PALATE DEVELOPMENT
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
developed palate
initially the nasal cavity and oral cavity are continuous
when developed, the palate separates the nasal cavity from the oral cavity
developed palate comprised of
hard bony portion
soft (soft tissue) portion
hard palate
anterior aspect of palate
bony portion (maxilla and palatine bones)
soft palate
posterior aspect of palate
mobile and comprised of muscle fibers covered by mucous membrane
posteriorly has a central process that is the uvula
primary palate begins to
develop early in week 6
first, medial nasal prominences merge to form intermaxillary segment
intermaxillary segment gives rise to
labial component
upper jaw component
palatal component
labial component
forms the philtrum of the upper lib
upper jaw component
carries the 4 incisors
palatal component
forms the triangular primary palate
primary palate
portion of palate that is anterior and midline (premaxillary portion of the maxilla)
small portion that is anterior to incisive foramen
also early in week 6, the secondary palate
begins to develop
max prominences expand medially and give rise to
projections called palatal shelves (or lateral palatine processes)
at first, palatal shelves are directed
obliquely inferior
after palatal shelves are directed obliquely inferior, they advance
medially and fuse at midline to form the secondary palate
secondary palate
develops into the majority (remaining portions) of the hard and all of soft palate
of the secondary palate, the palatal shelves (lateral palatine processes) initially project
infero-medially on each side of the tongue
during week 7 and 8, the palatal shelves
ascend and assume a horizontal position
after palatal shelves have ascended, tongue is
now inferior to palate
orofacial clefts
cleft lip
cleft palate
cleft lip and palate
most common oromaxillofacial anomalies
cleft lip
when portions of the lip fail to fusec
cleft palate
when portions of the palate fail to fuse
soft palate only
hard and soft palate, but secondary palate only
primary and secondary palates, includes lip
cleft lip and palate
when these clefts occur together, rather than in isolation
classified as anterior vs posterior cleft defects
incisive foramen is dividing landmark
cleft can occur
unilaterally or bilaterally
median cleft lip
medial nasal prominences fail to fuse in midline to form the philtrum portion of the IM segment
unilateral or bilateral cleft lip
max prominence fails to fuse with medial nasal prominence
unilateral or bilateral oblique facial cleft
max prominence fails to fuse with medial and lateral nasal prominences
cleft extends onto face
anterior cleft defect
cleft in palate and/or lip structures anterior to the incisive foramen (unilateral or bilateral)
cleft lip only
cleft primary palate and cleft lip
posterior cleft defect
clefts in palate posterior to incisive foramen
clefts of the secondary palate
complete cleft defect
combination of anterior and posterior cleft defects
orofacial cleft repair
surgery improves the ability to eat/drink, breathe, hear, and speak
cleft lip surgery (cheiloplasty)
to close the lip and improve symmetry of lip/nose
cleft palate surgery (palatoplasty)
to close the opening between the nasal and oral cavity
create a palate that works well for speech
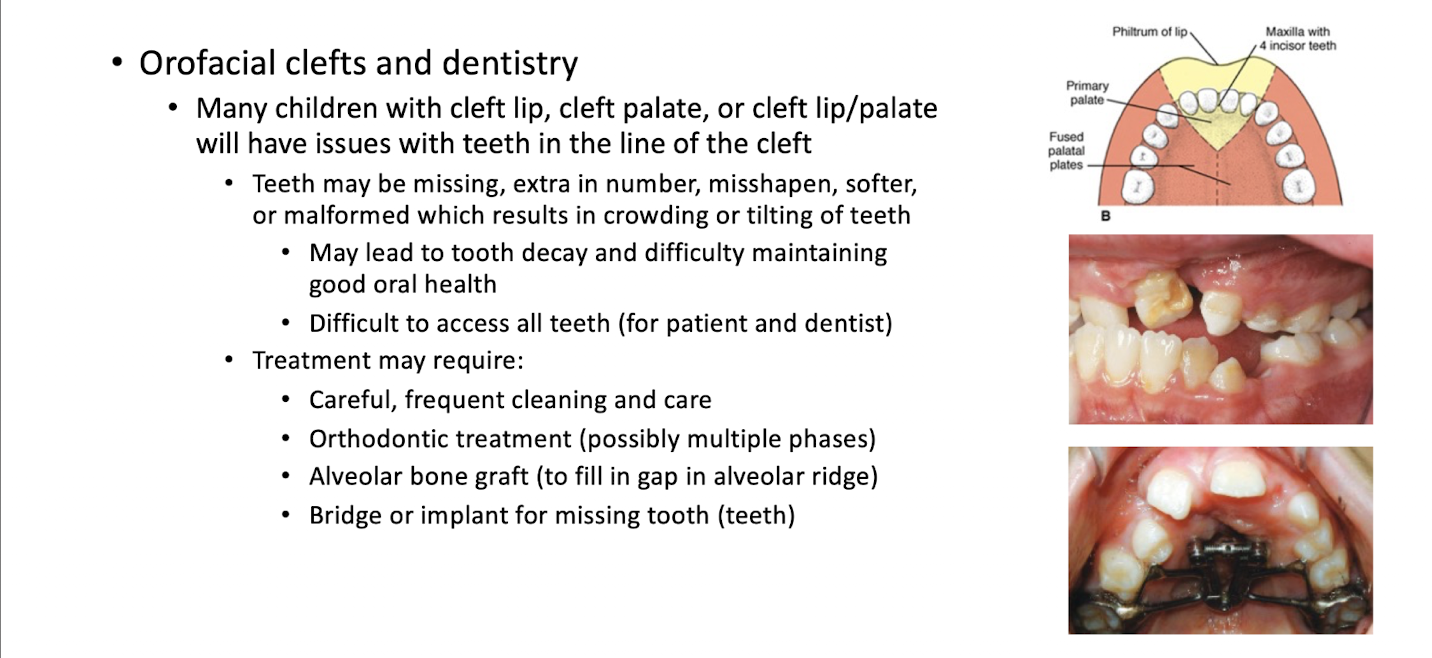
orofacial clefts and dentistry
developed nose portions
external nose
nasal cavity
developed nose boundaries
anterior - nares (nostrils)
posterior - choanae (opening/doorway between the nasal cavity and nasopharynx)
divide at midline by nasal septum
by the end of embryo week 4, nasal placodes develop on
each side of the frontonasal prominence
margins of the placodes proliferate
producing a horseshoe shaped elevation surrounding the nasal placode
lateral nasal prominence
medial nasal prominence
after proliferation of placode margins, nasal placodes now in a depression called
nasal pits
5 facial prominences that give rise to the external nose continue to grow and shape nose
frontal prominence - gives rise to the root
merged medial nasal prominences - form the crest and apex (tip)
lateral nasal prominences - form the alae (sides)
during the embryo 6th week, the nasal pits deepen considerably
partly due to growth of the surrounding medial and lateral nasal prominences
partly due to nasal pits penetration into the underlying mesenchyme and formation of primordial nasal sacs
each nasal sac grows dorsally (ventral to developing forebrain)
at first, the oronasal membrane separates the
nasal sacs from the oral cavity
by the end of embryo week 6, oronasal membrane ruptures
nasal and oral cavities are in communication by way of primitive choanae
choanae lie on each side of midline, posterior to primary palate
later, the choanae are pushed posteriorly with further development of secondary palate
will then be located at junction of nasal cavity and pharynx
nasal septum (midline structure separating nasal cavity into L and R cavities) grows
inferiorly
by embryo week 12, the nasal septum fuses
with the newly formed palate
choanal atresia
failure of the oronasal membrane to rupture
results in congenital narrowing of the back of the nasal cavity
causes difficulty breathing
unilateral or bilateral
unilateral - mild symptoms, can go unidentified at birth
bilateral - emergency, requires surgery
choanal atresia also often associated with other developmental anomalies including CHARGE syndrome
genetic syndrome (autosomal dominant) that affects many areas of the body
CHARGE
coloboma (iris defect(
heart defects
atresia (choanal)
slowed growth
genital anomalies
ear anomalies
developed paranasal sinuses
air filled cavities within the bones of the skull
frontal sinuses
maxillary sinuses
ethmoid air cells (sinuses)
sphenoid sinus
role in humidifying and heating air, speech sounds, reduce weight of skull
paranasal sinuses develop
as outgrowths from the walls of the nasal cavities
independently on differing timelines
paranasal sinuses extend into bones of same name to become
pneumatic (air-filled) extensions of the nasal cavities
paranasal sinus growth
alters shape of face during infancy/childhood
adds resonance to voice during adolescence
maxillary sinuses begin to develop as
spaces during late fetal life
very small at birth (pea-sized)
grows slowly until puberty
may continue to increase in size throughout lifetime
frontal, sphenoid, and ethmoid air cells (sinuses) develop as
spaces soon after birth
ethmoid air cells (sinuses)
small before the age of 2 yrs
begin to grow more rapidly at 6-8 yrs
frontal sinuses
rapid growth between puberty and adulthood
typically stops growing around 25 years of age
sphenoid sinus
rapid growth in childhood
majority of growth has occurred by puberty