20: edited from quizlet ryanef123 Endo 20 - Endo-Perio Lesions (Dr. Kai)
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
Define the following:
Endodontic/Periodontic Lesions are a process involving interaction of diseases of the pulp and periodontium
Endo-perio lesions
Define the following:
“The interrelationships between pulpal and periodontal disease primarily occur by way of the intimate anatomic and vascular connections between the pulp and the periodontium.” (Glickman and Iacono, Cohen’s Pathways of the Pulp)
Endo-perio lesions
In non-vital teeth with advanced periodontitis, describe the similar composition of the microbial flora of the root canals and periodontal pockets?
Obligate anaerobes (e.g. Streptococcus, Peptostreptococcus, Bacteroides, Fusobacterium, Eubacterium)
Fungi and viruses can be present in both the pulp and periodontium as well
shows the perio pocket may be possible source of root canal infections
Overlap in _______ suggests that the periodontal pocket may be a possible source of root canal infections
Bacterial colonizers
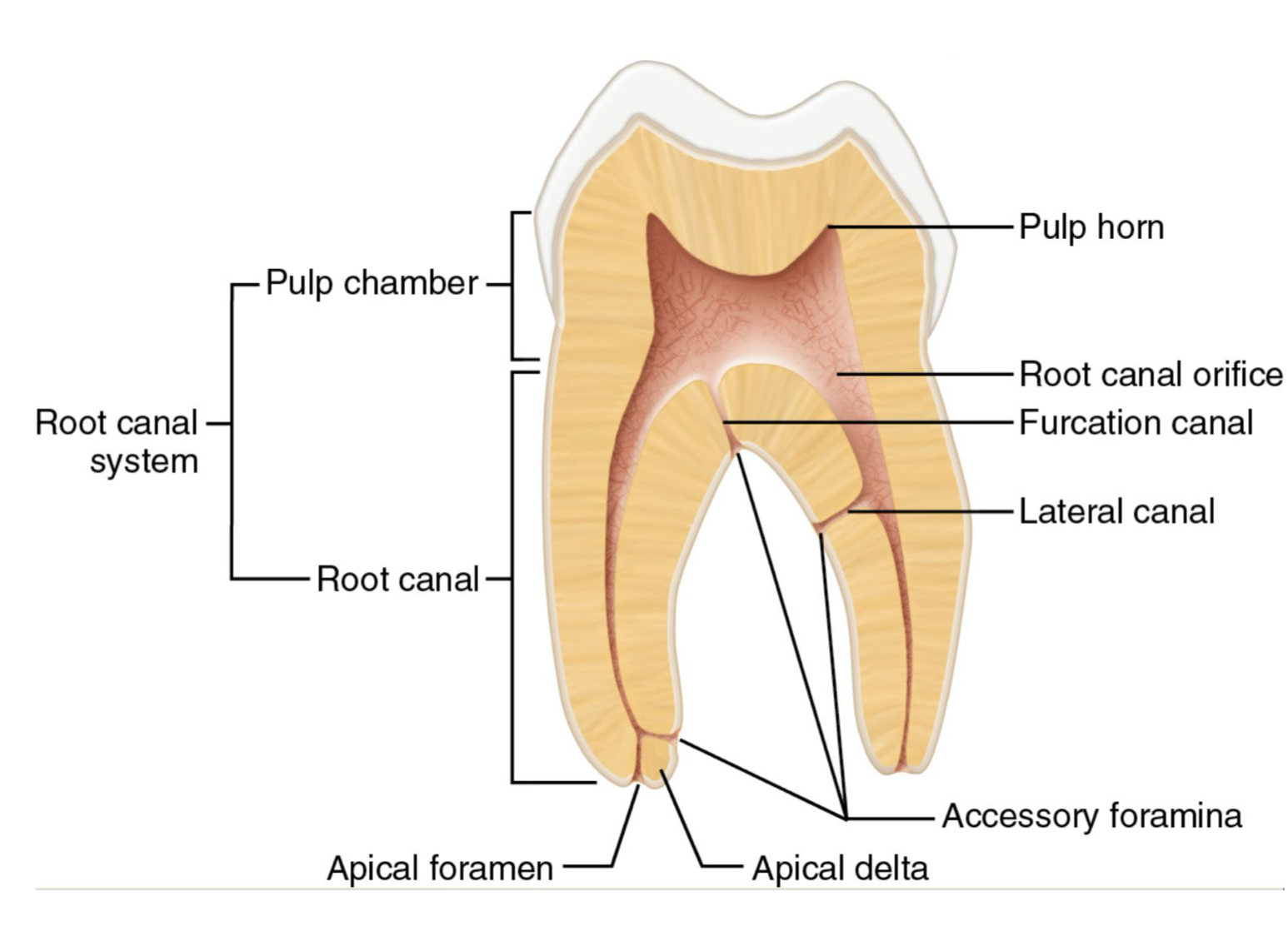
What are the three anatomical pathways of communication between the pulp and periodontium?
- Apical foramen and apical delta
- Lateral, furcation, and accessory canals
- Exposed dentinal tubules
What are two ways teeth can have exposed dentinal tubules?
- Aggressive SRP
- Gap between cementum and enamel at CEJ
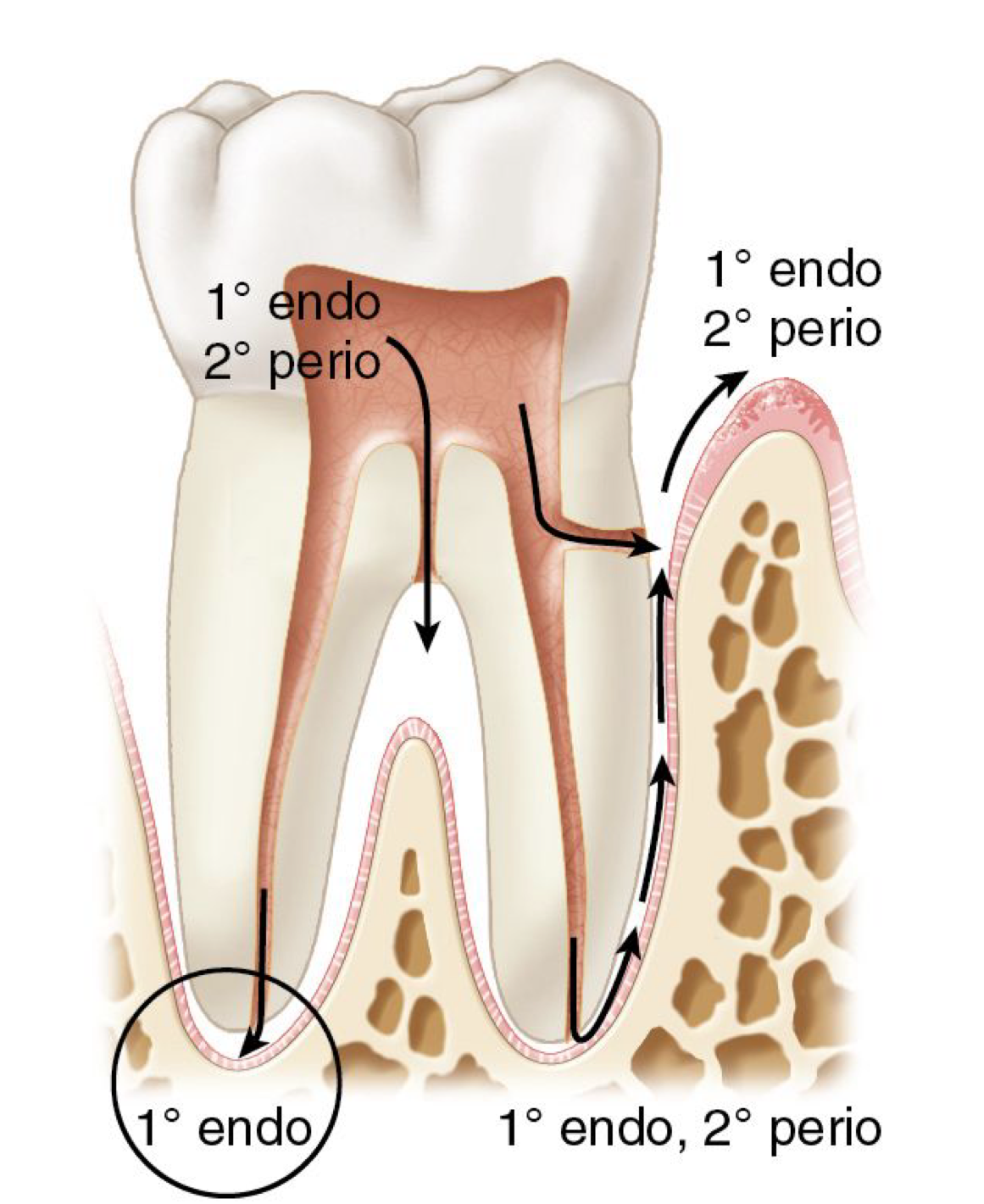
What type of lesion?
An endodontic problem originating from the pulp space, traveling through the apical foramen or accessory canals into the periodontium
Primary endo lesion
What are primary endo lesions caused by?
necrotic pulp (or reinfected previous endodontic treatment)
primary endo
What could present in the gingival sulcus with a narrow deep probing, infra-boney defect, furcation defect, or swelling of alveolar tissues in a primary endo lesion?
sinus tract (but only in apical location)
What is the pulpal diagnosis for primary endo lesions?
Necrosis (or Previously Treated)
What are the three periapical diagnoses for primary endo lesions?
- Symptomatic Apical Periodontitis
- Asymptomatic Apical Periodontitis
- Chronic Apical Abscess
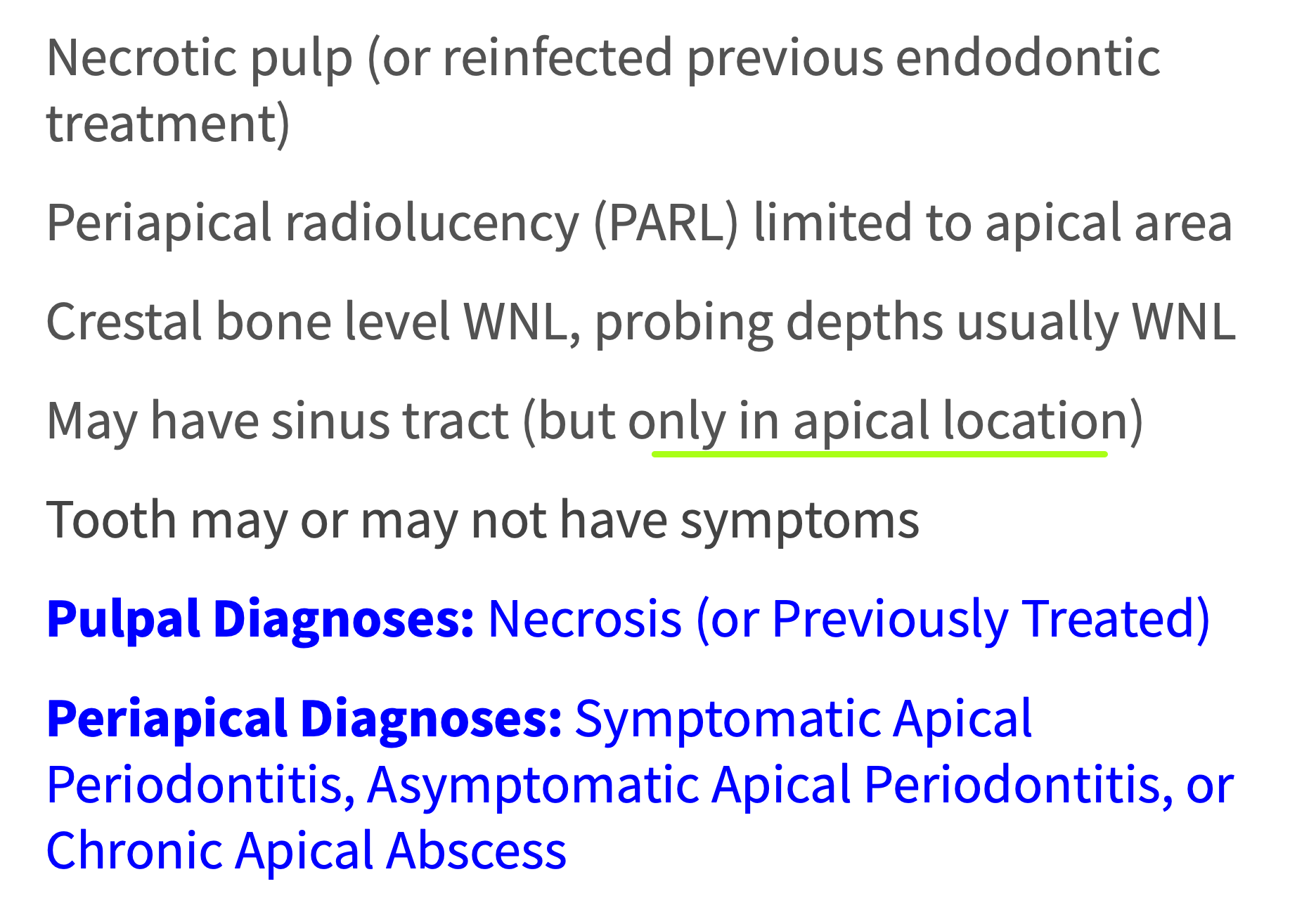
What type of lesion?
- PARL limited to apical area
- Crestal bone level and probing depths WNL
- Pulpal dx: necrotic pulp
- May have sinus tract (but only in apical location)
Primary endo lesion
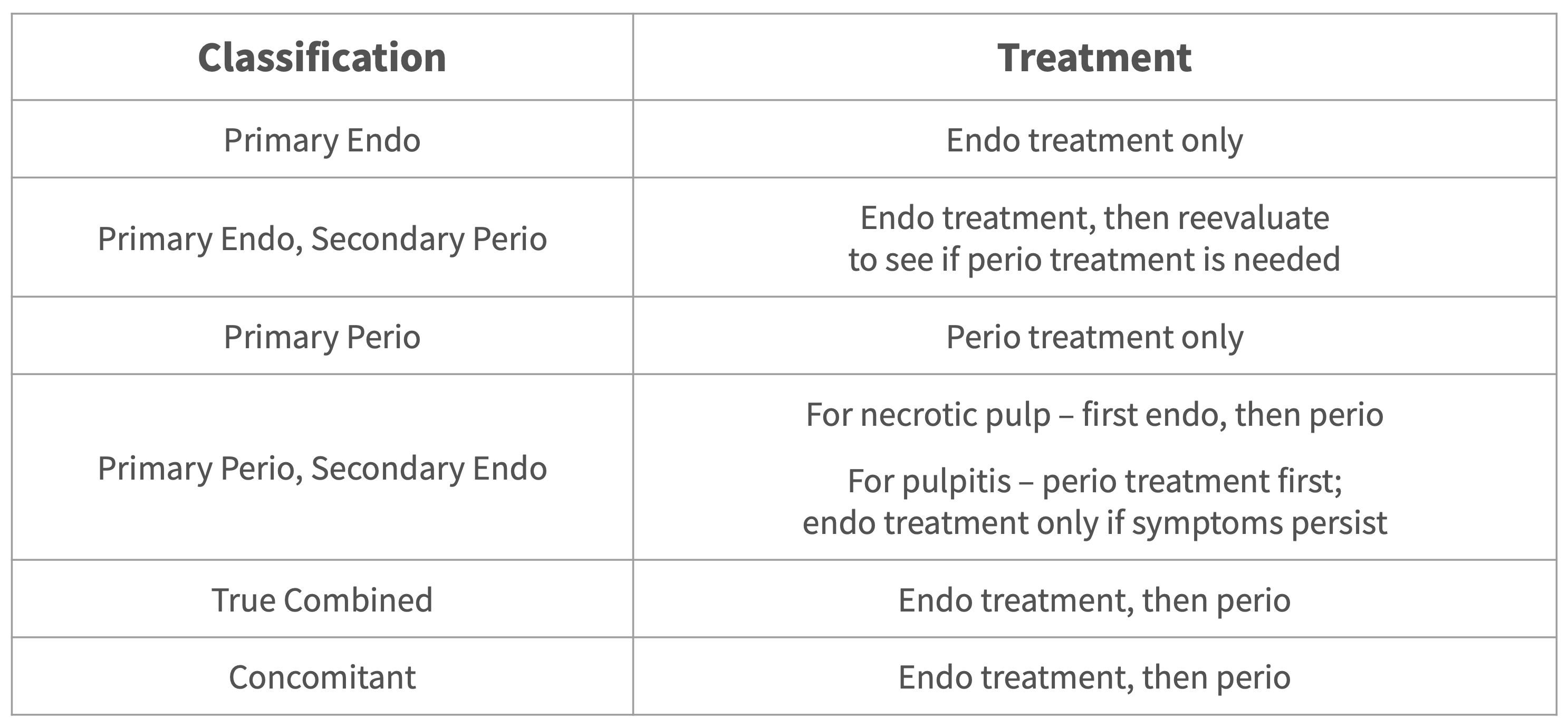
How do you treat a primary endo lesion?
non-surgical RCT only
What is the long-term treatment of a primary endo lesion after RCT?
- Full resolution of signs and symptoms is expected after RCT
- Any pockets should resolve without any further periodontal treatment
- Prognosis is dependent on endodontic treatment
What type of lesion?
Primary endo lesion
T/F: Primary endo lesions may give the impression that they are a primary perio lesion due to deep probing, furcation involvement, etc. however, the only way they are perio is because they pass through the PDL space
true
A sinus tract (primary endo lesion) follows the path of what?
least resistance
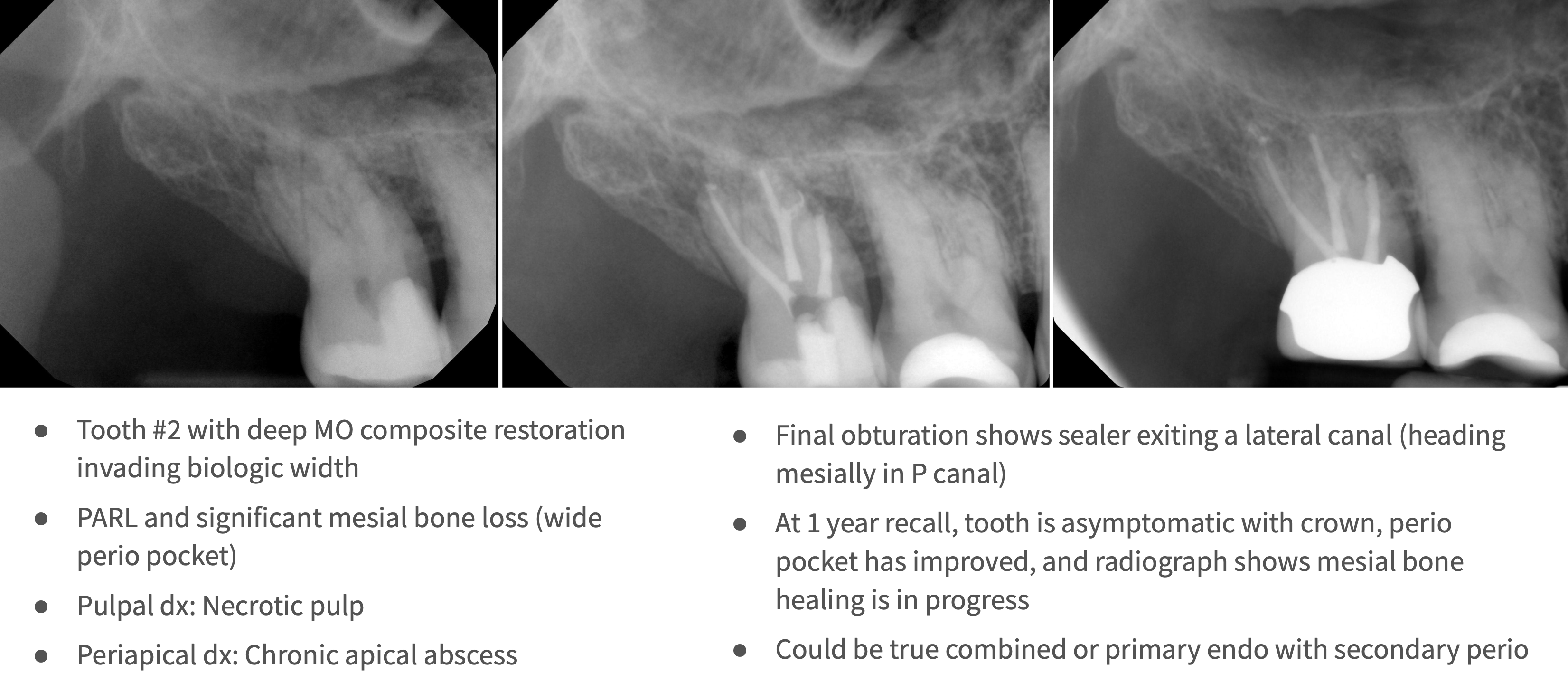
What type of lesion?
primary endo with secondary perio lesions
What is the pulpal diagnosis for primary endo with secondary perio lesions?
Necrosis (or Previously Treated)
What is the periapical diagnosis for primary endo with secondary perio lesions?
Chronic Apical Abscess
What is the treatment for primary endo with secondary perio lesions?
Non-surgical root canal treatment and final restoration
T/F: If perio was truly secondary in origin, any pockets and sinus tracts should resolve without any further periodontal treatment
True
When is the recommended follow up after RCT on primary endo, secondary perio lesion?
2-3 months to monitor gingival healing and to see if any additional treatment is needed
How long after RCT should bone heal on primary endo, secondary perio lesion?
1 year recall (but can take up to 5 years for resolution)
What does prognosis of on primary endo, secondary perio lesion depend on?
Endodontic treatment
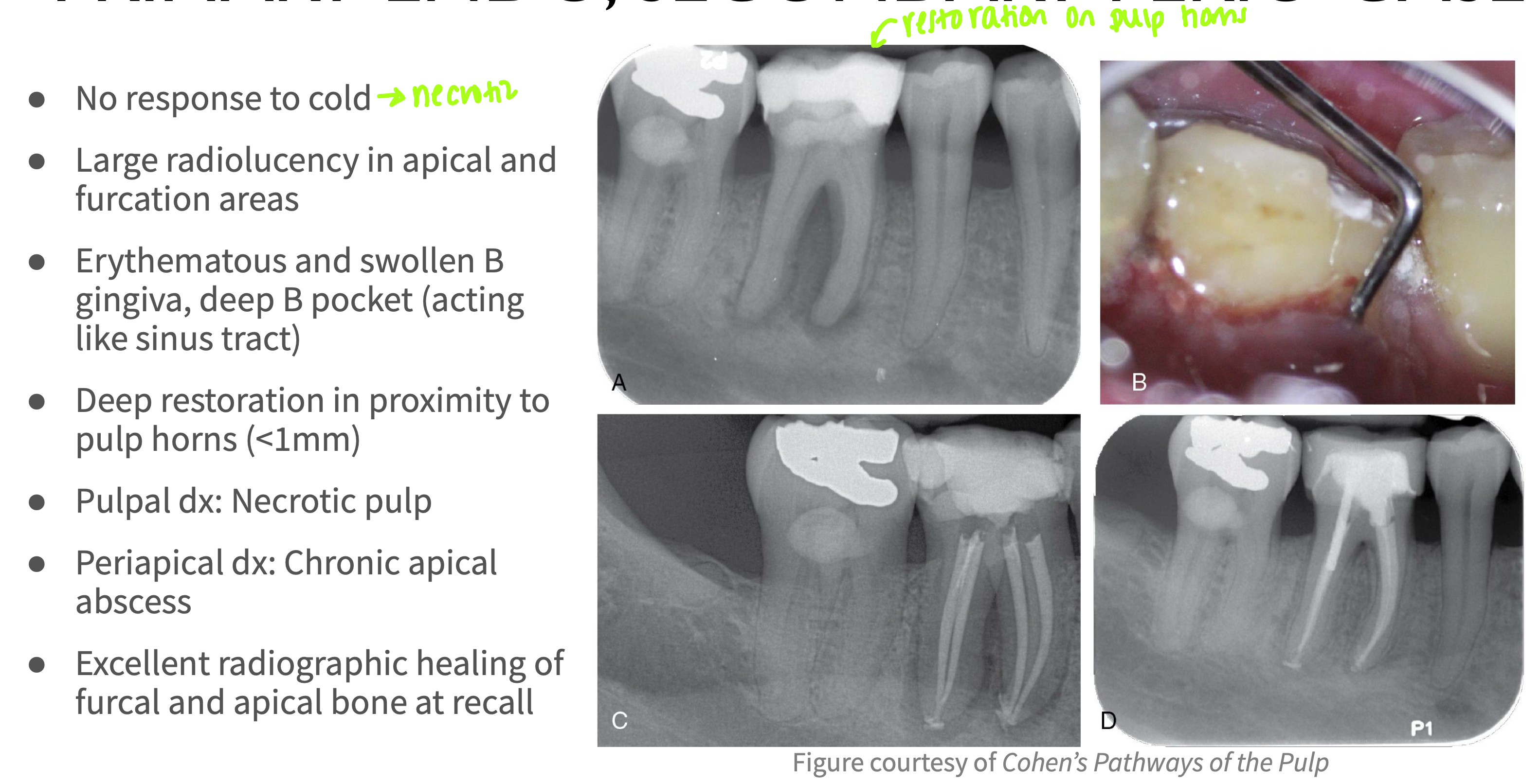
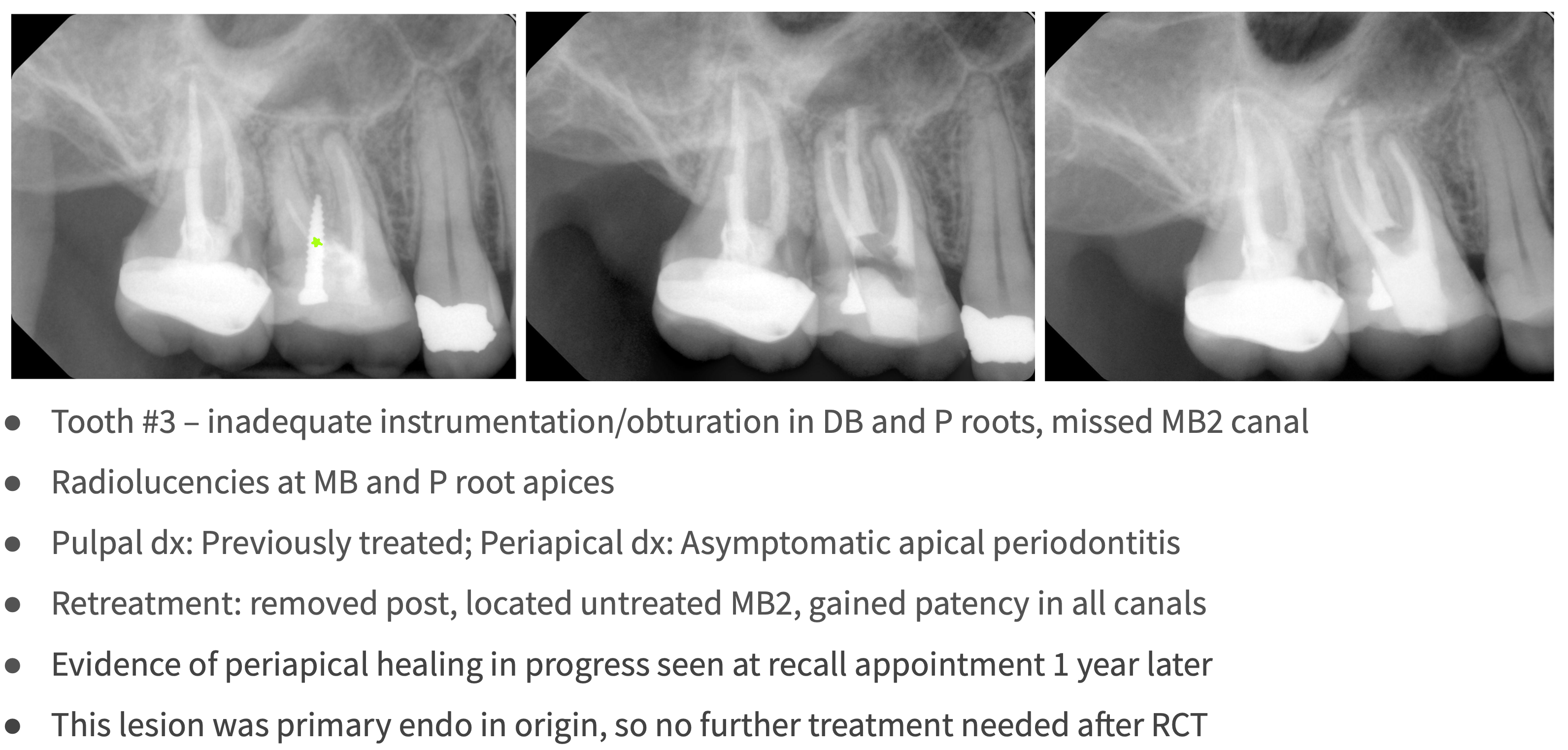
What type of lesion?
Primary endo with secondary perio lesions
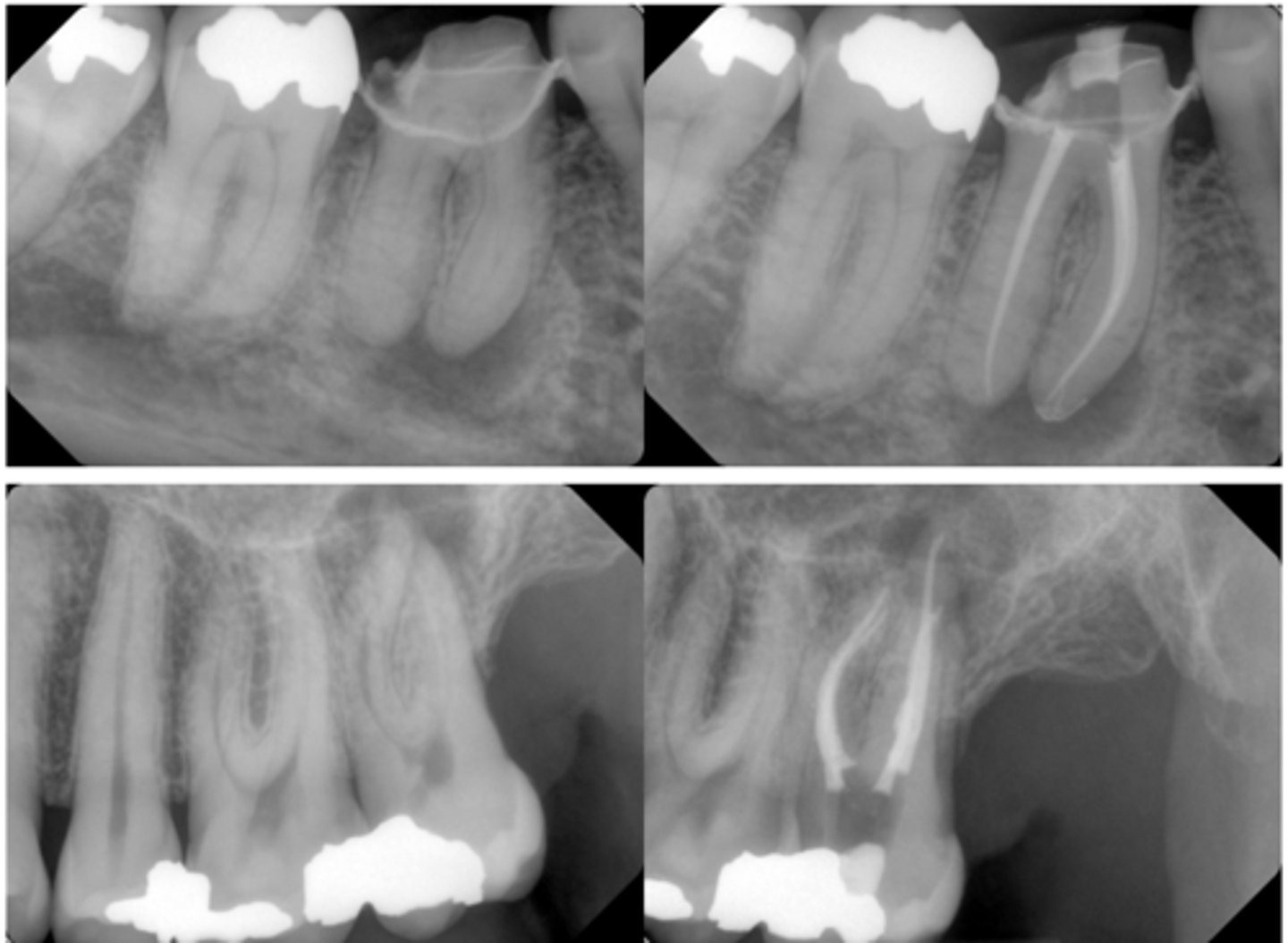
What type of lesion?
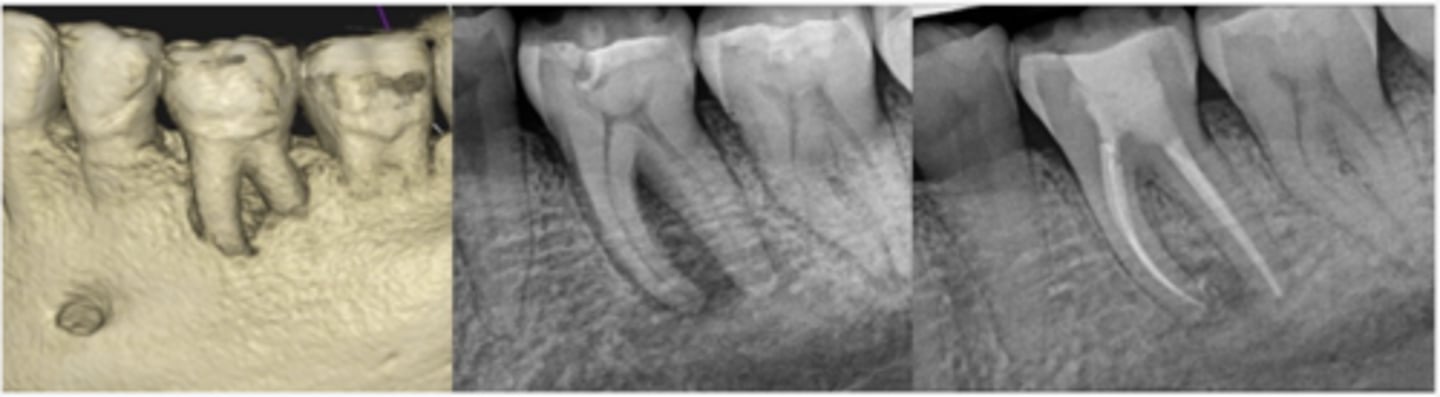
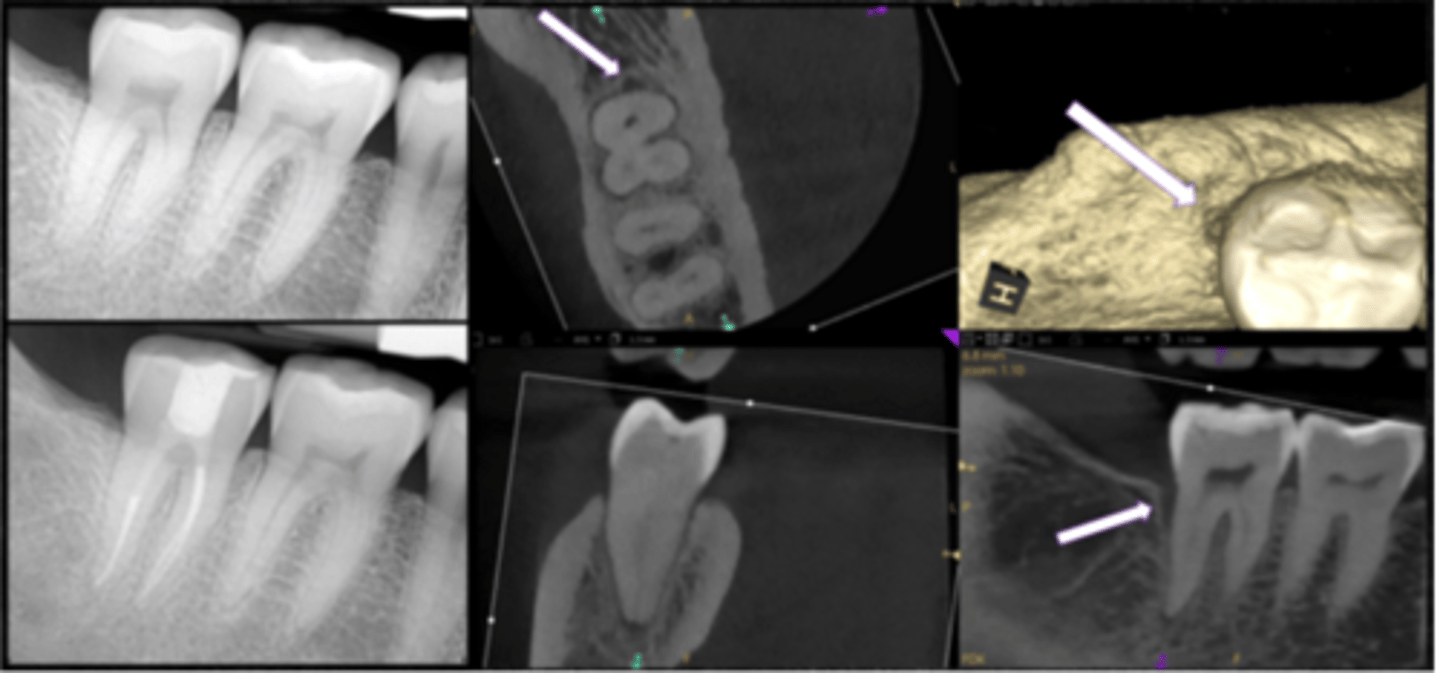
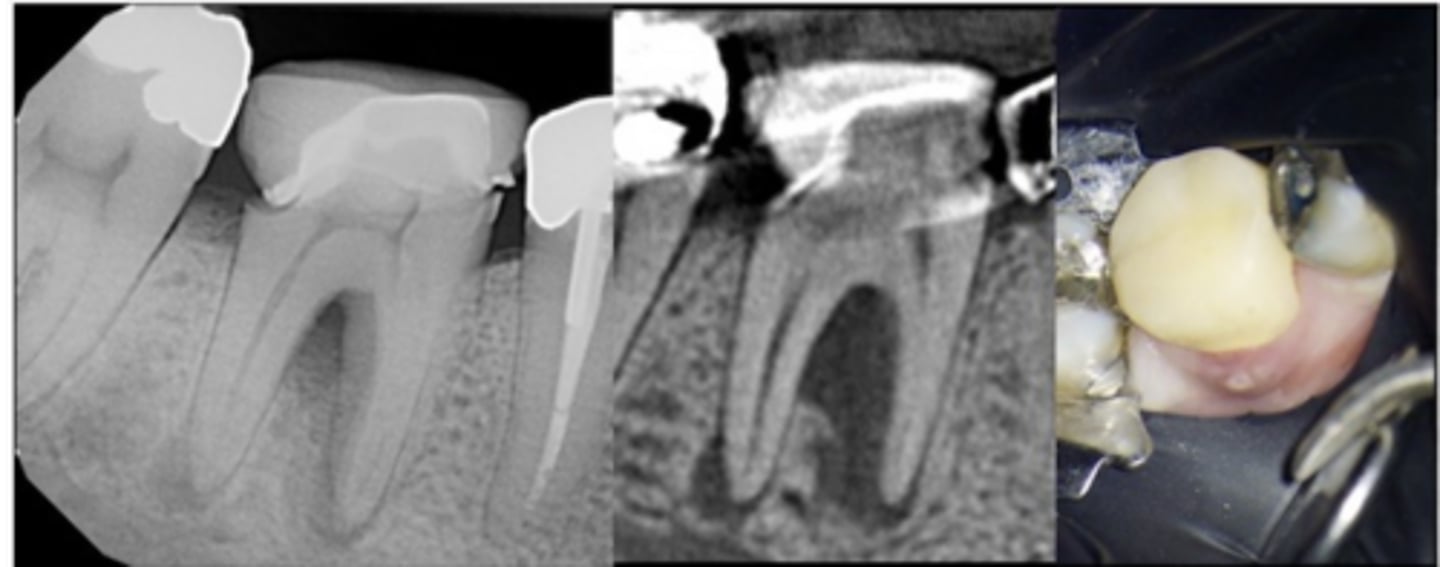
Furcation involvement and loss of buccal plate extending apically on tooth #19, visible in CBCT rendering (left) and pre-op PA radiograph (center)
Endodontic treatment was initiated and calcium hydroxide medication was placed
Four months later, tooth was obturated and healing of furcal bone was evident radiographically (right)
Primary endo with secondary perio lesions
In a primary perio lesion, periodontal disease slowly progresses coronally or apically?
apically
A primary perio lesion is vital or non-vital?
Vital
What type of lesion?
primary perio lesion
What is the pulpal diagnosis for primary perio lesions?
Normal pulp
What is the periapical diagnosis for primary perio lesions?
Normal tissues
What is the treatment of a primary perio lesion?
perio treatment (SRP, osseous surgery, gingival flap procedure with root planing, etc)
What is the prognosis of a primary perio lesion?
Depends upon the extent of the periodontitis and adherence to OHI/recall
What type of lesion?
primary perio with secondary endo
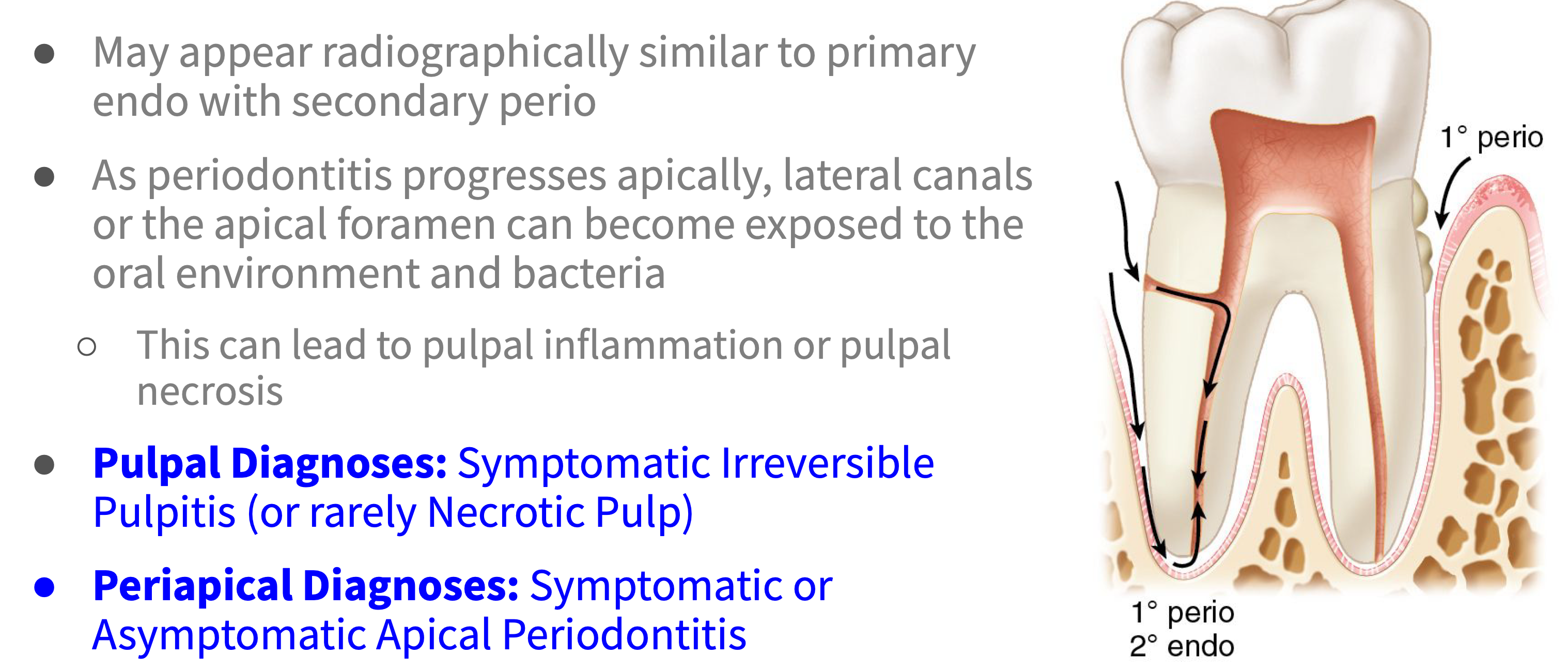
What is the pulpal diagnosis for primary perio with secondary endo lesions?
Symptomatic Irreversible Pulpitis (or rarely Necrotic Pulp)
What is the periapical diagnosis for primary perio with secondary endo lesions?
Symptomatic Apical Periodontitis or Asymptomatic Apical Periodontitis
Typically primary perio/secondary endo lesions lead to _________
Pulpitis (rarely necrosis)
What is the treatment for primary perio with secondary endo lesions with necrotic pulp?
First endo, then perio
What is the treatment for primary perio with secondary endo lesions with pulpitis?
Perio treatment first; endo treatment only if symptoms persist
Teeth undergoing periodontal treatment that are not responding to treatment as expected should have repeat sensibility testing; previously vital tooth could now be _________
Necrotic
What does the treatment prognosis depend on with primary perio/secondary endo lesions?
The extent of the periodontitis
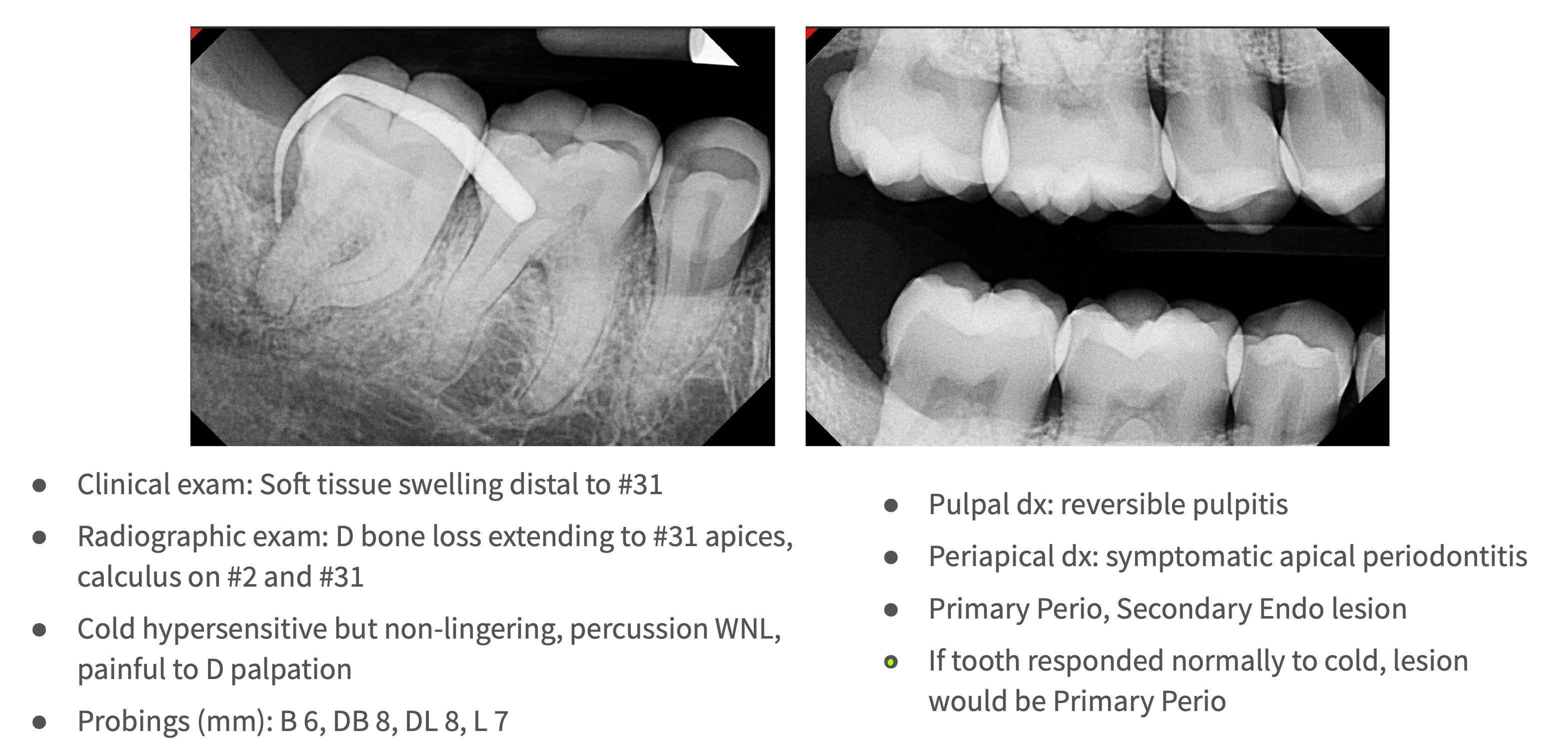
What type of lesion?
Primary perio with secondary endo
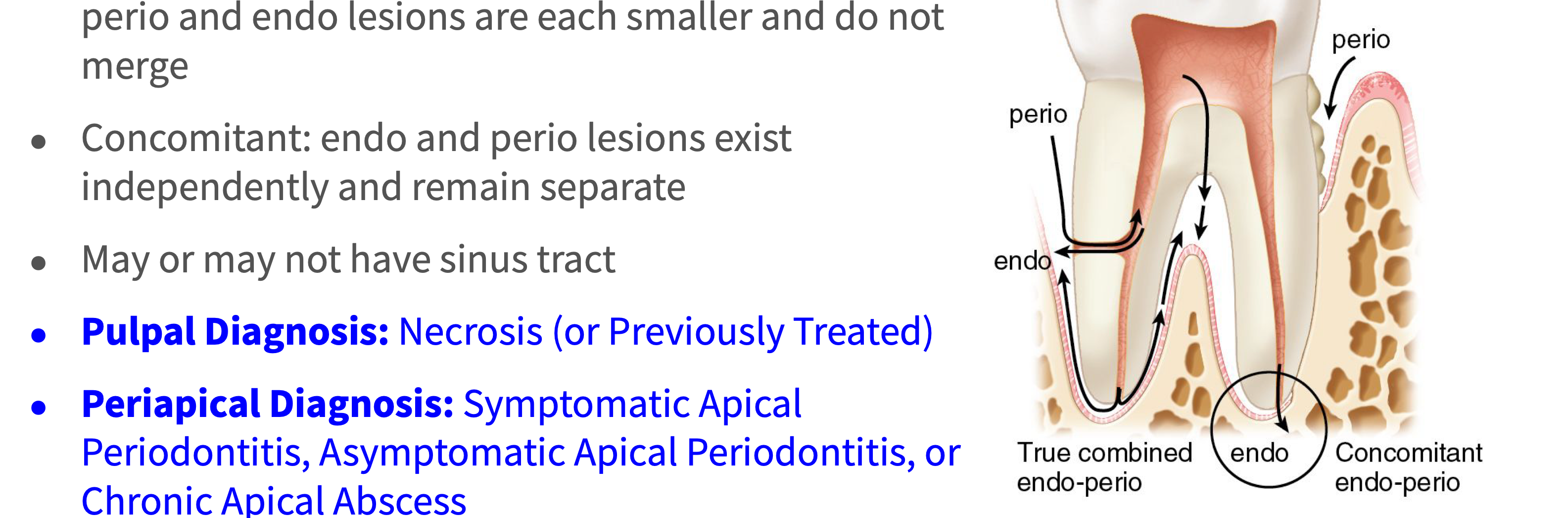
true combined
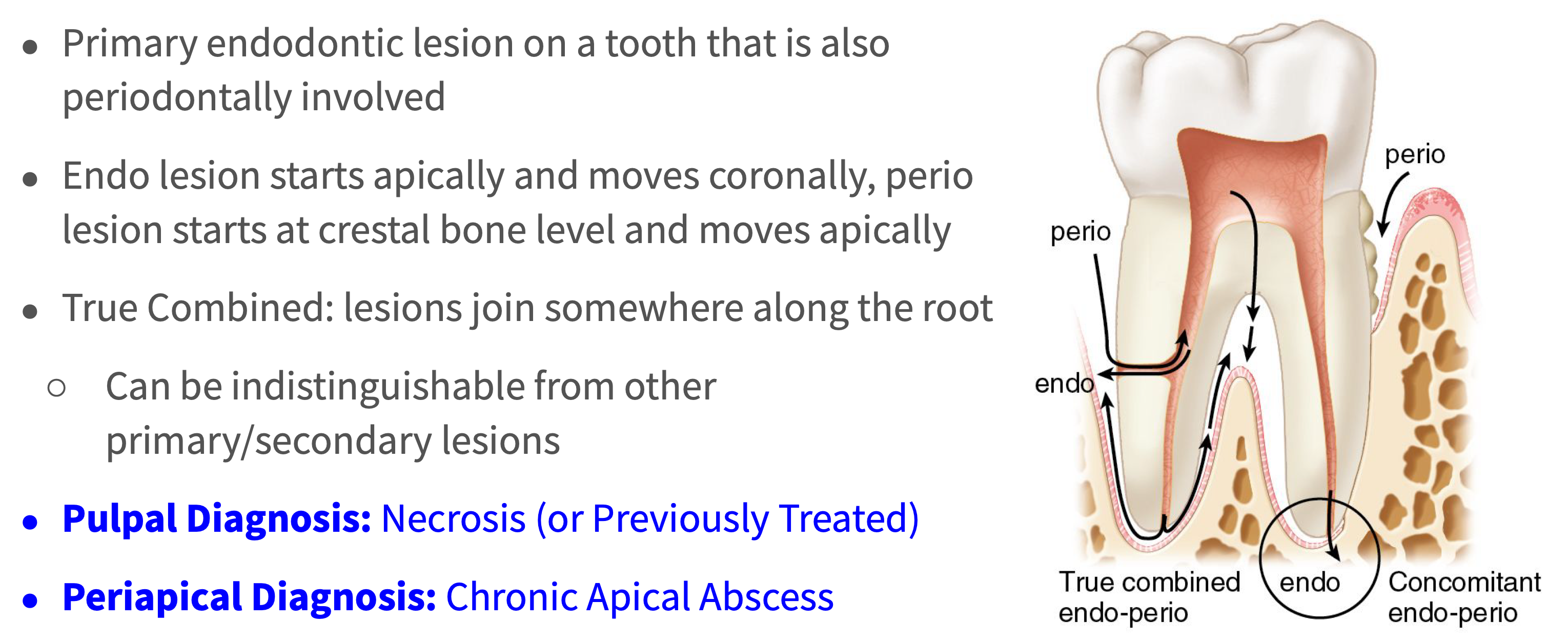
What lesion is a primary endo and primary perio lesion at the same time?
true combined lesion
In a true combined lesion, where do endo lesions start and move towards?
Starts apically and moves coronally
In a true combined lesion, where do perio lesions start and move towards?
Starts at crestal bone level and moves apically
T/F: True Combined can be indistinguishable from other primary/secondary lesions
True
What is the pulpal diagnosis for true combined lesions?
Necrosis (or Previously Treated)
What is the periapical diagnosis for true combined lesions?
Chronic Apical Abscess
What is the treatment for true combined lesions?
- The endodontic disease component of the lesion is expected to heal after RCT
- Discuss options with patient and let them decide: endo + perio treatment vs. extraction
What is the overall prognosis of a tooth with a true combined lesion?
Dependent on the extent of the periodontal disease component (also hygiene, recall, etc.)
discuss w pt: endo + perio tx vs ext
What type of lesion?
True combined lesion
What type of lesion?
Concomitant lesions
What type of lesion?
- Endo and perio lesions exist independently and remain separate
- May or may not have sinus tract
Concomitant lesions
What is the pulpal diagnosis for concomitant lesions?
Necrosis (or Previously Treated)
What is the periapical diagnosis for concomitant lesions?
- Symptomatic Apical Periodontitis
- Asymptomatic Apical Periodontitis
- or Chronic Apical Abscess
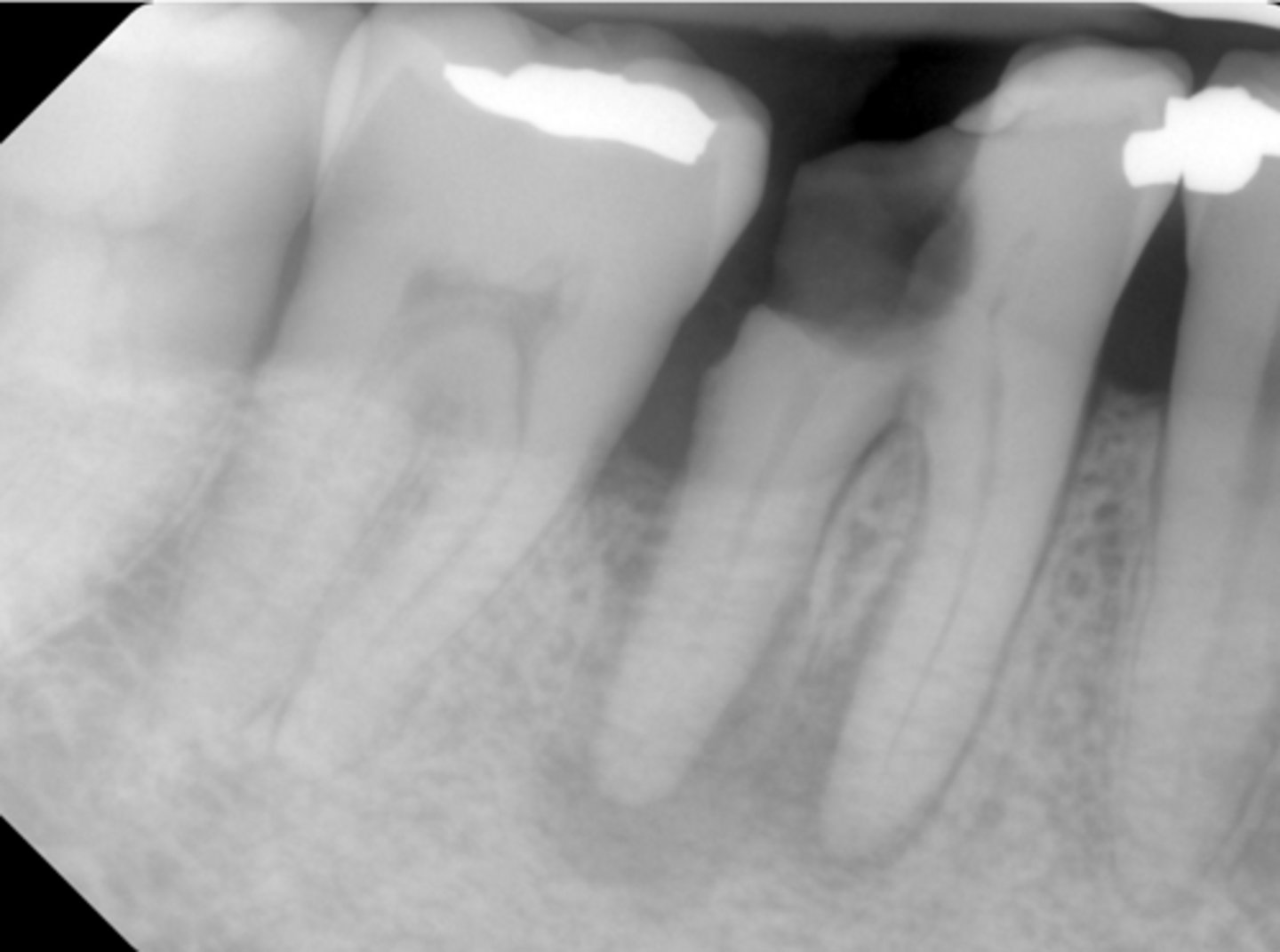
What type of lesion?
- No response to cold
- No pain on percussion or palpation
- Distal bone loss and deep pocket (independent of the PARL)
- Pulpal dx: Necrotic pulp
- Periapical dx: Asymptomatic apical periodontitis
Concomitant lesion
What is the treatment for concomitant lesions?
Endo treatment, then perio
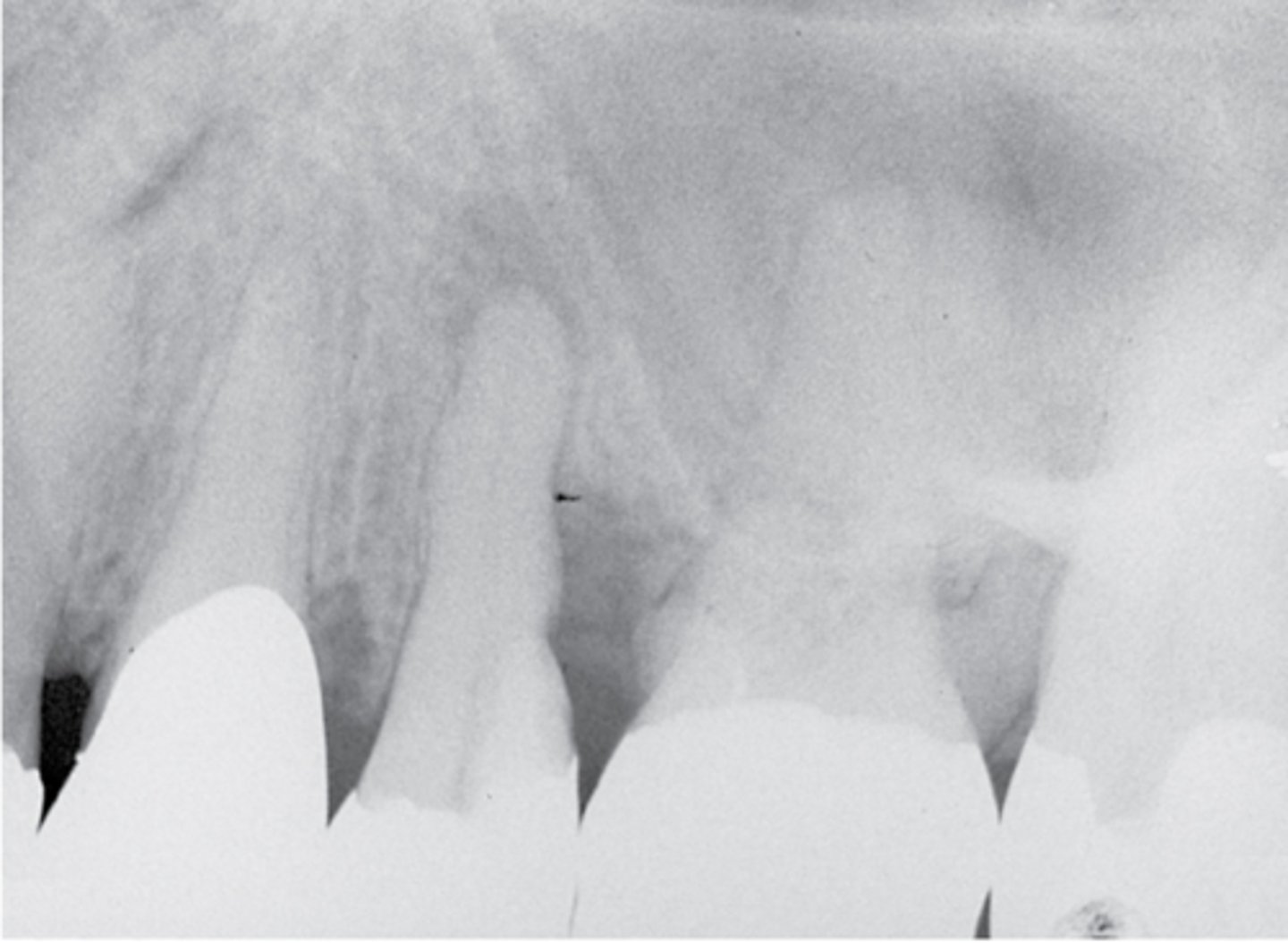
What type of lesion?
- Gross distal caries, generalized bone loss
- PARL at both apices, continuous with distal bone loss
- Which came first - endo lesion or perio lesion?
(Probably) a true combined lesion
what are each of the treatments?
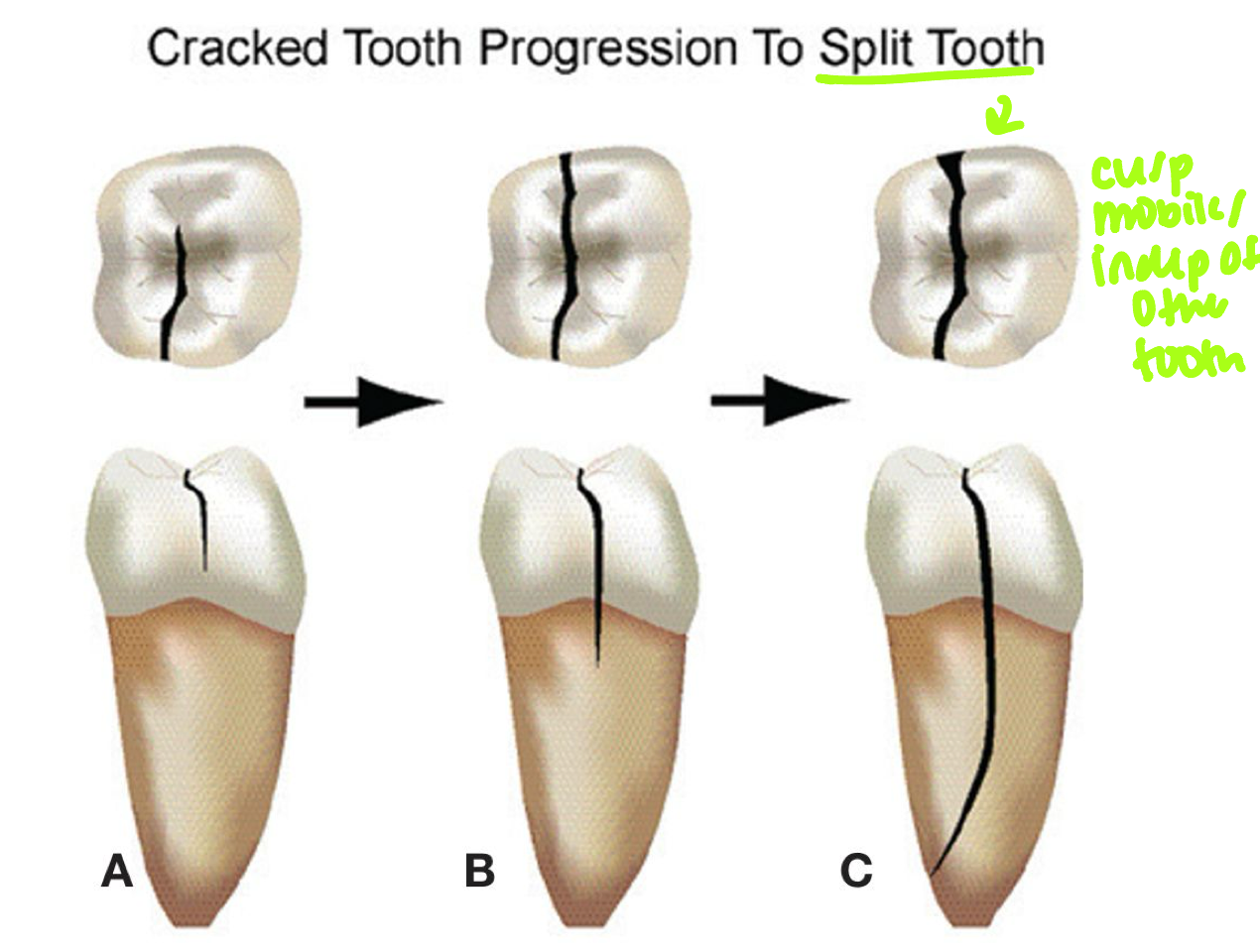
Cracks always start ________ and progress ________
Start coronally often in M→D direction and progress apically
Are cracked teeth visible in radiographs?
Not typically (due to M-D direction)
What are potential etiologies for cracked teeth?
- Poor occlusion
- Bruxism/parafunctional habits
Bacterial colonization along the crack in a tooth can lead to what?
- Pulpal inflammation
- Necrosis
How can cracks be detectable?
- Transillumination
- Dye
- Sometimes surgical assessment is needed
What is the treatment for cracked teeth?
Depends on extent of crack; split tooth will need extraction but other cracked teeth may be saved with RCT and crown
What type of lesion?
- Tooth #31 with shallow restoration. Crack developed extending through distal marginal ridge and onto distal surface
- Isolated, narrow area of bone loss develops adjacent to crack (see white arrows)
- Pulpal dx: pulp necrosis; Periapical dx: symptomatic apical periodontitis
- Recent study showed favorable longterm prognosis in cracked teeth after RCT, deep intraorifice barriers, occlusal adjustment, and immediate crown
Cracked teeth
What teeth do vertical root fractures ONLY occur on?
Previously root canal treated teeth
Where do vertical root fractures begin?
Mid-root level and can progress coronally and/or apically
What type of lesion?
- May occur buccal-lingually or mesial-distally
- May cause an isolated periodontal defect(s) or sinus tract
- May or may not be radiographically evident
- Bone loss pattern is not typically narrow like a cracked tooth
Vertical root fractures (VRF)
What is the treatment for vertical root fractures on single rooted teeth?
Extraction
What is the treatment for vertical root fractures on multi rooted teeth?
- Extraction (most common)
- Root amputation
- Or hemisection
Could this be a vertical root fracture or a crack?
- Tooth #30 CC: “There’s a bump on my gums”
- Sinus tract near B sulcus
- Probing: 12mm MB, 7mm B
- CBCT shows furcation bone loss joining with PARL at M apex; separate PARL at D apex; crestal bone appears WNL
- Pulpal dx: Necrotic
- Periapical dx: Chronic apical abscess
No (because it is not previously treated)
If a crack is suspected, what should you do?
Stain pulp chamber with dye (e.g. methylene blue) to detect any cracks
T/F: J-shaped lesions on necrotic teeth are always cracks!
False

What type of lesion?
- Tooth #30 CC: "There's a bump on my gums"
- Sinus tract near B sulcus
- Probing: 12mm MB, 7mm B
- CBCT shows furcation bone loss joining with PARL at M apex; separate PARL at D apex; crestal bone appears WNL
- Pulpal dx: Necrotic
- Periapical dx: Chronic apical abscess
- Apical and furcal bone healing observed at recall without additional periodontal treatment
Primary endo with secondary perio lesions
T/F: Interactions between endodontic and periodontal disease occur because of the numerous anatomic and vascular connections between the pulp and the periodontium
True
Shared bacterial species across endo and perio lesions suggest that the __________ may be a possible source of root canal infections
Periodontal pocket
Treatment depends on __________
Diagnosis
(in general, an endo lesion requires endodontic treatment first, then periodontal therapy may follow as needed)
Treatment prognosis for lesions of periodontal origin depends on the extent of the ____________
Periodontitis (not the endodontic prognosis)
T/F: It can be difficult to differentiate between endo/perio lesions, cracks, and vertical root fractures. Signs and symptoms can often overlap!
True