CH 32 section 2
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
PNF
-based on normal movement and motor development
-addresses posture, mobility, strength, effort, and coordination
-mass movement patterns are spiral and diagonal
PNF facilitation methods
-multisensory to facilitate movement
-use of manual contacts, verbal commands, visual cues
-sensory stimulation supports motor response
Auditory system
-verbal commands should be brief and clear
-timing of the command must match the motor act
-tone of voice influences response
-verbal mediation can improve sequencing and retention of safety routines
Visual system
-visual stimuli assist initiation and coordination of movement
-monitor that the client tracks in the direction of movement
-therapist positioning provides visual cues
-placement of activities can facilitate rotation and alignment
-diagonal patterns can reinforce oculomotor control and eye teaming
Tactile system
-matures before auditory and visual
-touch provides temporal and spatial discrimination
-client should feel coordinated and balanced movement patterns
-manual contacts guide and reinforce desired responses
Manual contacts
-tactile facilitation may include gentle guidance, stretch to initiate movement, and resistance to strengthen movement
-avoid stretch or resistance with musculoskeletal instability or early fracture healing
Stepwise procedures
emphasize difficult parts during performance of the whole task, then fade as skill improves
Part task practice
targets components the client can not perform independently
Whole task practice
integrates components into the full functional task
Sequence of PNF assessment
-proximal to distal
-begin with vital and related functions: breathing, swallowing, voice, facial/oral musculature, visual ocular control
-fatigues and endurance are evaluated during functional activity
Head and neck assesment
-assessed after vital functions
-deficits directly affects trunk and UE
-observed across postures, total patterns, and functional activities
-key observations: tone dominance, alignment, stability vs mobility needs
Upper trunk assessment
-observe: postural control, symmetry, and endurance
-supports reaching and manipulation
UE assessment
-observe: quality, coordination, synergy dominance
-impacts ADL and IADL
Lower trunk assessment
-observe: stability, weight shifting, and alignment
-affects transfers and mobility
LE assessment
-observe: movement quality, balance, and tone
-influences gait and functional mobility
Developmental postures assessment
-observe: ability to assume and maintain postures
-guides task grading and positioning
Diagonal patterns
-PNF uses mass movement patterns observed in functional activities
-patterns are spiral and diagonal, NOT isolated joint motions
-each body region has two diagonal motions with flex/ext
-diagonal patterns combine flex/ext, rotation, and movement toward or away from midline
Head, neck, and trunk proximal diagonal patterns
-flexion with rotation to the right or left
-extension with rotation to the right or left
Extremity diagonal patterns D1 & D2
-upper and lower extremity diagonals described by movements at shoulder and hip
-components include flex/ext, ab/adduction, and rotation
-D1 and D2 include flex/ext
-reference point for UE is shoulder
-reference point for LE is hip
diagonal one
-D1 extension begins in the shortened range of D1 flexion with hand closed toward radial side
-D1 extension leads with hand opening toward the ulnar side
-eyes follow hand of leading arm so that the head and hand cross midline
-elbows may be straight, flexed, or extended
(Starting with a fist near your opposite shoulder, then opening your hand and reaching out while looking at it)
diagonal two
-D2 flexion begins in the shortened range of D2 extension with hand closed toward the ulnar side
-D2 flexion leads with hand opening toward radial side
-all diagonal patterns, head to foot, cross midline when performed through full range
(ex. grabbing a seatbelt from your side and pulling it up and across your body while opening your hand)
Describe pattern used to comb hair
UPPER EXTREMITY D1 FLEXION PATTERN USED TO COMB THE HAIR, OPPOSITE SIDE
Symmetric patterns
-both extremities move similarly at the same time
-facilitate trunk flexion or extension
Asymmetric patterns
-extremities move towards one side simultaneously
-facilitate trunk rotation and increased control

Using both hands to put on an earring is an example of
asymmetric pattern
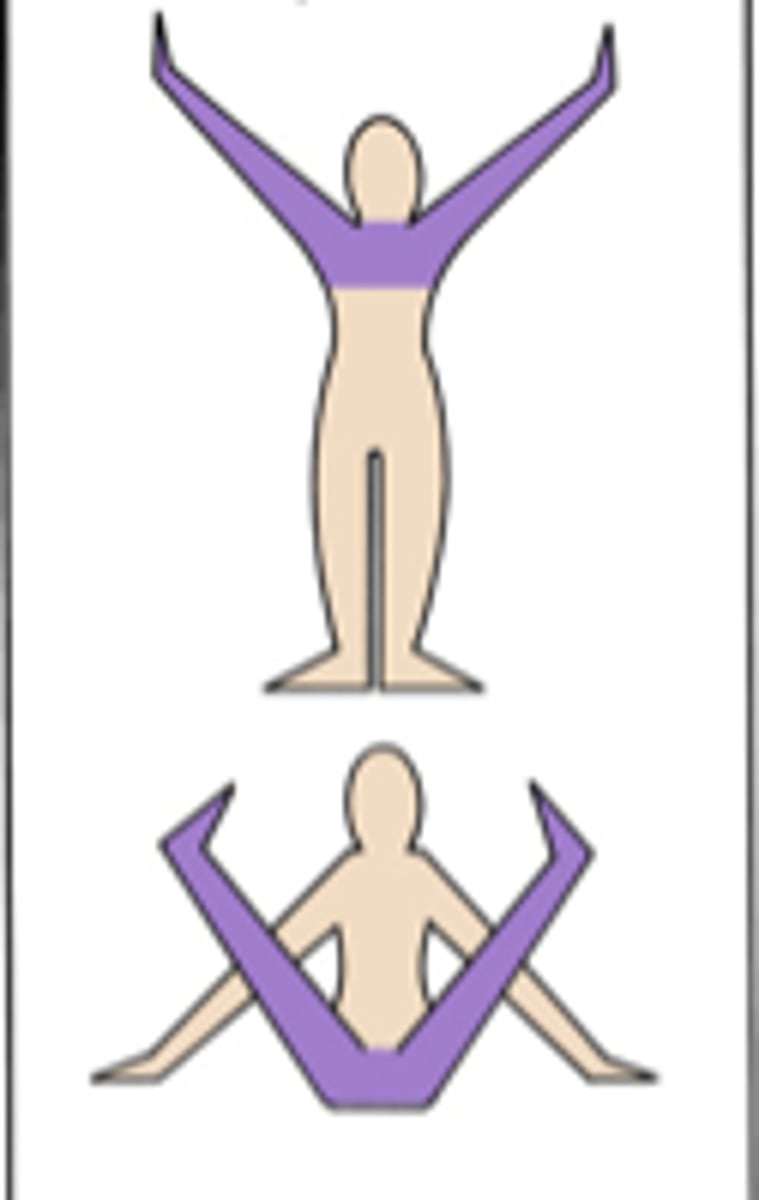
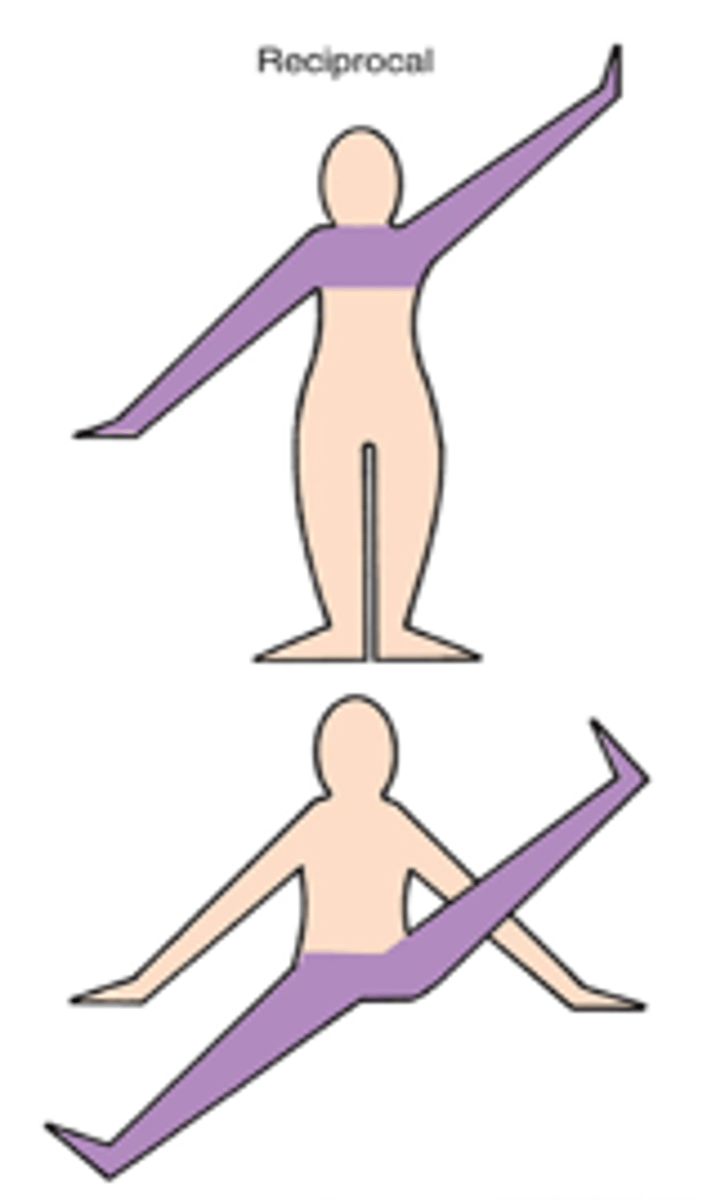
Reciprocal bilateral patterns
-extremities move in opposite directions simultaneously
-combined diagonal reciprocals stabilize head, neck, and trunk same diagonal reciprocals facilitate trunk rotation
-observed in walking, swimming, and higher level balance tasks
Ipsilateral patterns
same side extremities move together

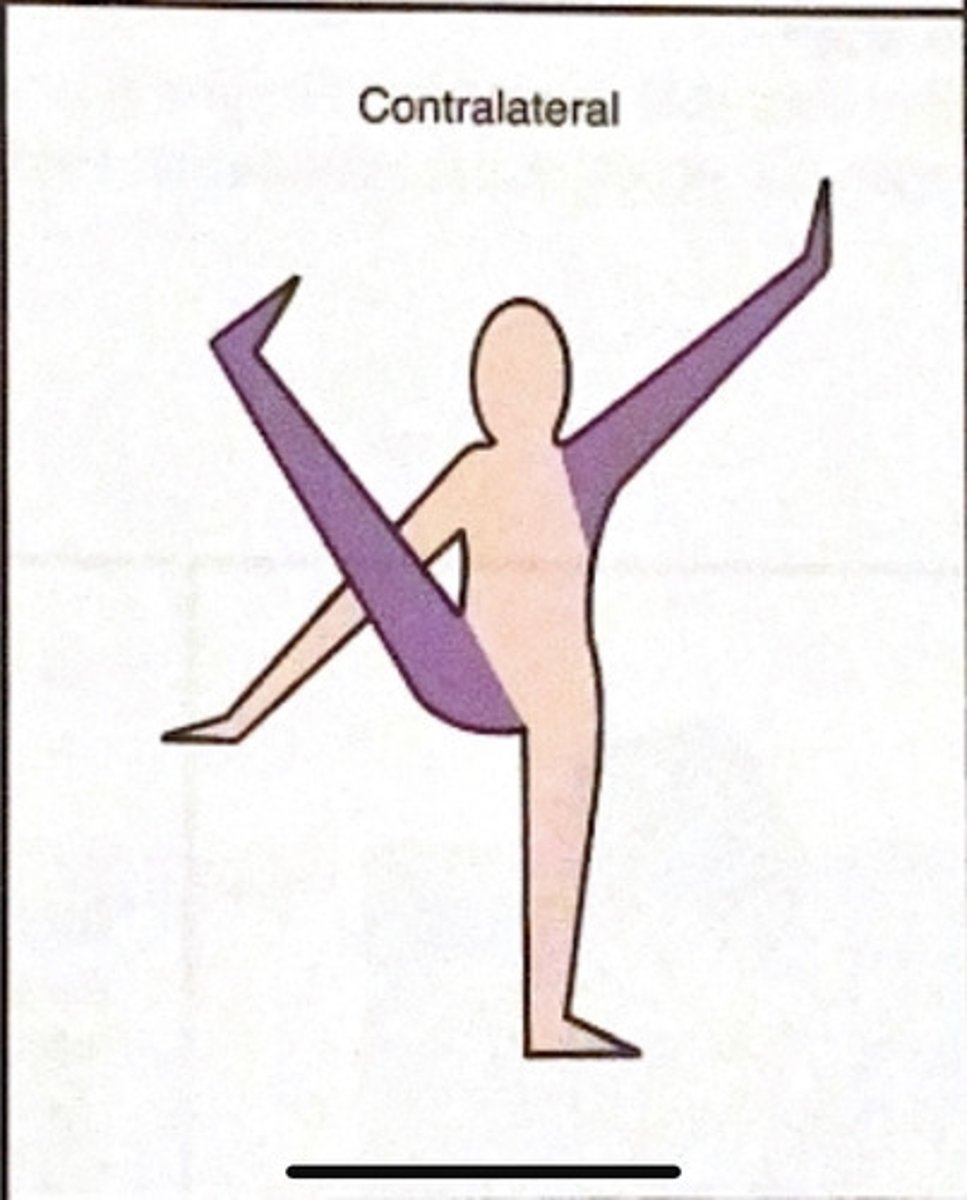
Contralateral patterns
opposite side extremities move together
Total patterns
-integrate head, neck, trunk, and extremities
-include assumption and maintenance of postures
-enhance postural control, balance, and coordination
-support reflex integration and antagonist balance
Manual contacts
-placement of therapists hand on client
-most effective when applied directly to the skin
-provide sensory cue and guide direction of movement
Stretch as a facilitation technique
-used to initiate voluntary movement
-enhances speed and strength in weak muscles
-based on reciprocal innervation
-excites agonist and inhibits antagonist
Traction
-facilitates joint receptors via joint separation
-promotes movement and pulling actions
-used in functional tasks such as carrying or pulling
Approximation
-facilitates joint receptors via compression
-promotes stability and postural control
-typically applied in weight bearing postures
Maximal resistance
-based on irradiation
-allows smooth movement
-elicits max effort from client
Techniques directed to the agonist: repeated contractions
-promote motor learning, strength, ROM, and endurance
-voluntary movement facilitated with stretch and resistance
-uses isometric and isotonic contractions
-aka Contract-Relax
Repeated contractions: technique sequence
-active movement to point of weakness
-isometric contraction against resistance
-isotonic contraction with stretch
-repeated until fatigue or goal achieved
Rhythmic initiation: effects
-enhances proprioceptive kinesthetic input
-resistance added as control improves
-reduces muscle stiffness in chronic stroke
-improves functional movement efficiency
Slow reversal
-Isotonic contraction of antagonist followed by agonist
- Resistance applied through full available range
- Enhances coordination and strength
- Example: D1 extension → D1 flexion for oral hygiene reach
- Power of agonist should build with repetitions
Rhythmic stabilization
- Simultaneous isometric contractions of antagonists
- Promotes co-contraction and postural stability
- Manual contacts applied to both agonist and antagonist
- Limit repetitions to avoid fatigue or breath holding
- Contraindicated with certain cardiac conditions
Contract-Relax
- Passive movement to point of limitation
- Isotonic contraction of antagonist against resistance
- Followed by relaxation and increased passive range
- Used when no active agonist movement is present
Hold-Relax
- Isometric contraction of antagonist
- Relaxation followed by active movement into agonist pattern
- Static contraction held ~3 seconds
- Useful in presence of pain or acute orthopedic conditions
Slow reversal hold-relax
- Isotonic contraction → isometric hold → relaxation
- Followed by active agonist movement
- Preferred when some active movement is present
- Improves functional ROM and control
Rhythmic rotation
- Slow passive rotation in both directions
- Used to decrease spasticity
- Increases available ROM
- Effective prior to dressing or splint fabrication