ABNORMAL PSYCHOLOGY - Midterm 1
1/123
Earn XP
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
124 Terms
Depressive Disorders
Major Depressive Disorder (MDD)
Persistent Depressive Disorder (Dysthymia)
Premenstrual Dysphoric Disorder
Major Depressive Disorder
intrapsychic disorder —> exists within the mind or psyche
frequently a chronic disorder & commonly re-occurs after recovery
WOMEN are at a much higher risk for depression —> average ratio 2:1
sex differences remain across countries, where overall prevalence rates vary
depression appears more commonly in younger than older adults —> younger generations more prone to depression
rates of depression seem to be increasing most quickly in young men
Life events
sudden, or at least relatively distinct, changes in the external environment
Severe Events — events with “marked or moderate long-term threat”–e.g. a spouse losing his or her job —> Clearly related to the onset of a depressive disorder
Less severe events–e.g. a spouse being threatened with a job loss —> Appear insufficient to elicit depression
Additivity effects — when severe or less-severe life events are summed
Severe life events have an even greater effect if they are summed
Less-severe life events are insufficient to elicit depression even when they are summed
Stress sensitization model (Depression Life Event Model)
A major event is needed to trigger a first onset
Less severe (but more common) life events can initiate recurrent episodes
Beck’s Cognitive Theory of Depression
Content develops from interactions that occur during childhood —> self-schema
e.g. Childhood experiences characterized by abuse, stress, or chronic negativity produced schemas that
Guide attention towards negative events
Lead to the enhanced recall of negative experiences
Distort information to fit the schema
“Cognitive Triad”
Those with depression have dysfunctional schemas that lead to negative thoughts about the self, the world, and the future
All-or-nothing thinking (Cognitive Models — Distortions — Depression)
when situations are viewed in only two categories instead of on a continuum
“If I am not a complete success I’m a failure
Selective abstraction (Cognitive Models — Distortions — Depression)
when negative details are focused on without taking into consideration the entire context
i.e. in conversing with a group of people, the depressed person may only notice the one person who yawned and not the others who appeared interested
Overgeneralization (Cognitive Models — Distortions — Depression)
sweeping judgements or predictions based on a single incident
“Because last night’s date did not go well, all women find me unattractive.”
Emotional reasoning (Cognitive Models — Distortions — Depression)
one thinks something must be true because one feels it to be so
“I feel ugly so I must look ugly”
Personalization (Cognitive Models — Distortions — Depression)
when the individual takes responsibility for the negative actions of others without considering more plausible explanations for their behaviors
Depression Attribution-Based Models
Seligman focused on depressed persons’ expectations that they are helpless —> learned helplessness theory
Nesse —> Suggests that depression is nature’s way of telling us that we are barking up the wrong tree
Abramson
Positive events are given specific unstable, external attributions–e.g. “I succeeded because the test was really easy.
Negative events are given global, stable, and internal attributions–e.g. “I failed because I am a stupid person.
Negative attribution styles are seen as a vulnerability factor to depression
OCD Four Basic Symptom Categories
Symmetry: symmetry obsessions and repeating, ordering, and counting compulsions
Forbidden thoughts: aggression, sexual, religious, and somatic obsessions and checking compulsions
Cleaning: cleaning and contamination
Hoarding: hoarding obsessions and compulsions
The belief that accurate knowledge can be acquired through observation*
An essential element of the scientific method
The tendency for people to cling to their assumption
the process by which individuals are assigned to already existing groups
An anxiety disorder characterized by recurrent unexpected panic attacks and one of the following:
Persistent worry about having attacks (or about their consequences)
The development of significant, maladaptive behavioral changes designed to avoid having attacks
EPIDEMIOLOGY
Lifetime prevalence of panic attacks (which often do not warrant a diagnosis) is 23%
Those with PD with agoraphobia are more likely to seek treatment than those with (just) PD
A chronic disorder characterized by excessive, uncontrollable worry about a number of different life circumstances
This worry must be accompanied by at least three common manifestations of anxiety–e.g. muscle tension, sleep disturbance, or irritability
EPIDEMIOLOGY
Between-group racial and ethnic differences —> White Americans are more likely to be diagnosed than are Black/African, Hispanic/Latino, and Asian Americans
Comorbidity —> 71% meet criteria for mood disorder, 90% have a comorbid anxiety disorder (most common being PD w/ agoraphobia and SAD)
A mental health condition featuring unwanted repetitive thoughts (obsessions) and actions (compulsions) aimed at reducing anxiety.
ego-dystonic disorder —> majority of patients have good insight regarding their obsessions
Patients misinterpret normally occurring intrusive thoughts as overly important and dangerous
Patient attempts to alleviate the distress using ritualistic behaviors or avoidance behaviors
Behaviors results in transient distress reduction —> paradoxically reinforces likelihood that patients will engage in similar behaviors in the future —> Maladaptive beliefs are never given the chance to be disconfirmed
heterogeneous disorder —> Different patients are characterized by different symptomatic manifestations
Contamination/washing and checking are the most prevalent–seen in more than ½ of OCD patient
Fear is an immediate alarm response to danger, while anxiety is a longer-lasting mood state associated with preparation for possible harm.
Fear - an alarm response when danger is perceived to be present
Involves a triggering of the fight-flight-freeze (FFF)
fear (panic) = more immediate
Purely excitatory input to the FF mechanism
Anxiety - a future-oriented mood state associated with preparation for possible harm
Involves a priming (simultaneous excitatory and inhibitory input to) the FFF mechanism when danger is perceived to be possible at a later point in time
longer lasting & future oriented
Simultaneous excitatory and inhibitory input to the FFF mechanism
A persistent and marked fear of social situations in which the individual might be judged or evaluated by others
exposure to the feared social situation(s) has to almost invariably provoke an immediate fear response
The fear must be associated with either some avoidance of the phobic cue, or endurance or exposure to that cue with intense fear or anxiety
EPIDEMIOLOGY
SECOND MOST PREVALENT ANXIETY DISORDER
Higher percentage of White Americans diagnosed than Black/African, Hispanic/Latino, and Asian Americans
Higher percentage among Native Americans than White Americans
Most common fears reported are those related to performance-based situations
Highly comorbid with other mood, anxiety, and personality disorders, particularly avoidant personality disorder
Most common comorbid anxiety disorders are PD, SP, and GAD
Diagnostic Criteria for Schizophrenia
A presence of two or more of the following for a significant portion of a month: delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, negative symptoms.
Major Depressive Episode Criteria
A period of at least two weeks with either depressed mood or loss of interest or pleasure, along with four additional symptoms such as weight change, sleep disturbances, or fatigue.
Panic Attack Criteria
An abrupt surge of intense fear or discomfort reaching a peak within minutes, featuring symptoms like palpitations, sweating, trembling, or feelings of choking.
Generalized Anxiety Disorder (GAD) Diagnostic Criteria
A. Excessive anxiety and worry (apprehension expectation), occurring more days than not for at least 6 months, about a number of events or activities (such as work or school performance)
B. The individual finds it difficult to control the worry
C. The anxiety and worry are associated with three (or more) of the following six symptoms (with at least some symptoms having been present for more days than not for the past 6 months):
Restlessness, feeling keyed up or on edge
Being easily fatigued
Difficulty concentrating or mind going blank
Irritability
Muscle tension
Sleep disturbance (difficulty falling or staying asleep, or restless, unsatisfying sleep).
D.The anxiety, worry, or physical symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
E. The disturbance is not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition
F. The disturbance is not better explained by another medical disorde
Social Anxiety Disorder Criteria
A. Marked fear or anxiety about one or more social situations in which the individual is exposed to possible scrutiny by others. Examples include social interactions, being observed, and performing in front of others
B.The individual fears that he or she will act in a way or show anxiety symptoms that will be negatively evaluated (i.e., will be humiliating or embarrassing; will lead to rejection or offend others)
C. The social situations almost always provoke fear or anxiety
D.The social situations are avoided or endured with intense fear or anxiety
E. The fear or anxiety is out of proportion to the actual threat posed by the social situation and to the sociocultural context
F. The fear, anxiety, or avoidance is persistent, typically lasting for 6 months or more
G.The fear, anxiety, or avoidance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
H.The fear, anxiety, or avoidance is not attributable to the physiological effects of a substance or another medical condition
I.The fear, anxiety, or avoidance is not better explained by the symptoms of another mental disorder, such as panic disorder, body dysmorphic disorder, or autism spectrum disorder
J.If another medical condition (e.g., Parkinson’s disease, obesity, disfigurement from burns or injury) is present, the fear, anxiety, or avoidance is clearly unrelated or is excessive
Hoarding Disorder Criteria
Persistent difficulty discarding possessions regardless of their actual value, resulting in clutter that severely impairs living efficiency.
Diagnostic Features of Panic Disorder
A. Recurrent unexpected panic attacks. A panic attack is an abrupt surge of intense fear or intense discomfort that reaches a peak within minutes, and during which time four (or more) of the following symptoms occur (see other flashcard)
B. At least one of the attacks has been followed by 1 month (or more) of one or both of the following:
Persistent concern or worry about additional panic attacks or their consequences (e.g., losing control, having a heart attack
A significant maladaptive change in behavior related to the attacks (e.g., behaviors designed to avoid having panic attacks, such as avoidance of exercise or unfamiliar situations)
C. The disturbance is not attributable to the physiological effects of a substance or another medical condition
D. The disturbance is not better explained by another mental disorder
Neurodevelopmental Disorders Overview
A group of disorders that manifest early in development, characterized by developmental deficits in personal, social, academic, or occupational functioning.
Diagnostic Criteria for Major Depressive Disorder
At least five depressive symptoms present during the same two-week period, including either depressed mood or loss of interest, causing significant impairment.
Obsessive-Compulsive Disorder (OCD) Diagnostic Criteria
A. Presence of obsessions, compulsions, or both
Obsessions defined by:
Recurrent and persistent thoughts, urges, or images that are experienced, at some time during the disturbance, as intrusive and unwanted, and that in most individuals cause marked anxiety or distress
The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some other thought or action
Compulsions defined by
Repetitive behaviors or mental acts that the individual feels driven to perform in response to an obsession or according to rules that must be applied rigidly
The behaviors or mental acts are aimed at preventing or reducing anxiety or distress, or preventing some dreaded event or situation; however, these behaviors or mental acts are not connected in a realistic way with what they are designed to neutralize or prevent, or are clearly excessive
B. The obsessions or compulsions are time-consuming (e.g., take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
Diagnostic Criteria for Hoarding Disorder
Persistent difficulty discarding possessions, resulting in clutter that significantly impairs functioning.
Diagnostic Criteria for Dissociative Identity Disorder (DID)
Presence of two or more distinct personality states or an experience of possession, causing significant distress or impairment.
Dogma
A principle or set of principles laid down by an authority as incontrovertibly true
The Scientific Method
A procedure for finding truth using empirical evidence
A way of knowing something —> any scientific theory that cannot be disproven is worse than useless
The Sacred Approach
Animistic Phase —> connection between primitive beings and the forces of nature —> world populated by animated entities and forces that act on mind & soul
Mythological Phase —> every symptom caused by deity who could cure the disorder if appeased
Demonlogical Phase —> two competing forces struggled for superiority: creative & positive (God) and destructive & negative (demons)
Pythagoras on Psychopathology
Three Parts of the Soul
Reason — truth
Intelligence — synthesized sensory perceptions
Impulse — derived from bodily energies
Brain
center for rational parts of soul
Heart
center for irrational parts of soul
Hippocrates on Psychopathology
work highlighted naturalistic view
thought source of all disorders, mental & physical, were within the patient, not within spiritual phenomena
Hippocrates Four Basic Temperaments
Choleric — excess yellow bile —> tendency towards irascibility
Melancholic – excess in black bile —> inclination towards sadness
Sanguine – excess in blood —> prompted towards optimism
Phlegmatic – excess in phlegm —> apathetic disposition
Aristotle on Psychopathology
gave special attention to experimental verification & use of sensory-based, observable data
first major philosopher to take an inductive and empirical approach
Thought data should be grounded in empirical observables
Emil Kraepelin (Modern Psychiatry)
Established definitive patterns on two major disorders
Manic-depressive psychosis(now known as bipolar disorder)
Dementia praecox(now known as schizophrenic disorders)
Termed the autistic temperament
Eugen Bleuler (Modern Psychiatry)
recognized for his description of Schizophrenia (replacing dementia praecox)
Adolf Meyer (Modern Psychiatry)
Saw psychiatric disorders as a consequences of environmental factors and life events
Psychobiological approach to schizophrenia
Ego-dystonic
having thoughts or behaviors that are different from or go against a person's values, self-perception, or beliefs
inconsistent w/ beliefs —> intrusive & unwelcome
ex: Obsessive compulsive disorder
Ego-Syntonic
thoughts, feelings, or behaviors that are consistent with a person's self-image, values, and goals
behaviors / thoughts align with personal values and goals
ex: obsessive compulsive personality disorder
Diagnostic/Classification systems
lists of terms for conventionally accepted concepts used to describe psychopathology
Generally called classifications
DSM-5 and ICD-10 are examples
Classification
The activity of forming groups
Diagnosis
the process by which individuals are assigned to already existing groups
Fundamental Problems of Psychiatric Classification
nature of entities being classified
definition of what a mental disorder is
nosological principles for organizing psychiatric classification (whats the best way to classify disorders?)
distinction between normality and pathology
validity of many diagnoses
Purposes of Classification
defines boundaries
defines the filed of psychopathology
provides nomenclature for practitioners
psychologists can “talk to each other”
provides short-hand
serves a basis for organizing and retrieving information
describes the common patterns of symptom presentation
provides a basis for making predictions
clinical course
response to treatment
forms the basis for the development of theories
theories of relationship between diagnoses can be helpful
Taxonomic Issues
Classification of syndromes, disorders, or diseases
Classification of disorders versus classification of individuals
Definition of Mental Disorder
Dimensions versus categories
DSM as atheoretical
Symptoms vs Showing Signs vs Syndorme
self-reported issues —> symptoms
issues observed by others —> signs
signs & symptoms co-occurring frequently —> syndrome (only descriptive)
Disorder
a pattern of symptoms and signs that includes an implied impact on the functioning of an individual
The term is more descriptive than syndrome
some causal factors might be understood
Etiology is still unclear and/or multiply determined
Disease
a condition with a known etiology & known path from the causal agent to the symptoms and signs
Categorical Classification
Advantages
Easy to use because they are more “black and white”
Consistent with biological and medical classification systems
Disadvantages
results in the loss of some information
some boundaries are arbitrary or ill-defined
Diagnostic Overlap = Comorbidity
Of those in the general population who meet criteria for a disorder, ½ meet criteria for two or more other disorders
About 95% of patients meeting criteria for borderline personality disorder meet criteria for another personality disorder
David Hume
“experience” can generate knowledge
How we perceive causality will be based on temporality and contiguity
We a naturally inclined to attribute the experience of constant contiguity to causality
John Stuart Mill: Five Methods of Induction
Direct Method of Agreement
If something is a necessary cause, it must always be present when we observe the effect
Method of Difference
the one aspect two identical situations do not have in common is likely to be the cause of the effect
Combination of the methods of agreement & difference
Method of Residue
remaining condition must cause remaining outcome if every other condition is matched to an outcome
Method of Concomitant Variation
if one property of a phenomenon varies in tandem with some property of the circumstance of interest, then that property most likely causes the circumstance
Austin Bradford Hill - Nine Criteria for Causal Inference
Strength – the larger the association, the more likely it is causal
Consistency – consistent observations of suspected cause and effect in various times and places raise the likelihood of causality
Specificity – the proposed cause results in a specific effect in a specific population
Temporality –the cause precedes the effect in time
Biological gradient – greater exposure to the cause leads to greater effect
Plausibility – the relationship between cause and effect is biologically and scientifically plausible
Coherence – epidemiological observation and laboratory findings confirm each other
Experiment – when possible, experimental manipulation can establish cause and effect
Analogy – cause-and-effect relationships have been established for similar phenomena
Karl Popper - Empirical Falsification
proving causality = wrong goal
induction should proceed not by proving, but by disproving
If it can be falsified, it might be true —> it is impossible to disprove
Goal of scientific experimentation: try to disprove a hypothesis by a process that resembles experience or empirical observation
Scientific Findings:
always a matter of rejecting the null hypothesis
never a matter of accepting the alternative hypothesis
Scientists hesitant to make declarative statements
Counterfactual Condition
refers to what would have happened in a different world
Unfortunately, it is impossible to observe — BUT! we can approximate it using scientific methodologies like random designs, replication, etc.
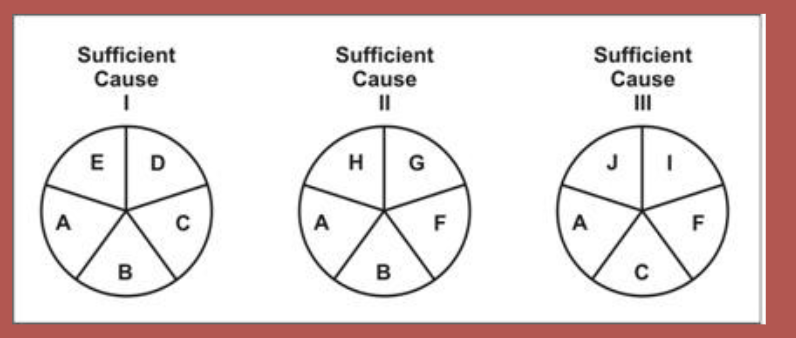
Ken Rothman — Sufficient Component Cause Model & “Causal Pies”
component causes — individual factors that contribute to a disease
Shown as individual “slices” of the pie —> disease can only occur if all slices of pie are present / when the pie is complete
sufficient cause —> the complete pie
Disease may have more than one sufficient cause
In image, component causes B and C: either one, the other, or both can contribute to the disease, but not a necessary cause
necessary cause —> a component causes that appears in every pie or pathway (without it, the disease doesn’t occur)
in image, component cause A is necessary because it exists within each pie (assuming the 3 pies are the only “casual pies”)
The presence of a third copy of chromosome 21 is a __________ cause of Down Syndrome (Sufficient Component Cause Model example)
necessary and sufficient
It’s all that is needed to cause Down Syndrome
One can’t have down syndrome without it
Alcohol consumption is a _____ cause of alcoholism (Sufficient Component Cause Model example)
necessary, but not sufficient
In order to be classified as an alcoholic, one must drink alcohol
Drinking alcohol, but itself, is not enough to cause alcoholism
Exposure to high doses of ionizing radiation is __________ cause of sterility in men (Sufficient Component Cause Model example)
a sufficient, but not necessary
This factor can cause sterility on it own
It is not the only cause of sterility and sterility can exist without it
A sedentary lifestyle is ________ to cause coronary heart disease (Sufficient Component Cause Model example)
neither sufficient nor necessary
A sedentary lifestyle on its own will not cause heart disease
Heart disease can certainly occur in the absence of a sedentary lifestyle
Smoking is ________ cause of lung cancer (Sufficient Component Cause Model example)
neither a necessary nor sufficient
People who smoke may not develop lung cancer
People who do not smoke may develop lung cancer
This does not mean that smoking is not a cause of lung cancer
Paul Meehl — Specific Etiology
a categorical (all-or-none) variable that is both necessary and sufficient for a disorder to emerge
ex: Huntington’s disease —> single dominant gene is both necessary and sufficient to produce the disease
RARE in psychopathology
Paul Meehl: Causes
Threshold Effect
A dimensional variable
When the threshold is exceeded, the individual is at risk for the disorder
Below the threshold, there is no risk for the disorder
Step Function
A dimensional variable
The individual’s risk for the disorder increases sharply once past the threshold
The individual's risk for the disorder is low below the threshold, but not zero
Diathesis-Stress
variables are necessary, but not sufficient for a disorder
elevated levels of certain variables create a diathesis (vulnerability)
both vulnerability factors and stressors are necessary for a disorder to emerge —> neither is sufficient
** a causal factor can also be neither necessary nor sufficient for psychopathology
Case Study
the detailed examination of a single individual
Good for the context of discovery —> Hypothesis generation
can function as existence proofs by negating a general proposition
Poor for the context of justification —> hypothesis testing; lack the controls found in systematic research; impossible to generalize findings
can never justify a generalization
Experimental Designs
when researchers randomly assign participants to one of two conditions
Experimental group – received the experimental manipulation
Control group – does not receive the experimental manipulation
**rarely possible to randomly assign conditions in psychopathology research —> even so, super unethical!
Quasi-experimental design
a comparison of two or more groups defined by pre-existing characteristics (e.g., depressed vs. non-depressed individuals)
“Mother Nature” has already assigned these groups
technically correlational studies
**Should not draw causal inferences from quasi-experimental studies —> confounding variables
Matching (Quasi-Experimental Design)
equating the quasi-experimental groups on potentially confounding variables
Difficulties:
confounding variable we haven’t thought of
rests on causal assumptions that may be incorrect
____ on a variable can create additional systematic differences
Analogue Experiment
an attempt to produce variants of psychopathology in either humans or animals
Two Pitfalls:
assumption that the analogue provides an adequate model of the condition
May be unethically unacceptable or impractical to create symptoms
Animal Models of Psychopathology
Involves attempts to produce a simulated form of a mental disorder in non-human —> (ex: learned helplessness)
Pitfalls:
Researchers must be cautious in generalizing findings to humans
Using animals does not sidestep ethical issues
Challenge Paradigm
when researchers present participants with stimuli thought to trigger a pathological response
Pitfall: ethical concerns
Single-Subject Experimental Designs
each subject serves as his or her own control
ABA or Reversal design —> research measure baseline behavior, then after introducing intervention, then again after withdrawing the intervention
Pitfalls: some interventions can’t be withdrawn / reversed
Epidemiology
study of distribution of disorders in a given population & the variables associated with this distribution
research on rate of a disorder can provide a baseline comparison
characteristics covarying with the frequency of a disorder can provide clues to etiology
Behavior Genetics
the study of genetic and environmental influences on behavior
Biological parents contribute genetic influences, environmental influences, and interaction between genetic and environmental influences to their offspring
These can’t be distinguished using family studies
Adoption and twin studies can determine their specific effects