Paramedic Drugs - SE MI Drug box meds
1/26
Earn XP
Description and Tags
Basic flash cards with med name, dosing, and basic usecase
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
Acetaminophen
Mild Pain reliever/ Fever reducer
Adult: 325-650mg PO every 4-6hrs
Ped: 10-15mg/kg PO every 4-6hrs
Adenosine
Decrease HR in SVT/PSVT
Adult: 6mg +20cc saline rapid IV/IOpush, repeat 1-2min later with 12mg
Ped: 0.1mg/kg IV/IO w/ 5-10cc saline, max 6mg. repeat at .2mg/kg, max 12mg
Albuterol
Bronchodilator for asthma, bronchospasms, reversible COPD, anaphylaxis
Adult: 2.5mg in 3ml saline, repeat as needed
Ped: 2.5mg in 3ml saline, repeat as needed
Amiodarone
reduce speed of conduction, prolongs cardiac action potential in stable VT, VF, pulseless VT
Stable VT
Adult: 150mg/100ml NS dripped over 10min, max dose 2.2g/24hrs
Peds: 5mg/kg drip over 20min, max 15mg/kg/day
VF/ pulseless VT
Adult: 300mg IV/IO rapid push, may repeat with 150 mg
Peds: 5 mg/kg IV/IO push
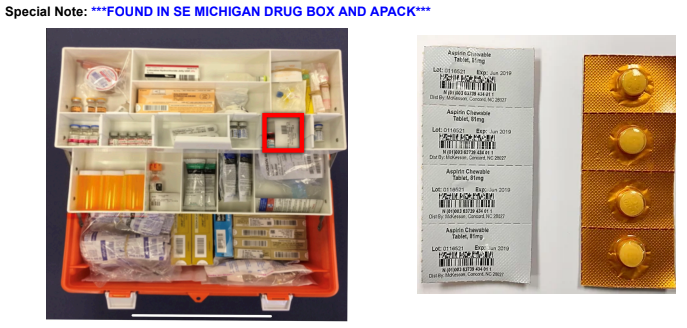
Aspirin
Analgesic, stop platelet aggregation, clot stops getting bigger, chest pain pts
Adult:
Mild pain/fever – 325-650 mg PO every 4 hours.
ACS – 4 81 mg chewable aspirin, 324 mg total OR 1 adult aspirin, 325 mg PO.
Peds: dont give
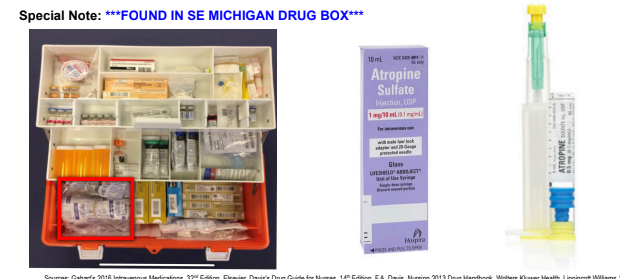
Atropine
Increases heart rate in bradycardic pts, decreases secretions in organophosphate poisoning pts
Adult:
Bradycardia – 1 mg IV/IO q 3-5 min up to max total of 3 mg
Organophosphate poisoning – 1 to 5 mg IV/IM/IO repeated 3-5 min until cessation of bronchial secretions
Peds:
Bradycardia NOT responding to Epi- 0.02mg/kg IV/IO (min dose of 0.1 mg and max single dose 0.5 mg) with a maximum total of 1 mg for a child and 3 mg for an adolescent.
Organophosphate peds < 12 yrs old - 0.05mg/kg IV/IM/IO may be repeated every 20-30 mins until cessation of bronchial secretions
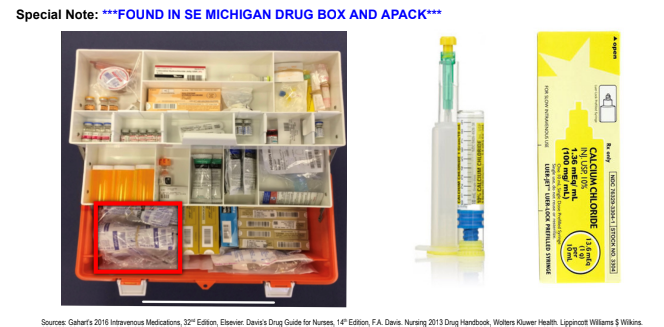
Calcium Chloride
helps regulate excitation threshold of nerves and muscles, give for hyperkalemia, hypocalcemia, hypermagnesemia, and calcium channel blocker OD
Adult:
Cardiac Arrest - 1 gm slow IV
Calcium channel blocker toxicity - 0.5 – 1 gm IV
Crush Injury - 1 gm slow IV over 5 minutes, after extrication
***Wide complex QRS developing after extrication is the heart screaming for Calcium***
Peds: 20 mg/kg slow IV of 10% solution
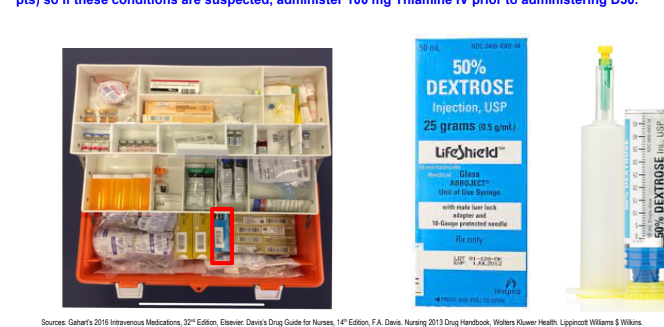
Dextrose
Fuel for cells, mainly given for low blood sugar
Adult: 12.5-25g slow IV push as needed
Ped: 0.5-1g/kg IV of 25% dilution. refer to MI-MEDIC cards
Infant: 0.5-1g/kg IV 10%
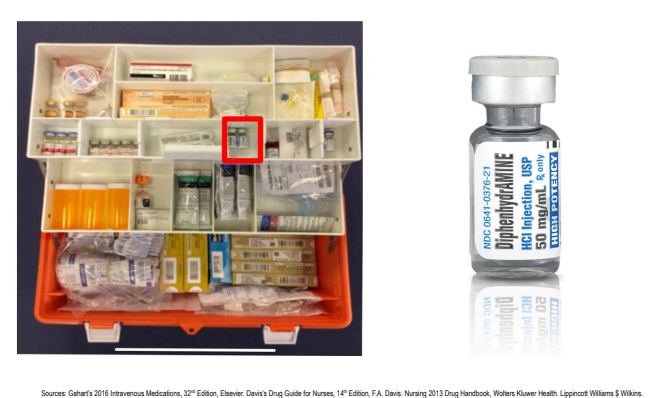
Diphenhydramine
Blocks Histamine release to reduce swelling in anaphalaxis/ allergic reactions
Adult: 25-50mg IV/IM/PO max 400mg/day
Ped: 1mg/kg IV/IM/PO max 300mg/day
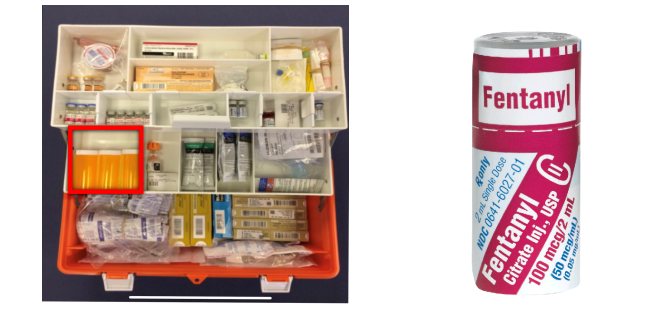
Fentanyl
Pain management
Adult: 0.5-2mcg/kg IV/IN/IM over 2 mins, q 5min, max single dose 100mcg, max total 300mcg
Ped: 0.5-1mcg/kg IV/IM/IN over 2 mins, q 5min, max single dose 100mcg, max total 3mcg/kg
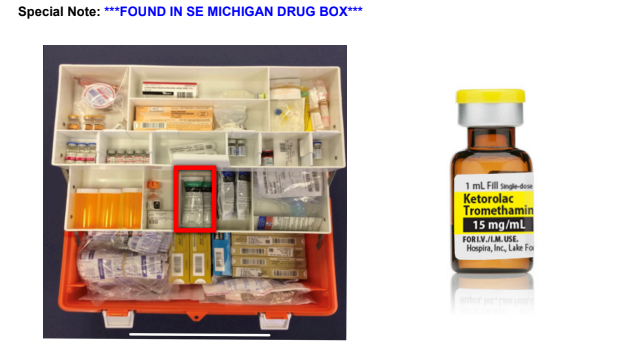
Ketorlac (Toradol)
NSAID pain relief for moderate non-operative pain
Adult: 15-30mg IM/IV
Ped: 1mg/kg IM/IV
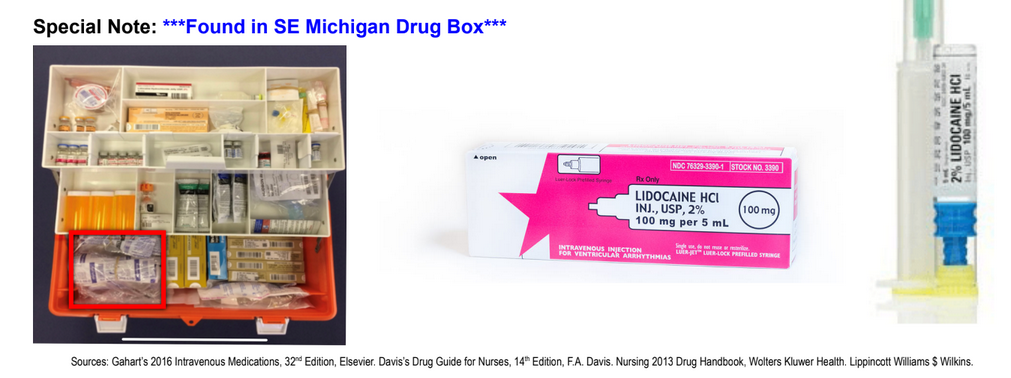
Lidocaine
sodium channel blocker, decreases ventricle automaticity, raises v-fib threshold. give for pulseless v-tach, stable v-tach, or v-fib CA
Adult:
Cardiac Arrest: Initial Dose: 1-1.5 mg/kg IV/IO
Refractory VF: 0.5-0.75 mg/kg IVP in 5-10 minutes (Max of 3 mg/kg)
For Stable VT, Wide-Complex Tachycardia of uncertain type, significant ectopy:
Initial Dose: Ranges may vary between 0.5-0.75 mg/kg and 1-1.5 mg/kg may be used
Redose: 0.5-0.75 mg/kg IVP in 5-10 minutes (Max of 3 mg/ kg)
Maintenance: 1-4 mg/min (30-50 mcg/kg/min). MAX 4 mg/min
Ped:
Cardiac Arrest: 1 mg/kg IV/IO bolus Maintenance infusion drip of 20-50 mcg/kg/min IV/IO post-cardiac arrest.
For PVC’s or V-tach with a pulse – 1 mg/kg IV/IO.
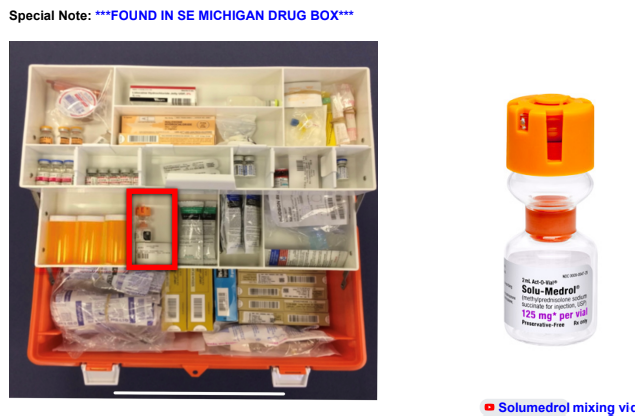
Methylprednisolone (Solu-Medrol)
steroid that suppresses acute and chronic inflammation, causes vascular smooth muscle relaxation to help in anaphalaxis, asthma unresponsive to bronchodilators, and adrenal insufficiency
Adult: 2mg/kg IV max 125mg
Ped: 1-2mg/kg IV max 60mg
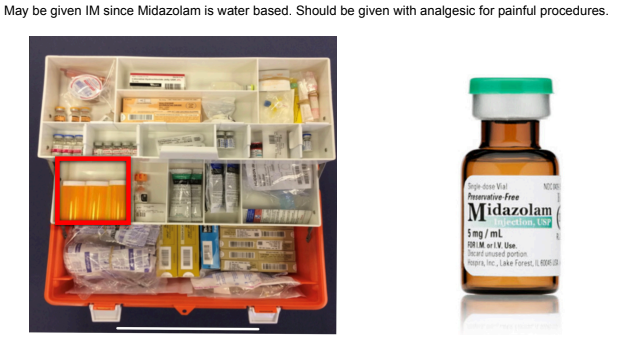
Midazolam (Versed)
benzodiazepine suppresses neuron electrical activity, raises seizure threshold, and gives anterograde amnesia
Adult: 0.1 mg/kg IV/IO/IM/IN (1-5 mg), every 5 min up to 10 mg max total dose
Ped: 0.05-0.3 mg/kg IV/IO/IM/IN, every 5 min up to 5 mg max single dose.
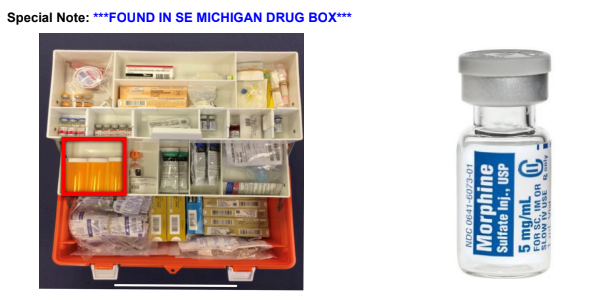
Morphine
Pain med that also causes venous dilation and decreased venous return to heart, reducing heart O2 demand
Adult: 2-10mg IV/IM/IO/SQ/PO
Ped: 0.1 mg/kg IV, every 10 min up to 5 mg max single dose (max total dose of 15 mg)
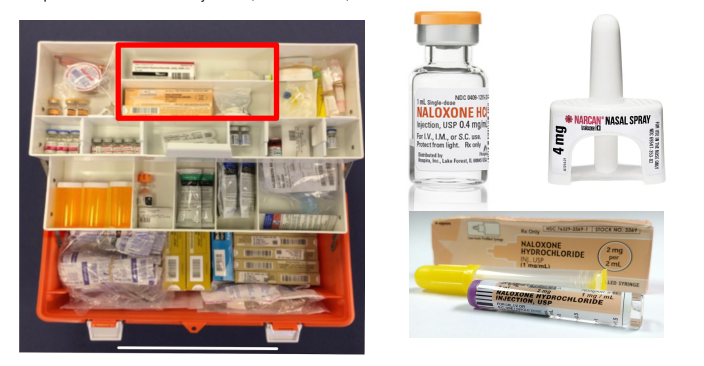
Naloxone (Narcan)
competitive opioid antagonist that kicks opiod off receptors and can reverse respiratory depression
Adult: 0.4-2mg IV/IO/IM/IN as needed up to 10mg max
Ped: 0.1mg/kg IV/IO/IM/IN max single dose of 2mg
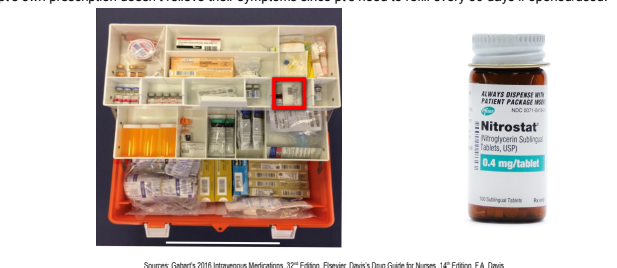
Nitroglycerine
vasodilator used in chest pain pts to relax vasdcular smooth muscle and decrease BP, preload, afterload, and myocardial O2 demand
Adult: 0.4 mg SL, every 3-5 min up to three total doses for 1.2 mg; metered dosing at 0.4 mg/dose (Max 5 doses within 15 min)
Pulmonary edema- 0.8mg (SBP >160mmHg) or 1.2mg (SBP >200mmHg)
Ped: dont give
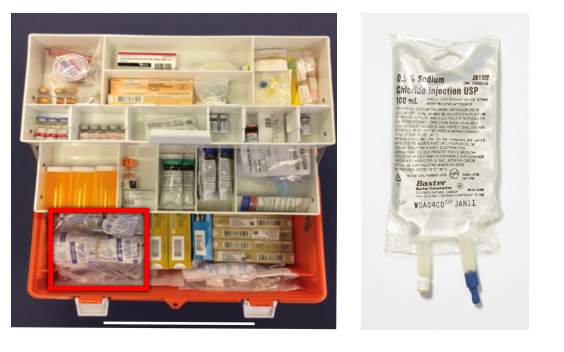
Normal Saline
biologically neutral fluids used to restore circulating blood volume in trauma, hypovolemia, burns, environmental emergencies, etc.
Adult: dose varies on pt condition
Ped: Hypotensive emergencies-20ml/kg IVP w/repeat dose within 15 min if no significant change in bp
Neonates: Hypotensive emergencies-10 ml/kg IVP w/repeat dose within 15 min if no significant change in bp
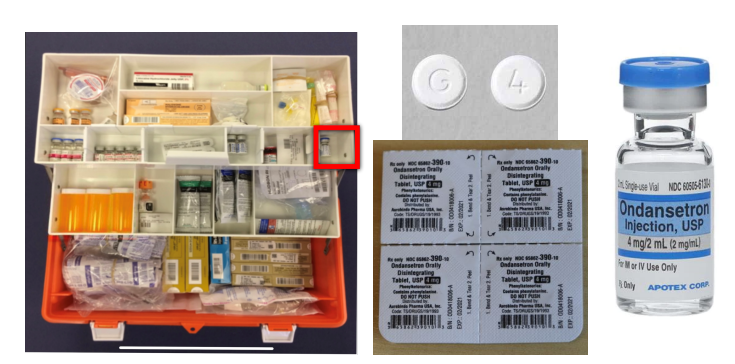
Ondansetron (Zofran)
Selective serotonin blocking agent that blocks chemoreceptors in intestinal vagal nerve terminals, minimizing nausea and vomiting
Adult: 4 mg ODT (oral dissolving tablet)
4 mg IM
4 mg slow IV (at least 30 seconds, recommended over 2 minutes)
Ped: (>6mo – 14 yrs) 0.15 mg/kg IV/IO/IM (Max 4mg) MI Medic Cards
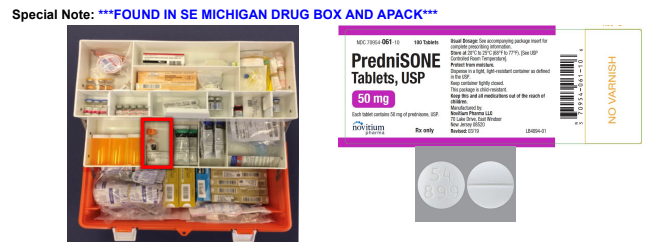
Prednisone
Cause decreased inflammation through various mechanisms at lower doses, higher doses cause immunosuppression. Use in allergic reactions or inflammatory respiratory conditions
Adult: 50mg tablet PO
Ped: 50mg tablet PO in kids over 6
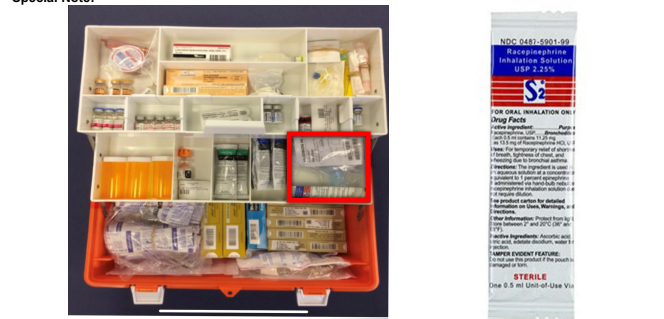
Racemic Epi
Inhaled version of Epi used for bronchodilation and is anti-inflammatory to treat larynx/trachea swelling and edema
Mainly for croup peds
Adult: 0.5mL (2.25%) in 5mL NS over 15 min
Ped: All doses given via aerosolized neb.
For pts < 6 months – 0.25 ml (2.25%) diluted in 3 ml NS.
For pts > 6 months – 0.5 ml (2.25%) diluted in 3 ml NS.
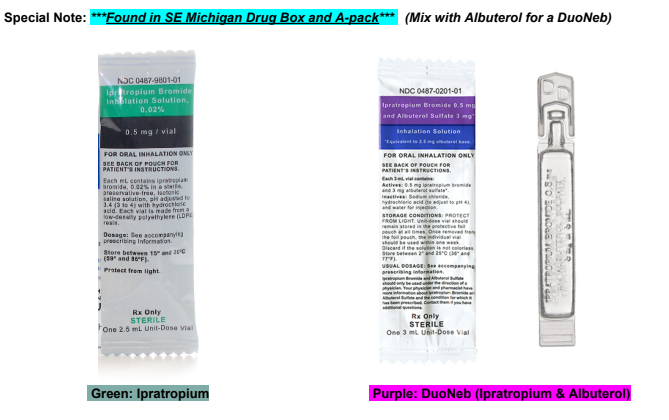
Ipratropium Bromide
blocks acetylcholine in bronchioles to cause bronchodilation and reduced mucous production
Adult: 0.5 mg diluted in 2.5 ml NS via nebulizer. May repeat dose twice
Ped: 250-500 mcg diluted in 2.5 ml saline via nebulizer every 20 mins up to 3 doses
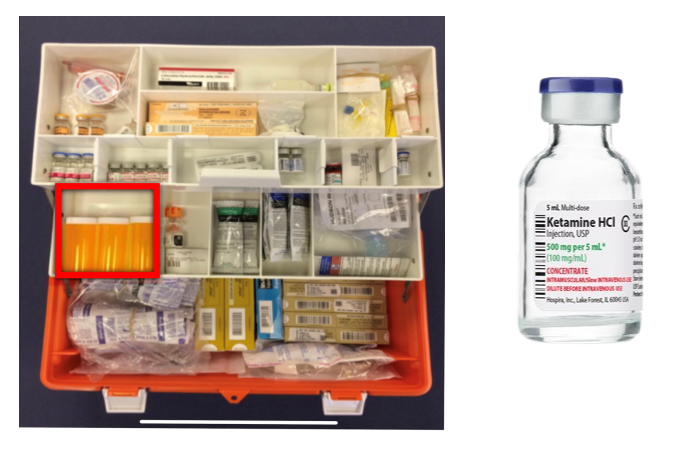
Ketamine
PCP derivative used to block impulses associated with pain perception, produces short acting amnesia without muscular relaxation
Adult: Pain Management: (For pain >4, but <8 on the Wong Pain Scale) 0.2mg/kg IV/IO | 0.5mg/kg IN | 0.02mg/kg IM. Max single dose is 25mg. May repeat Ketamine, ONCE.
Patient Sedation: 4 mg/kg IM | 1-2 mg/kg IV/IO* | 1-2 mg/kg IN. Max single dose is 500mg.
Excited Delirium: 4 mg/kg IM ONLY, to a MAX single dose of 500mg
Ped:
Pain Management: (For pain >4, but <8 on the Wong Pain Scale) 0.2 mg/kg IV/IO* | 0.5 mg/kg IN | 0.02 mg/kg IM. Max single dose is 25mg. May repeat Ketamine, ONCE.
Patient Sedation: 4 mg/kg IM | 1-2 mg/kg IV/IO* | 1-2 mg/kg IN. Max single dose is 500mg
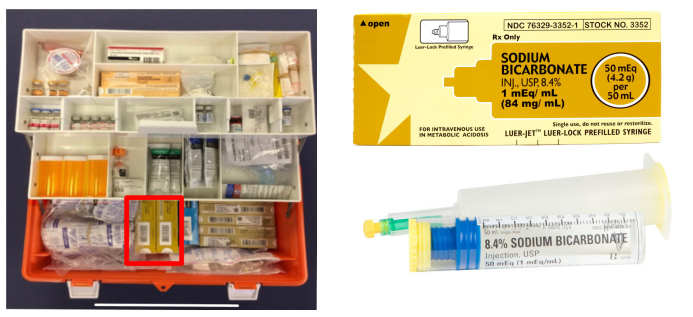
Sodium Bicarbonate
Short acting acid buffer that can absorb H+ ions to raise blood pH
Adult: 1mEq/kg IV
Ped: same as adult but infuse slowly only if ventilations are adequate
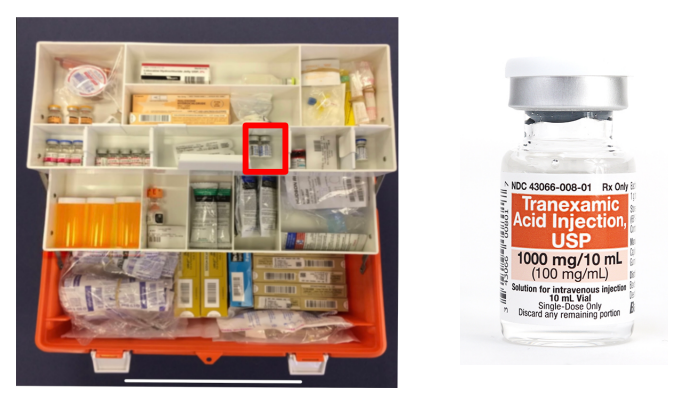
Tranexamic Acid (TXA)
Inhibits the breakdown of fibrin and helps stop bleeding, only thing we have to treat internal bleeding
Adult: 1 g IV slow push over 1-2 minutes
Ped: 10mg/kg IV
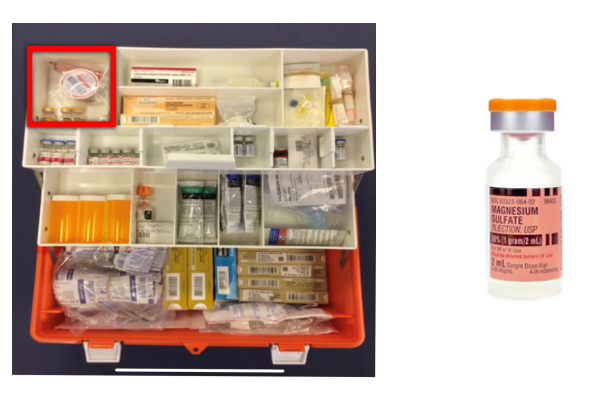
Magnesium Sulfate
Reduces striated muscle contractions and blocks peripheral neuromuscular transmission. Give for Seizures due to eclampsia after seizure activity is stopped, torsades de pointes, unstable V-Tach attributed to digitalis toxicity, hypomagnesemia, status asthmaticus unresponsive to beta-adrenergic drugs.
Adult:
Pulseless arrest (hypomagnesemia and torsades de pointes) and status asthmaticus:
1-2 g diluted in 10 ml D5W/NS IV/IO
Torsades de pointes or hypomagnesemia WITH A PULSE:
1-2 g in 100ml D5W/NS over 5-60 min IV
Eclampsia
4 g IV drip over 20 min, with a max dose of 30-40 g/day
Peds:
Pulseless arrest or hypomagnesemia/torsades with a pulse:
25-50 mg/kg IV/IO (max 2 g) over 10-20 mins
Status asthmaticus
25-50 mg/kg IV/IO (max 2 g) diluted 100 ml D5W/NS over 15-30 mins.
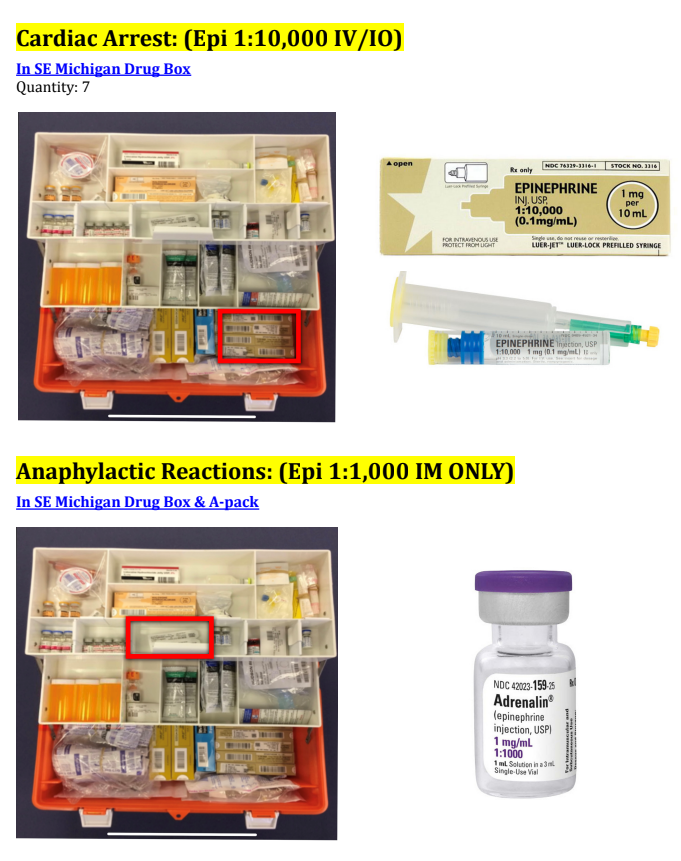
Epinephrine
Increases cardiac HR, contraction force, and cardiac output. Acts as a potent vasoconstrictor and bronchodilator. Also suppresses release of mediators from mast cells and basophils (supresses inflammation)
Adult:
Cardiac Arrest: 1mg every 3-5 minutes Epi 1:10,000 IV/IO
Anaphylactic Reactions: 0.3mg Epi 1:1,000 IM ONLY
Post ROSC or Bradycardia with severe hypotension: 2-10 mcg/ min IV Infusion
Push Dose Epi 1:100,000(Post ROSC, Severe Hypotension): 10-20 mcg every 3-5 minutes and titrate to a BP >90
Peds:
Cardiac Arrest: 0.01 mg/kg every 3-5 minutes Epi 1:10,000 IV/IO
Anaphylactic Reactions: 0.15mg for <30kg /// 0.3mg for >30kg Epi 1:1,000 IM ONLY
Bradycardia: 0.01 mg/kg every 3-5 minutes
Push Dose Epi (Post ROSC, Severe Hypotension): 1 mcg/kg every 3-5 minutes; Max 10 mcg