Radiographic Densities and Chest X-Ray Anatomy
1/41
Earn XP
Description and Tags
These flashcards cover essential vocabulary regarding radiographic densities, chest X-ray anatomy, and common terms related to imaging techniques.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
42 Terms
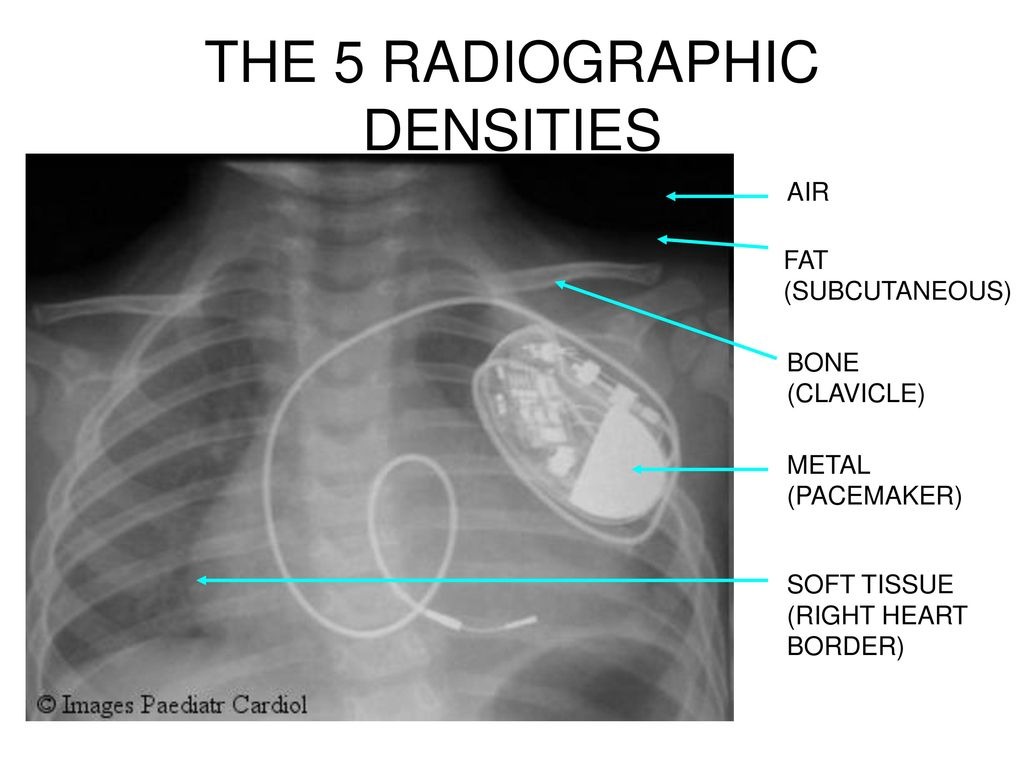
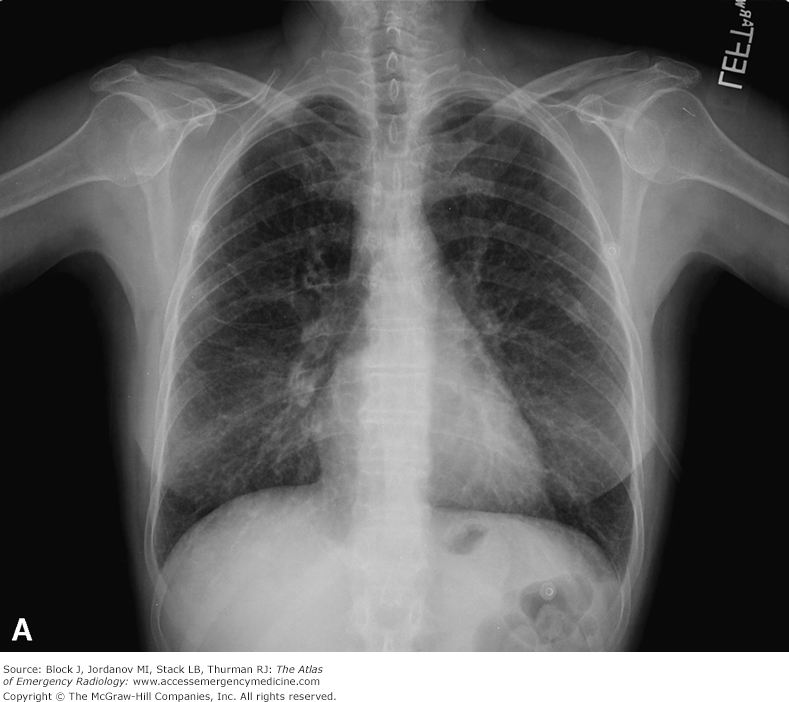
Radiographic Densities
The varying appearances of structures in radiographic imaging based on their density.
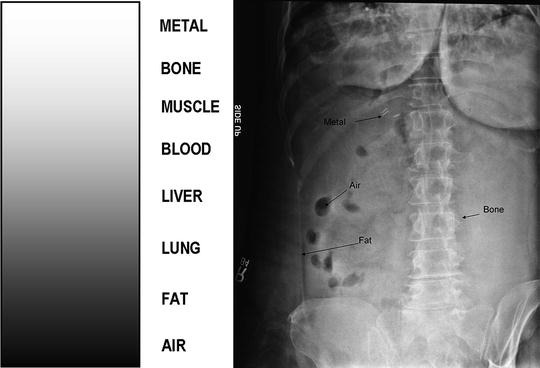
Air Density
The lowest density in radiographic imaging, appearing black on images.
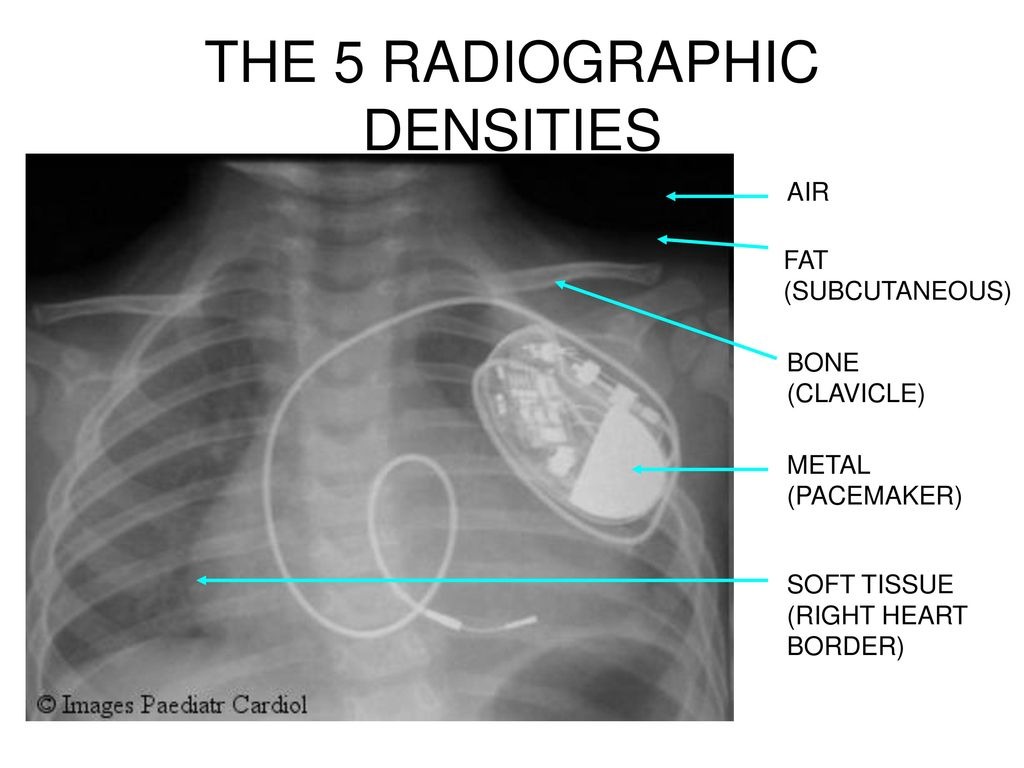
Fat Density
A density level that appears darker than soft tissue on radiographs.
Bone Density
The density that shows up white on radiographs due to high calcium content.
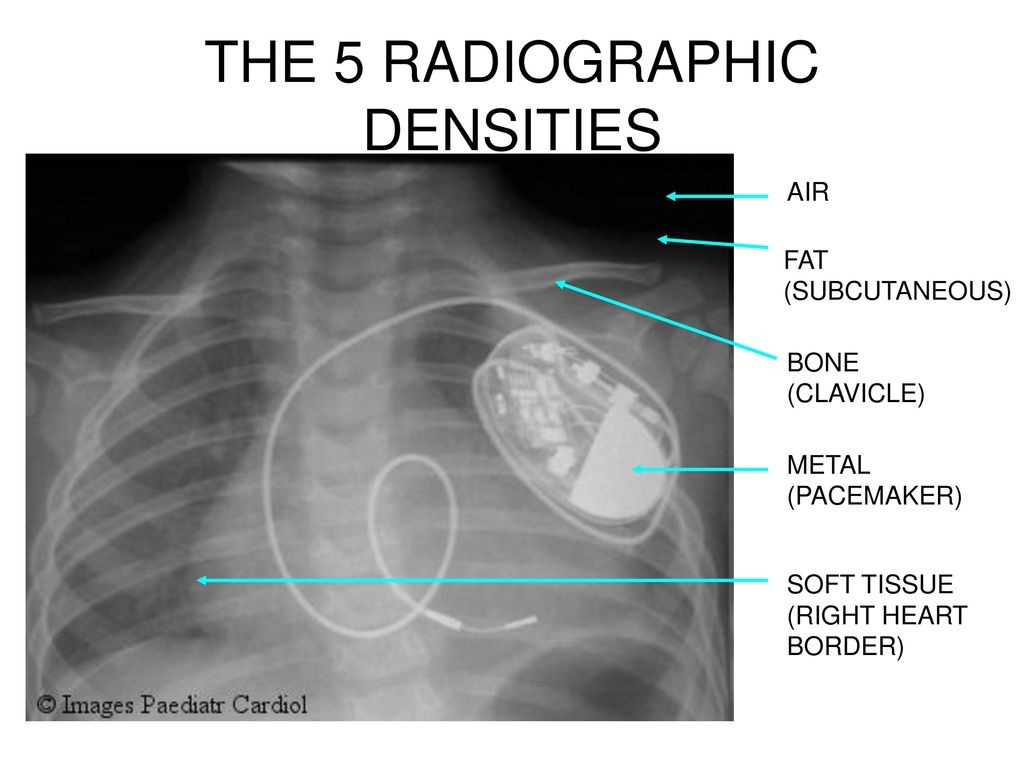
Metal Density
The highest density appearing as bright white on imaging, indicating the presence of metal objects.
Soft Tissue Density
Refers to structures like muscles and organs that appear as shades of gray on radiographs.
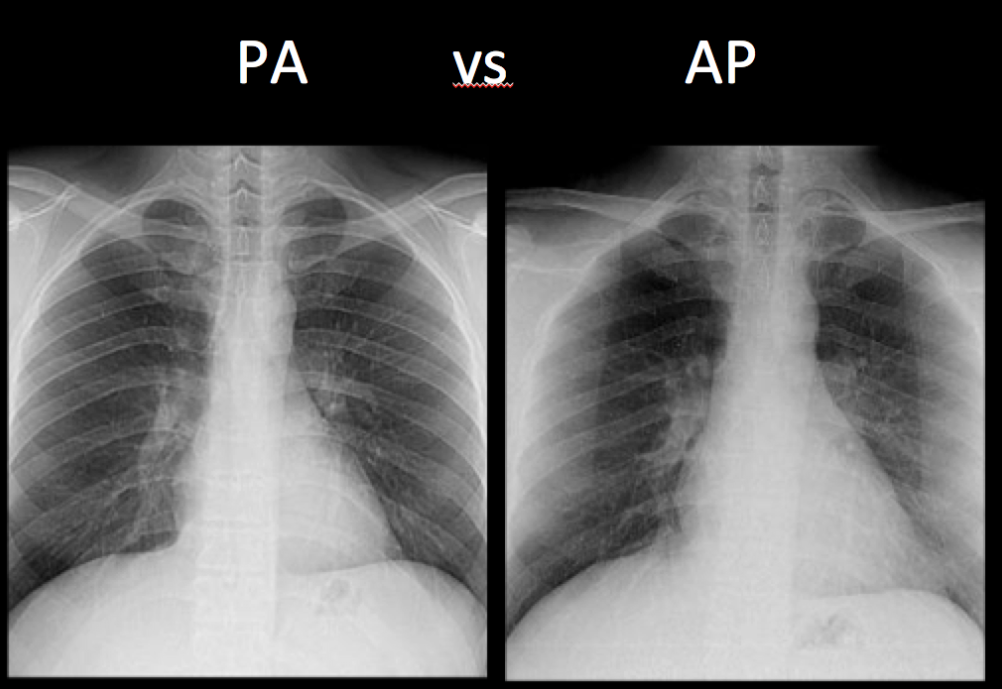
Posteroanterior View (PA)
A standard view for chest X-rays taken with the X-ray beam directed from posterior to anterior.
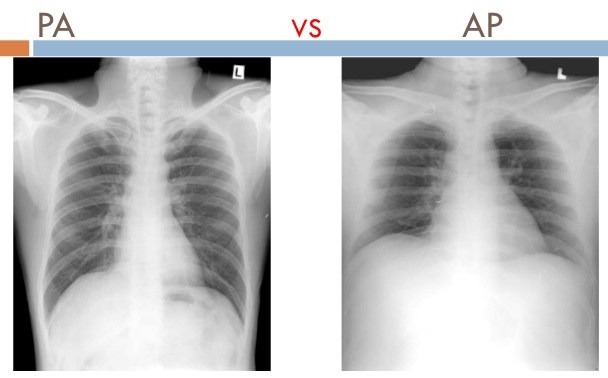
Anteroposterior View (AP)
A chest X-ray view taken with the X-ray beam directed from anterior to posterior.
Trachea
A structure seen on chest X-ray that represents the airway.
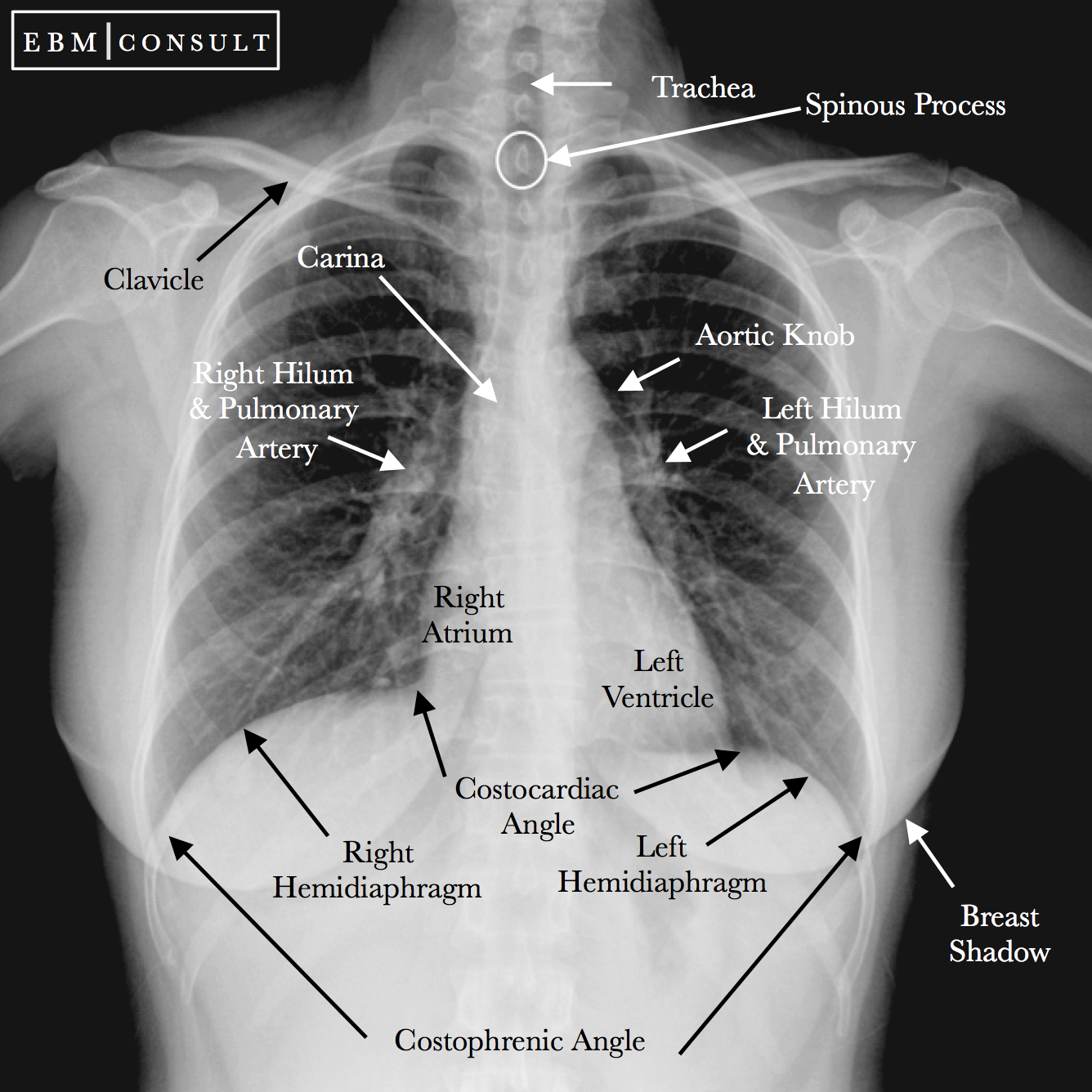
Hila
Areas on a chest X-ray where the lungs' blood vessels enter and exit.
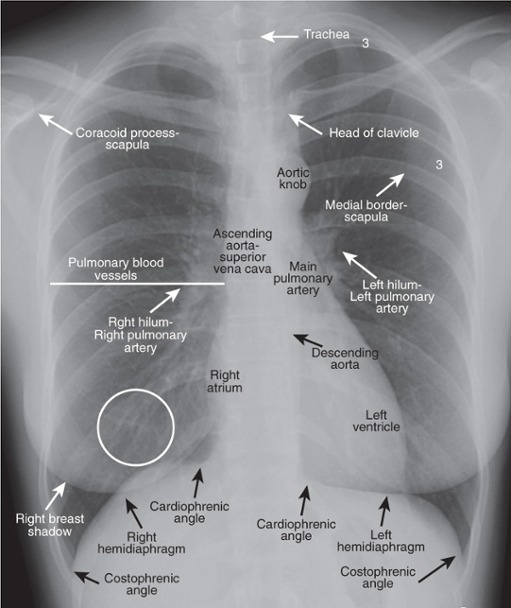
Diaphragm
The muscle seen on chest X-ray that separates the thoracic and abdominal cavities.
Congestive Heart Failure (CHF)
A condition visible on a chest X-ray indicated by enlarged heart size and various vascular patterns.
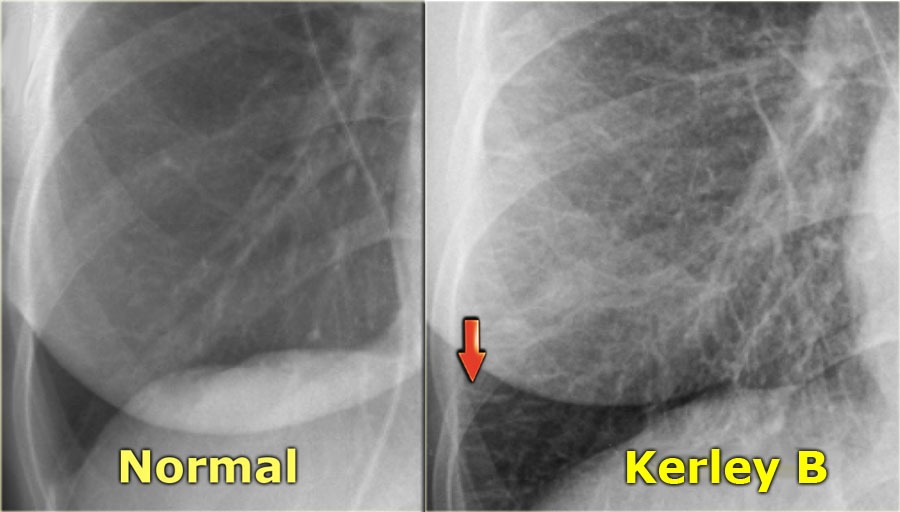
Kerley B lines
Thin linear opacities seen on chest X-ray indicative of interstitial edema.
Aortic Knob
The curved appearance of the aorta as seen in chest imaging.
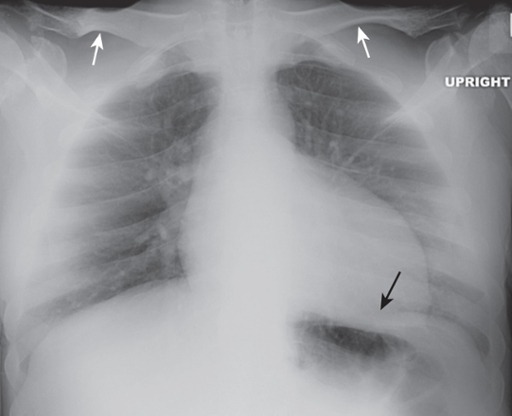
Pneumothorax
Air in the pleural space, leading to potential lung collapse visible on a chest X-ray.
Pleural Effusion
Fluid accumulation in the pleural cavity visible on chest imaging, typically seen at the costophrenic angle.
Aortic Aneurysm
An abnormal dilation of the aorta that can be visualized on chest radiographs.
Endotracheal Tube (ETT)
A tube placed in the trachea to ensure an open airway, visible on X-ray.
Central Venous Catheter (CVC)
A catheter placed in a large vein that can be viewed on radiographs for positioning verification.
Pulmonary Artery Catheter
A type of catheter used to monitor heart function, which should not be kinked or malpositioned as seen on X-ray.
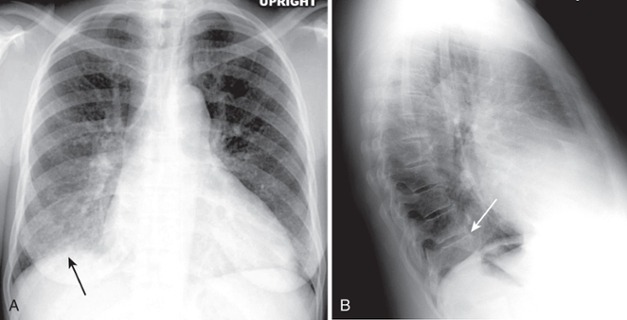
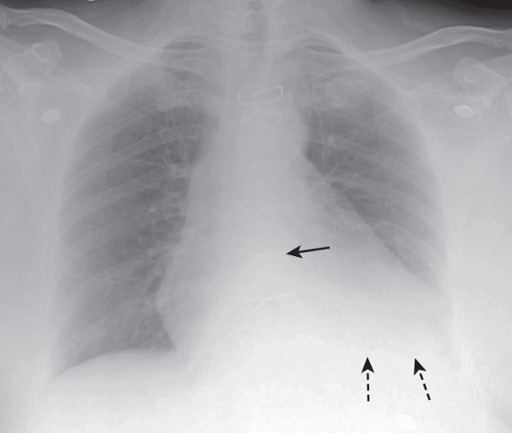
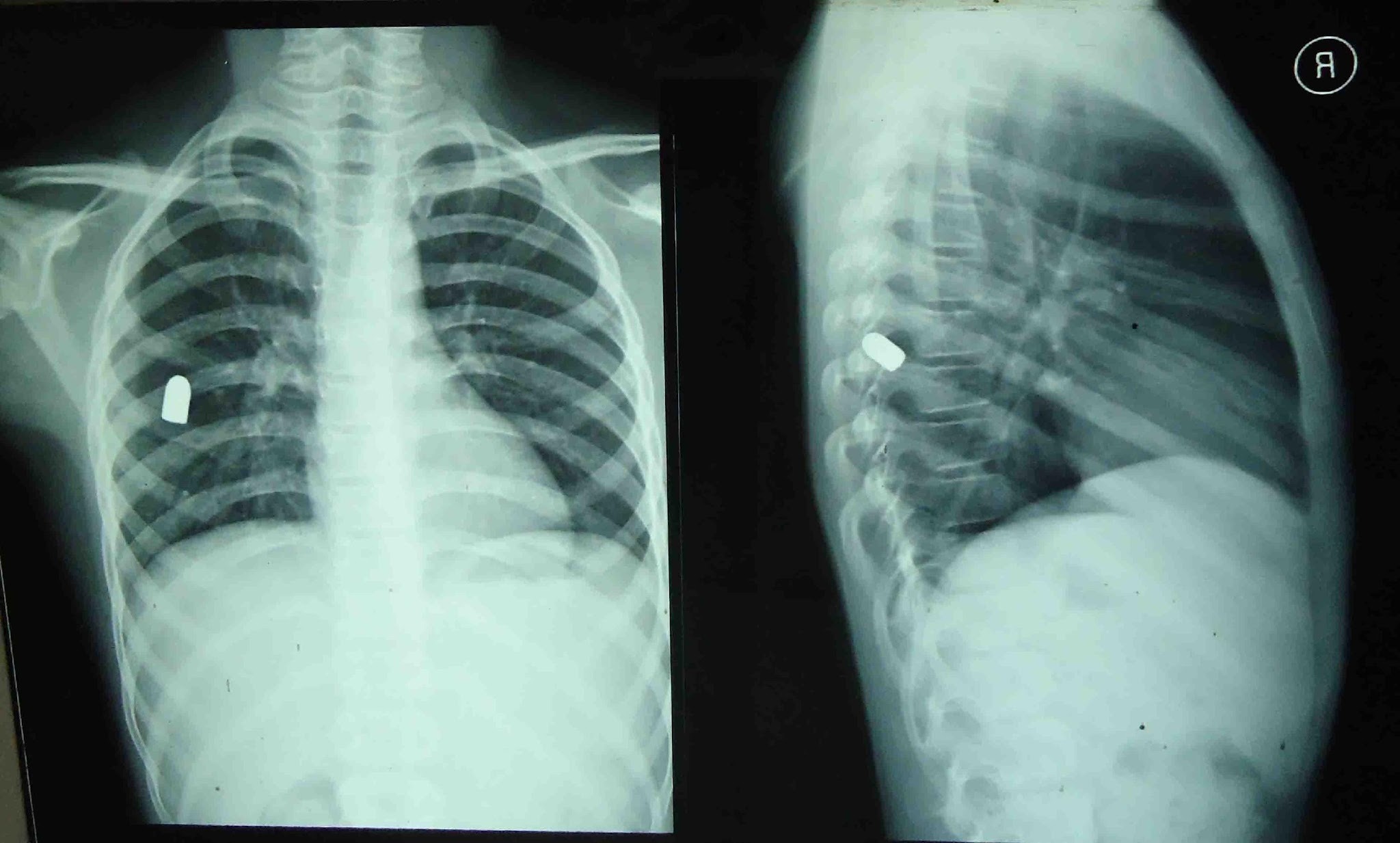
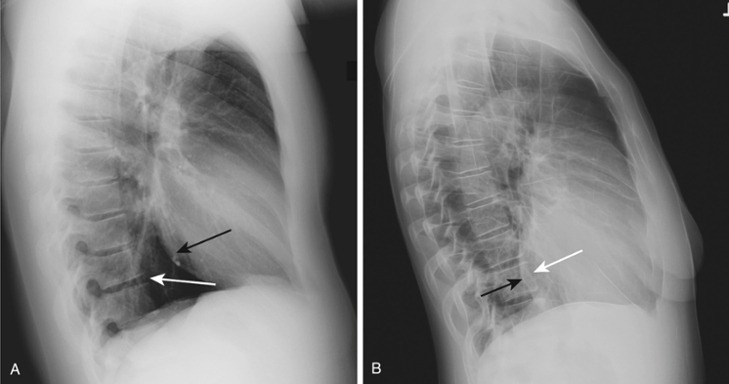
Airspace Disease (pneumonia)
Frontal and lateral views of the chest demonstrate airspace disease on the lateral film (B) in the right lower lobe (white arrow) that may not be immediately apparent on the frontal film (you can see the pneumonia in the right lower lobe in [A] [black arrow]).
In this case, a right lower lobe pneumonia superimposed on the lower spine on the lateral view makes the spine appear “whiter” (more dense) just above the diaphragm. This is called the spine sign.
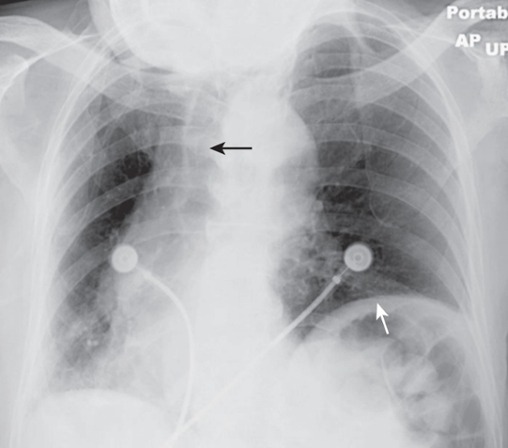
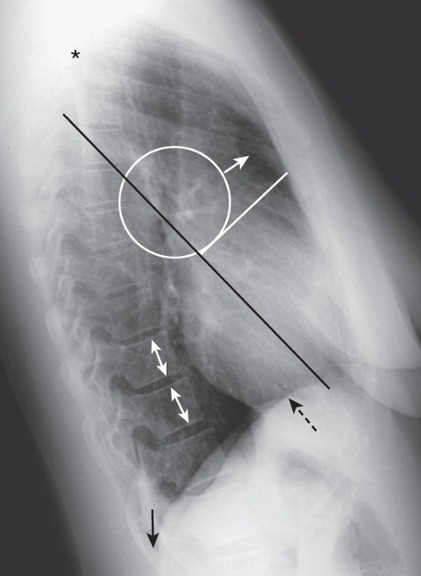
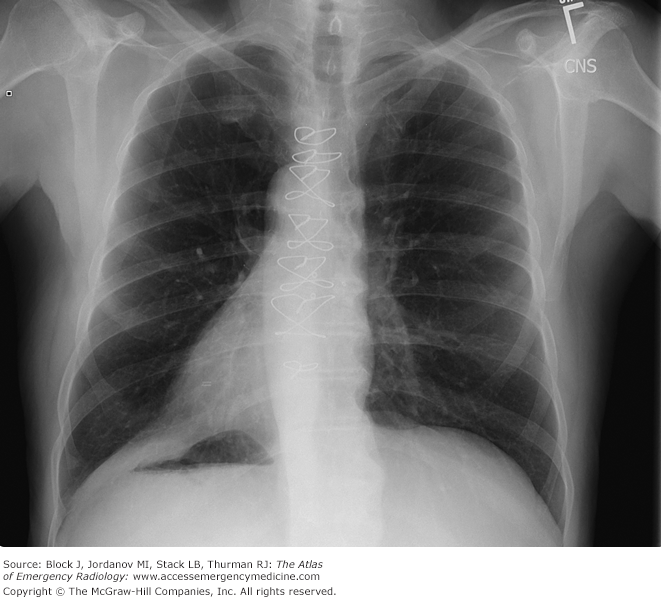
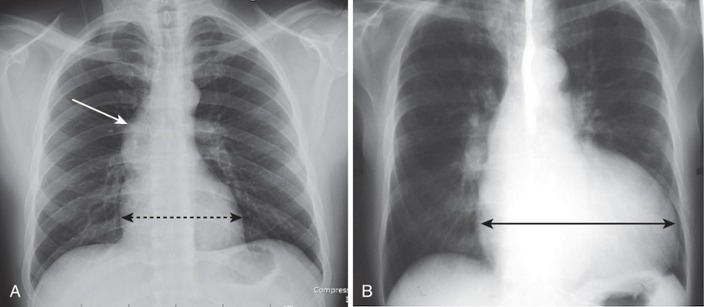
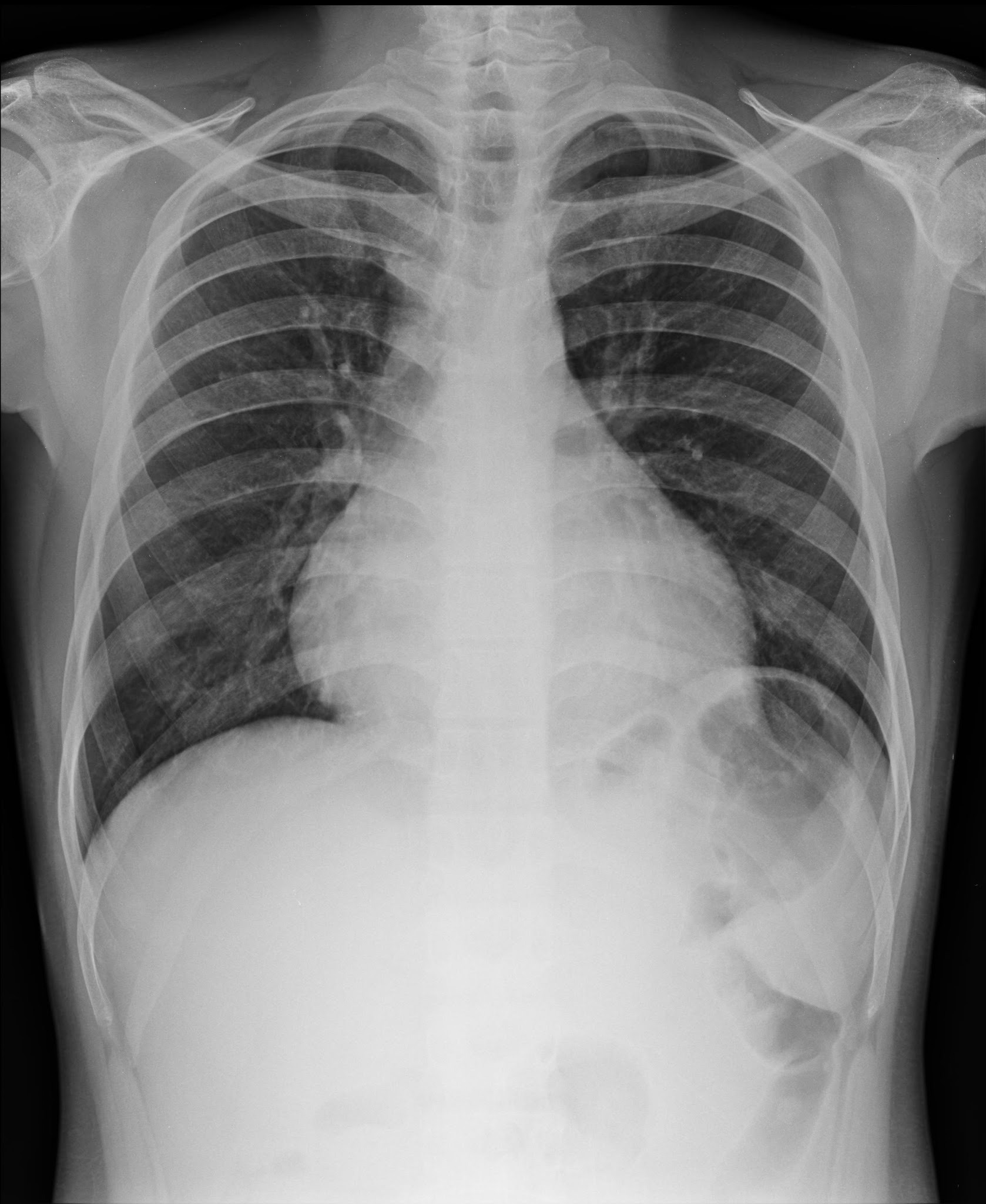
Penetration
The degree of penetration is adequate since we can see the spine (solid white arrows) through the heart.
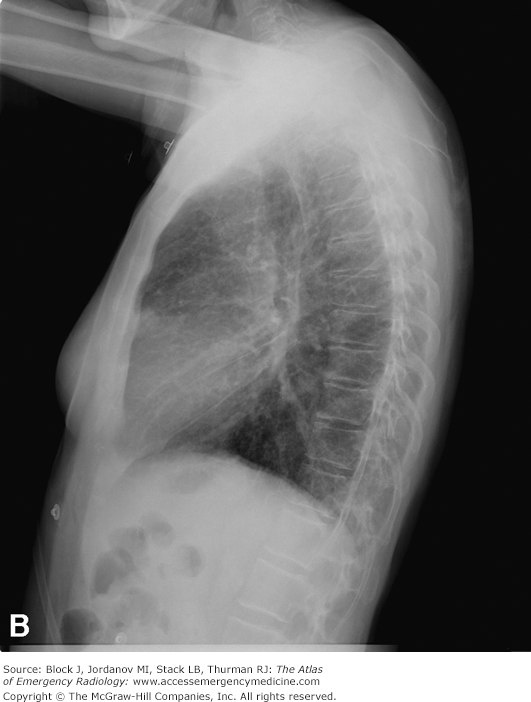
Underpenetration
Underpenetration – cannot see thoracic spine through the heart
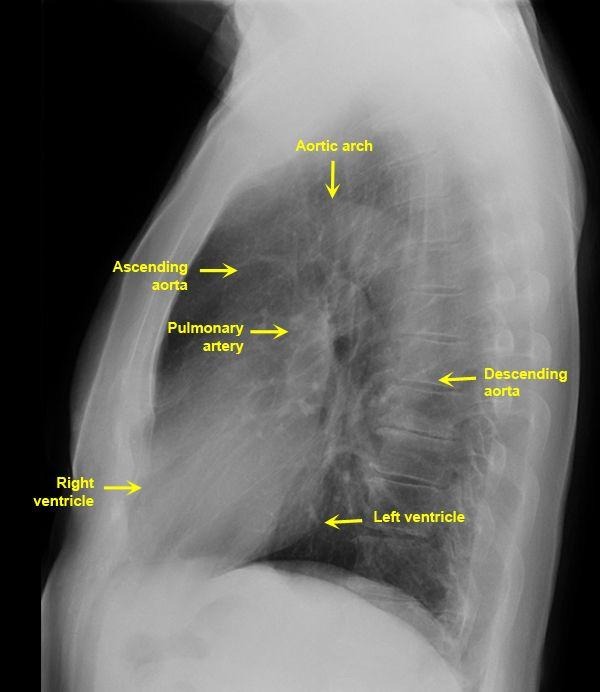
Lateral CXR
Left vent is posterior structure
Right vent is anterior and closest to chest wall
Lateral CXR
Clear space behind the sternum (solid white arrow)
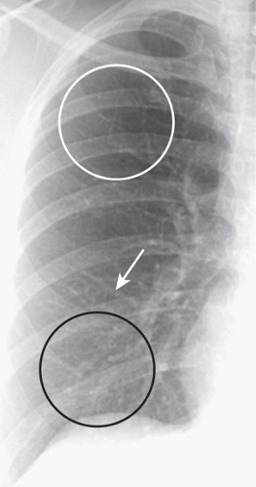
Normal Pulmonary Lung Vasculature
Lung markings. “White lines” are blood vessels (branch and taper gradually from the hill centrally to periphery of lung)
In the upright position, the lower lobe vessels (black circle) are larger in size than the upper lobe vessels (white circle) and all vessels taper gradually from central to peripheral (white arrow)
Over penetration
Too dark and will miss things.
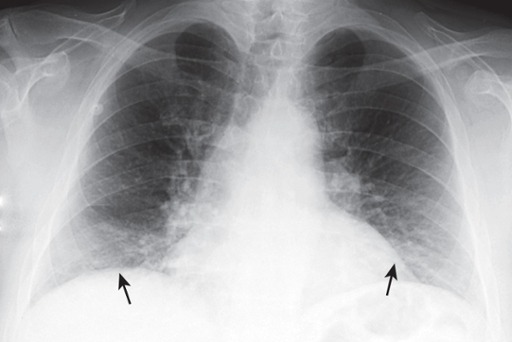
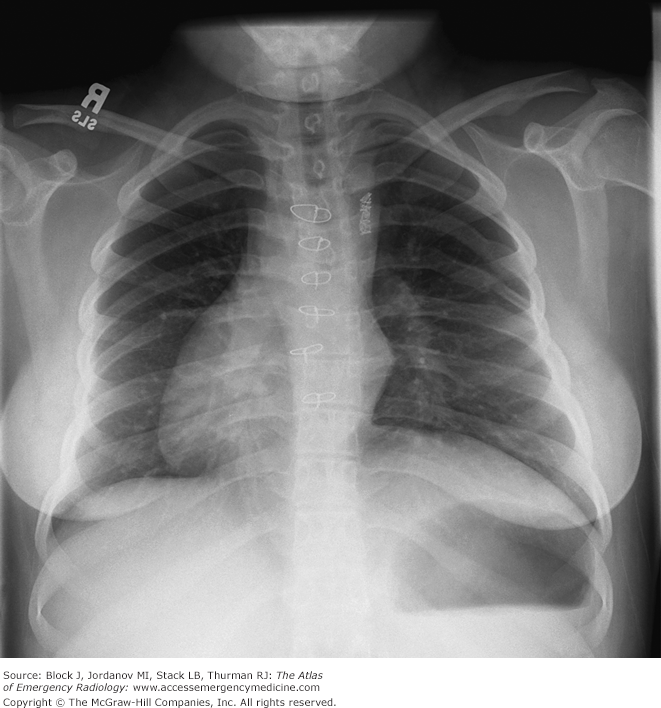
Poor Inspiration
Only eight posterior ribs are visible on this frontal chest radiograph.
A poor inspiration may “crowd” and therefore accentuate the lung markings at the bases (black arrows) and may make the heart seem larger than it actually is.
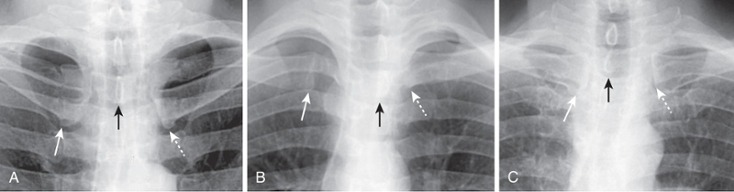
Rotation
Close-up view of the heads of the clavicles demonstrates that each (solid white arrow for right and dotted white arrow for left) is about equidistant from the spinous process of the vertebral body between them (black arrow). This indicates the patient is not rotated.
Close-up view of the heads of the clavicles in a patient rotated toward his own right (remember that you are viewing the study as if the patient were facing you). The spinous process (black arrow) projects much closer to the left clavicular head (dotted white arrow) than to the right clavicular head (solid white arrow).
Close-up view of the heads of the clavicles in a patient rotated toward his own left. The spinous process (black arrow) is much closer to the right clavicular head (solid white arrow) than it is to the left (dotted white arrow).
Example of Rotation
Patient markedly rotated toward her own right. Rotation can distort the appearance of the normal contours of the heart and hila.
Notice how the left hemidiaphragm, being farther from the cassette than the right hemidiaphragm because of the rotation, appears higher than it normally would (white arrow).
The hilum could also appear larger than its actual size because of rotation. The heart and the trachea (black arrow) appear displaced into the right hemithorax because of the rotation.
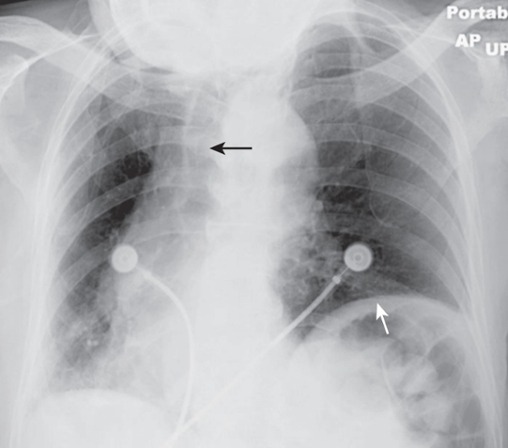
Angulation
An apical lordotic view of the chest is most frequently obtained inadvertently using the portable technique in patients who are semirecumbent because they are bedridden and cannot stand. Notice how the clavicles are projected above the first ribs and their usual “S” shape is now straight (white arrows). The lordotic view also distorts the shape of the heart and produces spurious obscuration of the left hemidiaphragm (black arrow).
Dextroposition
Dextroposition – heart points more to right
Dextrocardia with situs inversus – heart is completely on right side
Situs inversus totalis – heart and all organs are mirrored from normal configuration
Situs inversus totalis
Dextroposition – heart points more to right
Dextrocardia with situs inversus – heart is completely on right side
Situs inversus totalis – heart and all organs are mirrored from normal configuration
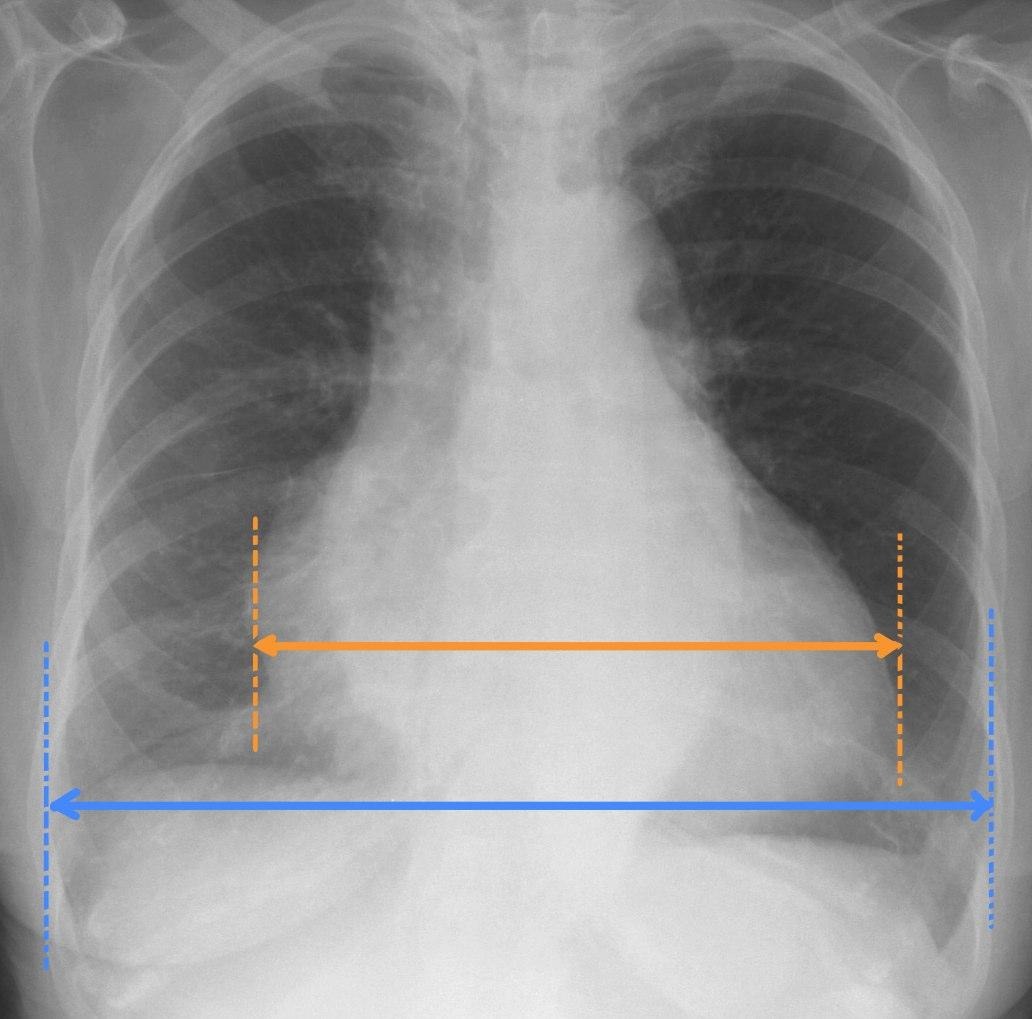
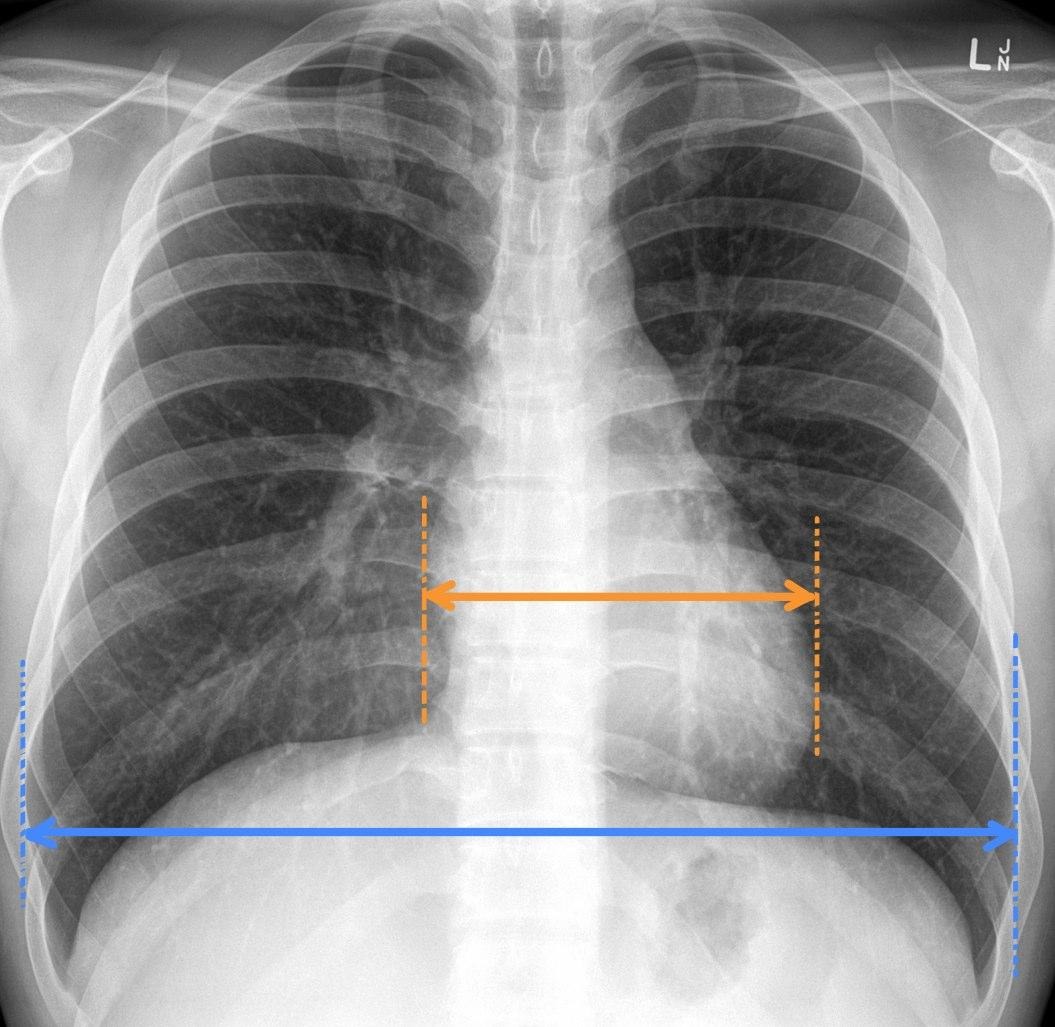
Cardiothoracic ratio
Cardiothoracic ratio: widest transverse diameter of the heart compared with the widest internal diameter of the rib cage (from inside of rib to inside of rib at the level of the diaphragm)
In most normal adults at full inspiration, the cardiothoracic ratio is less than 50%
Normal CT ratio should be less than or equal to 50%
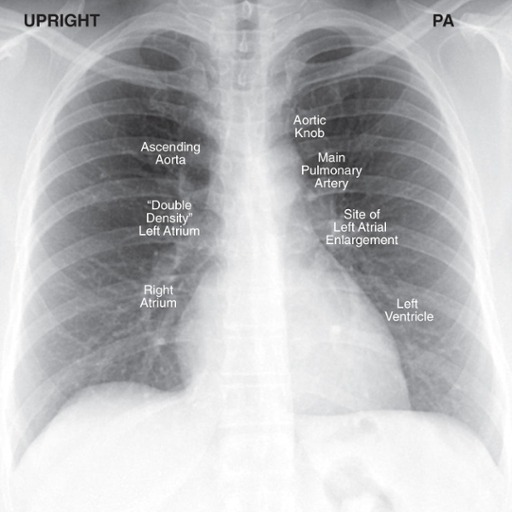
Cardiac Contours
Since we are looking at shadows (knowing the heart is soft tissue density), the silhouette of the heart demonstrates certain contours
Aorta – knob on frontal view
PA – vascular so visible, unlike bronchus; left main sits higher than right
Right and left atria – right atria makes up right heart border; left atria will enlarge superior portion of left heart border
LV – posterior structure; more prominent filling retrocardiac space on lateral
Descending aorta disappears because it is buried in mediastinal soft tissue densities
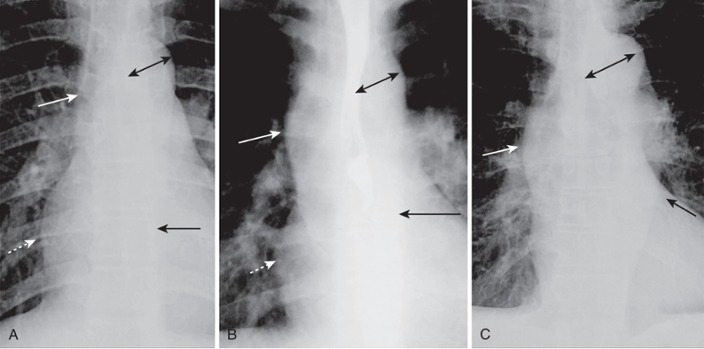
Aortic Contours
Normal
The ascending aorta is a low-density, almost straight edge (solid white arrow)
Does not project beyond the right heart border (dotted white arrow).
The aortic knob is not enlarged (double arrow)
The descending aorta (solid black arrow) almost disappears with the shadow of the thoracic spine
Aortic stenosis
The ascending aorta is abnormal as it projects convex outward (solid white arrow) almost as far as the right heart border (dotted white arrow)
This is secondary to post-stenotic dilatation
The aortic knob (double arrow) and descending aorta (solid black arrow) remain normal.
Systemic hypertension
Both the ascending (solid white arrow) and descending aorta (solid black arrow) project too far to the right and left, respectively
The aortic knob is enlarged (double black arrow)
Cardiothoracic ration
Cardiothoracic ratio: widest transverse diameter of the heart compared with the widest internal diameter of the rib cage (from inside of rib to inside of rib at the level of the diaphragm)
In most normal adults at full inspiration, the cardiothoracic ratio is less than 50%
Normal CT ratio should be less than or equal to 50%
Cardiac Remodeling
Cardiomegaly - enlargement of the cardiac silhouette produced by ventricular enlargement

Pericardial Effusion
Pericardial effusion is fluid within the pericardium; Normal 15 to 50 mL of fluid in the pericardial space between the parietal and visceral pericardial layers, just enough to prevent friction
The heart is not enlarged, but the silhouette appears that way
Accumulation starts in dependent portions of the pericardial space in the supine position
Subsequent fluid collects along the right heart border until it fills the pericardial space and encircles the heart
“Water bottle” sign
Cardiac Enlargement
The heart should not encroach on the spine; retrocardiac clear space
Cardiac silhouette should not extend posteriorly project over the spine
CHF
(CHF) Congestive heart failure typically presents with one of two radiographic patterns:
pulmonary interstitial edema
pulmonary alveolar edema
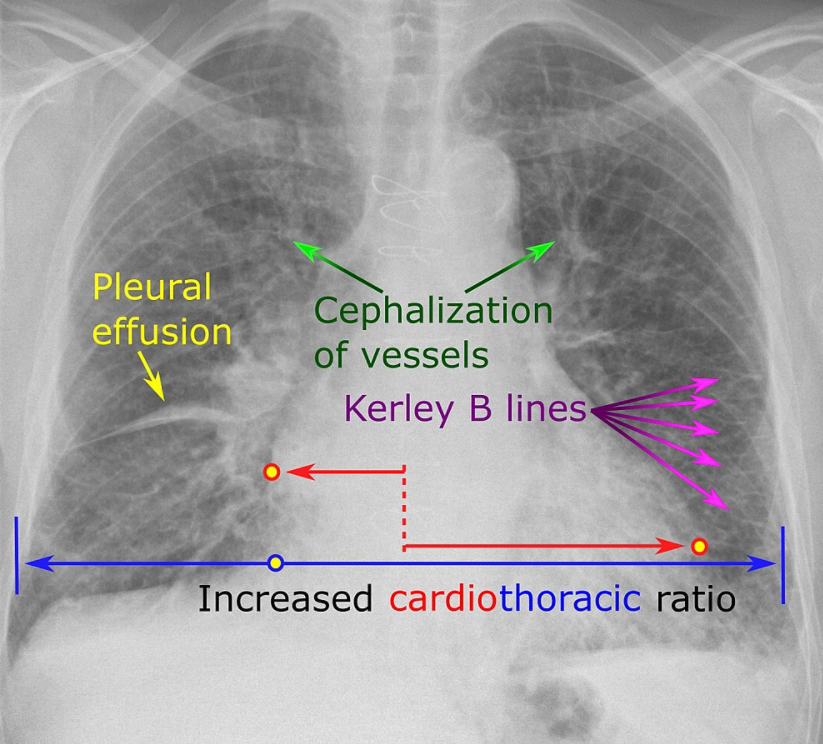
CHF Interstitial Findings
Four Key Findings in Pulmonary Interstitial Edema:
Thickening of the interlobular septa—Kerley B lines—and fluid in the central connective tissue of the lungs—Kerley A lines
Peribronchial cuffing: fluid-thickened bronchial walls visualized on-end
Fluid in the fissures: opacification and thickening of the interlobar fissures
Pleural effusion: usually bilateral but, when unilateral, usually right-sided