Retinal And Other Disorders
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
16 Terms
coloboma
•Failure of closure of fetal fissure in development
•
•Typically inferonasal in position
•May be associated with microphthalmia
•Autosomal dominant
Optic Nerve Hypoplasia Septo-optic dysplasia
Optic Disc Abnormalities
Retinal Pigment Epithelium
Congenital Infections -TORCHES
Maternal infection during pregnancy may have significant consequences to the developing fetus.
Toxoplasmosis
Other
Rubella
CytoMegaloVirus
HErpes virus
Syphilis
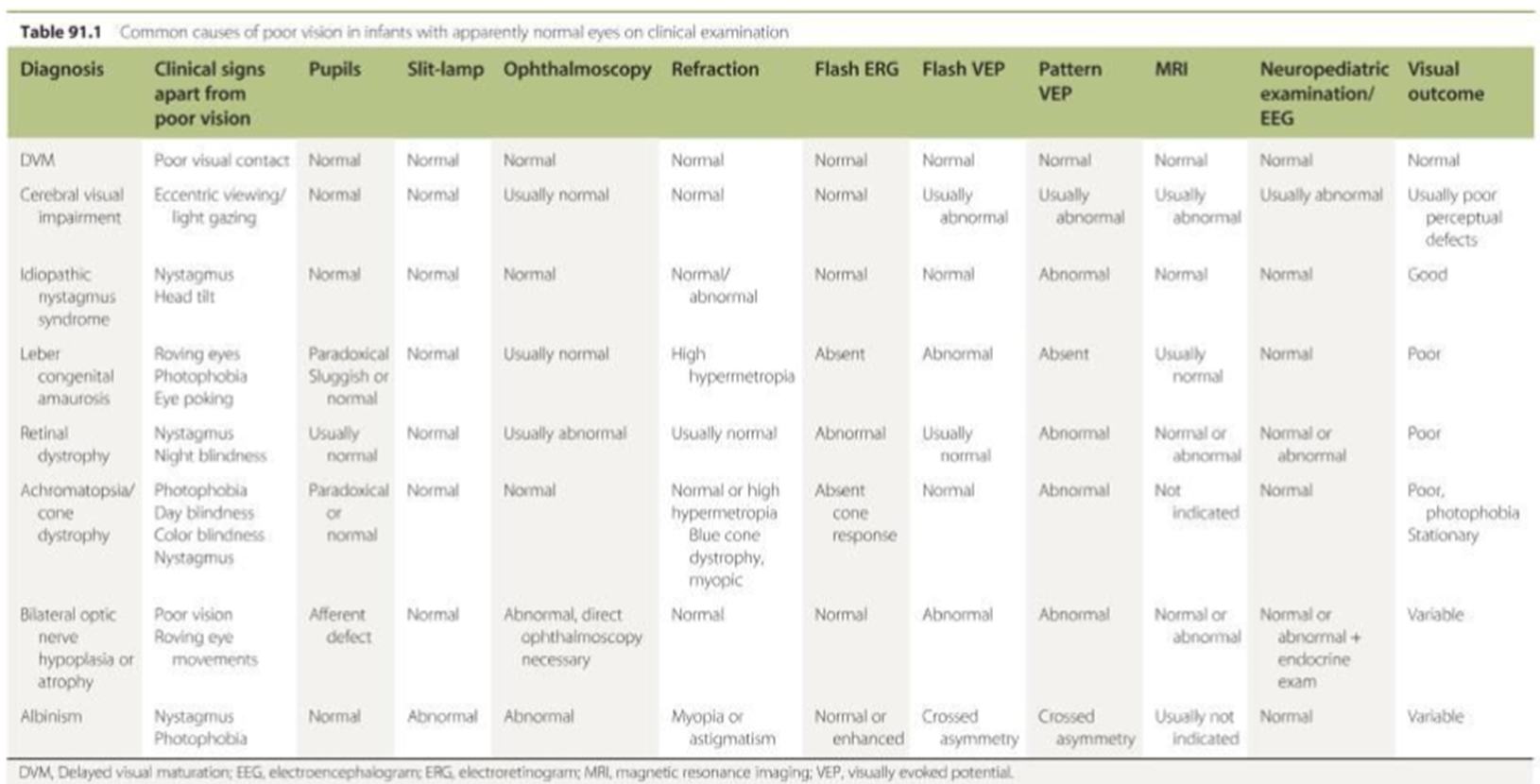
Photoreceptor Disorders
Congenital Stationary Night Blindness
Achromatopsia
Lebers Congenital Amaurosis
Retinitis Pigmentosa
Cone Dystrophy
These can be split into
•Stationary Conditions
•Affecting Rods primarily
•Affecting Cones primarily
•
•Progressive conditions
•Affecting Rods primarily
•Affecting Cones primarily
Congenital stationary night-blindness (rods)
None progressive
Variable vision
Normal looking retina
Moderate myopia
Nystagmus
Strabismus
Variable inheritance
Leber’s Congenital Amaurosis
Roving eye movements
Poor pupil response
Very poor vision
Initially normal looking retina
ERG is undetectable
Multiple gene’s
Gene therapy using viral vector – RPE 65 has had proof of concept and trials are underway.
Retinitis Pigmentosa
Predominantly rod dysfunction
Diverse range of inheritance
50% with no family history
Usually isolated but may have associations with other conditions
e.g. hearing loss – Ushers Sydrome
cardiac disease – Kearns Sayre
Often initially asymptomatic, but progressive
Peripheral visual field loss
Night blindness
Cataract
Macular oedema
Progressive Cone Dystrophy
Usually presents later that the stationary disorders
Photophobia
Nystagmus
Progressive loss of vision
Central scotoma (compare with optic neuropathies)
May have a ‘bulls eye’ macular appearance
Principally cone dysfunction as on ERG
Diverse range of inheritance
Retinal Pigment Epithelium Disorders
Stargardts - Autosomal recessive (ABCA4)
Initially presents with central visual loss in teen age years with an abnormal looking macular. Then develop white flecks at the level of the RPE and macular atrophy.
Flash ERG may be normal
mfERG is usually abnormal
Bests Disease - Autosomal Dominant (BEST1)
ERG is often normal
EOG is abnormal with an absent ‘light rise’
Vision is often good even with a typical vitelliform lesion (stage 2)
Vision declines beyond stage 2
Albinism - ocular - x linked = foveal hypoplasia
Choroidal Dystrophies
Choroideremia - X Linked recessive (Xq21)
Progressive RPE atrophy
Early onset presenting in first decade
Night blindness
Progressive peripheral field loss
Very reduced ERG