HIV/AIDS Pre Lecture
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
What type of virus is HIV?
HIV is a retrovirus, meaning it carries genetic material as RNA instead of DNA.
What are the two main types of HIV and how do they differ?
HIV-1: Most common worldwide.
HIV-2: More prevalent in Western Africa, progresses more slowly.
What is the structure of an HIV virion?
HIV has a viral core containing RNA, surrounded by a glycoprotein envelope (GP) that attaches to host cells.
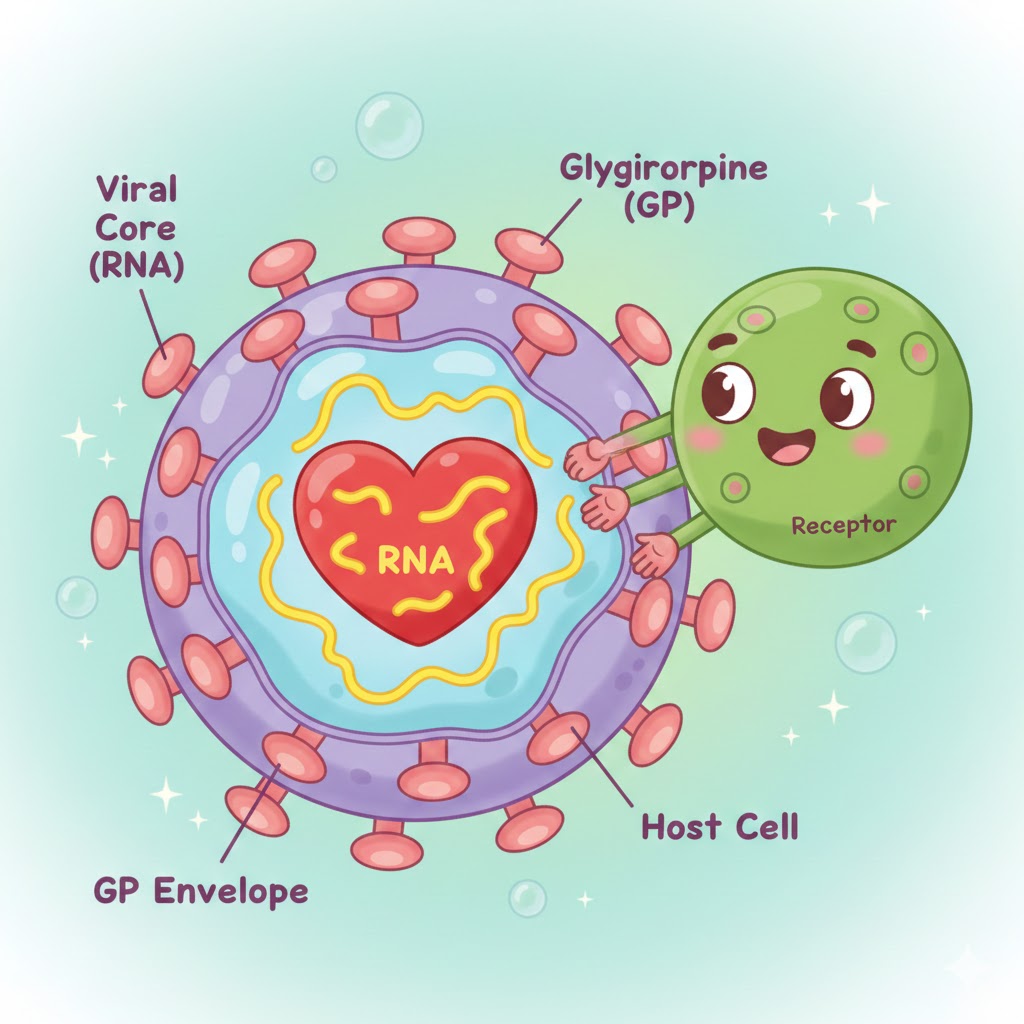
Which receptor does HIV primarily bind to on host cells?
CD4 receptor.
What are the coreceptors HIV uses to attach to host cells?
CCR5 and CXCR4.
Which immune cells are primary targets of HIV?
CD4+ T lymphocytes (Helper T Cells).
Besides T lymphocytes, which other cells have CD4 receptors and can be targeted by HIV?
Macrophages, monocytes, dendritic cells, and brain microglia.
How does HIV become a chronic disease?
It integrates into the host’s immune cells, allowing it to persist long-term.
What topics are typically covered in an HIV pathophysiology lecture?
HIV lifecycle
Staging
Lab tests
Common opportunistic illnesses associated with AIDS
Why is it important to remember CCR5 and CXCR4 in pharmacology?
These coreceptors are targets for certain HIV medications, influencing treatment strategies.
How many main stages are in the HIV lifecycle?
Several stages: Binding/Attachment, Fusion, Reverse Transcription, Integration, Replication, Assembly, Budding.
Why is understanding the HIV lifecycle important for nursing practice?
Explains why HIV remains chronic and requires lifelong treatment
Shows how medications block replication
Helps understand how the virus destroys host cells and can remain latent
Why is developing a vaccine for HIV difficult?
HIV mutates rapidly during replication, changing its genetic material.
What happens during the binding/attachment stage of HIV?
HIV attaches to CD4 receptors and coreceptors (CCR5/CXCR4) on the host cell surface.
What occurs in the fusion stage?
The HIV envelope fuses with the CD4 cell membrane, allowing HIV to enter the host cell.
Why are binding and fusion important targets for medications?
Drugs like entry inhibitors block HIV from attaching to or entering the host cell.
What happens during reverse transcription?
HIV uses reverse transcriptase to convert single-stranded RNA into double-stranded DNA.
What occurs during integration?
HIV DNA is inserted into the host cell’s DNA by integrase, creating a permanent, lifelong infection.
Which medications target these stages?
Reverse transcriptase inhibitors (RTIs) block reverse transcription
Integrase inhibitors block integration of viral DNA into host DNA
What happens during replication?
HIV uses the host cell to produce viral RNA and polyproteins (long chains of HIV proteins) to build new viral components.
What occurs during assembly?
Viral RNA and proteins move to the host cell surface and assemble into immature, non-infectious HIV particles.
Why are these stages important for treatment?
Drugs that block replication or protein synthesis help prevent new virus formation.
What happens during budding?
Viral particles push out of the host cell, forming immature HIV particles.
How do HIV particles become mature and infectious?
The protease enzyme cuts polyprotein chains into functional proteins, creating mature, infectious viruses.
Which medications target this step?
Protease inhibitors prevent maturation of new viral particles.
How does HIV affect the immune system?
HIV entry and replication cause cell death, leading to serious impairment of the immune system.
Through which body fluids can HIV be transmitted?
Blood, semen, vaginal secretions, amniotic fluid, breast milk.
How is HIV transmitted person-to-person?
Sexual intercourse
Contaminated needles
Mucous membrane contact with infected blood or body fluids
Perinatally from mother to fetus (during pregnancy, birth, or breastfeeding)
Can HIV be spread through casual contact or fluids like saliva, tears, urine, or sweat?
No, HIV is not spread through casual contact or those fluids.
Why is HIV medication management challenging?
HIV frequently mutates, changing its genetic material and potentially affecting treatment effectiveness.
What happens to viral load and CD4 count as HIV progresses?
Viral load rises, and CD4 count falls as the infection progresses through stages.
When does Stage 1 of HIV infection typically occur?
Within 1 to 4 weeks after initial infection.
What symptoms might a person experience during acute HIV infection?
Nonspecific, flu-like symptoms such as fever and headache.
What happens to viral replication during this stage?
Rapid viral replication occurs, with HIV spreading throughout the body.
How does Stage 1 affect CD4 cells?
HIV targets and destroys CD4+ T cells, impairing the immune system.
How contagious is a person during this stage?
Highly contagious due to the high amount of virus in the blood.
When do antibodies appear, and are they effective?
Antibodies appear after 2–3 weeks, but they are largely ineffective at destroying HIV.
What does a positive antibody test indicate during Stage 1?
It indicates that HIV infection is established, not that the person is immune.
What is another name for Stage 2 of HIV infection?
Clinical latency, asymptomatic HIV, or chronic HIV.
How active is HIV during this stage?
HIV is still active but reproduces at lower levels than in Stage 1.
What symptoms are typically present in Stage 2?
Few or no symptoms; many people are asymptomatic.
How long can Stage 2 last?
Can last for 10 years or more, especially with effective antiretroviral treatment.
Can a person transmit HIV during Stage 2?
Yes, even with low-level viral replication, HIV can still be transmitted.
When is Stage 3 of HIV infection diagnosed?
When CD4 count drops below 200 cells/mm³ or when opportunistic illnesses develop.
What is another name for Stage 3 of HIV infection?
Acquired Immunodeficiency Syndrome (AIDS).
How is the immune system affected in Stage 3?
The immune system is substantially damaged, leaving the person highly susceptible to infections.
What are opportunistic illnesses?
Infections or diseases that occur more frequently or severely because the immune system is weakened by HIV.
What is the CD4 count used for in HIV management?
It is a major lab indicator of immune function.
What is the normal CD4 count?
500–1400 cells/mm³ (variations exist).
At what CD4 count is AIDS diagnosed?
When CD4 count drops below 200 cells/mm³.
What does a Nucleic Acid Test (NAT) measure?
The amount of virus (viral load) in the blood.
How does NAT compare to antibody tests?
NAT can detect HIV sooner than antibody tests.
What does an Antigen/Antibody Test detect?
Both HIV antigens (parts of the virus) and antibodies produced by the body.
What are the two main types of HIV Antibody Tests?
EIA: Enzyme Immunoassay
ELISA: Enzyme-Linked Immunosorbent Assay
What is Pneumocystis Pneumonia (PCP)?
Most common life-threatening lung infection in people with severe immunosuppression from AIDS, caused by Pneumocystis jiroveci.
What are the clinical manifestations of PCP?
Nonproductive cough (mucus too thick to cough up)
Shortness of breath (SOB), dyspnea
Fever and chills
Respiratory failure if untreated
How is PCP diagnosed?
Sputum culture to identify the organism.
Why is PCP particularly dangerous in AIDS patients?
Severe immunosuppression makes the infection life-threatening and can lead to respiratory failure if untreated.
What causes Cryptococcus meningitis?
The fungus Cryptococcus neoformans, often affecting severely immunocompromised patients.
How can people become infected with Cryptococcus neoformans?
By inhaling fungal spores.
What are the clinical manifestations of Cryptococcus meningitis?
Fever
Headache and stiff neck
Nausea and vomiting (N/V)
Mental status changes
Seizures
How is Cryptococcus meningitis diagnosed?
Cerebrospinal fluid (CSF) analysis.
Why is Cryptococcus meningitis particularly severe in HIV/AIDS patients?
Severe immunosuppression allows the fungus to invade the CNS, causing life-threatening meningitis.
How common is candidiasis in patients with AIDS?
It occurs in almost all patients with AIDS and is very common in immunocompromised individuals.
What is the most common presentation of oral candidiasis?
White patches on the oral mucosa—cheeks, palate, throat, or tongue
Can candidiasis spread beyond the mouth?
Yes, it can progress to the esophagus and stomach.
Are the white patches in oral candidiasis usually painful?
They are often painless.
What type of cancer is Kaposi’s sarcoma?
Cancer of the endothelial layer of blood and lymphatic vessels.
What are the clinical manifestations of Kaposi’s sarcoma on the skin?
Localized cutaneous lesions
Color: brownish-pink to deep purple
Lesions can be flat or raised
Often surrounded by ecchymosis (bruising) and edema (swelling)
Can Kaposi’s sarcoma affect other organs?
Yes, it can affect multiple organs including lymph nodes, GI tract, and lungs.
How is Kaposi’s sarcoma diagnosed?
Biopsy of the lesion.
Why is Kaposi’s sarcoma significant in AIDS patients?
It is an opportunistic cancer that occurs due to severe immunosuppression.
What is HIV encephalopathy?
A condition caused by HIV infection in the brain, leading to progressive cognitive, behavioral, and motor decline.
Where is HIV present in this condition?
In the brain and cerebrospinal fluid (CSF).
What causes cellular dysfunction in HIV encephalopathy?
What causes cellular dysfunction in HIV encephalopathy?
What are the clinical manifestations of HIV encephalopathy?
Memory deficits
Difficulty concentrating, confusion
Ataxia (uncoordinated movement)
Delay in verbal responses
Psychosis or hallucinations
Seizures
How is HIV encephalopathy diagnosed?
CT scan, MRI, or CSF analysis to detect HIV in the CNS.
Why is HIV encephalopathy significant in AIDS patients?
It represents CNS involvement and shows progressive neurological deterioration due to severe immunosuppression.