Anemia and Cell Histology Vocabulary
1/96
Earn XP
Description and Tags
Vocabulary flashcards related to Anemia and Cell Histology
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
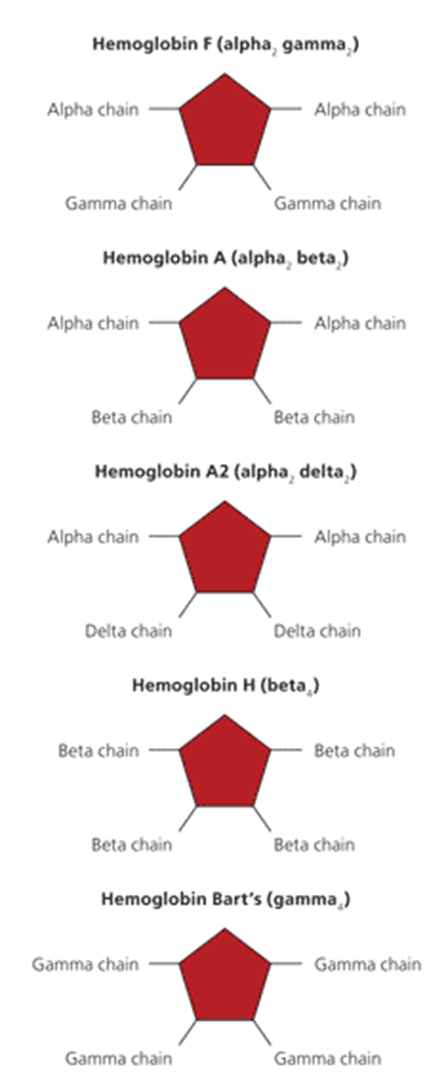
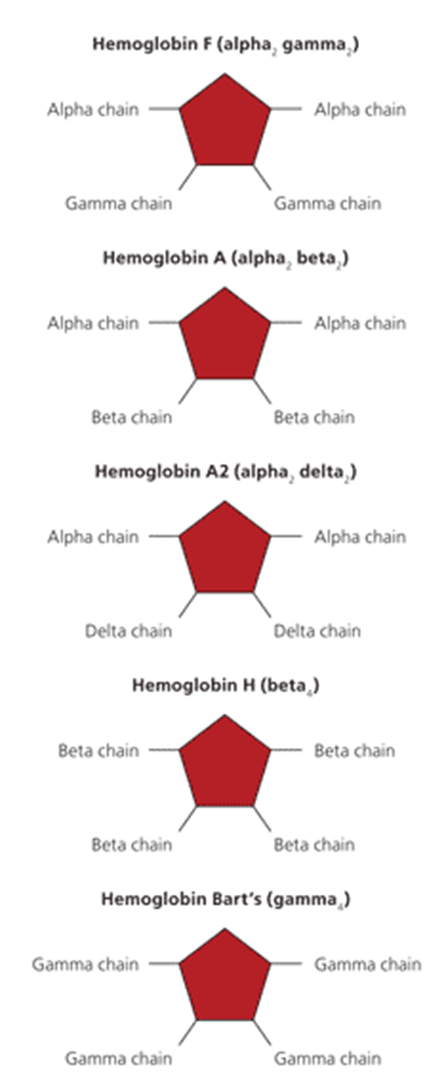
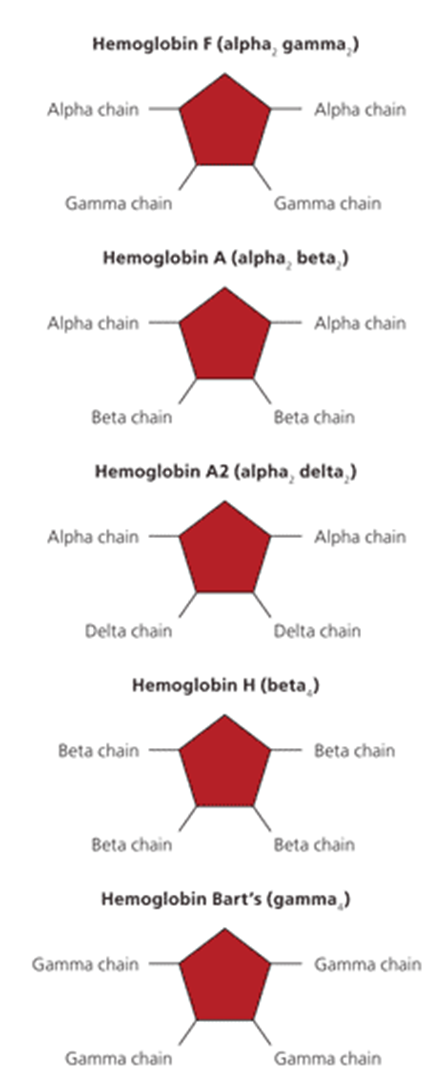
Hemoglobin A
Normal adult hemoglobin, consisting of 2 alpha chains and 2 beta chains, making up 98% of adult hemoglobin.
Hgb A2
Hemoglobin consisting of 2 alpha and 2 delta chains, making up 2% of adult hemoglobin.
Hgb F
Fetal hemoglobin, consisting of 2 alpha and 2 gamma chains.
present to 4-6 months of life.
allows transfer of O2 from maternal to fetal in utero
present in thalassemia major
Bohr Effect
The effect where O2 dissociates from hemoglobin more readily when the pH is lowered (acidic conditions).
increased O2 demand due to increased metabolism
increased metabolism → more CO2 → intracellular pH lowers resulting in enhanced oxygen release from hemoglobin, facilitating oxygen delivery to tissues.
Left Shift
Hgb-O2 affinity increases
lower co2
higher pH
low temp
Right Shift
Hgb-O2 affinity decreases
higher co2
lower pH
higher temp
acidosis
sickling can occur
EPO (erythropoietin)
Kidneys produce this to stimulate RBC production.
RBC
Life cycle of ~120 days; lack nucleus and mitochondria
Globin and Heme
Macrophages break down RBC into
Haptoglobin
Protein that binds to free hemoglobin, and then the complex is removed by RES.
hemolysis causes increased hemoglobin → more haptoglobin binding → decrease free haptoglobin levels
Ferroportin
Allows Fe export out of macrophages and into circulation.
Hepcidin
Blocks ferroportin so Fe stays within macrophage.
high wen iron stores are high and during inflammation
low during IDA
prevents iron from being used
Transferrin
Binds to and transports iron throughout circulation.
TIBC
Total Iron Binding Capacity – “how many seats are available on the bus” Indirect measurement of transferrin
% Saturated
How many seats are taken on the bus
UIBC
“How many seats are remaining on the bus” indirect measure of how many transferrin are not bound to iron
Anemia
Anemia: reduction of RBC, hemoglobin (hgb) or hematocrit (HCT)
MCV
Mean corpuscular volume – the size of the RBC
MCH
Mean corpuscular hemoglobin – average hemoglobin content (color of the RBC)
RDW
Red cell distribution width – variation in RBC size
Reticulocyte count
Immature RBCs - rate of RBC production
Normocytic
MCV 80-100
Microcytic
MCV <80
defect in cellular hemoglobin synthesis
mostly iron deficiency
thalassemia, sideroblastic
Macrocytic
MCV >100
asynchronous maturation of nuclear chromatin
rate of cell division is reduced
B12,folate, copper deficiency
myelodysplastic syndrome
HPLC (High performance liquid chromatography)
genetic newborn screening for common hemoglobinopathies
Thalassemia
Reduced Alpha chains – alpha thalassemia; in utero or at birth
Sickle Cell
Valine substituted for glutamic acid on beta chains; 4-6 months
Hemolysis
Breakdown of RBC – many causes including genetic, acquire, infectious
Intravascular
Within blood vessels
Extravascular
Within tissue. Typically RES (spleen) causing sequestration
Anisocytosis
Increase in RBC that vary in size
poikilocytosis
Increase in RBC that vary in shape.
Reticulocytosis
Increase in RBC production.
Band cell
Immature Neutrophil
hemoglobin structure
4 heme molecules & 4 iron
how many hemoglobin per RBC?
280 million
what hemoglobin is present in thalassemia?
A2
where do all cells come from?
pleuripotent cell
erythropoiesis fetal
liver, spleen, lymph nodes
erythropoiesis infant
bone marrow of all bones
erythropoiesis adult
ribs, sternum, vertebrae, pelvic bones
liver function in erythropoiesis
stores elements and synthesize proteins necessary for formation of RBC, EPO production, RBC breakdown
Cirrhosis/Hepatitis/Inflammation à decreased synthesis of proteins for RBC production, reduced storage ability or sequestered stores, decreased ability to process bilirubin
GI function in erythropoiesis
intrinsic factor, absorption of necessary components of RBC production: iron, vitamins, amino acids
gastric bypass à gastric cells that produced intrinsic factor do not encounter food à inability to absorb B12 à pernicious anemia
inflammatory disease à inability to adequately absorb nutrients à ineffective RBC production
lungs in erythropoiesis
oxygenation can influence EPO production
hypoxia stimulates epo and RBC production
lung disease (COPD, etc) hypoxic environment increased EPO and increased RBC
High RBC & High hematocrit = High viscosity and High risk for stroke
What does glucose oxidation capacity do?
allows ATP production
why are RBCs phagocytized by macrophages in the reticuloendothelial system
so they can fit through the small capillaries in the spleen
Iron + transferrin
transported to the liver for storage
biliverdin
oxidized and reduced to bilirubin by biliverden reductase
hemolytic anemia
bilirubin + albumin
transported to liver for conjugation
what happens to the spleen after it has been overworked
it dies
ferritin
protein that contains iron in organs, can store 4500 Fe atoms
primarily stored in the liver
why is ferroportin increased during IDA
to maximize iron absorption and mobilization
type A blood
a antigen
compatible with A & O
type B blood
B antigen
compatible with B, O blood
AB blood
A and B antigens
compatible with A, b, ab, and O blood (Universal recipient)
O blood
no antigens
only compatible with O blood (universal donor)
iron levels in thalassemia
generally fine but hemoglobin chains are abnormal
High MCV
B12 or folate deficiency
low MCV
iron deficiency or thalassemia
RDW in anemia
high variation in cell size
labs in IDA
Low MCV
Low Iron
high TIBC
Low ferritin
low Transferrin
liver synthesizes more transferrin = increase TIBC
labs in thalassemia
Low MCV
High Iron
Low TIBC
High Ferritin
High Transferrin
labs for anemia of chronic disease
normal to low MCV
low iron
low TIBC
normal to high ferritin
normal to low transferrin
liver synthesize less transferrin
what should you do first for anemia
history and physical
what should you do second for anemia
the work up
CMP
peripheral blood smear
iron panel
vitamin
what if a CBC confirms microcytic anemia
order iron
what if a cbc confirms macrocytic anemia
order b12

IDA

B12 deficiency

IDA

hemolysis
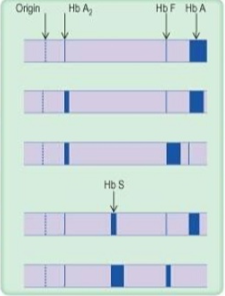
row 1
normal
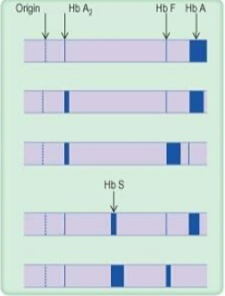
row 2
thalassemia trait
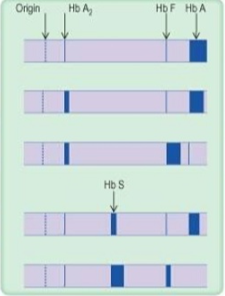
row 3
thalassemia major
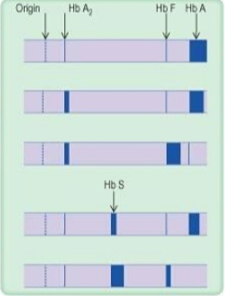
row 4
Sickle cell trait
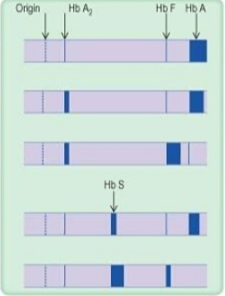
row 5
sickle cell anemia
what is IDA in older adults
colon cancer until proven otherwise
sideroblastic
Fe not incorporated normally
hgb S
valine substituted no beta chains
less soluble
Hgb C
lysine is substituted
Hgb D
glutamine is substituted
hgb H
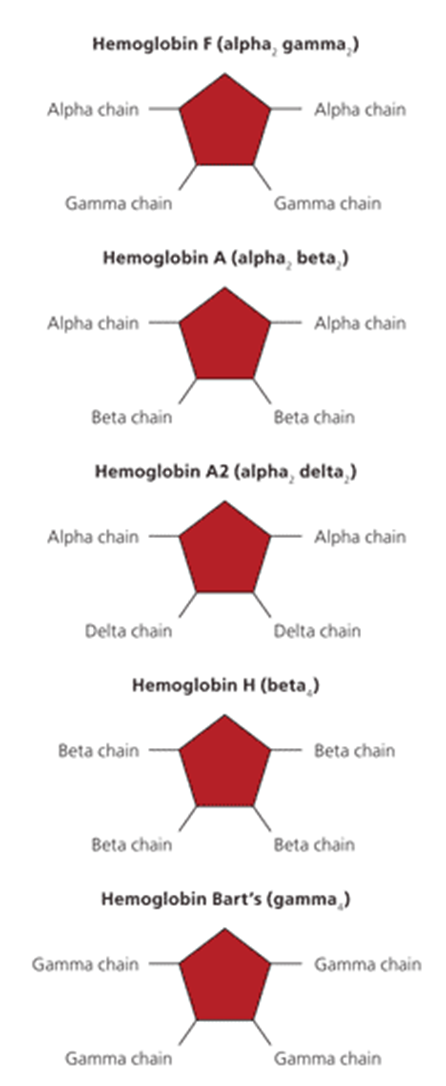
beta chain tetramers
alpha thalassemia type where 3-4 alpha chains are missing
what causes sickling
1. Exercise, etc → Increased O2 demand → localized or systemic effect
2. Infection → Incr. metab → anaerob metab → lactic acid in plasma
Plasma pH decreases → RBC’s unload O2 more readily → sickling
3. Fever → Increased metab → O2 unloads → sickling
Prolonged Fever/Infection → anaerobic metab → lactic acid → decr. pH → sickling
4.If the patient has another medical problem with acidosis risk – ie DM
when and what should SC patients be vaccinated
get more & more frequent vaccines
pneumococcus and meningococcus
effects of SC
renal failure
delayed puberty
skeletal abnormalities
functional asplenia
cholelithiasis (stones)
pulmonary HTN
hilar region
where vessels go to lung
dactylitis
vaso-occlusive crises that cause swelling in the hands and feet. repeated episodes of dactylitis will lead to a mottled appearance of the small bones
chronic osteomyelitis
happens in long bones
tibial infarctions
infection of infarcted bones
common organisms: salmonella species
frontal bossing
large and pronounced forehead
in any childhood anemia
sickle cell trait
heterozygous for HgB S
Hgb is still produced
rare sickling events
cells only sickle under severe hypoxic stress
adaptive for malaria
Thalassemia facial features
saddle nose
frontal bossing
maxillary expansion
A2 electophoresis
hgb F for beta thallassemia
consequences of hemolysis
Anemia → decreased O2 delivery →tissue ischemia
Anemia → decreased O2 delivery → increased cardiac demand
increased rbc synthesis→follate and Fe use→ deficiency
need for transfusions leading to fe overload
abnormal erythropoiesis
increase RBC production
howell jolly bodies
nuclear reminants not removed due to splenic dysfunction
functional asplenia
why could a patient have anemia and a normal reticulocyte count
ther is a problem with erythrocyte production
what effects size variation
MCV
what effects hemoglobin distribution
MCH
esr and rouleaux
high