SMED UNIT 6- HEAD AND NECK
5.0(1)
Card Sorting
1/66
Study Analytics
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
67 Terms
1
New cards
PEARL
pupil equal and reactive to light
2
New cards
Cranial nerves
12 nerve pairs that begin in areas of the brain. They are designated by number and name
3
New cards
Cognitive testing
study the effects of head trauma on cognitive function (mental processes that allow us to carry out common tasks)
4
New cards
Alert
awake and responds immediately and appropriately
5
New cards
confused
impaired memory, disorientation and confusion
6
New cards
Lethargic
drwosy yet easily arouswed, oriented to persono, place and time
7
New cards
Stuporous
asleep most of the time, difficult to arouse, responds inappropriately
8
New cards
Semicomatose
no response to verbal stimuli, some response to painful stimuli
9
New cards
comatose
no response
10
New cards
epistaxis
bloody nose
11
New cards
anterograde amnesia
length of time from injury until conscious memory returns
12
New cards
retrograde amnesia
loss of memory of events that occurred before the injury
13
New cards
immediate recall
can recite 4-5 words or numbers right after you say them
14
New cards
Tinnitus
ringing in the ears
15
New cards
Rhomberg’s test
balance testing for intracranial damage
16
New cards
Diplopia
double vision
17
New cards
Acronym for cranial nerves…
On Old Olympus Towering Tops, A Finn And Greek Viewed Some Hops
18
New cards
Olfactory
Smell (I)
19
New cards
Optic
vision (II)
20
New cards
Oculomotor
eye movement, constriction of pupil (III)
21
New cards
Trochlear
eye movement (IV)
22
New cards
Trigeminal
head and face sensation (V)
23
New cards
Abducens
lateral movement of the eye (VI)
24
New cards
Facial
taste, facial movements (VII)
25
New cards
Acoustic
hearing and equilibrium (VIII)
26
New cards
Glossopharyngeal
swallowing (IX)
27
New cards
Vagus
speech (X)
28
New cards
Spinal Accessory
movement of neck and spine (XI)
29
New cards
Hypoglossal
movement of the tongue (XII)
30
New cards
Skull Fracture
Blunt trauma to head.
S/S- blood and/or CSF in ear or nose, severe headache, nausea, skin indentation
T/X- 911
S/S- blood and/or CSF in ear or nose, severe headache, nausea, skin indentation
T/X- 911
31
New cards
Concussion
Direct or indirect trauma to head
S/S- confusion, headache, dizziness, trouble concentrating, abnormal pupil response
T/X- take out of play, determine LOC, watch for symptoms to worsen
S/S- confusion, headache, dizziness, trouble concentrating, abnormal pupil response
T/X- take out of play, determine LOC, watch for symptoms to worsen
32
New cards
Intracranial Hemorrhage
Blow to head (may be a slow bleed)
S/S- show signs of mild headache but then has sever head pains, dizziness, nausea, unequal pupils.
TX- referral to the ER
S/S- show signs of mild headache but then has sever head pains, dizziness, nausea, unequal pupils.
TX- referral to the ER
33
New cards
Epidural Bleeding (FAST)
blow to the head
S/S- extremely fast bleeding, arterial. (in 10-20 min the athlete will go grom fine to having major symptoms
TX- ER, surgery
S/S- extremely fast bleeding, arterial. (in 10-20 min the athlete will go grom fine to having major symptoms
TX- ER, surgery
34
New cards
Subdural Bleeding
__Veins__ are torn that bridge the dura mater to the brain (Contrecoup)
S/S- bleeding is slow, s/s may not appear for hours
TX- 911 after s/s appear
S/S- bleeding is slow, s/s may not appear for hours
TX- 911 after s/s appear
35
New cards
Countercoup
occurs at site opposite of impact
36
New cards
Intracerebral bleeding
Force trauma to being (bleeding within the brain)
S/S- deterioration of neurological function
TX- 911, ER
S/S- deterioration of neurological function
TX- 911, ER
37
New cards
Post Concussive Syndrome
Happens after head injury
s/s- impaired memory, lack of concentration, anxiety, depression
TX- may not return to play until symptoms are gone and have been cleared by a health care provider
s/s- impaired memory, lack of concentration, anxiety, depression
TX- may not return to play until symptoms are gone and have been cleared by a health care provider
38
New cards
Second impact Syndrome
Second head injury before S/S of initial injury go away ( caused 50 deaths over the last decade)
S/S- appear stunned, within short time athlete may collapse, dilated pupils, loss of eye movement, respiratory failure.
TX- prevention
S/S- appear stunned, within short time athlete may collapse, dilated pupils, loss of eye movement, respiratory failure.
TX- prevention
39
New cards
Chronic Traumatic Encephalopathy (CTE)
Repetitive blows to the head (progressive degenerative brain disease
S/S- depression, mood changes, impulse control problems (eventually causes dementia)
TX- no cure
S/S- depression, mood changes, impulse control problems (eventually causes dementia)
TX- no cure
40
New cards
Cerebellum (SMALL)
Motor function, balance, posture
41
New cards
Cerebrum (LARGEST)
Voluntary movements
Sensory
Motor functions
Consciousness depends on excitation of the cerebral cortex
Sensory
Motor functions
Consciousness depends on excitation of the cerebral cortex
42
New cards
Cerebrospinal fluid
between arachnoid and pia mater (subarachnoid space)
\-Suspends brain
\-Cushions it from shock
\-Suspends brain
\-Cushions it from shock
43
New cards
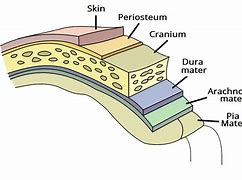
Meninges (4 LAYERS)
Dura Mater- Dense, inelastic, outermost matter
Arachnoid membrane- thin, delicate membrane, attached to the spinal cord by small tissue strands
Subarachnoid space- in between the arachnoid and the pia mater. Helps contain the spinal fluid
Pia Mater- innermost layer
Arachnoid membrane- thin, delicate membrane, attached to the spinal cord by small tissue strands
Subarachnoid space- in between the arachnoid and the pia mater. Helps contain the spinal fluid
Pia Mater- innermost layer
44
New cards
Cranium consists of large FLAT bones…
Frontal, Occipital, 2 Sphenoid, 2 Parietal, 2 Temporal
45
New cards
Brainstem
Medulla- heart, lungs motor
Pons and midbrain- reflexes
Pons and midbrain- reflexes
46
New cards
Hops (Questions)
Note length of time unconscious for
Alert-comatose
Headache- Location, type
Memory- immediate recall, recent memory
QUESTIONS-
* Do you know where you are
* What happened
* Does your head hurt
* Do you have pain in your neck
* can you move your hands and feet
\
Alert-comatose
Headache- Location, type
Memory- immediate recall, recent memory
QUESTIONS-
* Do you know where you are
* What happened
* Does your head hurt
* Do you have pain in your neck
* can you move your hands and feet
\
47
New cards
hOps
obvious deformity
slurred or incoherent speech
gross disturbance in coordination
length of time athletes affects abnormal
swelling or bleeding from scalp
discoloration
disorientation
delayed verbal and motor responses
slurred or incoherent speech
gross disturbance in coordination
length of time athletes affects abnormal
swelling or bleeding from scalp
discoloration
disorientation
delayed verbal and motor responses
48
New cards
hoPs
-skull deformity
\-open wounds
\-palpate both neck and skull
\-open wounds
\-palpate both neck and skull
49
New cards
hopS
BALANCE TESTS-
Rhomberg (stand with eyes closed, single leg and tandem stance)
BESS (balance error scoring system)
COORDINATION TESTS-
finger to nose
heel-to-toe walk
heel to knee test
CONGITIVE TESTS-
count backwards from 100 by 7
spelling a word backwards
3 word recall
name the months in reverse order
Rhomberg (stand with eyes closed, single leg and tandem stance)
BESS (balance error scoring system)
COORDINATION TESTS-
finger to nose
heel-to-toe walk
heel to knee test
CONGITIVE TESTS-
count backwards from 100 by 7
spelling a word backwards
3 word recall
name the months in reverse order
50
New cards
Special Tests (neurological exam)
Cerebral testing- cognitive function
Cranial nerve testing- rule out isolated injury
Cerebellar testing- coordination and motor function
Sensory testing- dermatomes
Reflex testing
Cranial nerve testing- rule out isolated injury
Cerebellar testing- coordination and motor function
Sensory testing- dermatomes
Reflex testing
51
New cards
CAM Log
Cognitive Activity Monitoring Log
52
New cards
What is the first step in any concussion management plan
the institution of both physical and cognitive rest
53
New cards
What does cognitive rest possibly include?
no school attendance, no home/school work, no reading, no video games, no texting, no computer time, and no television
54
New cards
mTBI
mild traumatic brain injury
55
New cards
RTL
return to learn
56
New cards
when should you stop the cognitive activity when returning from a brain injury
after mild symptoms develop and before severe symptoms develop
57
New cards
Idaho concussion law is under house bill NO.
577
58
New cards
what are the stages of the symptoms monitoring tool or RTL plan
1. NO activity
2. Gradual reintroduction of cognitive activity
3. Homework at home before schoolwork at school
4. School re-entry
5. Gradual reintegration into school
6. Resumption of full cognitive workload
59
New cards
Home care OK TO
ice pack for head and neck, eat light diet, go to sleep, rest, tylenol
60
New cards
Home care NO NEED TO
check eyes with flashlight, wake up every hour, test reflexes, stay in bed
61
New cards
Home care DO NOT
drink alcohol, eat spicy foods, drive
62
New cards
Gradual RTP Protocol
Step 1- light aerobic exercise
Step 2- Sport specific exercise
Step 3- noncontact training drills and resistance training.
Neurocognitive test=
PASS- non contact training drills and resistance training
FAIL- retake in 48 hours
Step 4- full contact practice
Step 2- Sport specific exercise
Step 3- noncontact training drills and resistance training.
Neurocognitive test=
PASS- non contact training drills and resistance training
FAIL- retake in 48 hours
Step 4- full contact practice
63
New cards
Each step of RTP is….
a full 24-hour period. if symptoms return athlete drops back one level
64
New cards
External occipital protuberance
bump of knowledge
65
New cards
Where is CSF
between arachnoid and pia mater
66
New cards
What does CSF do
suspends brain, and cushions it from shock
67
New cards
Meninge layers