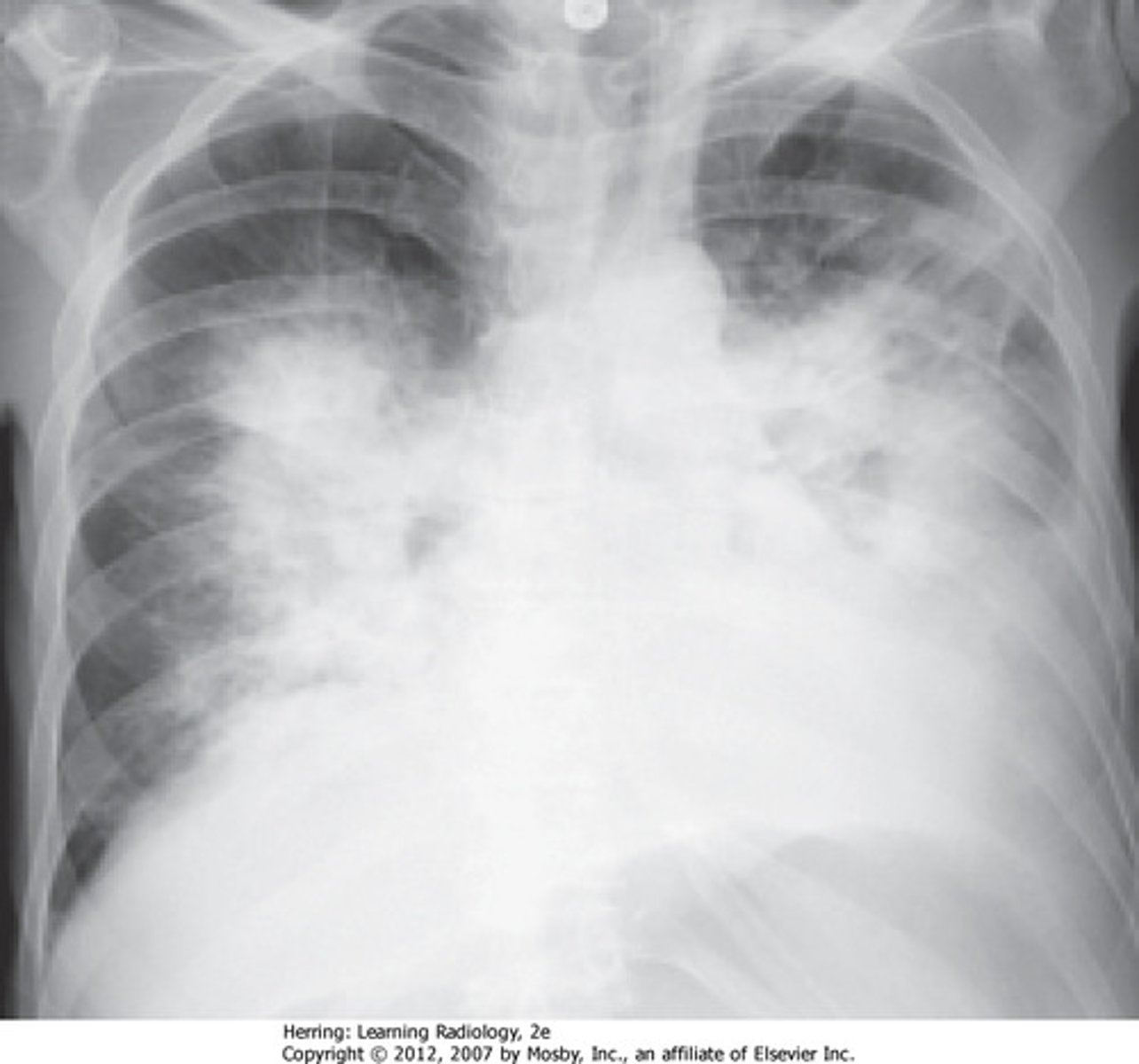
Sepsis/Septic Shock: Dx
CXR (ARDS)
Dense infiltrates (non-cardiac origin)
What do you want to order within the 1st hour of sepsis diagnosis to help guide your treatment?
Blood cultures -> gram stain.
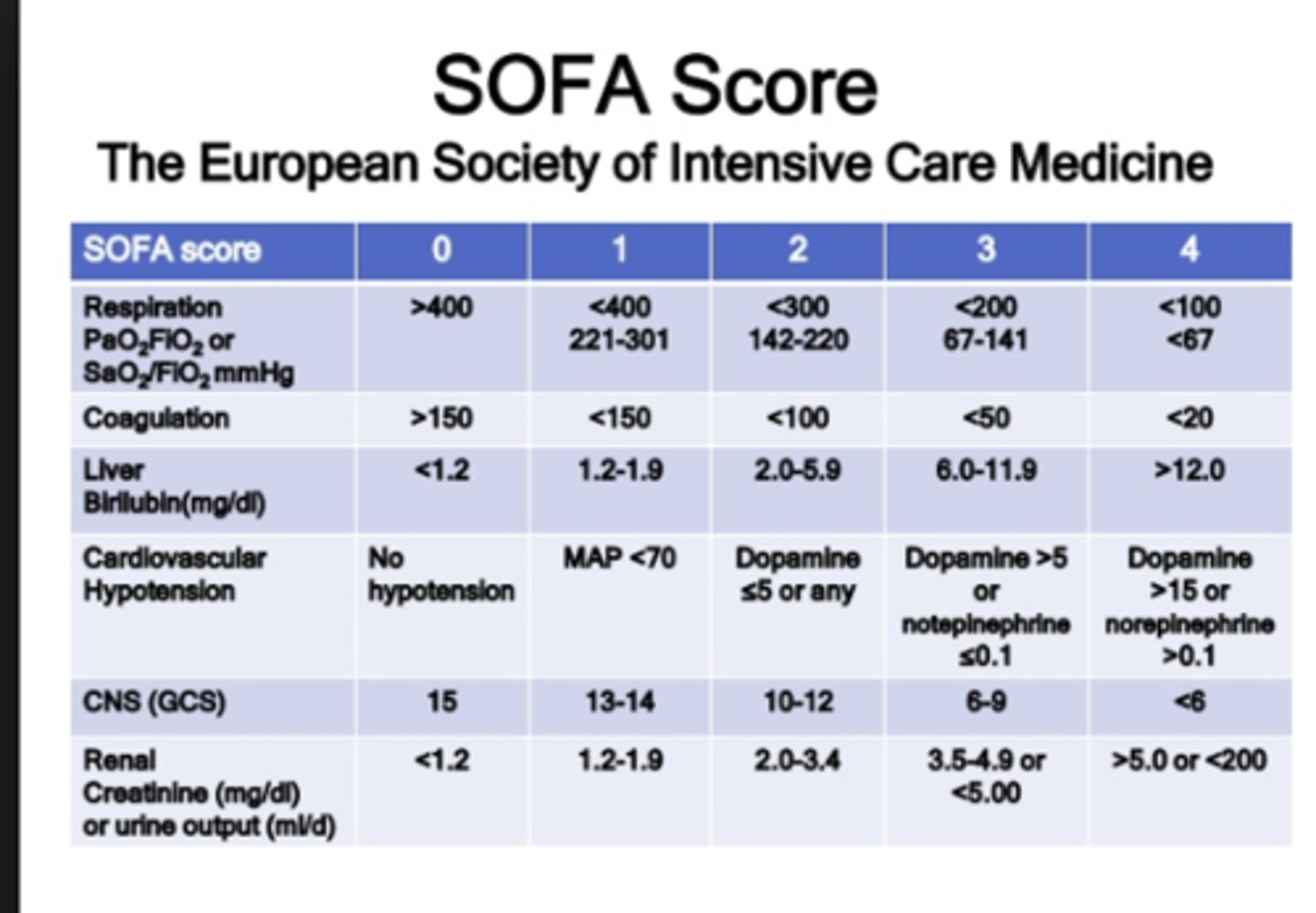
What is the SOFA score? What does it tell you?
What does a score of greater than 2 mean?
SOFA: Sequential Organ Failure Assessment (ICU)
- Tells us if/when organ function is impaired
- 10% death increase
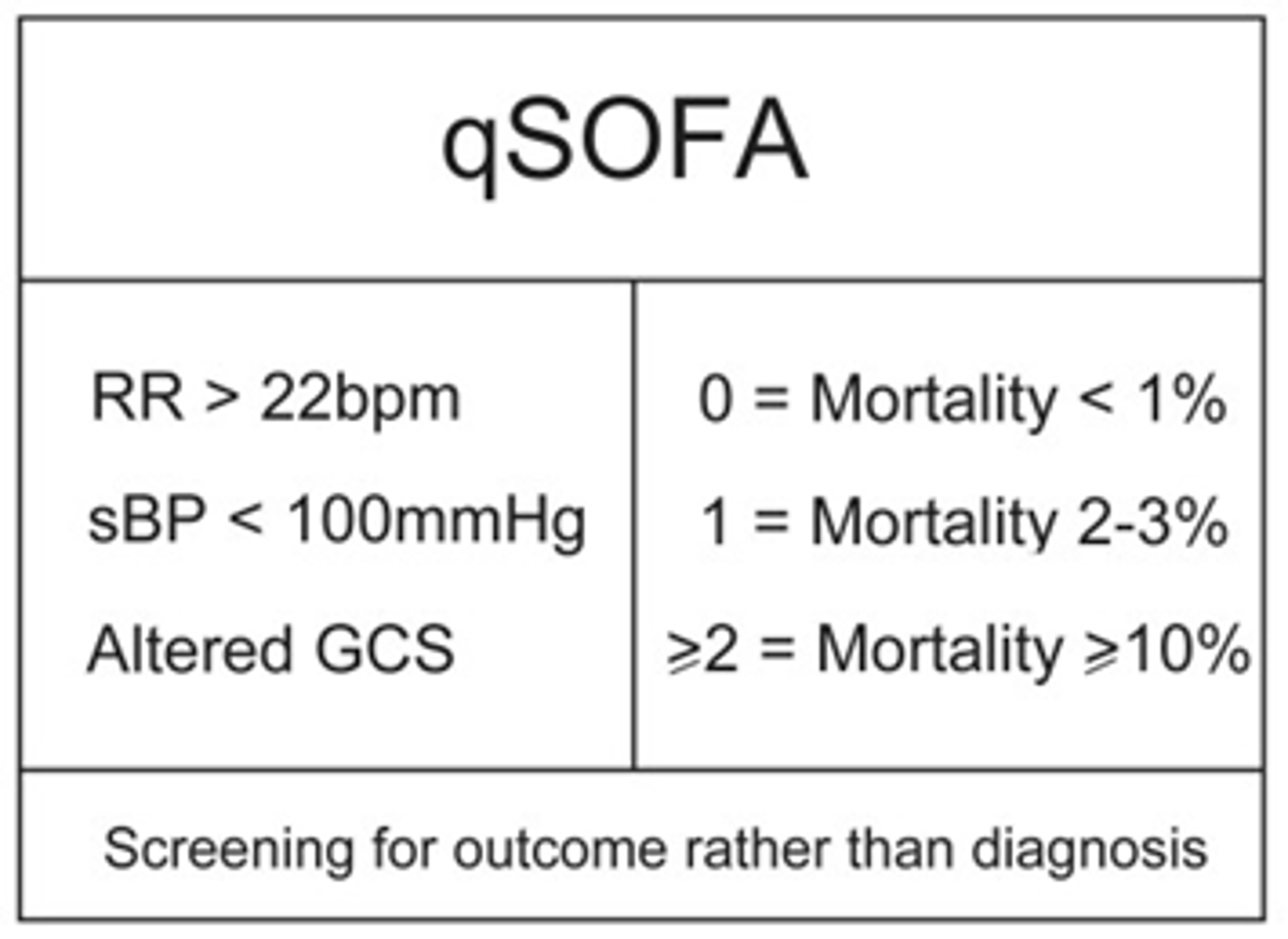
What is the qSOFA score? What does it tell us? How does the point system work? What does a score above 2 mean?
qSOFA:
- Tells us risk of sepsis outside the ICU
- 10% death increase
What are the 3 qSOFA criteria?
RR > 22
sBP < 100mmHg
Altered mental status
Sepsis/Septic Shock: Tx
Fluids
Fluids:
- Volume resuscitation
- IV crystalloid (30mL/kg/3hr)
What is the goal MAP with fluid treatment? What is the main goal of using fluids aside from gaining pressure?
MAP > 65
Goal = normalize lactate.
Sepsis/Septic Shock: Tx
Antibiotics
Empiric Antibiotics (broad):
- Start within 1hr before culture results
- Pip/Taz, cefepime, meropenem, imipenem/cil
When would you want to throw in MRSA to the empiric treatment?
Hx of MRSA or possible abscess.
Sepsis/Septic Shock: Tx
Vasopressors
NE -> increase BP.
Avoid dopamine.
What will you do to the patient in order to administer pressors?
Central and arterial line.
Why would you want to add in a steroid such as hydrocortisone? Why can it be bad?
Reduce systemic inflammation, but must consider that it can worsen bacterial infections.
Sepsis/Septic Shock: Prognosis
Mortality Rate
Complications
MR: 20%
Complications: Lasting neuro symptoms, low quality of life
Sepsis/Septic Shock: Prevention (3)
1) Avoid unnecessary abx
2) Limit indwelling catheters
3) Adhere to infection control protocols
Fever of Unknown Origin: Etiology (3)
1) Cancer
2) Infection
3) Autoimmune - SLE
Fever of Unknown Origin: Diagnostic Requirements
Illness Length
Temperature
Immune Status
Diagnosis Progress
Illness Length: >3 weeks
Temperature: >100.9 (2x)
Immune Status: Immunocompetent
Diagnosis Progress: 3x visits/days w/ no confirmed diagnosis
How would you define neutropenic fever of unknown origin?
ANC<500 (including all other criteria).
Fever of Unknown Origin: Diagnostic Criteria
Prolonged Fever
Episodic Fever
Prolonged: >6 months (granulomatous disease)
Episodic: Meet criteria, can go 2 weeks without fever
Fever of Unknown Origin: Clinical Findings
Behavior
Vitals
History
- Observe patient temp. taking
- Tachy, chills
- Social, travel, diet
What do you want to order for ALL patients with FUO? What are some other diagnostics worth ordering (3)?
- CXR all patients
- Cultures of sputum, blood, urine, CSF, stool
- Blood smears
- Imaging: CT, MRI
-> Keep looking until you find cause!
Fever of Unknown Origin: Tx
No empiric antibiotics/steroids until culture results come back.
What would you do if a patient with FUO was immunocompromised, exhibits signs of rapid decline, or has constitutional symptoms?
Admit.
Infectious Diarrhea: Etiology
Culprits (4)
1) Norovirus
2) C. diff
3) E. coli
4) Shigella (bloody)
Infectious Diarrhea: Length
Acute
Chronic
Acute: <14 days
Chronic: >14 days
Infectious Diarrhea: Quantity
Mild
Moderate
Severe
Mild: 3 or less daily
Moderate: 4 or more daily with local abdominal symptoms
Severe: 4 or more daily with systemic symptoms
Infectious Diarrhea: Clinical Presentation (Freq, Vol, blood)
Inflammatory
Non-Inflammatory
Inflammatory:
Frequent, bloody, low volume stool with urgency, fever
Non-Inflammatory:
Less frequent, watery, very high volume
How will infectious diarrhea look if a preformed toxin is consumed versus a toxin produced after ingestion?
Pre-Formed: 1-6 hr, no fever, vomiting, toxin detected in food
Post-Ingestion: 8-16 hr, cramping, less vomiting, toxin in stool
Infectious Diarrhea: Dx
Culture
Stool -> fecal leukocytes. Perform if symptoms lasting 3-4 days.
Infectious Diarrhea: Tx
Non-Pharmacological
Often self-limiting.
IV fluids and electrolytes.
Infectious Diarrhea: Tx
Pharmacological
If severe illness/dehydration or immunocompromised.
Fluoroquinolone or Azithromycin.
What do you want to avoid regarding infectious diarrhea treatment?
Loperamide (anti-motility).
Osteomyelitis: Etiology
MCC
S. aureus
Osteomyelitis: Pathogenesis (3)
Long Bones or Vertebrae:
1) Direct inoculation (fracture, surgery)
2) Invasion
3) Skin breakdown
Osteomyelitis: Complication + Presentation
Epidural abscess on vertebrae.
Radicular (radiating) back pain + fever.
Osteomyelitis: Clinical Presentation (3)
Local tenderness
Constitutional sxs
Back pain
Osteomyelitis: Dx
Cultures (2)
ESR/CRP
Culture: Blood -> if negative -> BM bx and culture
ESR/CRP: Elevated (follow course of tx)
Osteomyelitis: Dx
XR
CT
MRI
XR: Early findings normal, later see demineralization
CT: Localize abscess
MRI: Most specific
What is the best diagnostic tool because it is the most sensitive for osteomyelitis?
Bone scan w/ gallium.
Osteomyelitis: Tx
Pharmacological (2)
Duration
Cefazolin/Naficillin (MSSA) or Vanco (MRSA)
- 4 to 6 weeks
- IV preferred
What is required for osteomyelitis with extensive disease, epidural abscess or recurrent infection?
Surgical consult.
UTI: Etiology
MCC (Uncomplicated)
E. coli
UTI: Definitions
Unresolved
Persistent
Reinfection
Unresolved: never sterilized (non compliance, bacteria resistance, mixed infection and only treated one)
Persistent: initially sterilized but comes back
Reinfection: new infection, new pathogen
UTI: Pathogenesis
Ascending route up the urinary tract MCC.
Why are women more likely to get a UTI? In what situation would a male be likely to get one?
Female: Sex, short urethra, normal flora
Male: Uncircumcised
Acute Cystitis: Epidemiology and Etiology
Usually bacterial (UTI). Can also be viral or other pathogenesis.
Rare in adults.
Rare in men -> investigate pathology (renal stone, prostatitis, chronic urinary retention).
UTI: Clinical Presentation
- Urinary frequency/urgency
- Suprapubic pain
- Hematuria possible
- CVA tenderness
What do you want to rule out when working up a UTI?
PID, vulvovaginitis, urethritis, prostatitis.
UTI: Dx
Urine (2)
UA: Nitrites
Clean Catch Urine Culture: >100k
What imaging is indicated for men if presenting with UTI/acute cystitis?
US of abdomen.
CT if recurrent.
UTI: Tx
Female
Male
Adjuvant
Female: Fosfomycin, nitrofuratonin, tri/sulf
Male: Find underlying etiology
Adjuvant: Phenazopyridine (urinary analgiesic)
UTI: Complications
Pyelonephritis (WBC casts in urine).
Prostatitis in men.
UTI: Prevention (3)
Hydration - frequently empty bladder.
Prophylactic abx for post-menopausal women.
Minimize indwelling catheter use.
Endocarditis: Etiology
MCC
S. aureus
Endocarditis: Essentials of Diagnosis (5)
Fever
Pre-existing organic heart lesion
Positive blood cultures
Vegetation on echo.
Systemic emboli
Endocarditis: Risk Factors (2)
1) Valvular Disease
2) Congenital Defects
What bacteria commonly causes native valve, early prosthetic valve, or IVDU endocarditis? What about late prosthetic valve endocarditis?
S. aureus.
Strep.
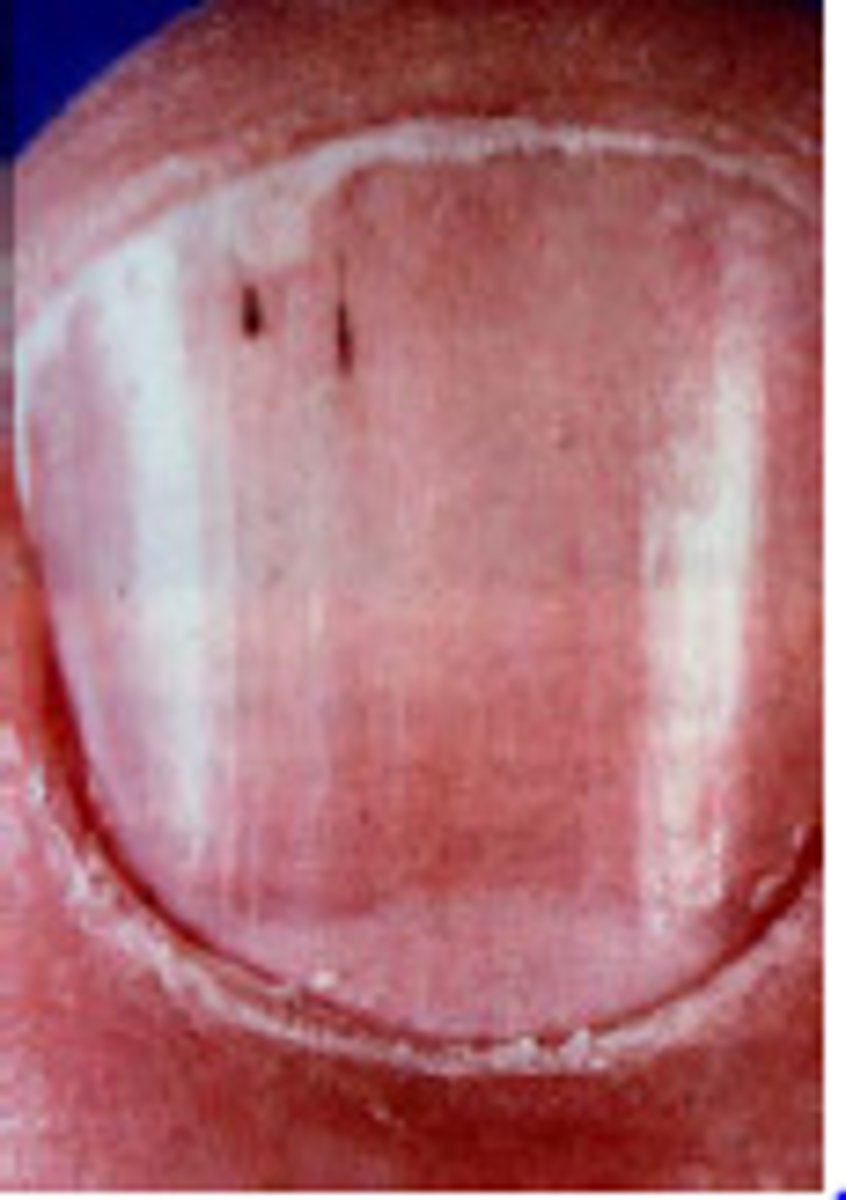
Endocarditis: Clinical Presentation
Nails
Heart Sounds
Nails: Splinter hemorrhages
Heart: Changing regurgitant murmur (caused by valve/cardiac damage)
Endocarditis: Clinical Presentation
Eyes
Roth spots
Endocarditis: Clinical Presentation
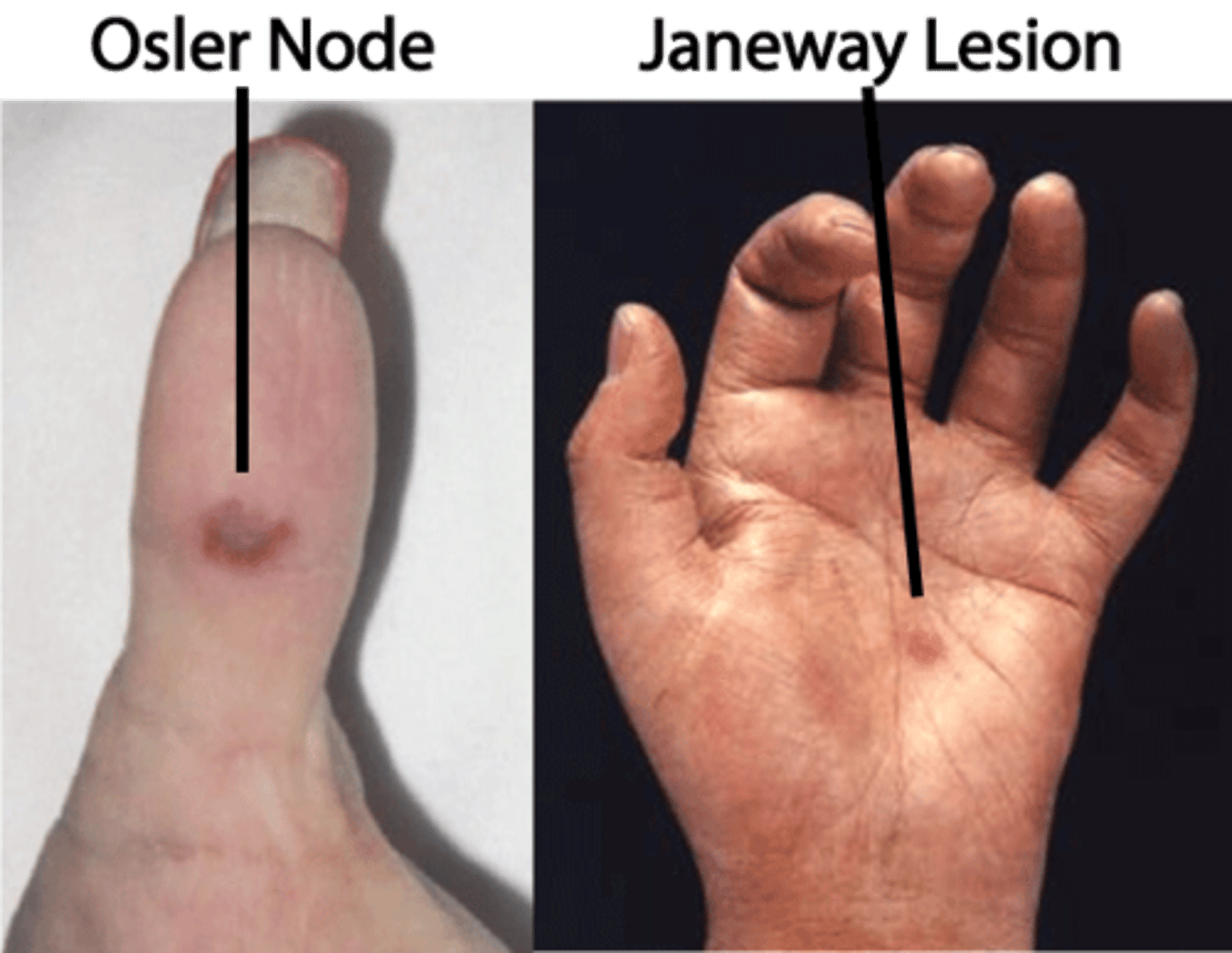
Peripheral Lesions (3)
1) Osler Nodes (painful, on fingers/toes)
2) Janeway Lesions (painless, on soles/palms)
3) Petechiae-palate
Endocarditis: Dx
CXR
EKG
CXR: Pulmonary infiltrates
EKG: Conduction abnormalities
What are the two echocardiography studies for diagnosing endocarditis?
TTE - transthoracic (less sensitive)
TEE - transesophageal (more sensitive)
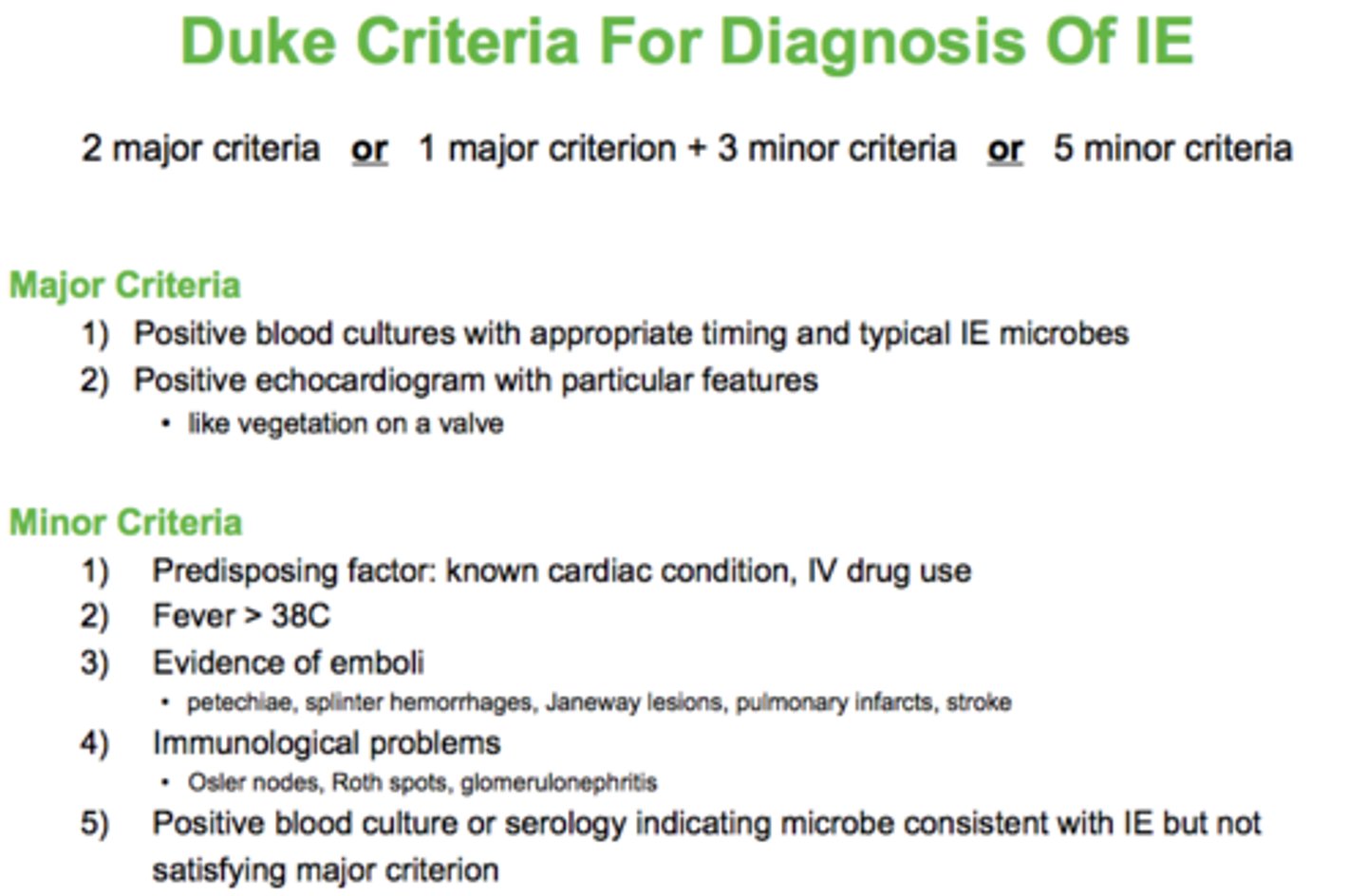
What is the Duke criteria used for diagnosing bacterial endocarditis?
2 major criteria
OR
1 major + 3 minor criteria
OR
5 minor criteria
Endocarditis: Dx
Cultures
Blood Culture: 3 sets
Does a negative blood culture rule out endocarditis?
No - transient bacteremia.
Endocarditis: Tx
Pharmacological
Empiric treatment for Staph, Strep, Enterococci:
Ceftriaxone + Vancomycin (2-4 weeks)
-> move to narrow regimen based on cultures.
How long do you treat prosthetic valve endocarditis?
6 weeks.
If someone has a prosthetic valve and is going for a dental or respiratory procedure, what should you do?
Antibiotic prophylaxis pre-procedural (Amoxicillin).
Meningitis: Etiology
Bacterial (4)
Can spread to CNS hematogenously from other infection sites. Massive inflammatory response to pathogen.
Bacterial:
S. pneumoniae (MCC)
N. meningitidis
GBS
Listeria
Meningitis: Clinical Presentation
- Headache
- Sensory disturbance
- Head/neck stiffness
- Fever
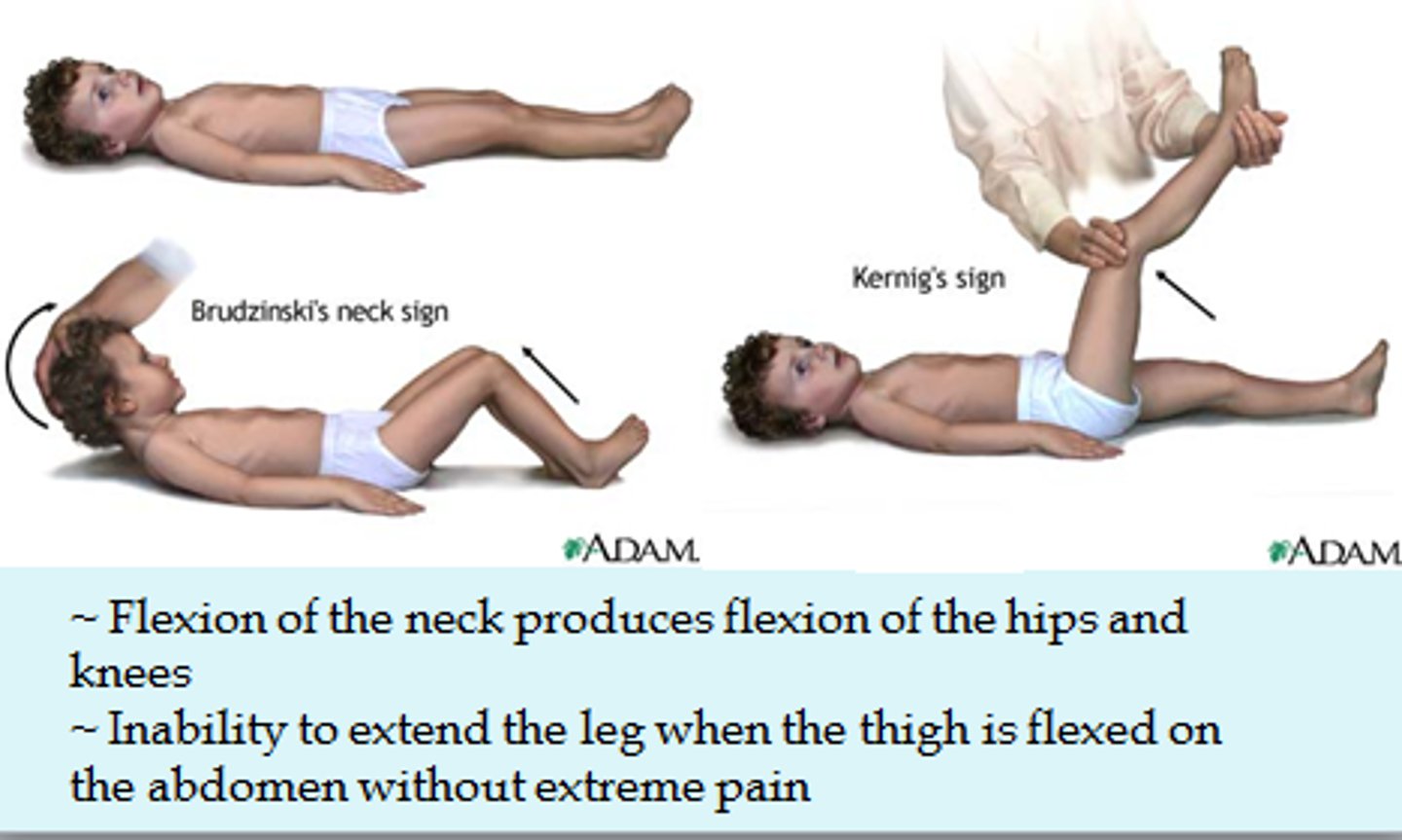
Meningitis: Clinical Presentation
Special Tests
Brudzinski's and Kernig's positive
Meningitis: Clinical Presentation
Elevated Intracranial Pressure (5)
Altered level of consciousness
Papilledema
Dilated, non-reactive pupils
Decerebrate posturing
Cushing reflex
Meningitis: Dx
Cultures
Imaging
Culture: Blood and CSF
Imaging: CT, MRI
What does CSF show in bacterial meningitis?
WBC elevated
Glucose low
Protein elevated
Bacterial Meningitis: Tx
Pharmacological (2)
Abx (Empiric - ampicillin + 3rd gen cephalosporin)
Dexamethosone
Neisseria meningitis:
Presentation
Tx
Prophylaxis
Presentation: Petechial rash, myalgia
Tx: Pen G or Vanco + ceftriaxone
Prophylaxis: Rifampin
Pneumococcal meningitis:
Presentation
Treatment
Presentation: Associated with sinus infection, head trauma, pneumonia; no rash
Treatment: Ceftriaxone + Vanco
When would you need to do a CT scan prior to a lumbar puncture? Why?
Abnormal neuro exam. Want to ensure no ICP before LP, can cause herniation.
Viral Meningitis: Etiology (2)
Herpes simplex
Enterovirus
What is the most important diagnostic for viral meningitis?
CSF PCR.
How will glucose and protein look in CSF of viral meningitis?
Normal.
How do you treat viral meningitis?
Acyclovir. Usually self-limited process.
Most likely also empiric antibiotic treatment because you cannot initially tell which it is. Taper as labs come back.
Encephalitis: Etiology
Inflammation of brain tissue (not meninges).
EBV, HIV, CMV, HSV.
Encephalitis: Clinical Presentation
Hallucinations, agitation, psychosis, seizures.
Encephalitis: Dx (3)
CSF -> PCR
CT/MRI/EEG
Brain bx
Encephalitis: Tx (2)
Acyclovir and anti-convulsants for seizures.
URI: Etiology
Viral. Easily transmitted.