AUBF- URINE CRYSTALS
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
41 Terms
to detect the presence of few abnormal types that may represent disorders caused by crystallization of medications compounds within the tubules.
The primary reason for the identification of urinary crystals is
Rare, few, moderate, or many per hpf
Urine crystals reported as
caused by medications or treatments
Iatrogenic
Crystal formation
Urinary solute increase + Ability to remain in solution decrease =
refrigerated acid urine
Amorphous urates form in
refrigerated alkaline urine
Amorphous phosphates form in
Heat
Amorphous urates dissolves with
Acetic acid
Amorphous phosphates dissolve with
Urine pH
The first consideration when identifying crystals
amorphous urates, uric acid and sodium urates
Most common crystals seen in acidic urine
Yellow to reddish brown
Color of crystals in acidic urine
a pH greater than 5.5
Amorphous urates found in urine pH with
Amorphous urates (Acidic)
-Yellow-brown granules microscopically
-Pink sediment due to pigment uroerythrin
-pH greater than 5.5
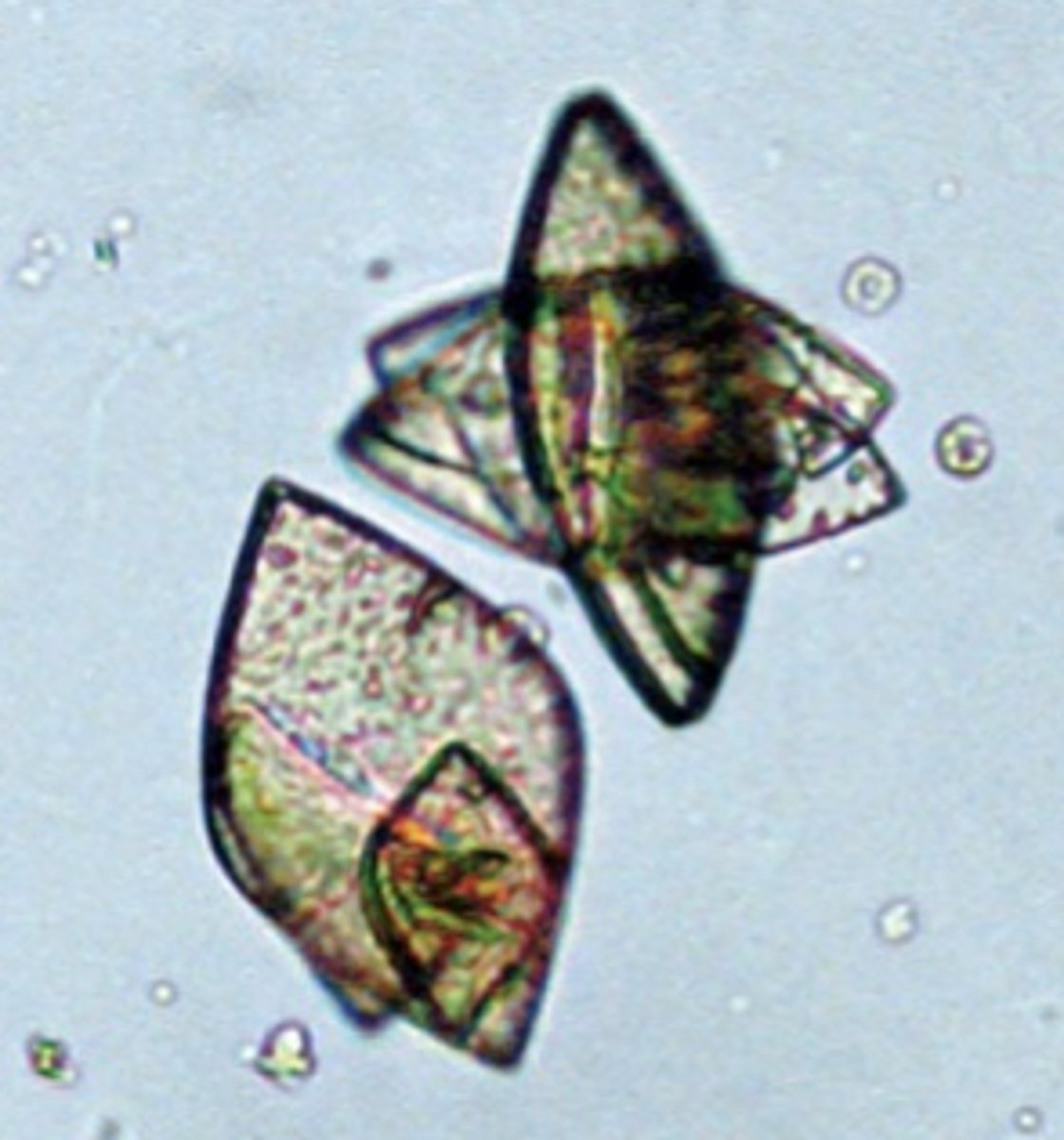
Uric Acid Crystals (Acidic)
-Shapes: rhombic, four-sided flat plates, wedges, and rosettes.
-Color: Yellow- brown, may be colorless
-Highly birefringent under polarized light.
-↑ purines, nucleic acids
-Can be seen with patients receiving chemotherapy for leukemia, gout.

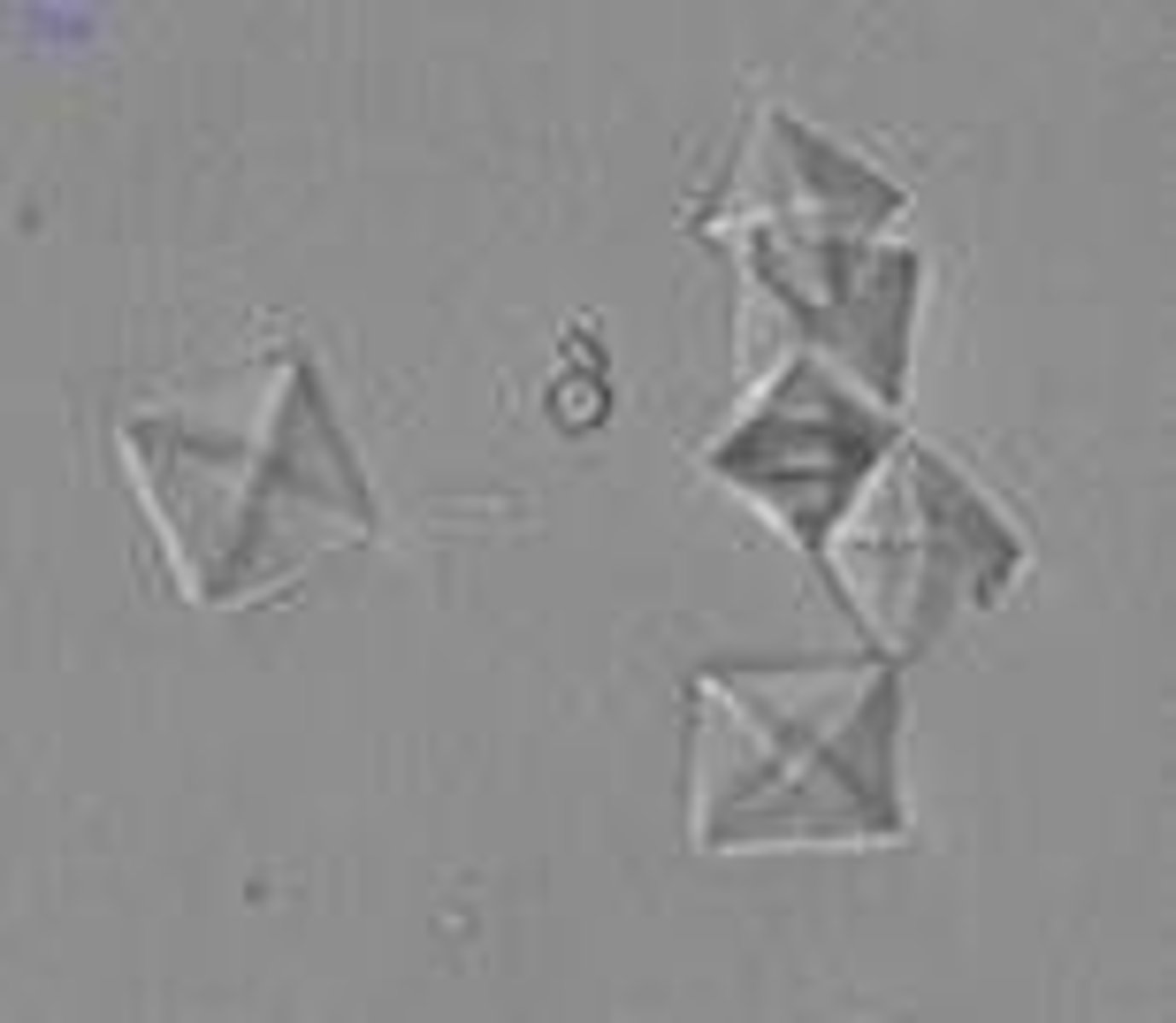
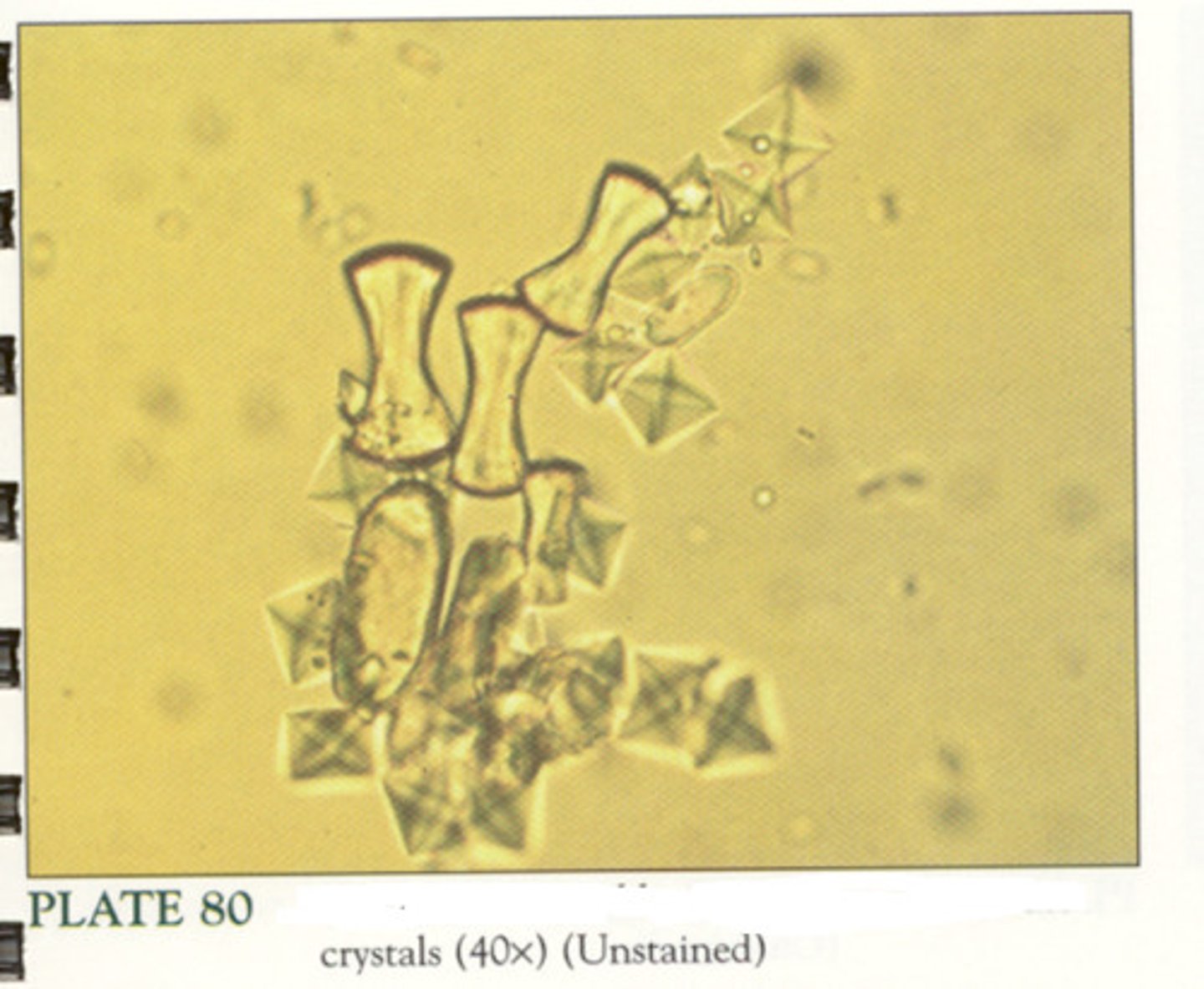
Calcium Oxalate Crystals (Acidic)
-Acid/neutral (alkaline)
-Common form: dihydrate or colorless, pyramid like
-Monohydrate is oval or dumbbell shaped; ethylene glycol poisoning.
- can relate to renal calculi
Amorphous Phosphates (Alkaline)
- Similar to amorphous urates
- Alkaline pH and heavy white precipitate after refrigeratio
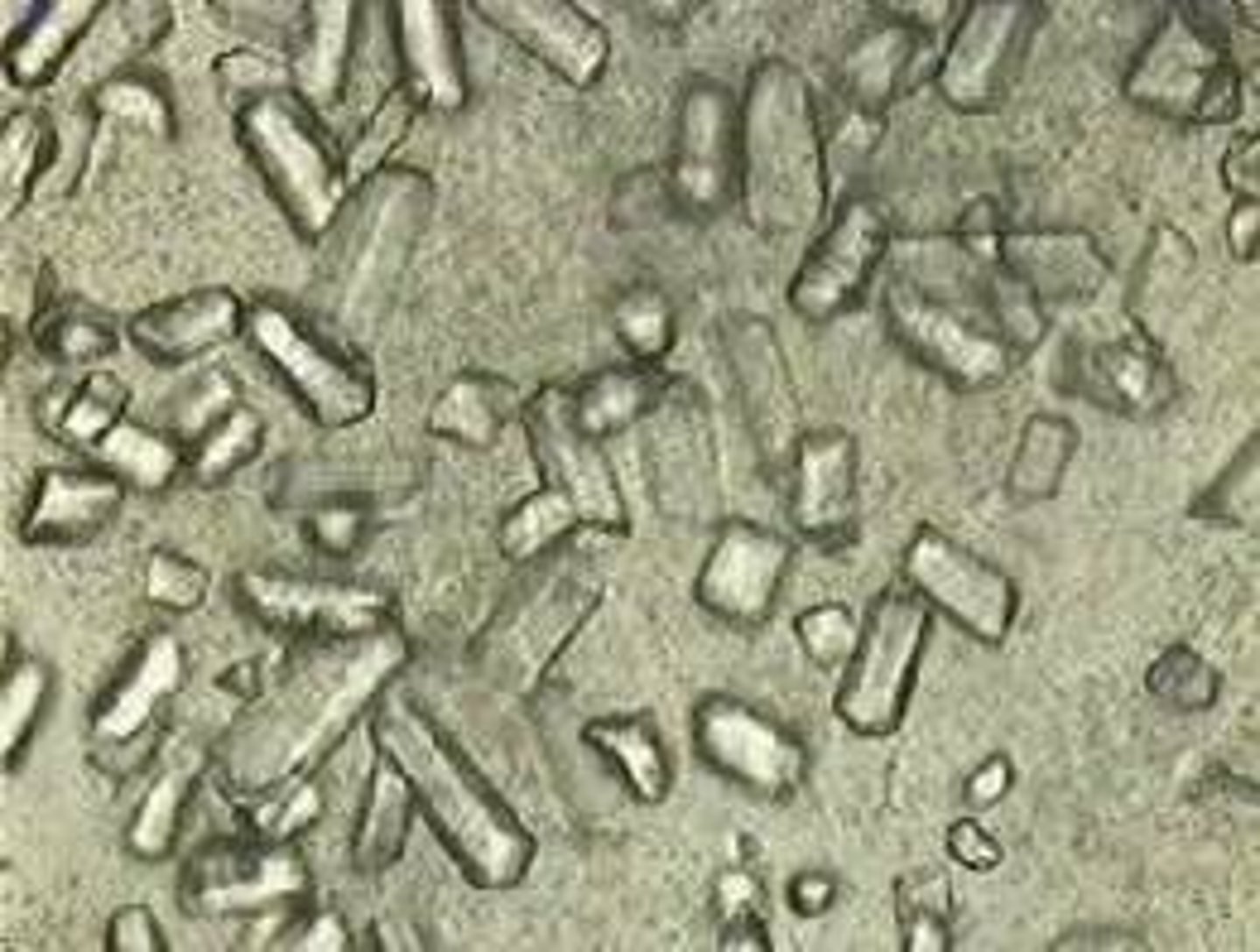
Triple Phosphate (Alkaline)
-prism shape "coffin lid"
-Highly alkaline urine and urinary tract infections (UTIs)
-colorless
Calcium Phosphate(Alkaline)
-may appear colorless
-rosette form
-Calcium phosphate crystals dissolve in dilute acetic acid and sulfonamides do not.
-common constituent of renal calculi.

Calcium Carbonate (Alkaline)
- Small, dumbbell, and spherical shapes , colorless
- Gas produced with addition of acetic acid
- No clinical significance
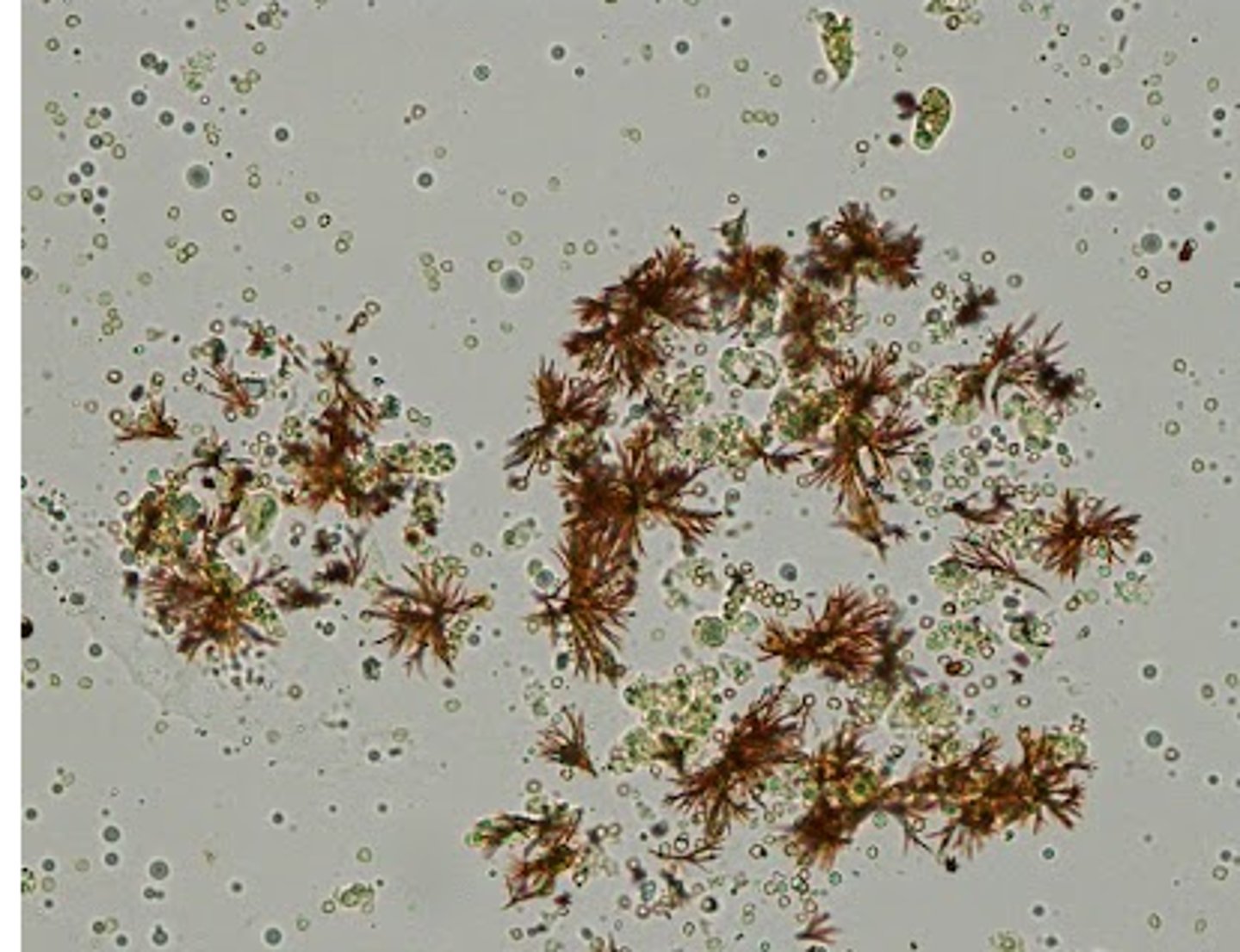
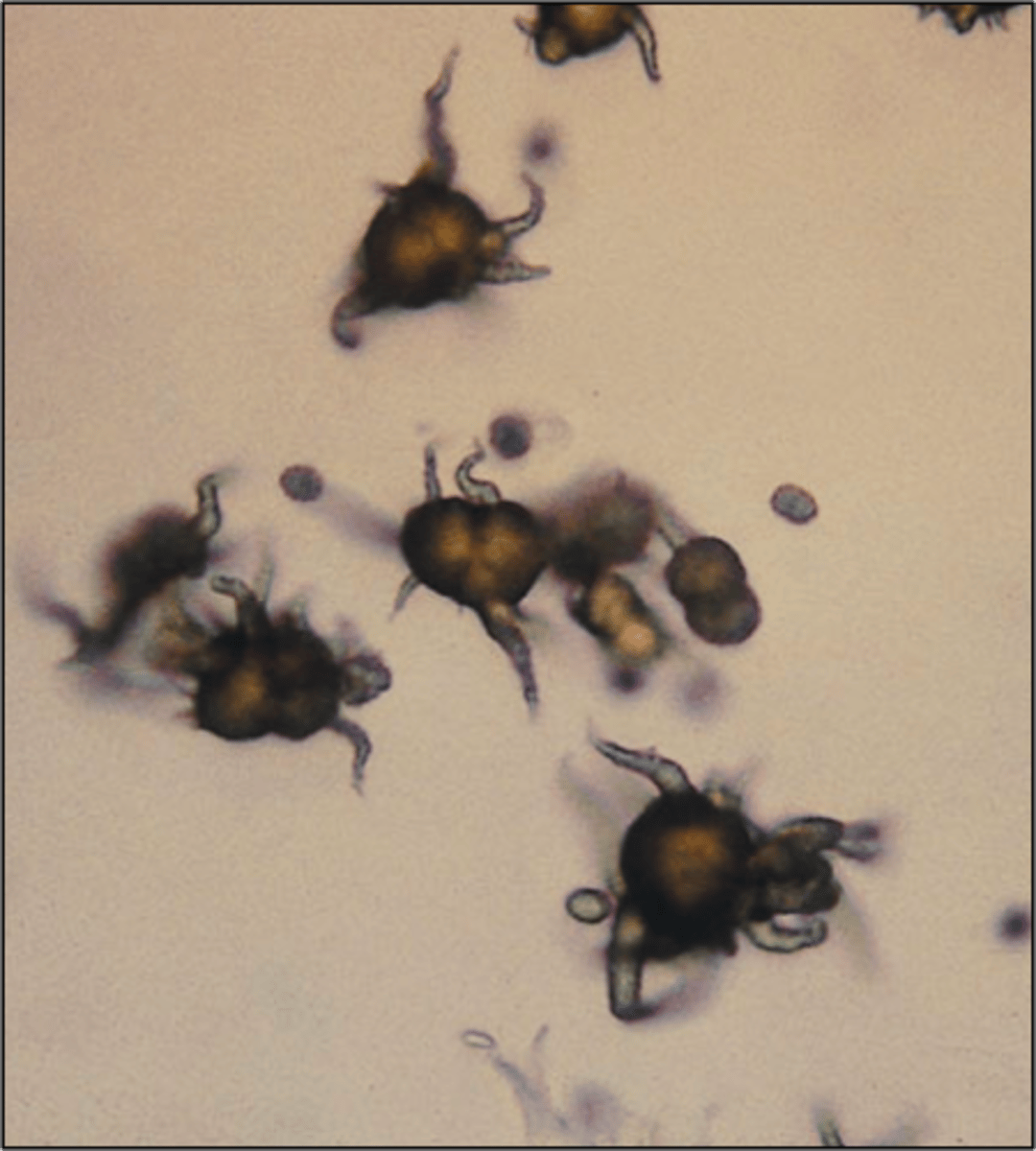
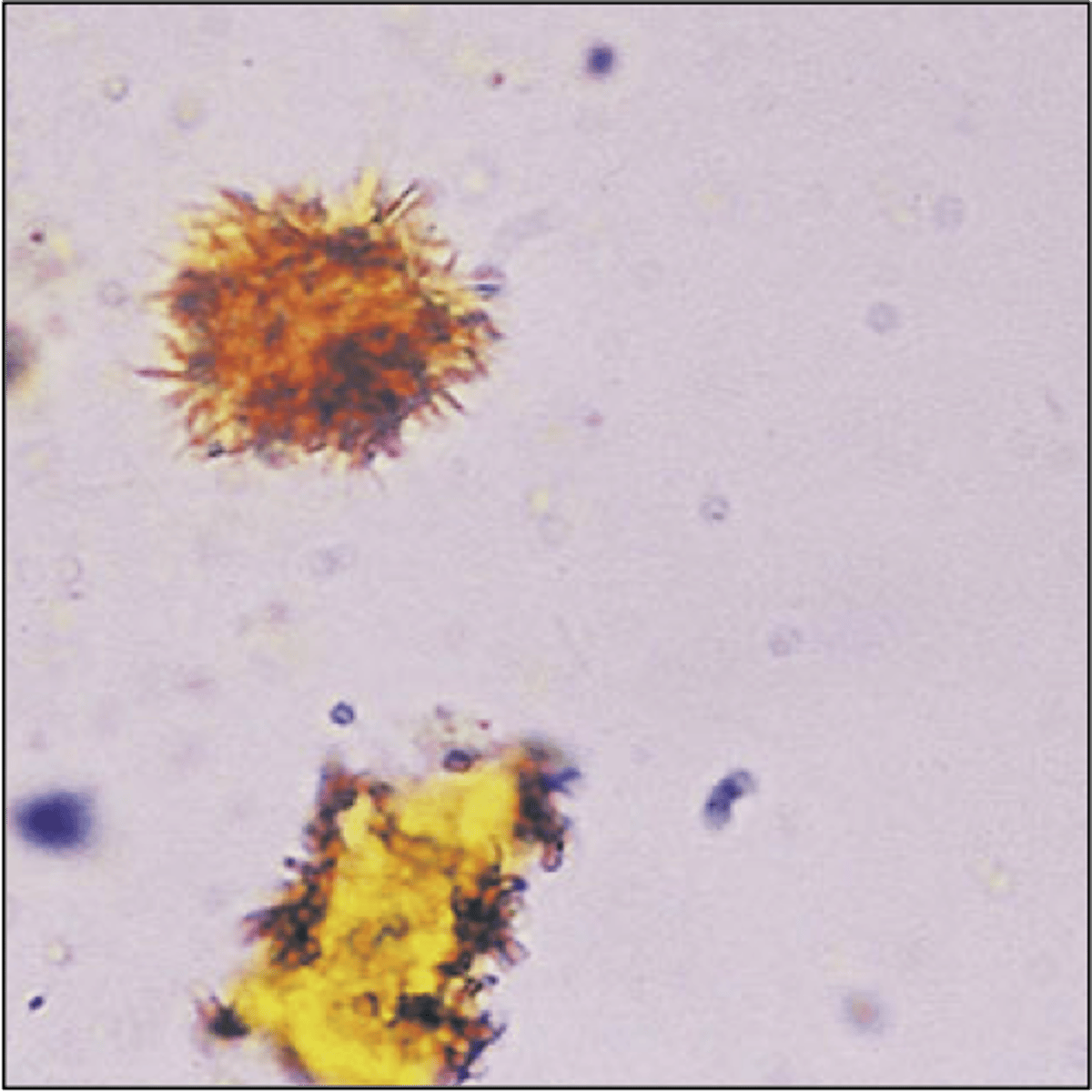
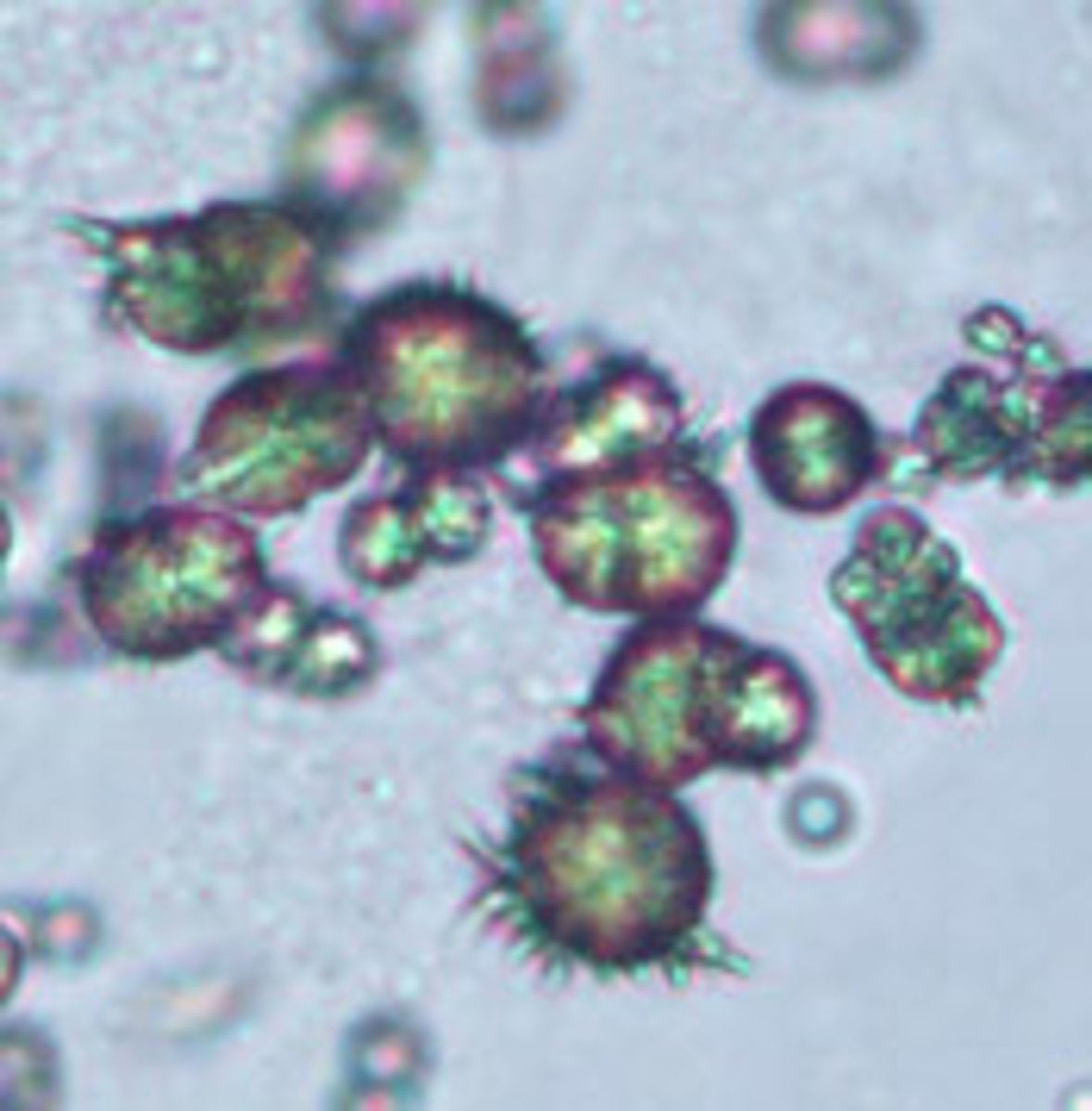
Ammonium biurate crystals (Alkaline)
-thorny apple appearance
- Yellow-brown, spicule-covered spheres
-old specimens
-may be associated with the presence of the ammonia produced by urea-splitting bacteria
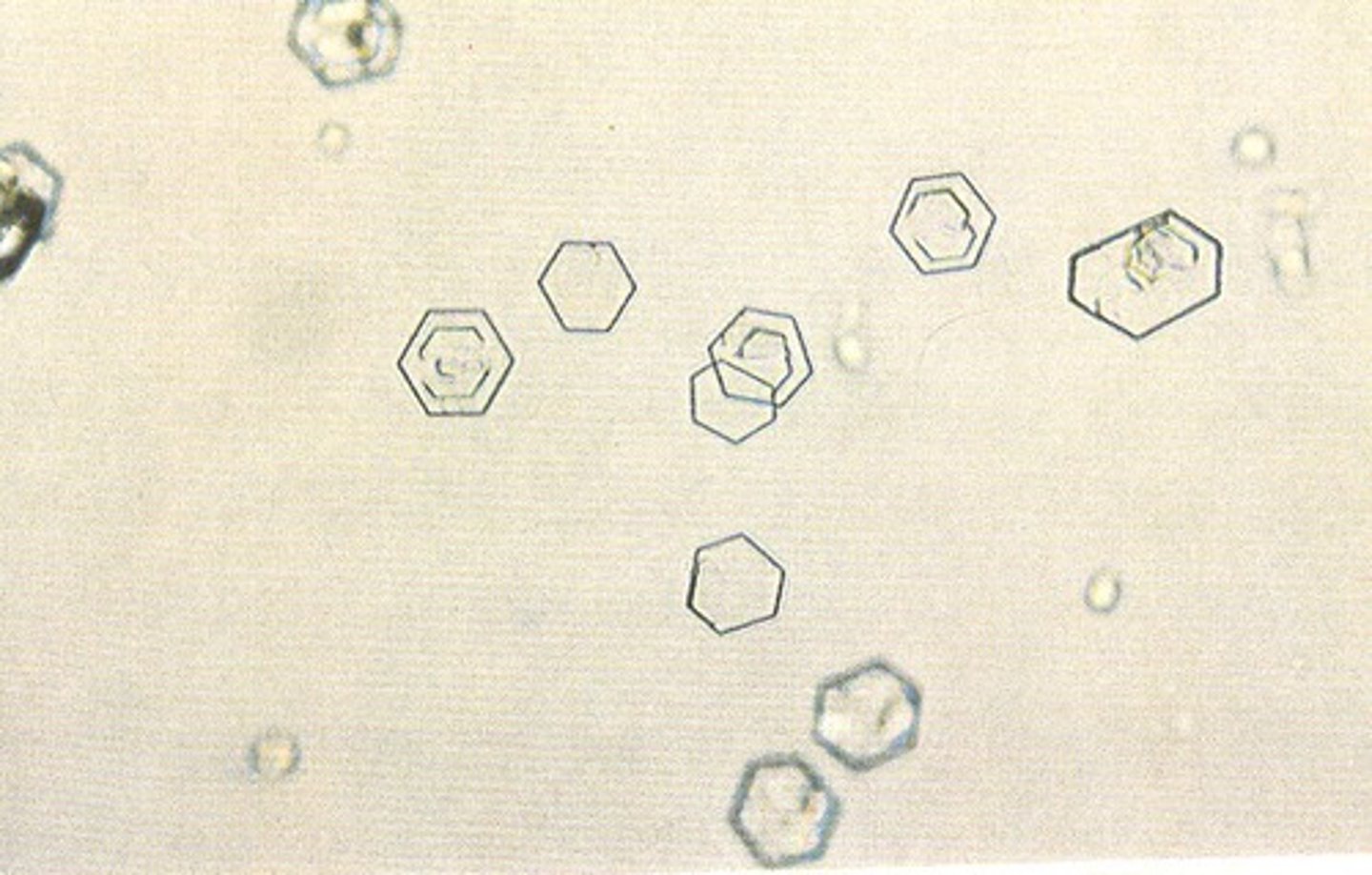
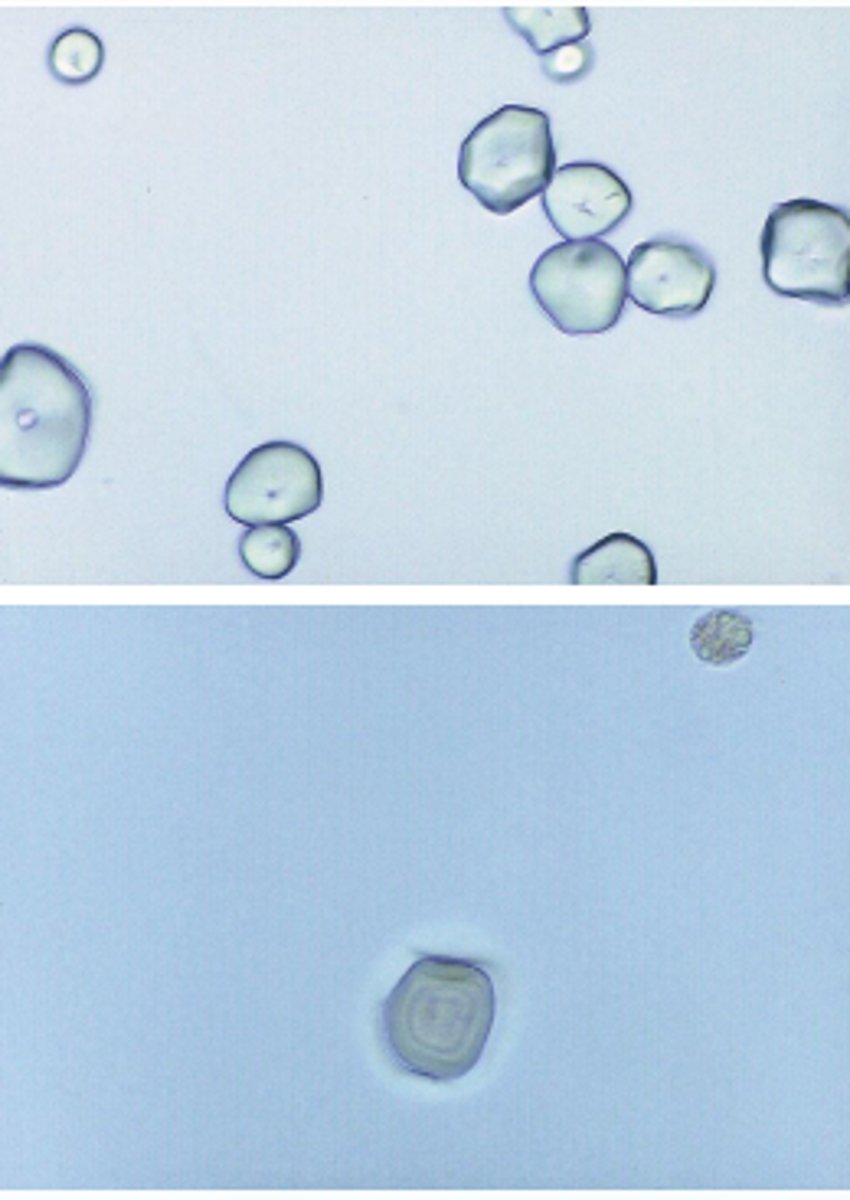
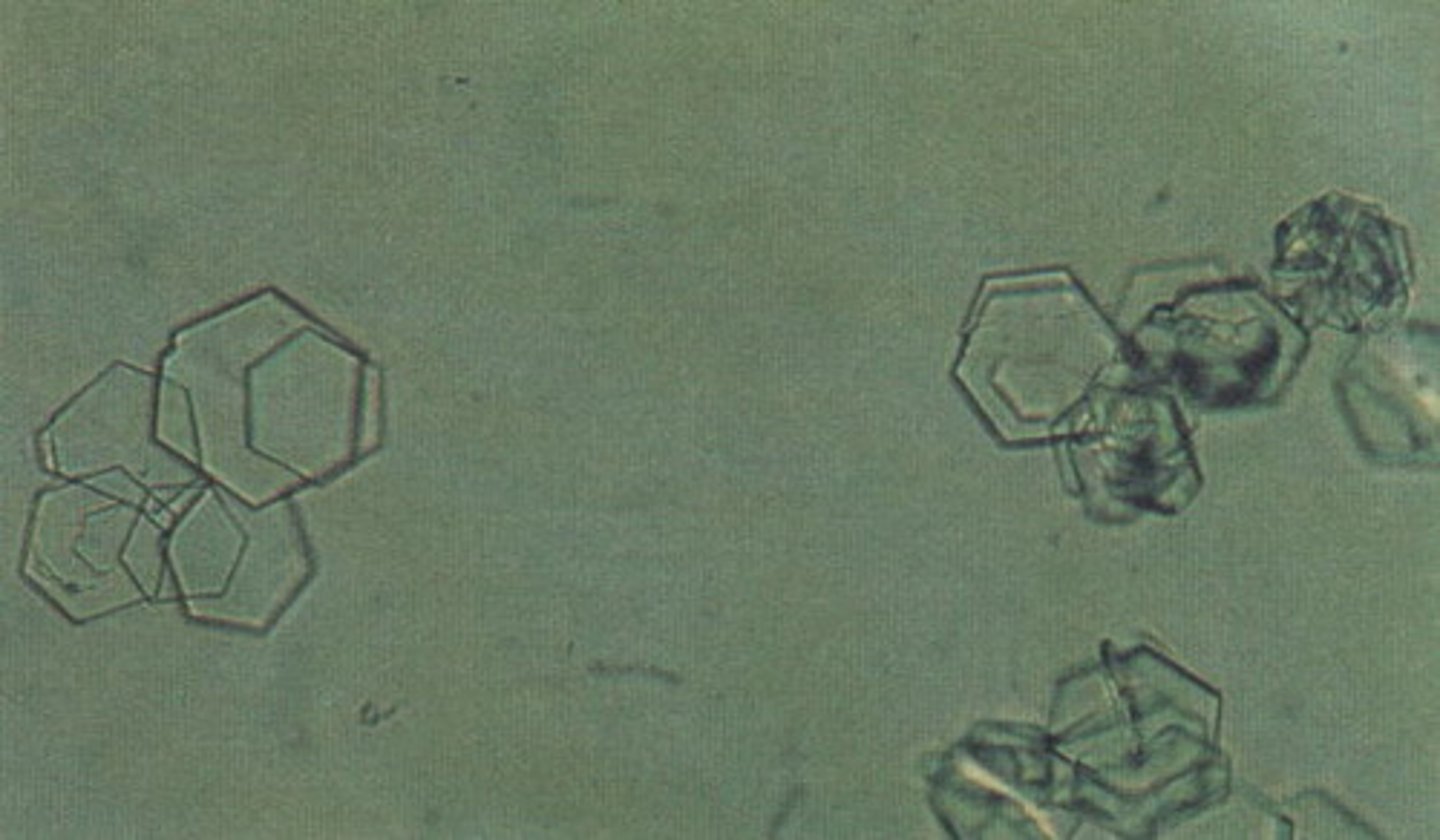
Cystine Crystals
-found in persons who inherit metabolic disorder prevent reabsorption of cystine
-Hexagonal, thin and thick plates
-Seen in cystinuria: inability to reabsorb cystine
-Confirmation by: Cyanide nitroprusside
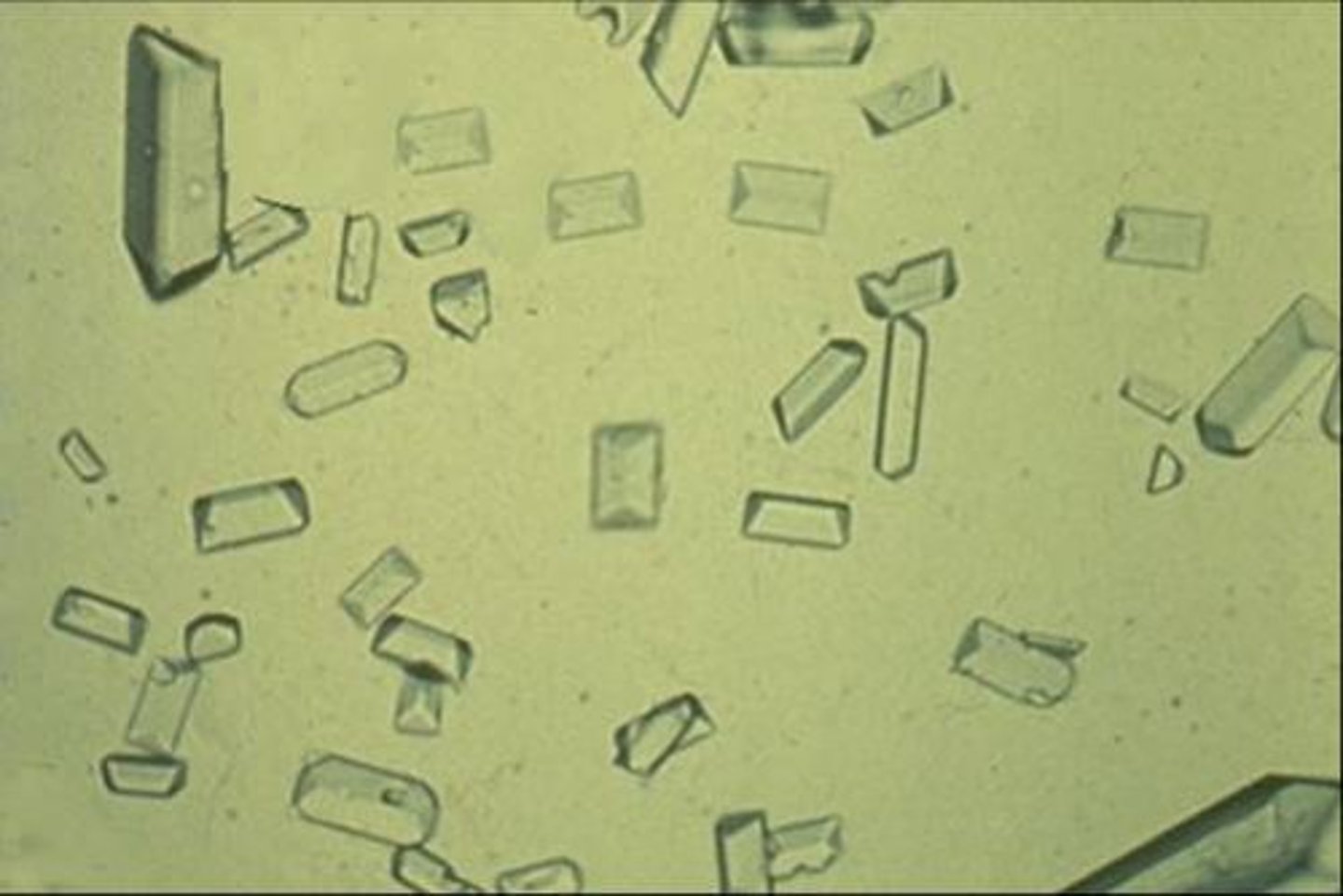
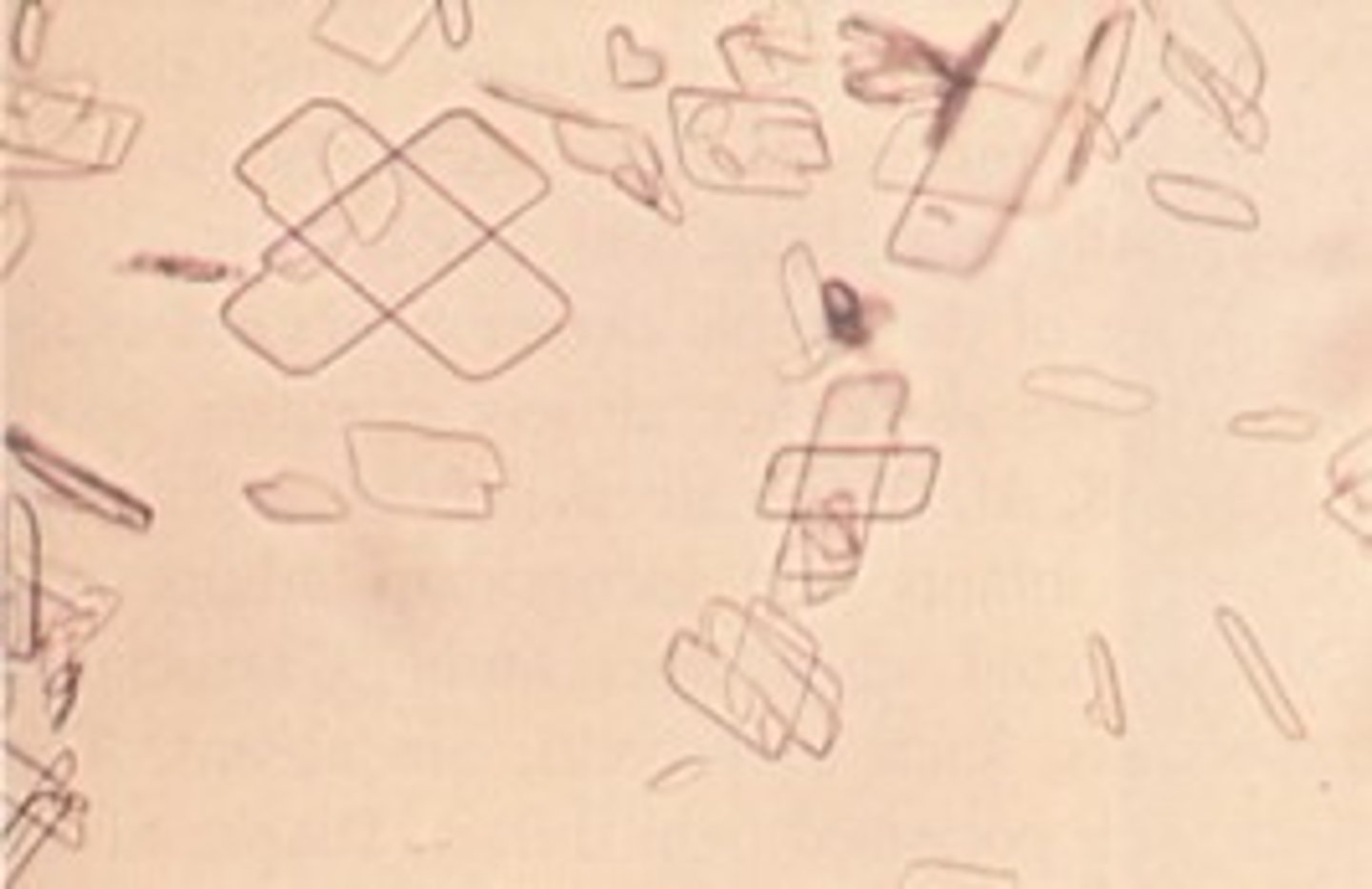
Cholesterol Crystals
-seen in refrigerated specimens
-Rectangular plates with characteristic notched corners
-associated with disorders producing lipiduria (Nephrotic S. ,fatty casts, & Oval fat bodies)

Radiographic Dye Crystals
Very high specific gravity
Similar to cholesterol crystals, polarize
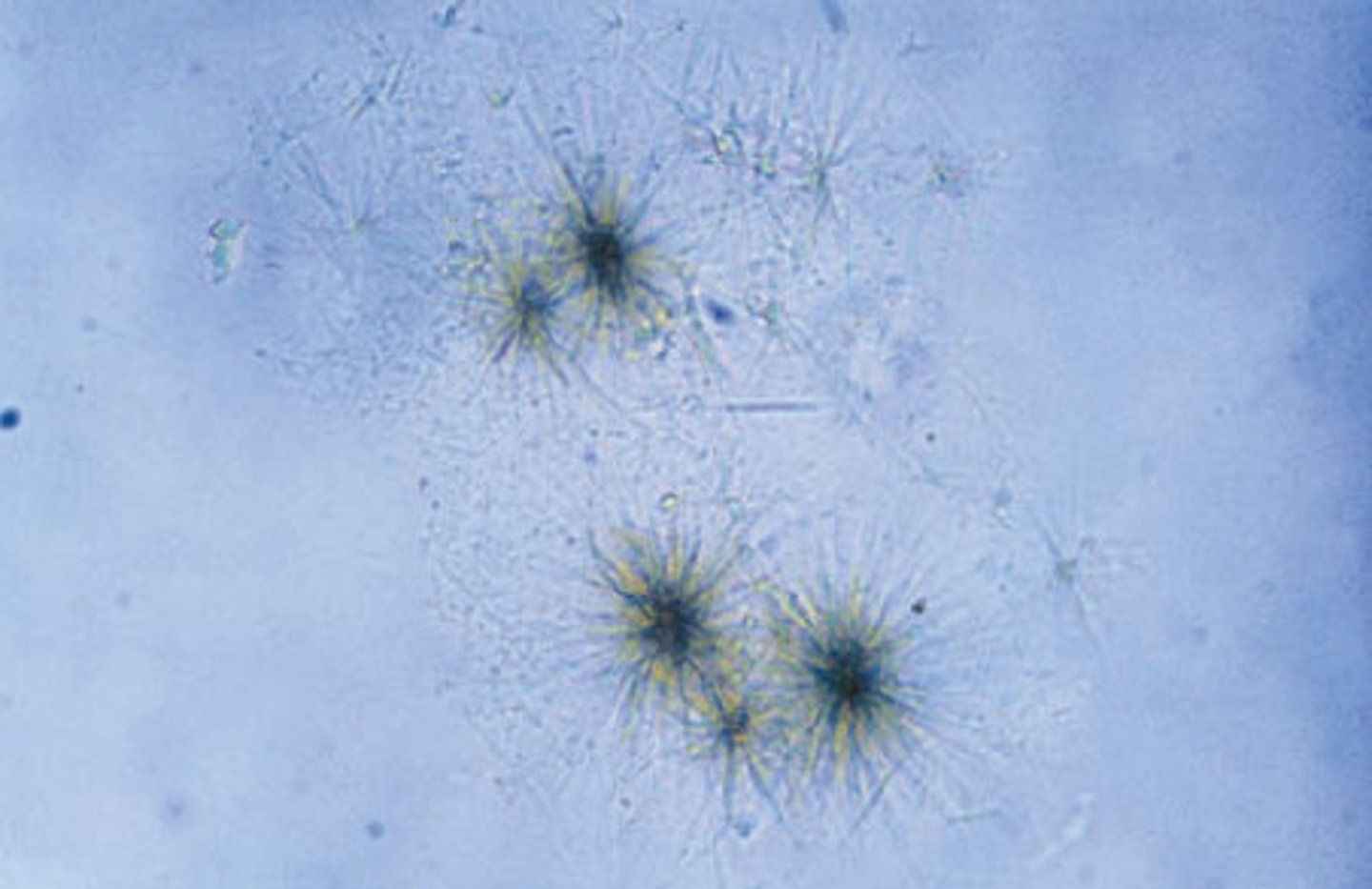
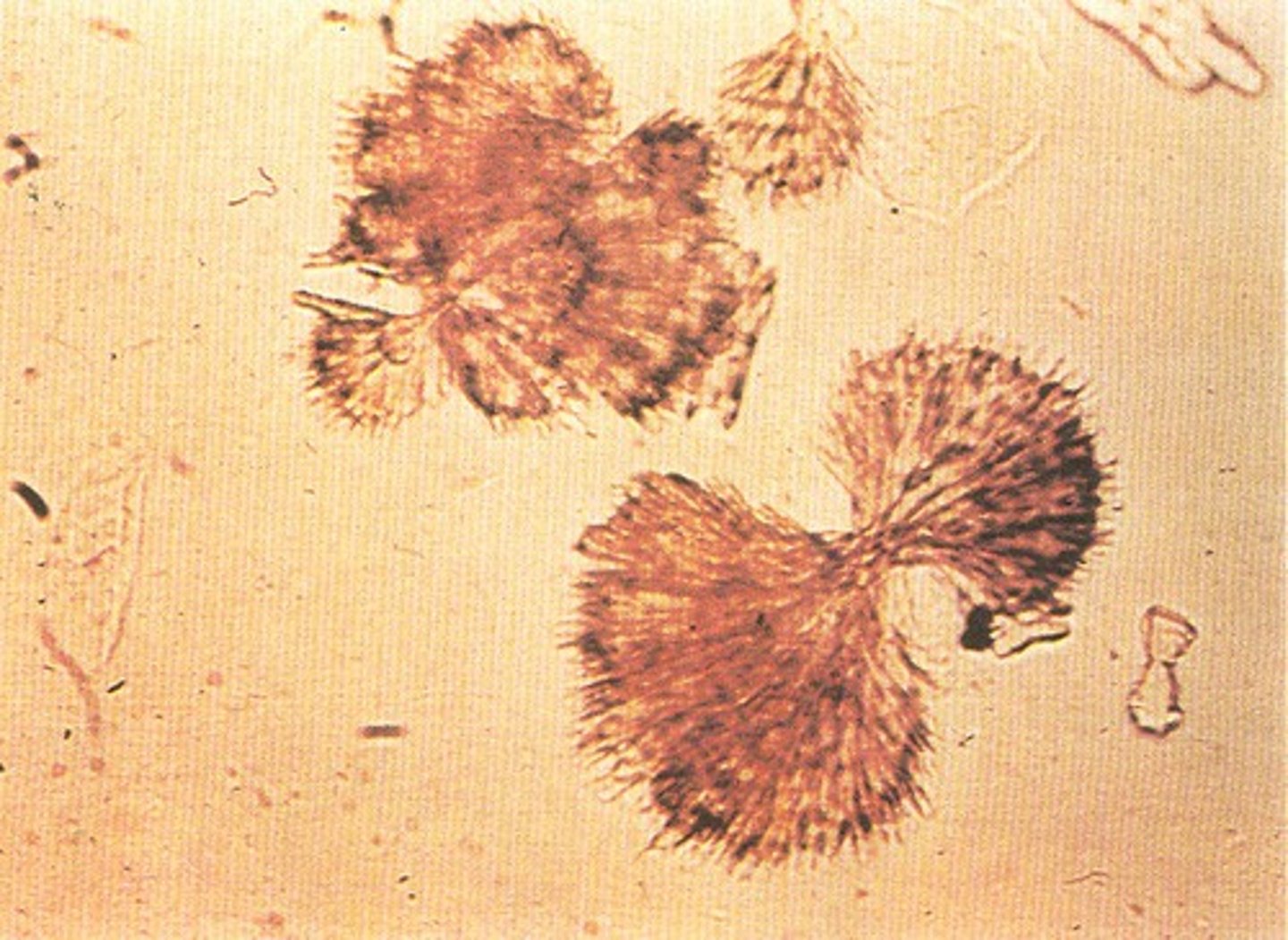
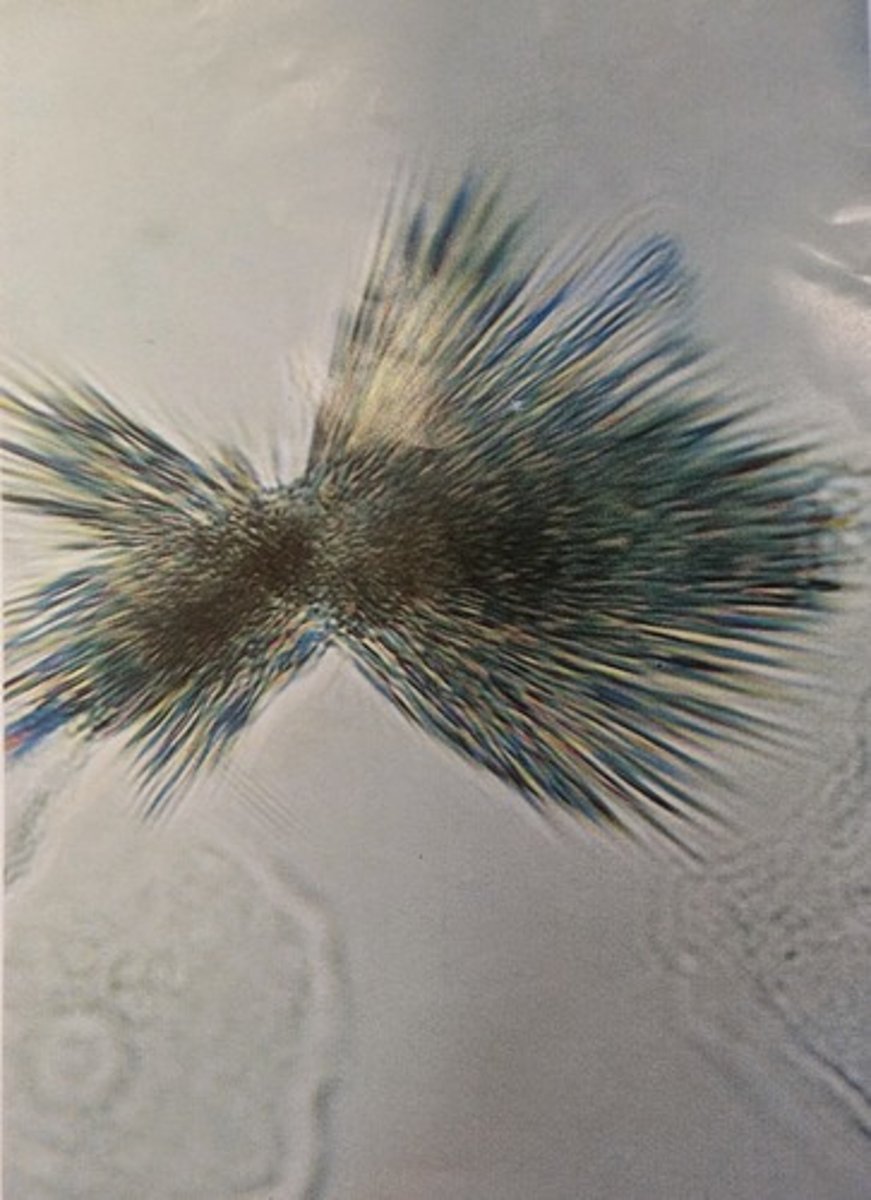
Tyrosine crystals
Fine yellow needles in clumps or rosettes
Seen with leucine crystals
Seen w/ Inherited amino acid disorders
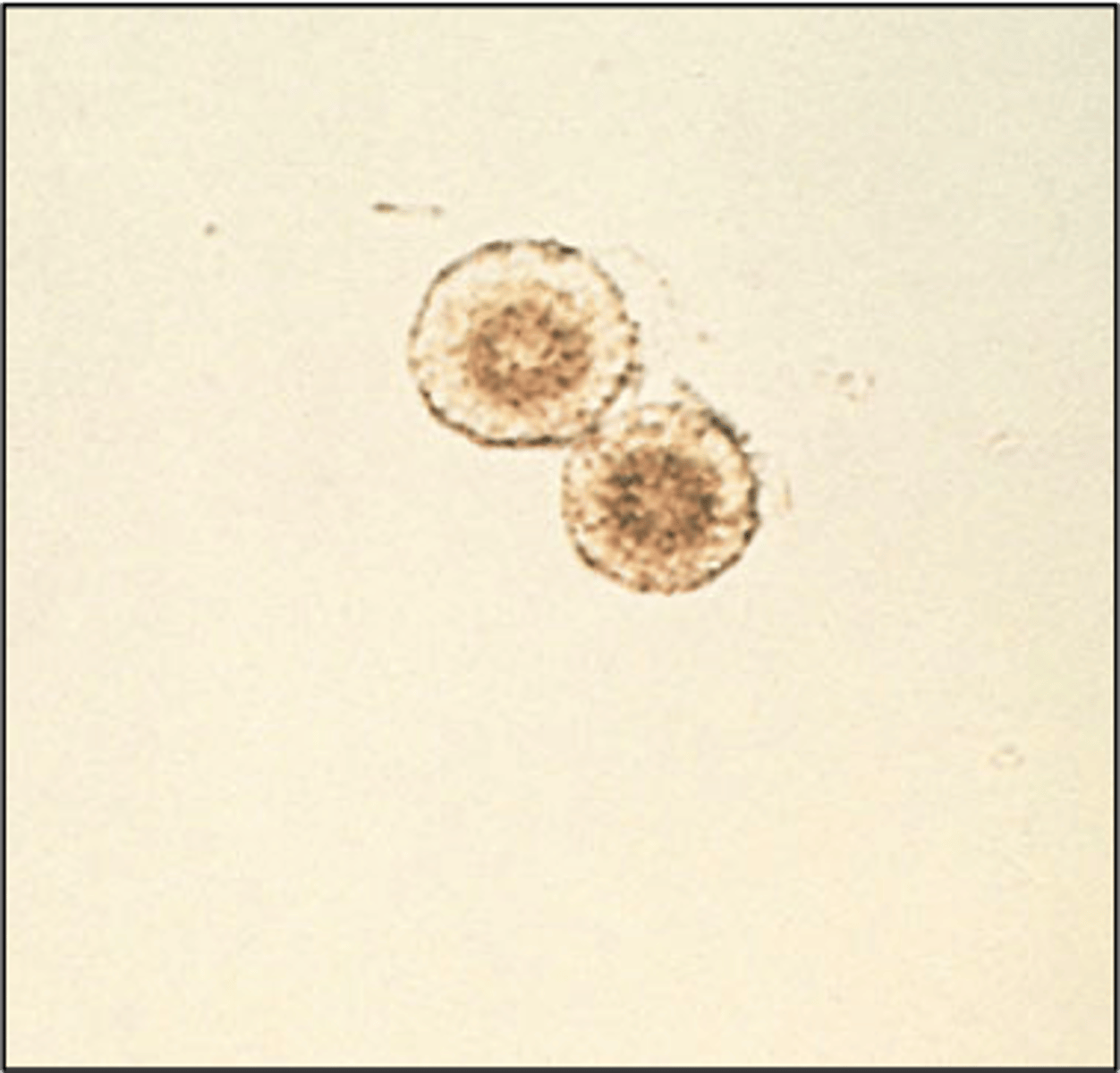
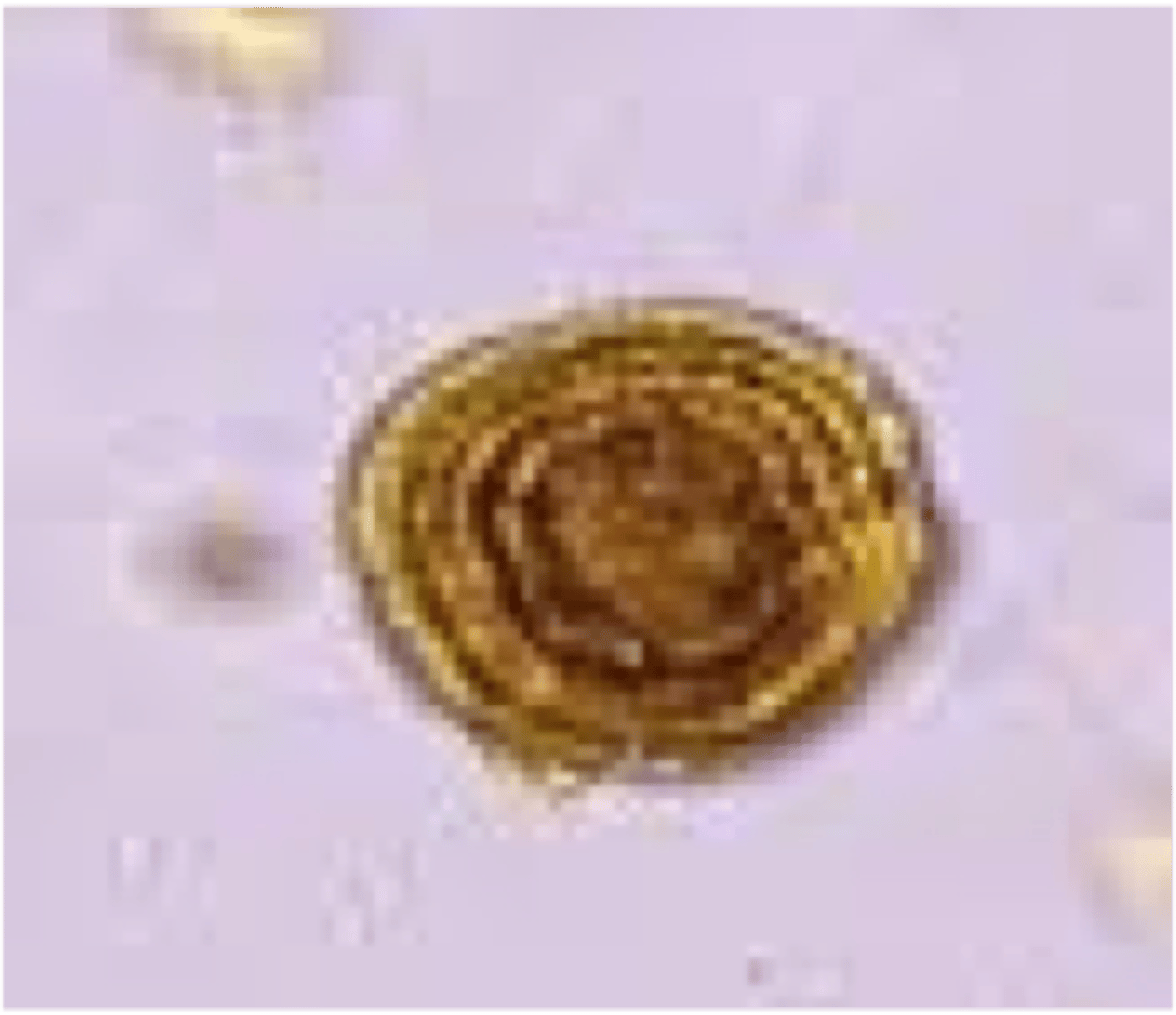
Leucine crystals
Yellow-brown spheroids with concentric rings and radial striations in the center
when present, should be accompanied by tyrosine crystals
Bilirubin crystals
present in hepatic disorders (Viral Hepatitis) producing large amounts of bilirubin in the urine
Color: Yellow
Clumped needles or granules
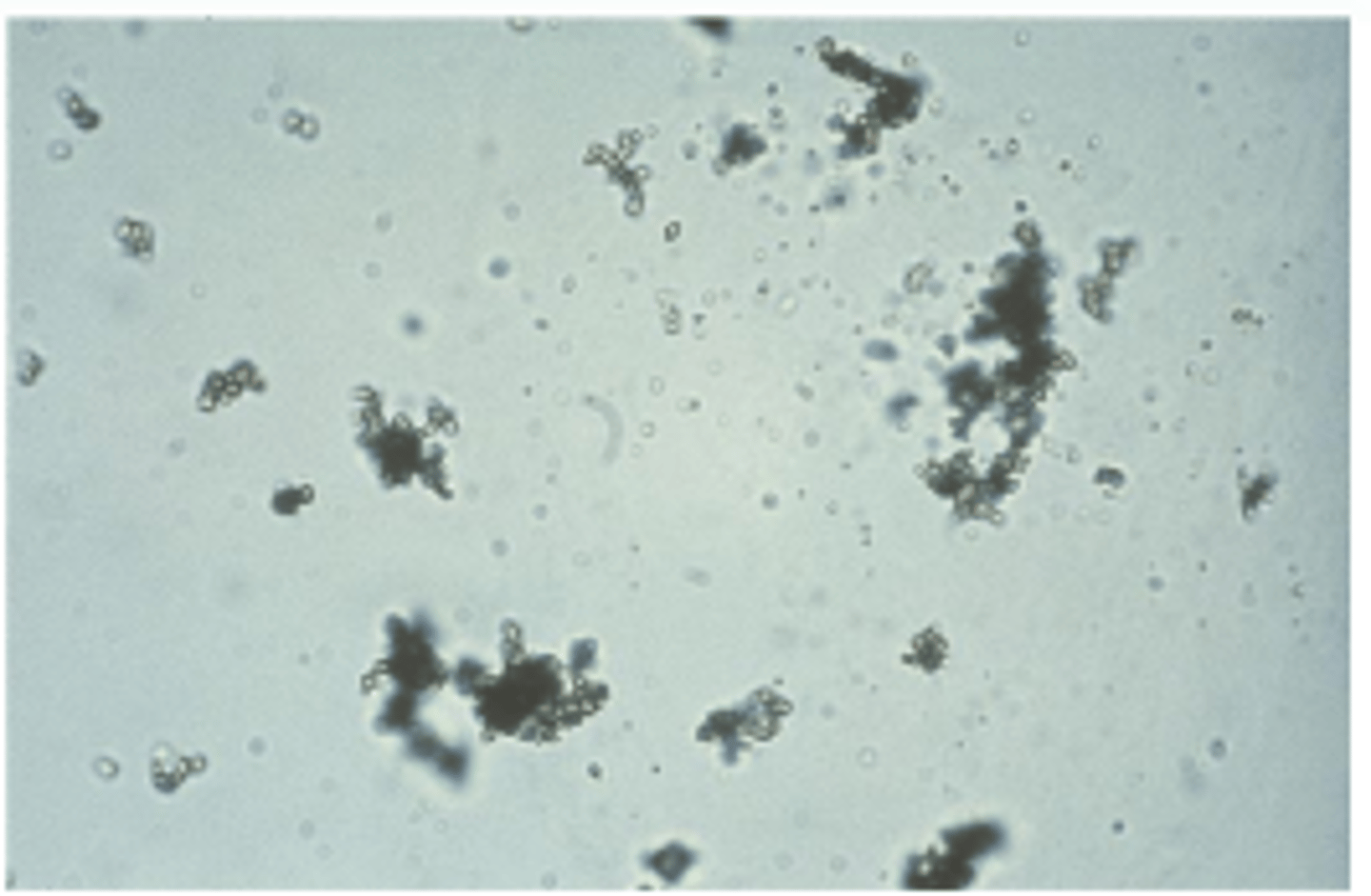
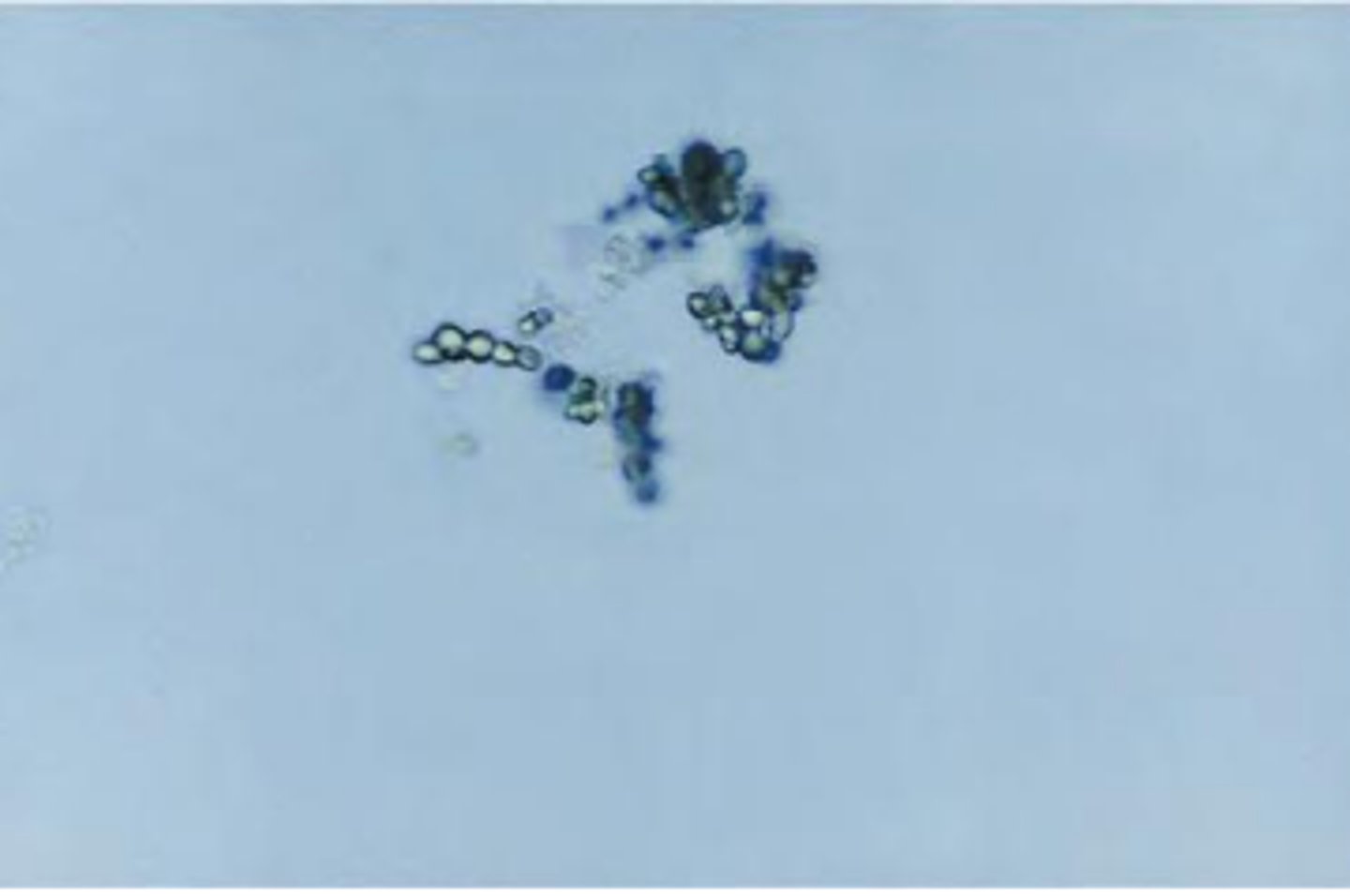
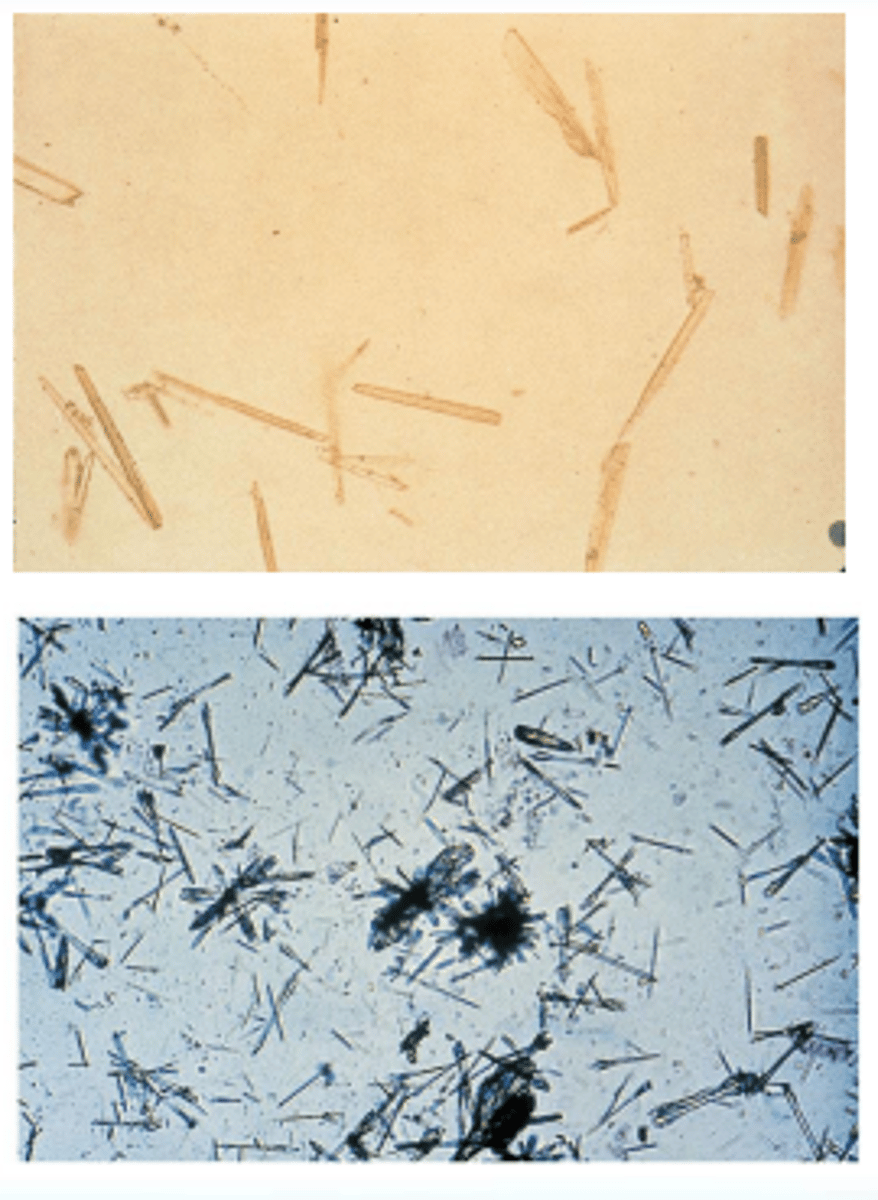
Sulfonamide Crystals
Seen in patient treated for UTI
Possibility of tubular damage if crystals are forming in the nephron
Shapes and Color: needles, rhombics, whetstones, sheaves of wheat, and rosettes with colors ranging from colorless to yellow-brown
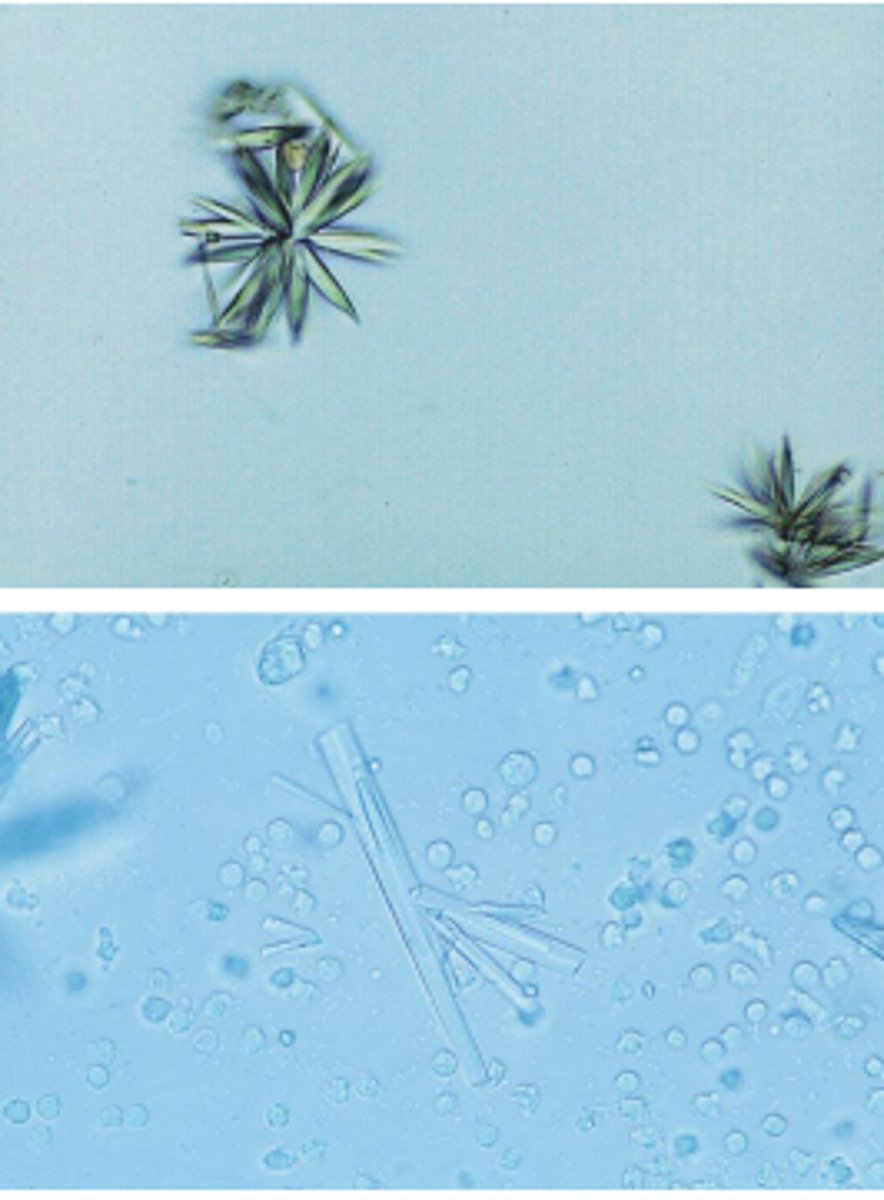
Ampicillin Crystals
Colorless needles that tend to form bundles following refrigeration
Urinary Sediment Artifacts
Material fibers, meat
and vegetable fibers,
and hair
Starch, oil droplets, air
bubbles, pollen grains,
vegetable fiber, hair,
diaper fiber
SULFONAMIDE

AMPICILLIN

URIC ACID
CHOLESTEROL

SULFONAMIDE
CALCIUM OXALATE
TRIPLE PHOSPHATE
TYROSINE
CYSTINE
LEUCINE
AMMONIUM BIURATE
BILIRUBIN