Proced II: Comprehensive Study of Skull Morphology and Topography
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
82 Terms
Mesocephalic skull
The shape of the average head
-Width 75%-80% of length
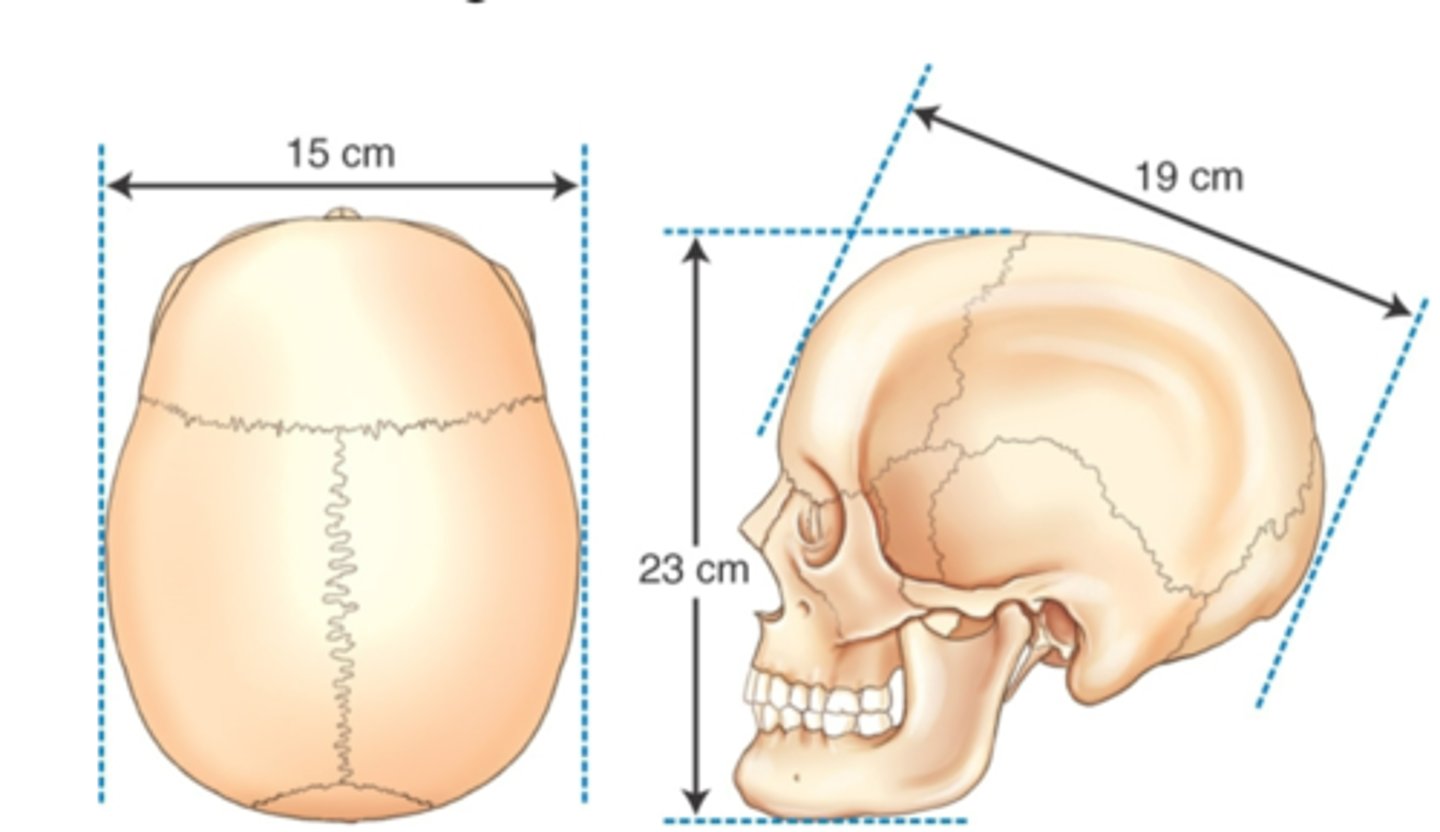
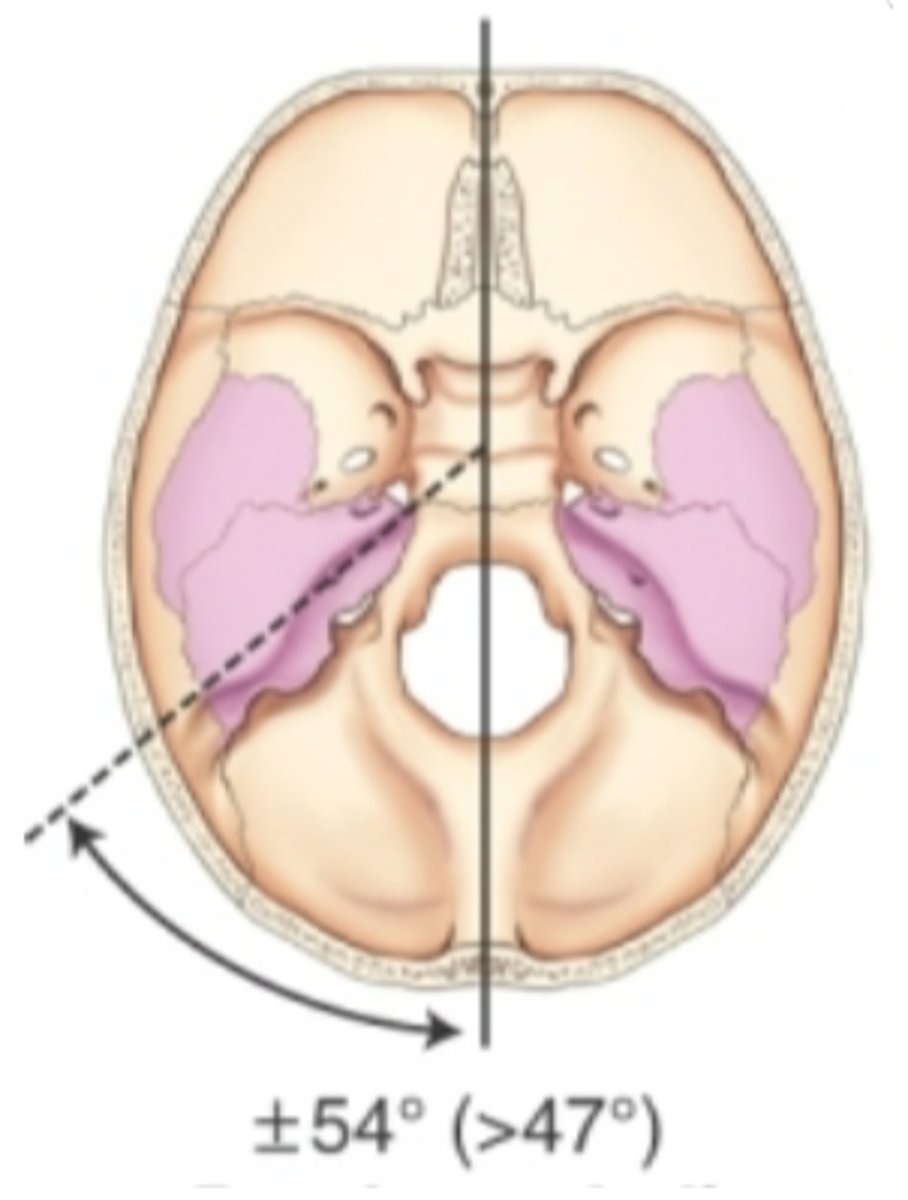
Brachycephalic skull
Shorter, broader, wider skull
-width is 80% or more of length
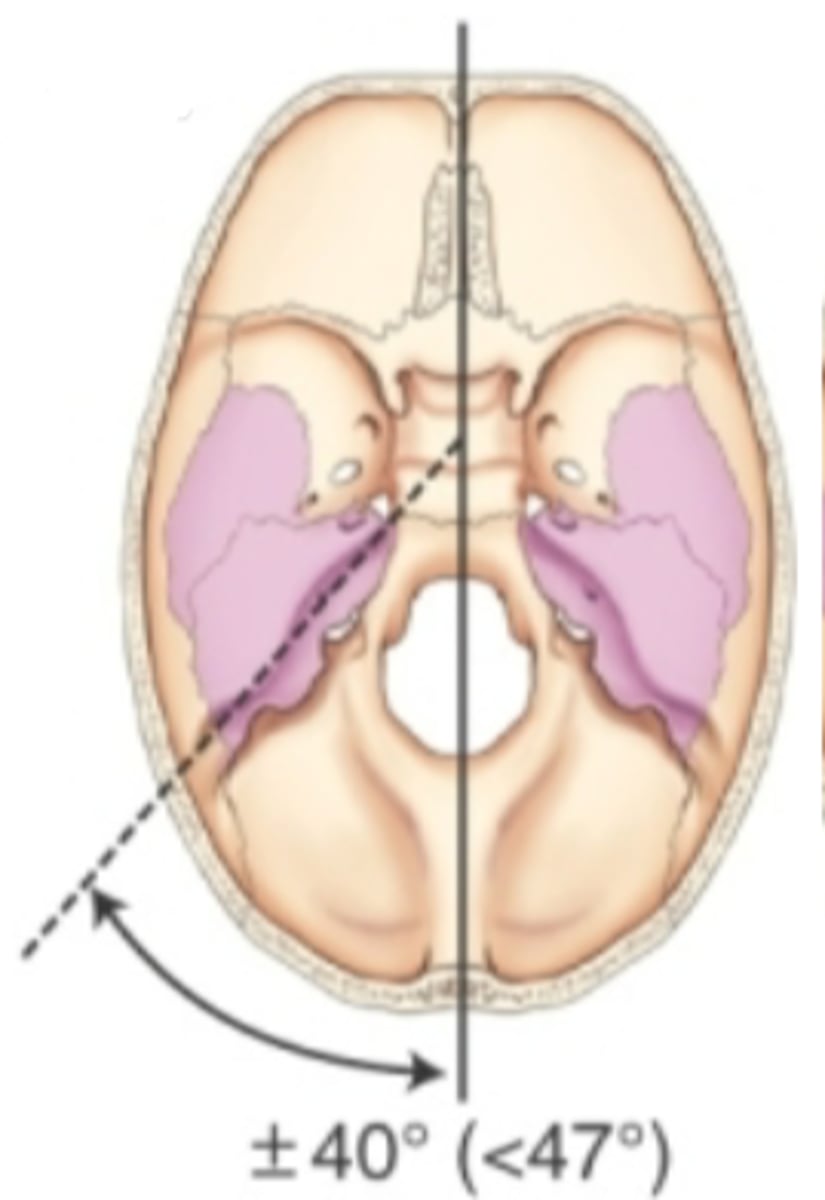
Dolichocephalic
long narrow skull
-width is less than 75% of length
SOM
supraorbital margin
IOM
inferior orbital margin

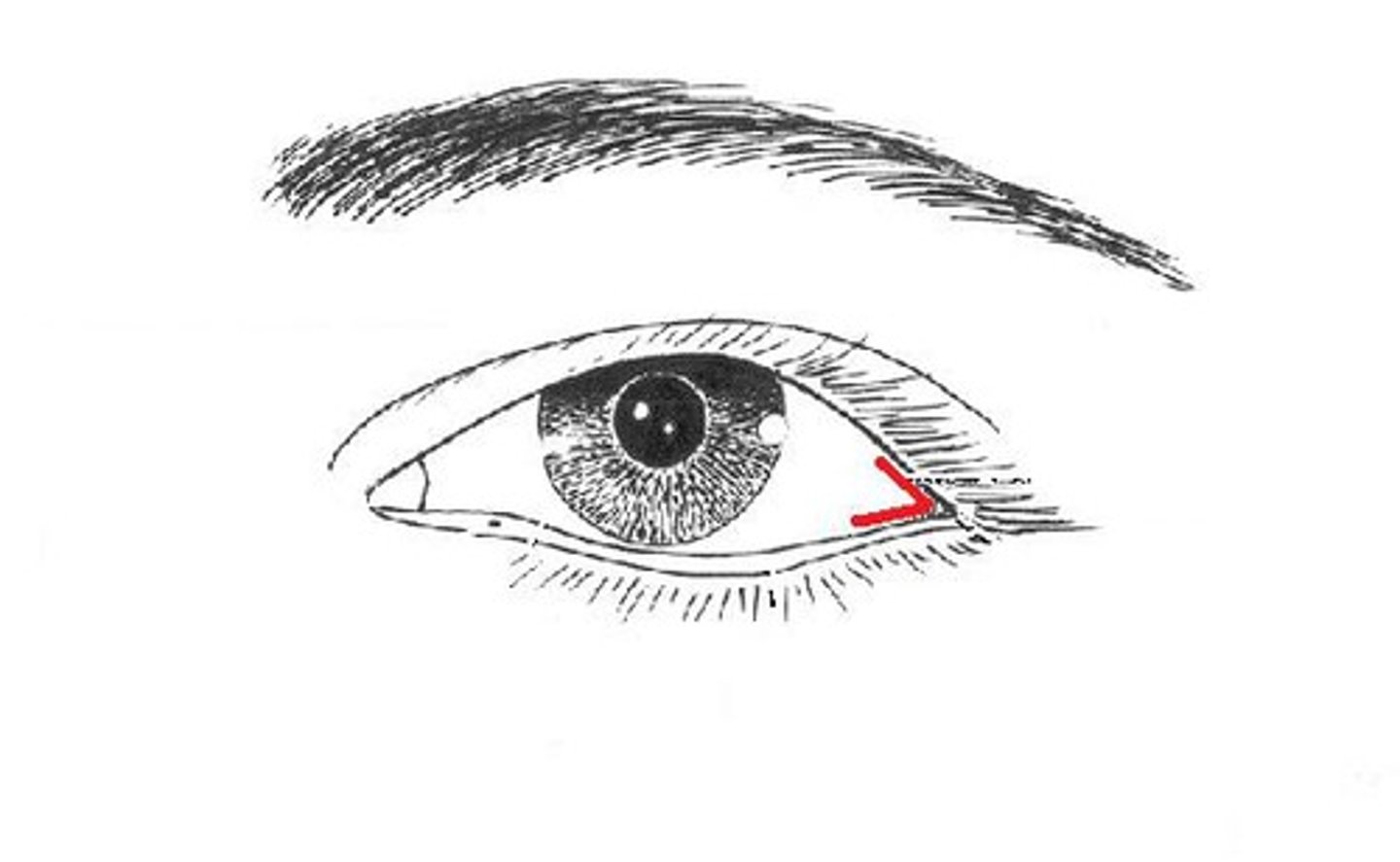
Outer canthus
the more lateral junction of the eyelids
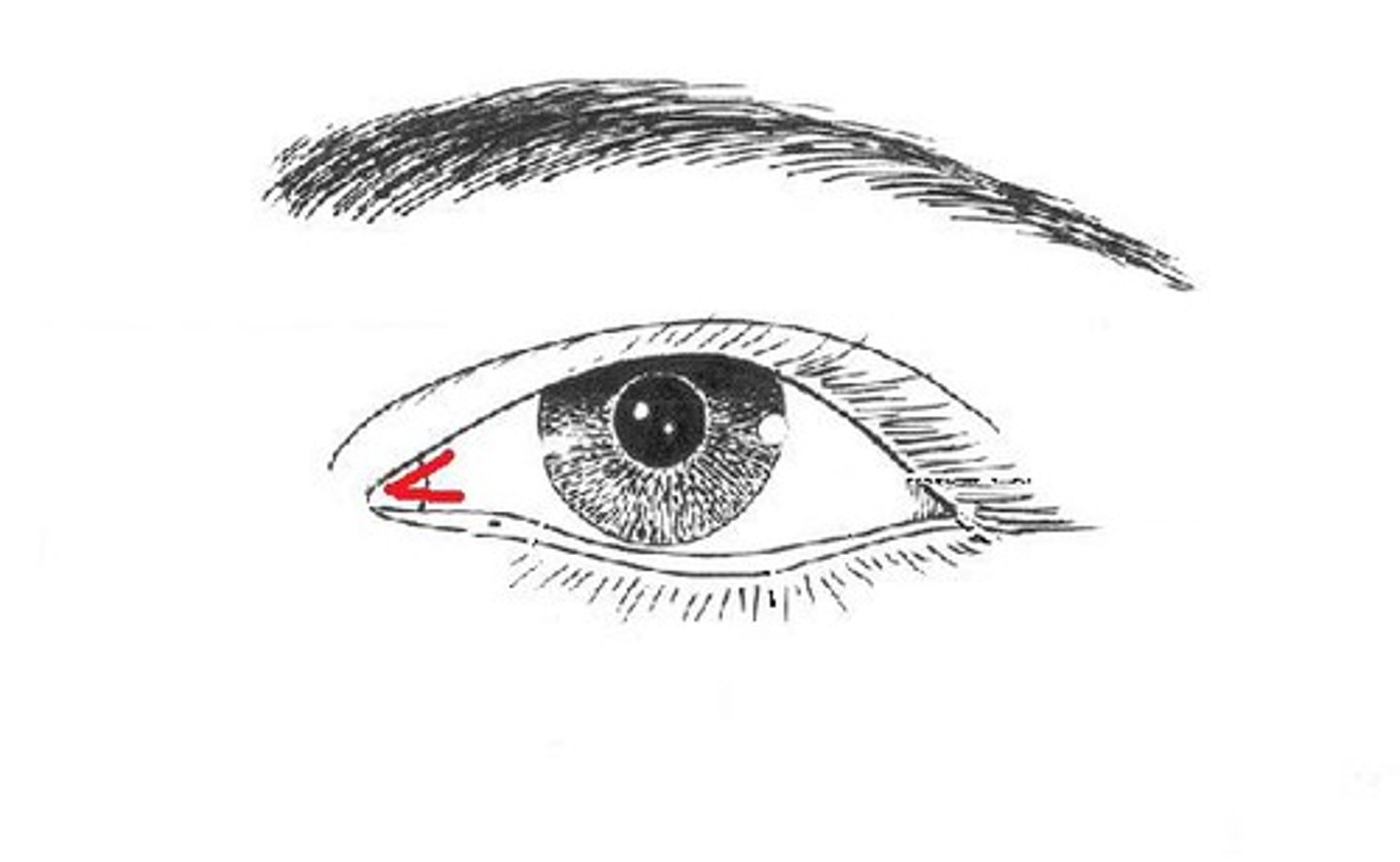
Inner canthus
where the eyelids meet near the nose
Midlateral orbital margin
the portion of the lateral rim that is near the outer canthus of the eye
SOG
supraorbital groove
-correlates with orbital plate
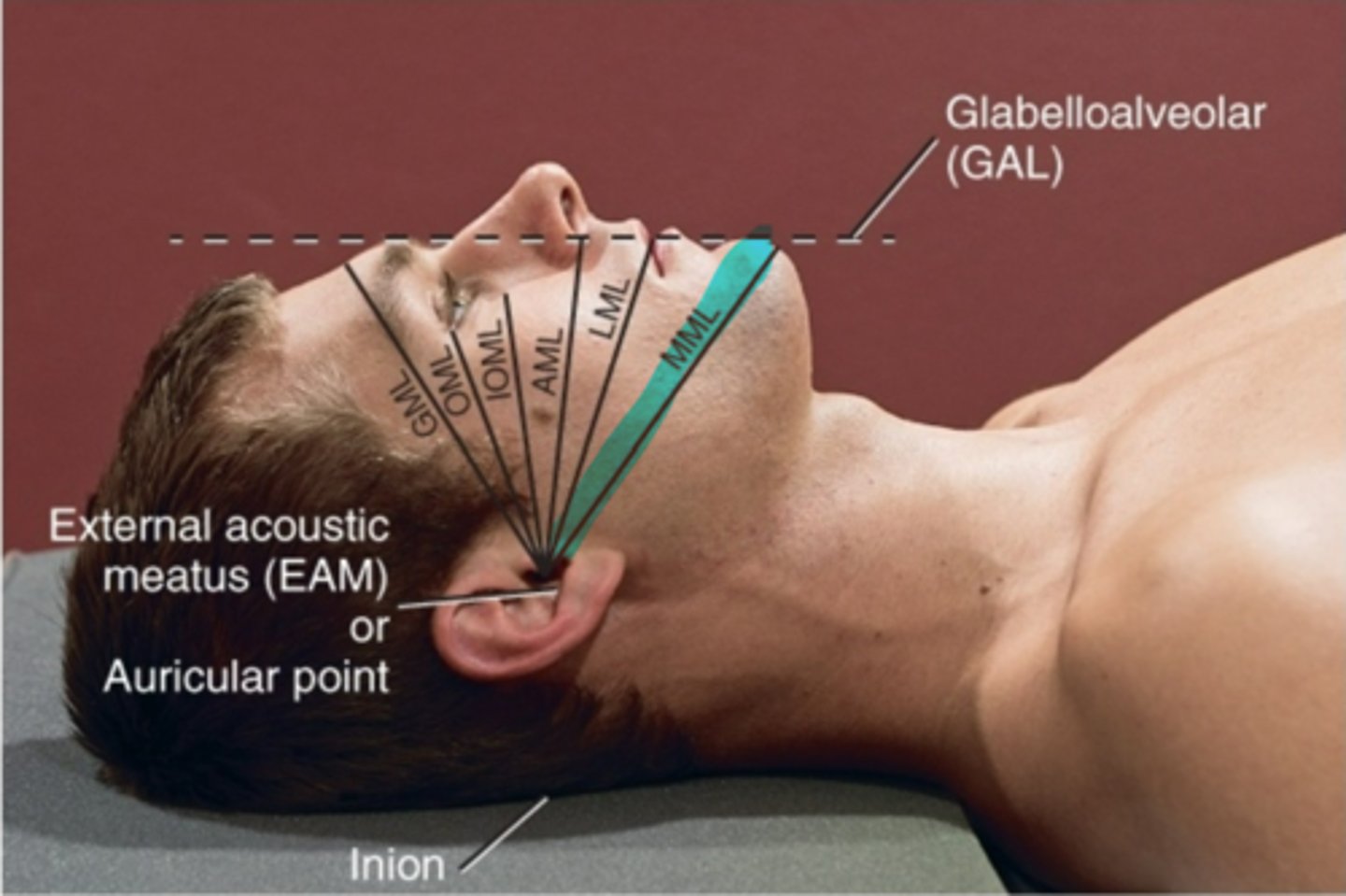
GML
Glabella meatal line
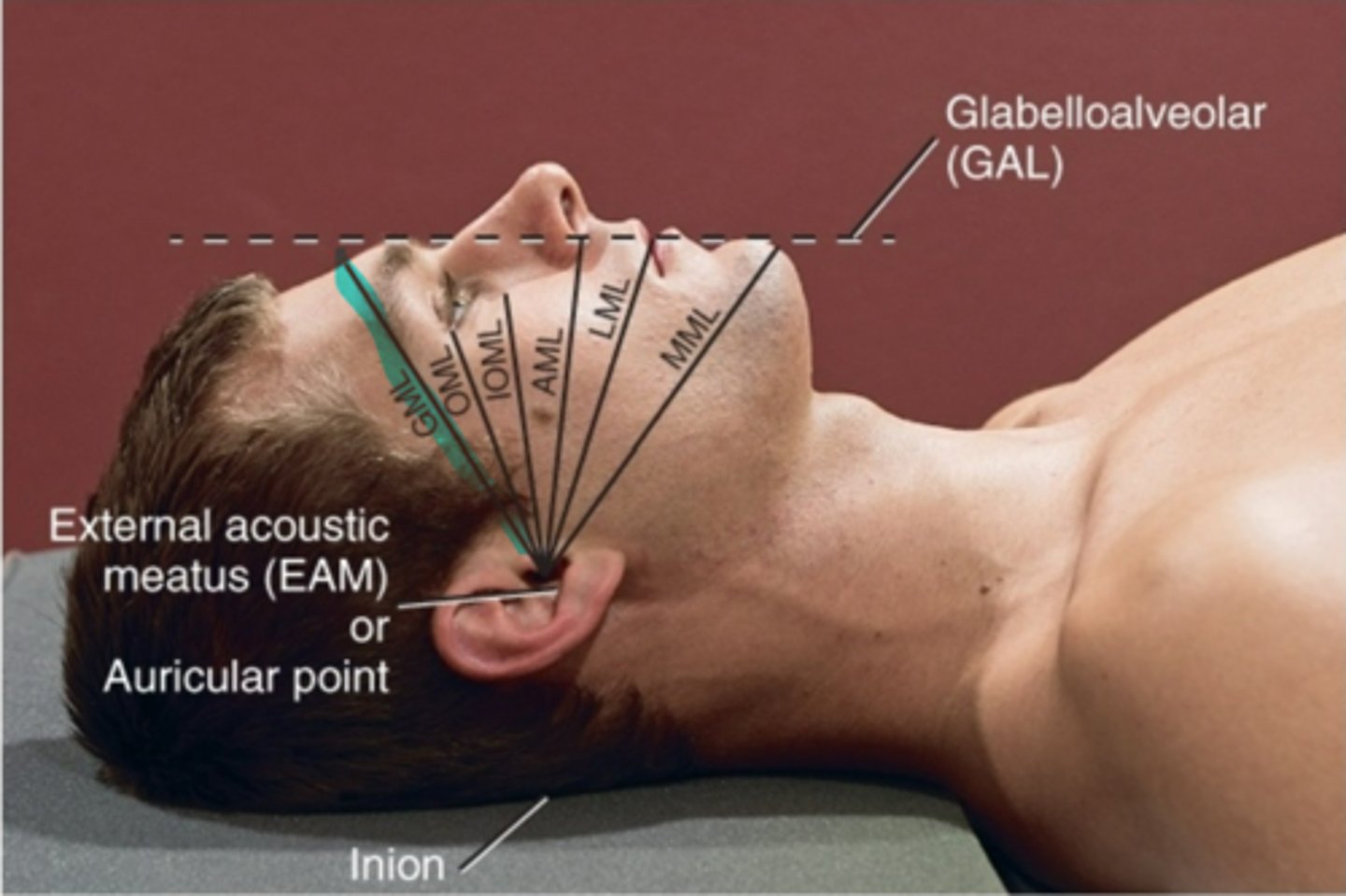
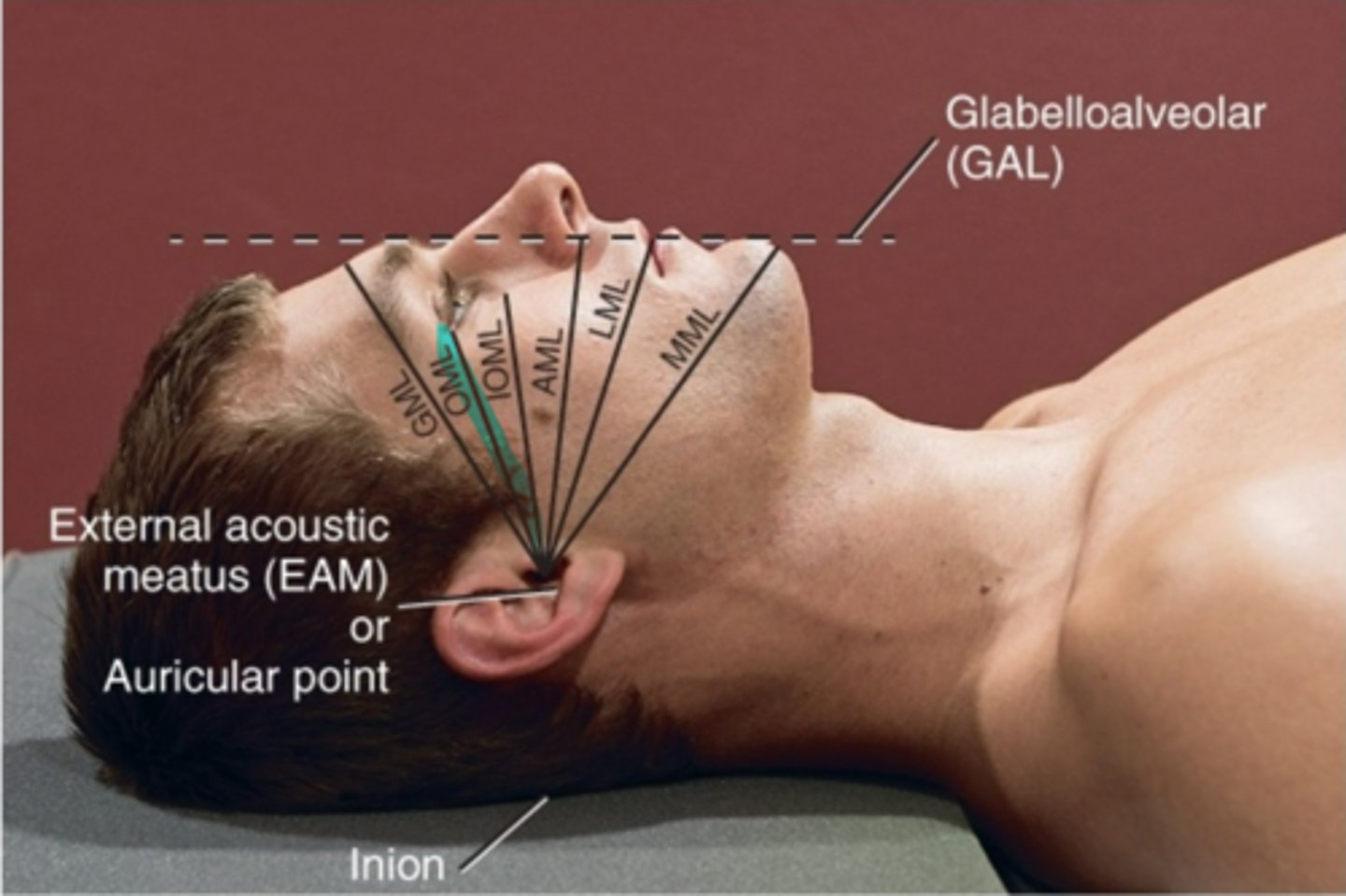
OML
orbital meatal line
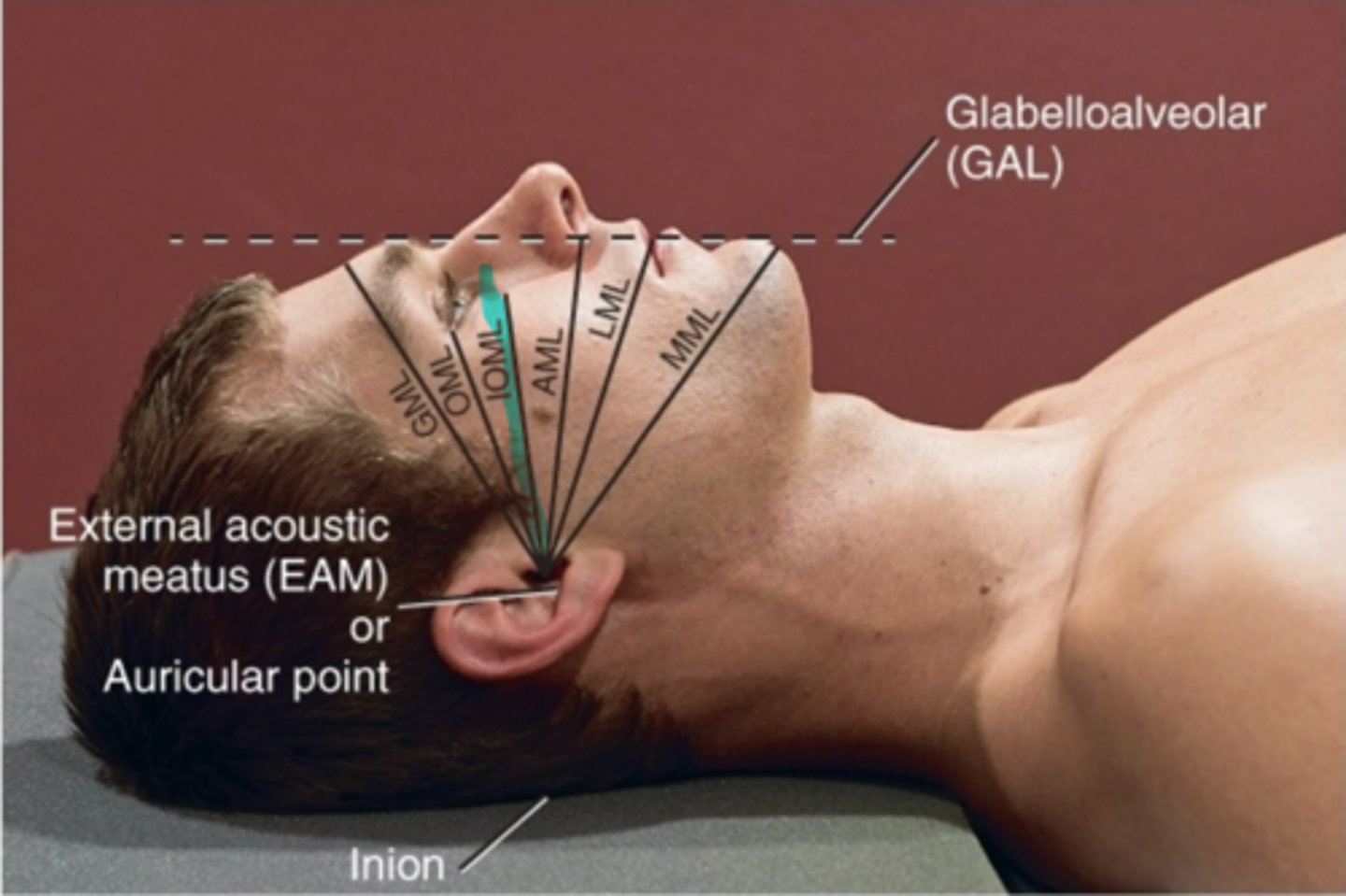
IOML
infraorbitalmeatal line
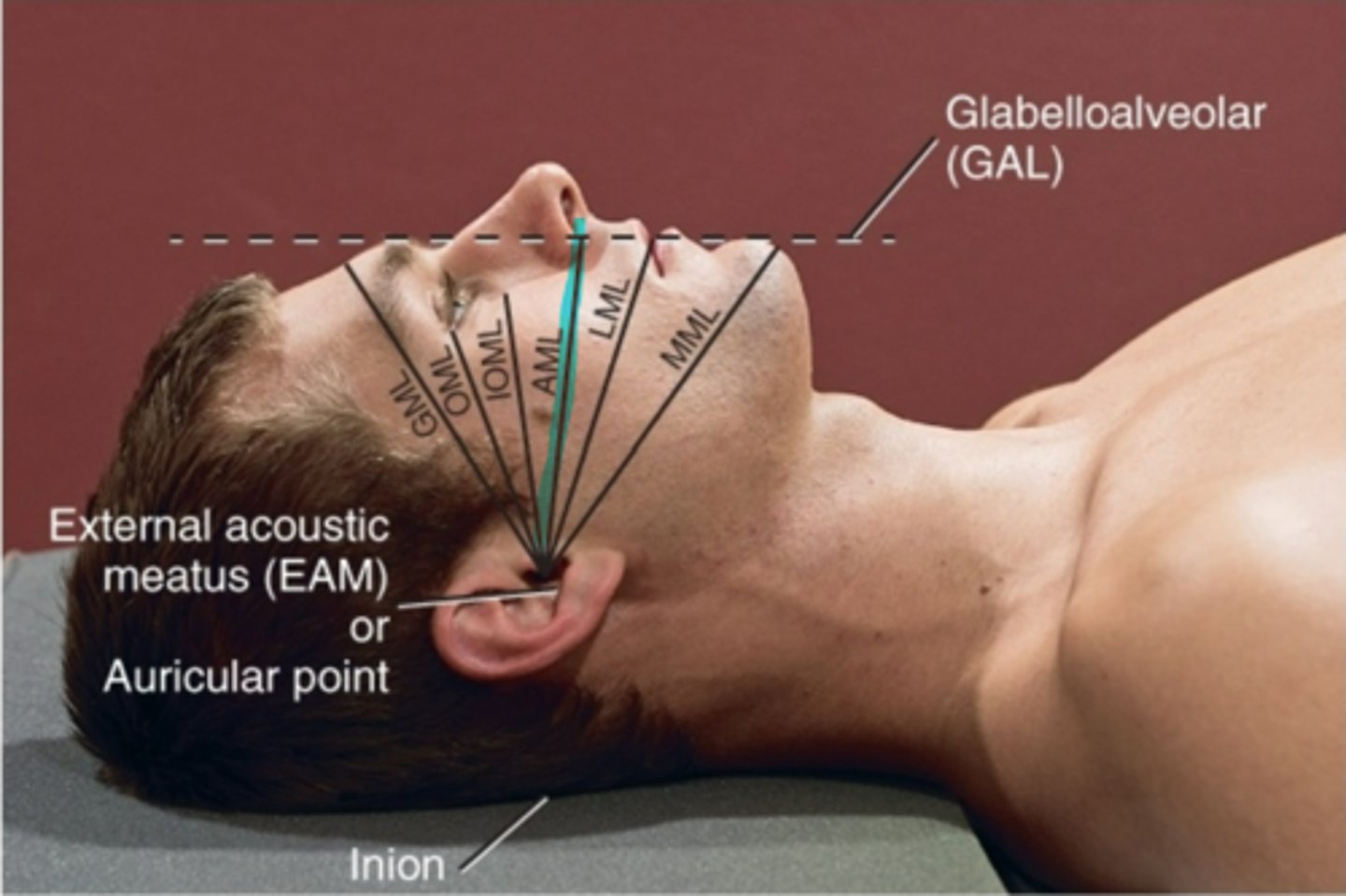
AML
Acanthiomeatal line
LML
lips-meatal line
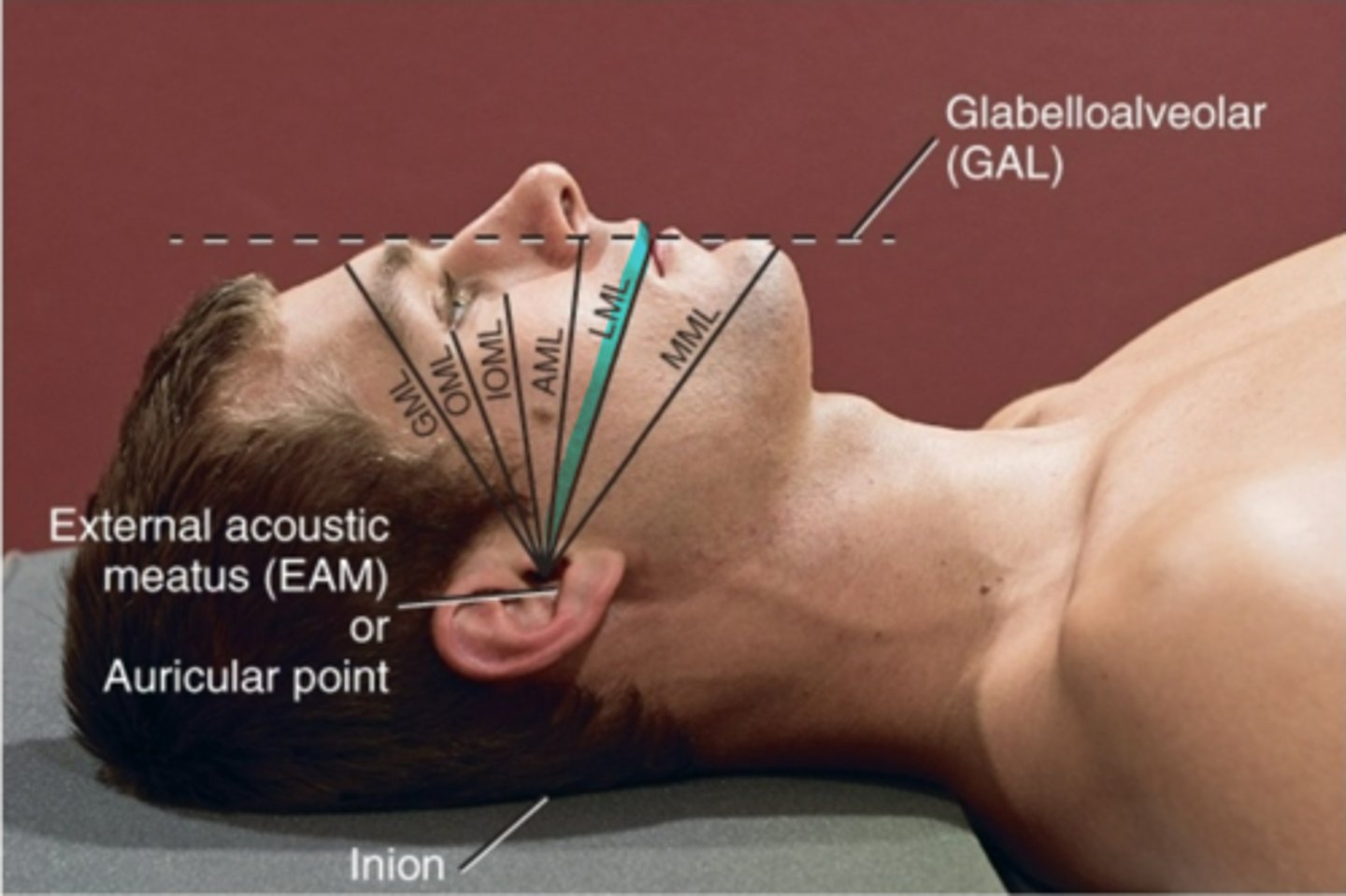
MML
mentum to meatal line
TEA
top of ear attachment
Auricle
pinna
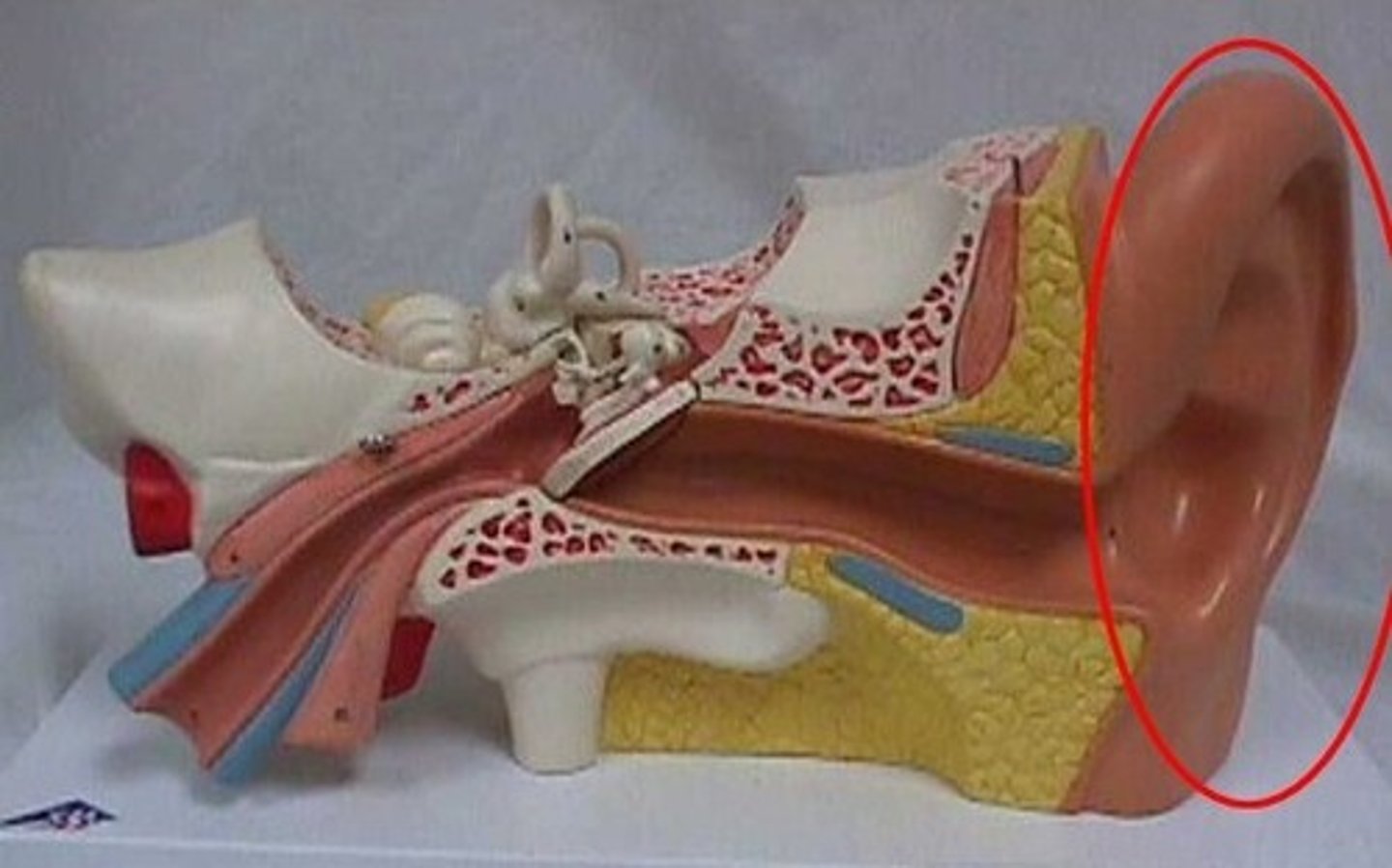
Tragus
covers the EAM

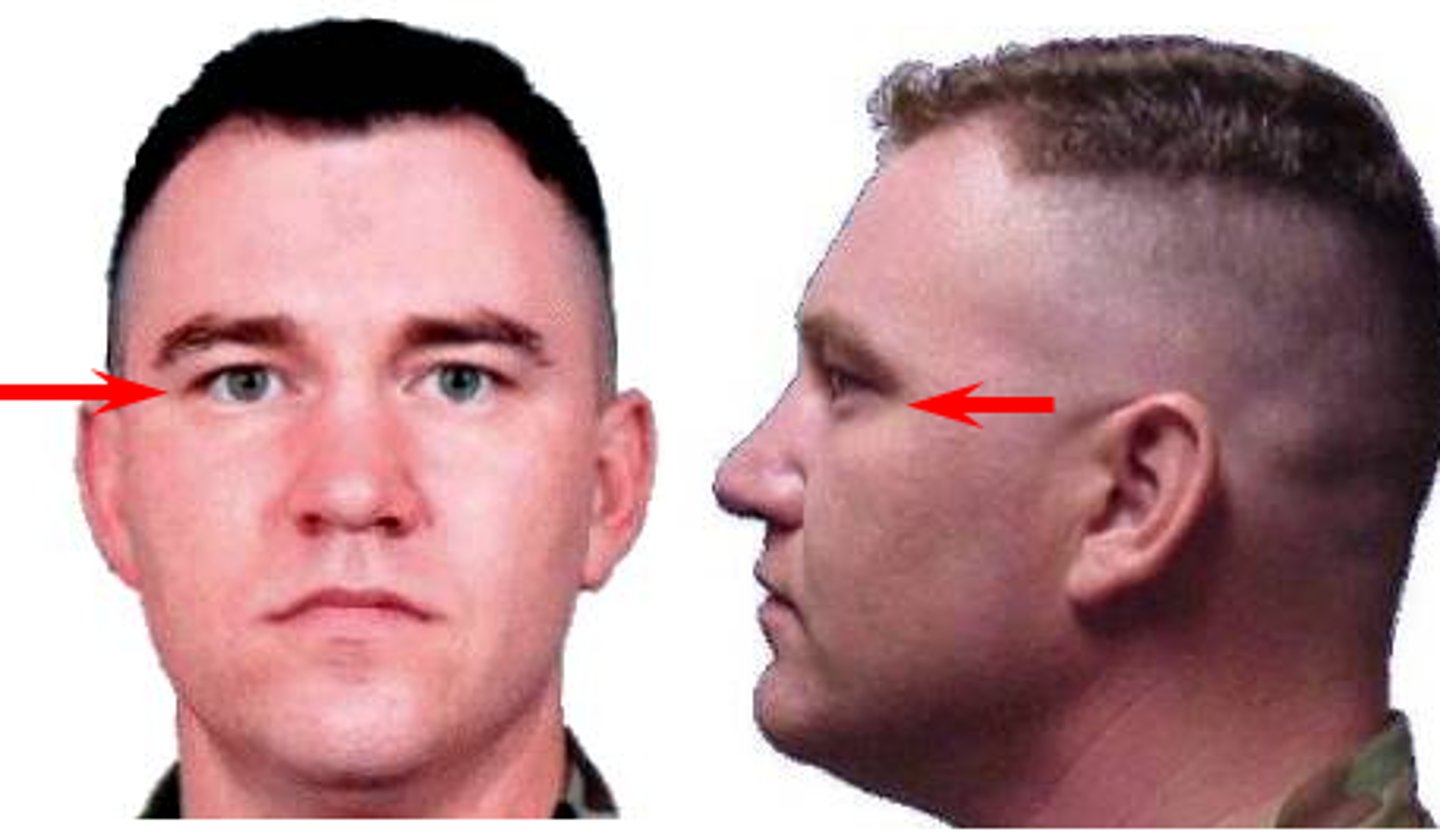
Glabella
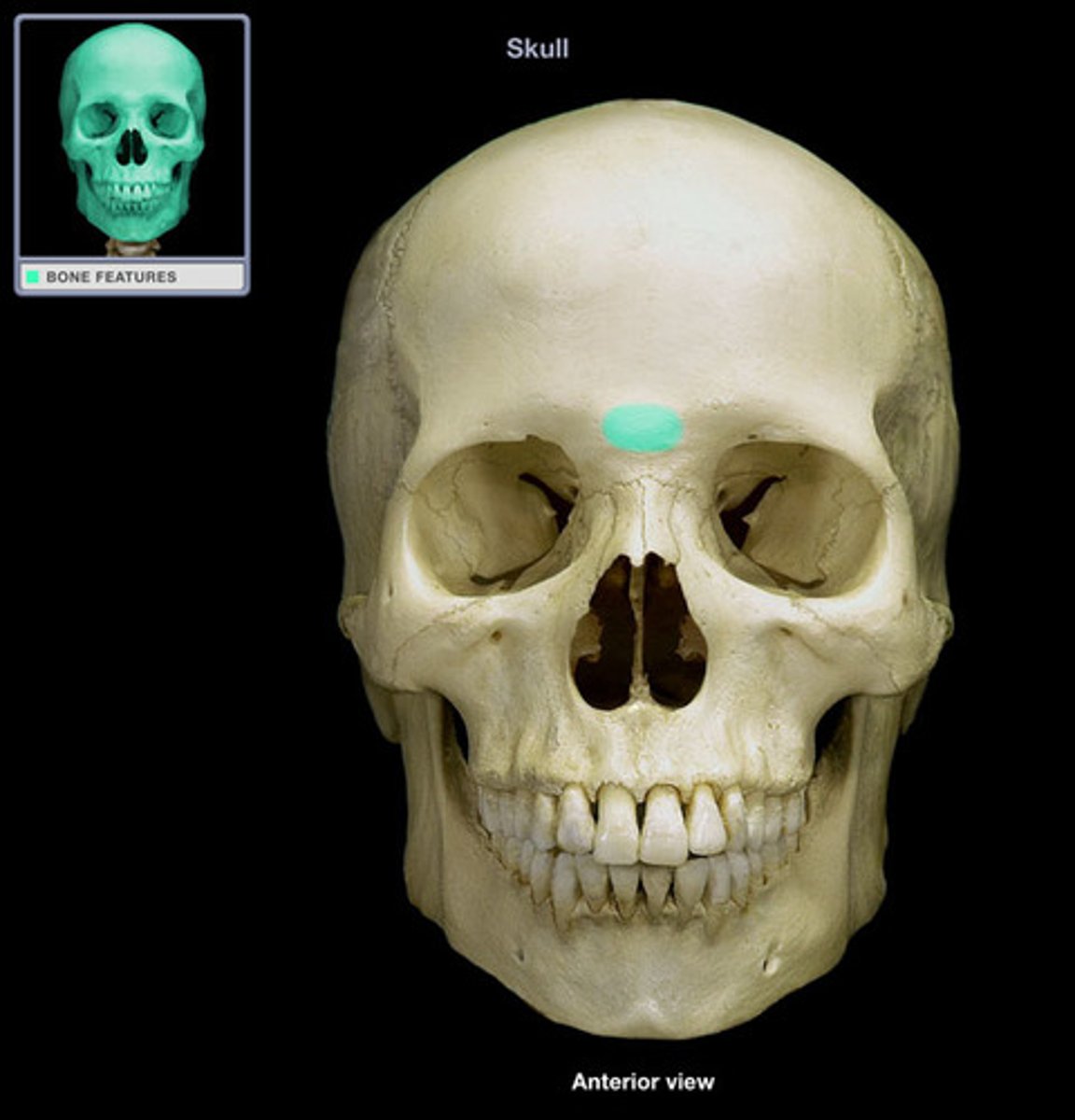
Nasion

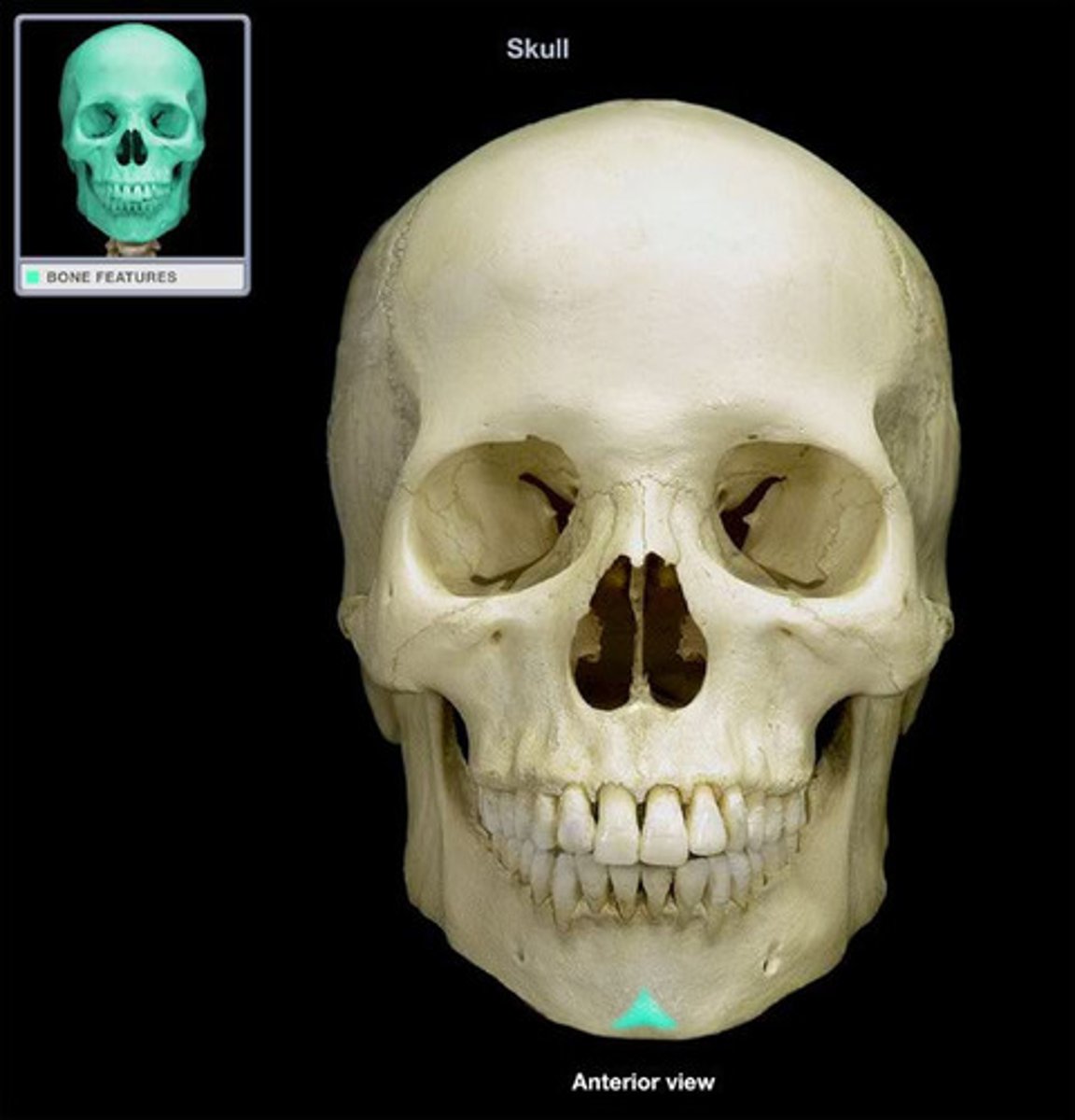
Acanthion
Junction of the nose and upper lip

Mental point
Angle (gonion)

When positioning for facial bone projections, an __________ position is preferred
erect
List the 5 common positioning errors
1. Rotation
2. Tilt
3. Excessive neck flexion
4. Excessive neck extension
5. Incorrect CR angle
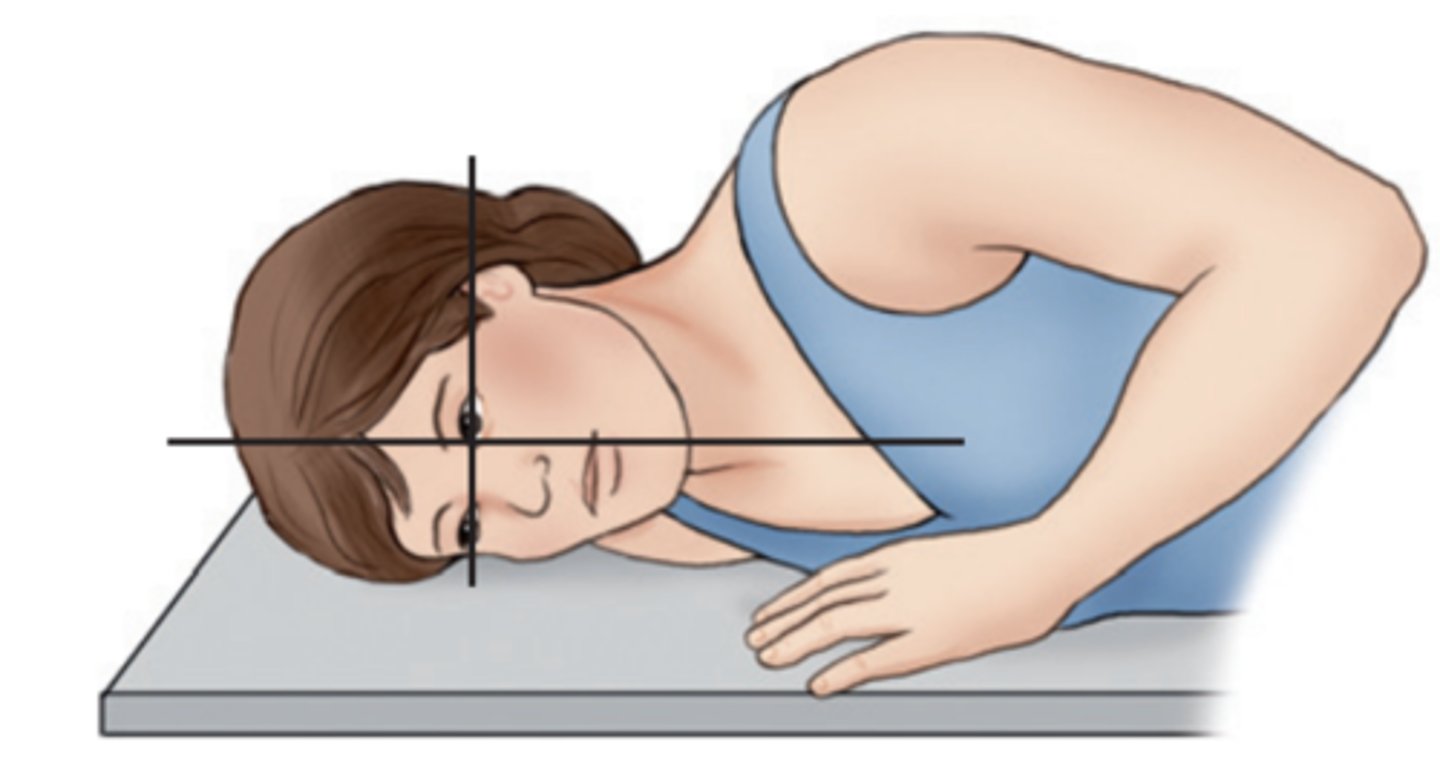
Rotation
When MSP isn't parallel to the IR in a lateral position
-when turned right or left
-usually evident by looking at Rami of mandible. anterior and posterior clinoid processes
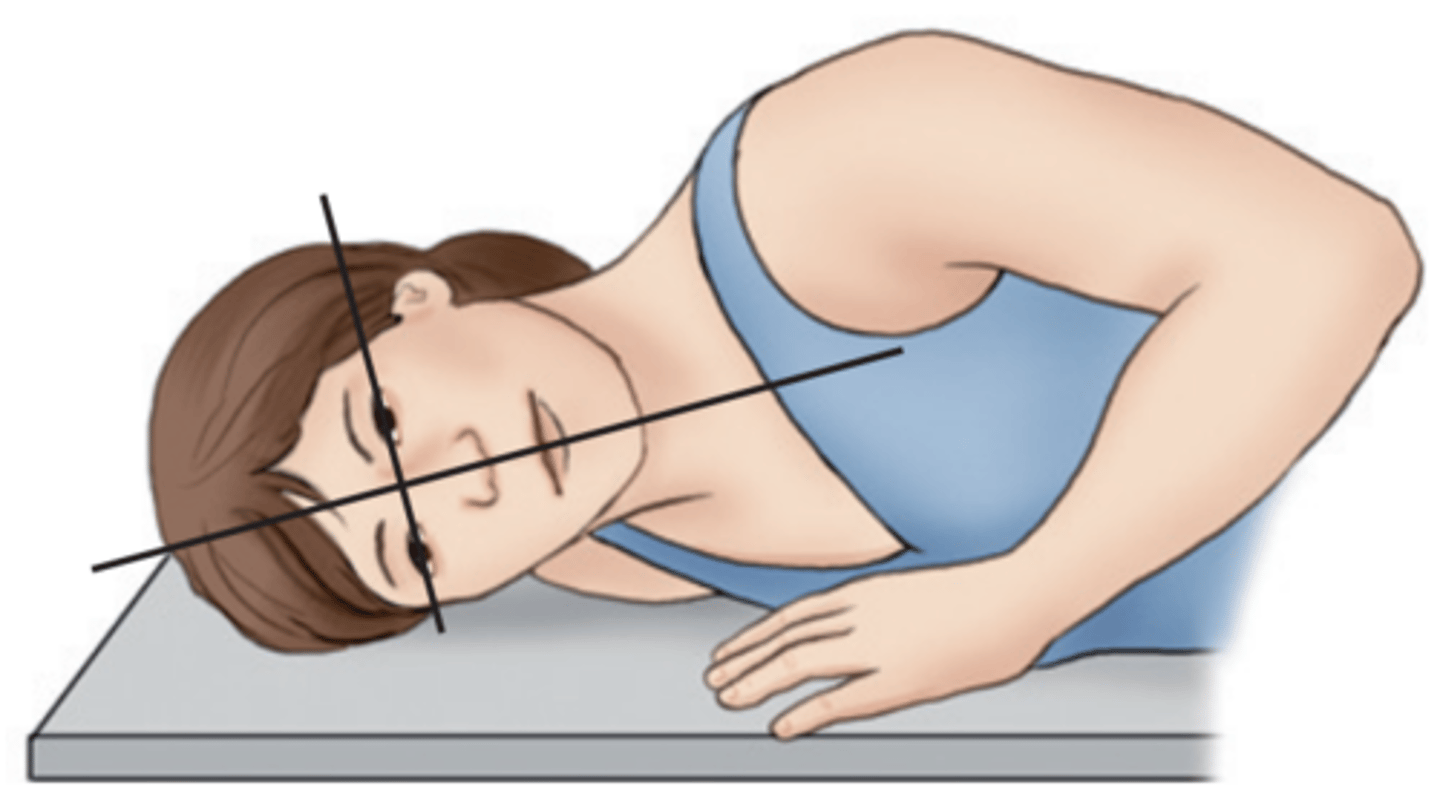
Tilt
a tipping or slanting of the MSP laterally, even though rotation may not be present.
-one area closer to the shoulder than the other
-usually evident by looking at orbital plates, body of mandible, or horizontal structures
Excessive neck flexion
Excessive neck extension
when the CR is parallel to the OML. This position causes the petrous pyramids to be projected-
directly into the orbits
To visualize the facial bone mass with conventional radiography, the petrous pyramids must be removed from the facial bone area of interest. How do we accomplish this?
This can be done either by tube angulation or by extension of the neck
When the CR is parallel to the MML this position causes the petrous pyramids to be projected-
just below the maxillary sinuses
things to ask during patient history if examining the skull
has the patient have any loss of consciousness, any loss in vision or injury? What is the mechanism of injury?
things to ask during patient history if examining the sinuses
ask about recent sinus infection, chronic or acute symptoms, location, chronology, history of surgeries.
Cranium Routine
-AP Axial (Towne Method)
-Both Laterals
-PA 15° (Caldwell Method) or PA 0°
Special Cranium Routines
-PA Axial (Haas)
-SMV (Submentovertex)
AP Axial (Towne Method) Skull
-Position:
• Petrous ridges should be symmetric, indicating no rotation (petrous ridge will appear narrowed in the direction of rotation).
• Dorsum sellae and posterior clinoids visualized in the foramen magnum indicate correct CR angle and proper neck flexion/extension.
• Underangulation of CR or insufficient flexion of neck projects the dorsum sellae superior to the foramen magnum. Overangulation of CR or excessive neck flexion superimposes the posterior arch of C1 over the dorsum sellae within the foramen magnum and produces foreshortening of the dorsum sellae.
• Shifting of the anterior or posterior clinoid processes laterally within the foramen magnum indicates tilt
Lateral of Skull
-Position:
• No rotation or tilt of the cranium is evident.
• Rotation is evident by anterior and posterior separation of symmetric vertical bilateral structures such as the mandibular rami, and greater wings of the sphenoid.
• Tilt is evident by superior and inferior separation of symmetric horizontal structures such as the orbital roofs (plates) and greater wings of sphenoid

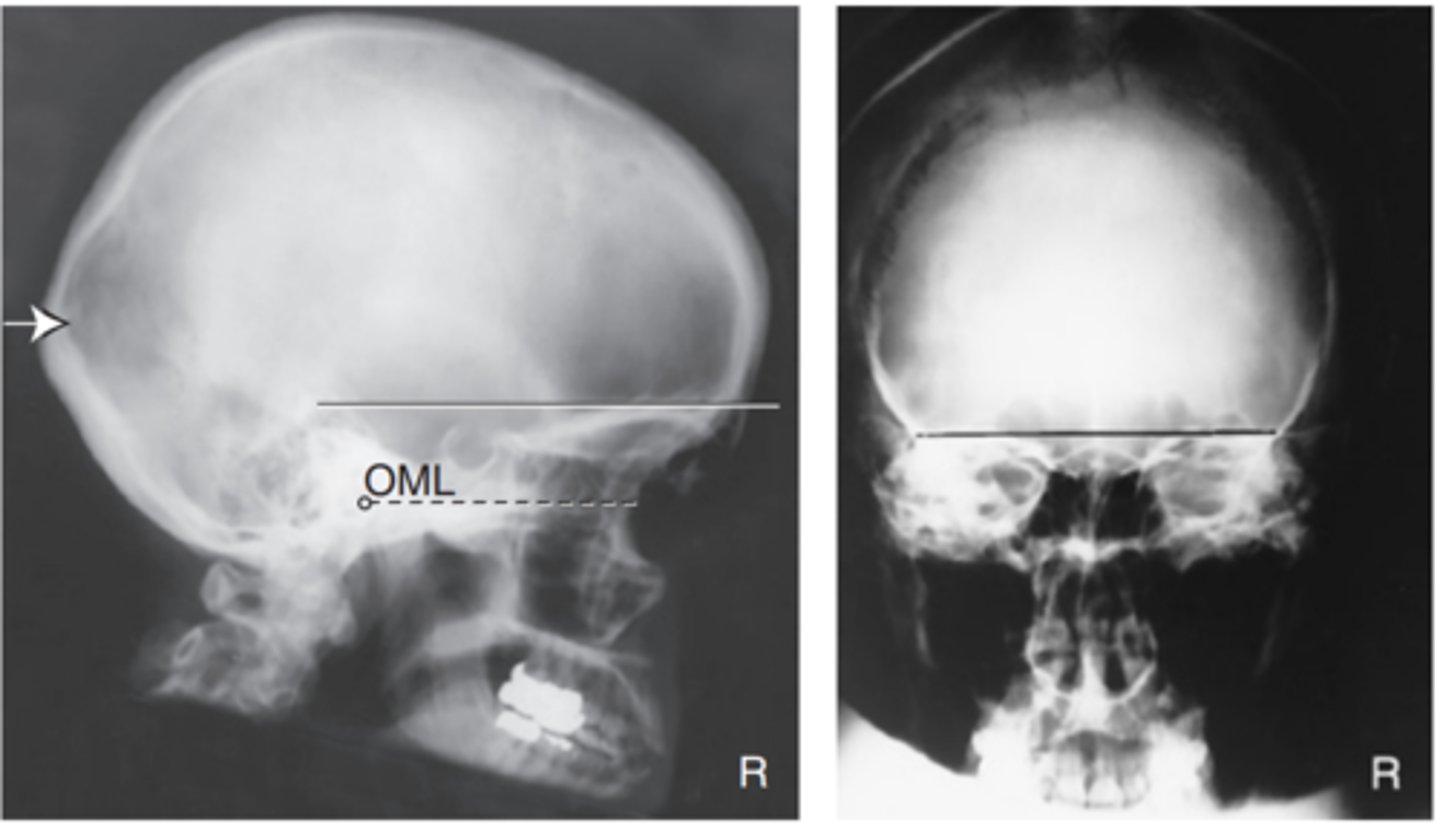
PA axial—15° caudad (Caldwell) of Skull
-Position: No rotation as assessed by equal distance from the midlateral orbital margins to the lateral cortex of the cranium on each side, superior orbital fissures symmetric within the orbits, and correct extension of neck (OML alignment).
Petrous pyramids are projected into the lower one-third of the orbits.
• Supraorbital margin is visualized without superimposition
Alternative PA axial—30° caudad
-Position: No rotation as assessed by equal distance from the midlateral orbital margins to the lateral cortex of the cranium on each side, superior orbital fissures symmetric within the orbits, and correct extension of neck (OML alignment).
Petrous pyramids are projected at or just below the IOM to allow visualization of the entire orbital margin
PA Skull CR
-Position:
• No rotation is evident, as indicated by equal distance bilaterally from lateral orbital margin to lateral cortex of skull.
• Petrous portion of temporal bone fills the orbits with the petrous ridges at the level of the supraorbital margin.
• Posterior and anterior clinoids are visualized just superior to ethmoid sinuses
Submentovertical (SMV) projection Skull
-Position:
• Correct extension of neck and relationship between IOML and CR as indicated by mandibular mentum anterior to the ethmoid sinuses.
• No rotation evidenced by the MSP parallel to edge of IR.
• No tilt evidenced by equal distance between mandibular ramus and lateral cranial cortex.

PA Axial Skull (Haas Method)
-Position:
• No rotation is evident, as indicated by bilateral symmetric petrous ridges.
• Dorsum sellae and posterior clinoid processes are visualized in the foramen magnum, which indicates correct CR angle and proper neck flexion and extension.
• No tilt as evidenced by correct placement of anterior clinoid processes within the middle of the foramen magnum
Facial Bones Routine
-Lateral
-PA Axial (Caldwell Method)
-Parietoacanthial (Waters Method)
Special Facial Bone Routines
-Modified Parietoacanthial (Waters Method)
-Addition of Nasal Bone Routine
Nasal Bone Routine
-Lateral
-Parietoacanthial (Waters)
Lateral Facial Bones
Position:
• An accurately positioned lateral image of the facial bones demonstrates no rotation or tilt.
• Rotation is evident by anterior and posterior separation of symmetric vertical bilateral structures such as the mandibular rami and greater wings of the sphenoid.
• Tilt is evident by superior and inferior separation of the orbital roofs (plates).

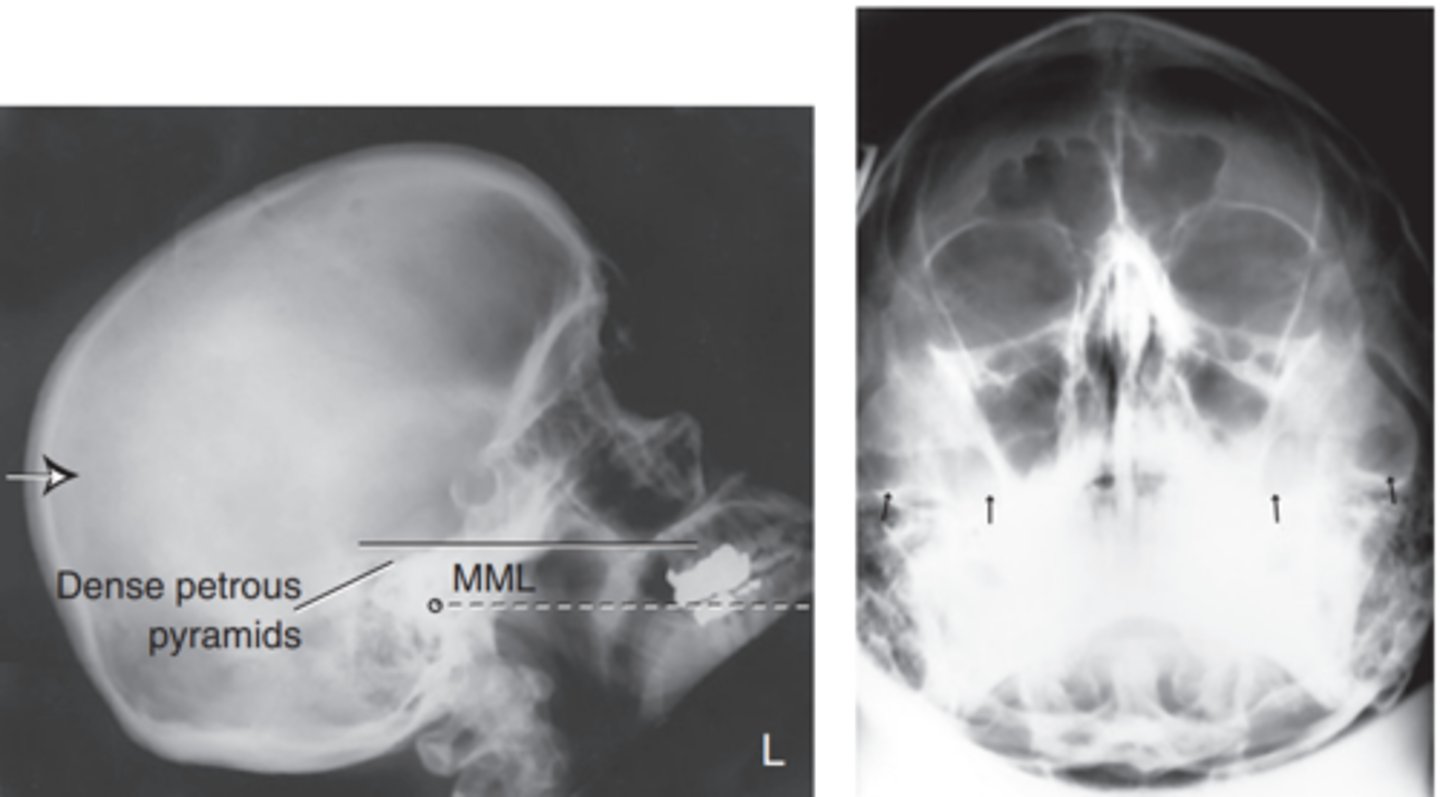
Parietocanthial projection (Waters) Facial Bones
-Position:
• Correct neck extension demonstrates petrous ridges just inferior to the maxillary sinuses
• No patient rotation exists, as indicated by equal distance from the midlateral orbital margin to the lateral cortex of cranium on each side.
PA Axial (Caldwell) Facial Bones
-Position:
• Correct patient position/CR angulation is indicated by petrous ridges projected into the lower one-third of orbits with 15° caudad CR. If the orbital floors are the area of interest, 30° caudad angle projects the petrous ridges below the IOMs.
• No rotation of cranium is indicated by equal distance from midlateral orbital margin to the lateral cortex of the cranium; superior orbital fissures are symmetric
Modified Parietoacanthial (Modified Waters) Facial Bones
-Position:
• Correct position/CR angulation is indicated by petrous ridges projected into the lower half of the maxillary sinuses, below the IOMs.
• No rotation of the cranium is indicated by equal distance from the midlateral orbital margin to the lateral cortex of the cranium.
Lateral Nasal Bones
Superoinferior Tangential (Axial) Special Nose Projection
-Position:
• No patient rotation is evident, as indicated by equal distance from anterior nasal spine to outer soft tissue borders on each side.
• Incorrect neck position is indicated by visualization of alveolar ridge (excessive extension) or visualization of too much glabella (excessive flexion).

Optic Foramina Routine
-Modified Parietoacanthial (Modified Waters) - Facial Bone Projection
-PA Axial (Caldwell) - Facial Bone ProjectionCopyright © 2014 by Mosby, an imprint of Elsevier Inc. 81
Axiolateral oblique (general survey)
-Position:
• The appearance of the image/position of the patient depends on the structures under examination.
• For the ramus and body, the ramus of interest is demonstrated with no superimposition from the opposite mandible (indicating correct CR angulation).
• No superimposition of the cervical spine by the ramus should occur (indicating sufficient extension of neck).
• The ramus and body should be demonstrated without foreshortening (indicating correct rotation of head).
• The area of interest is demonstrated with minimal superimposition and minimal foreshortening
PA Mandible
-Position:
• No patient rotation exists, as indicated by mandibular rami visualized symmetrically, lateral to the cervical spine.
• Midbody and mentum are faintly visualized, superimposed on cervical spine.
PA Axial Mandible (CR 20° cephalad)
-Position:
• No patient rotation exists, as indicated by mandibular rami visualized symmetrically, lateral to the cervical spine.
• Midbody and mentum are faintly visualized, superimposed on cervical spine.
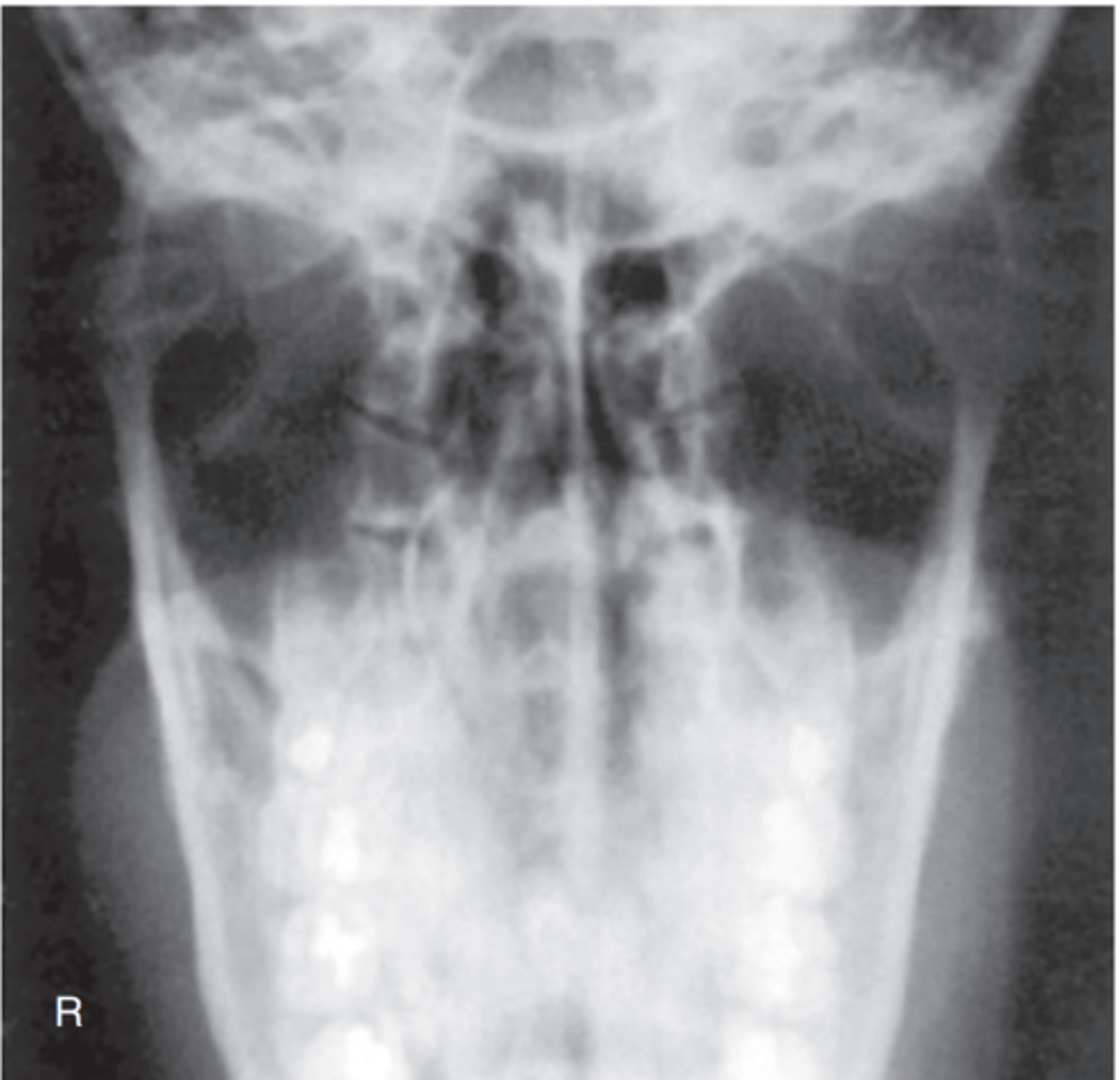
AP Axial Projection (Towne) Mandible
-Position: A correctly positioned image with no rotation demonstrates the following: condyloid processes visualized symmetrically, lateral to the cervical spine; clear visualization of condyle/TM fossae relationship, with minimal superimposition of the TM fossae and mastoid portions

Submetovertical SMV Projection Mandible
-Position:
• Correct neck extension is indicated by the following: mandibular symphysis superimposing frontal bone; mandibular condyles projected anterior to petrous ridges. • No patient rotation or tilt is indicated by the following: no tilt as evidenced by equal distance from mandible to lateral border of skull; no rotation as evidenced by symmetric mandibular condyles

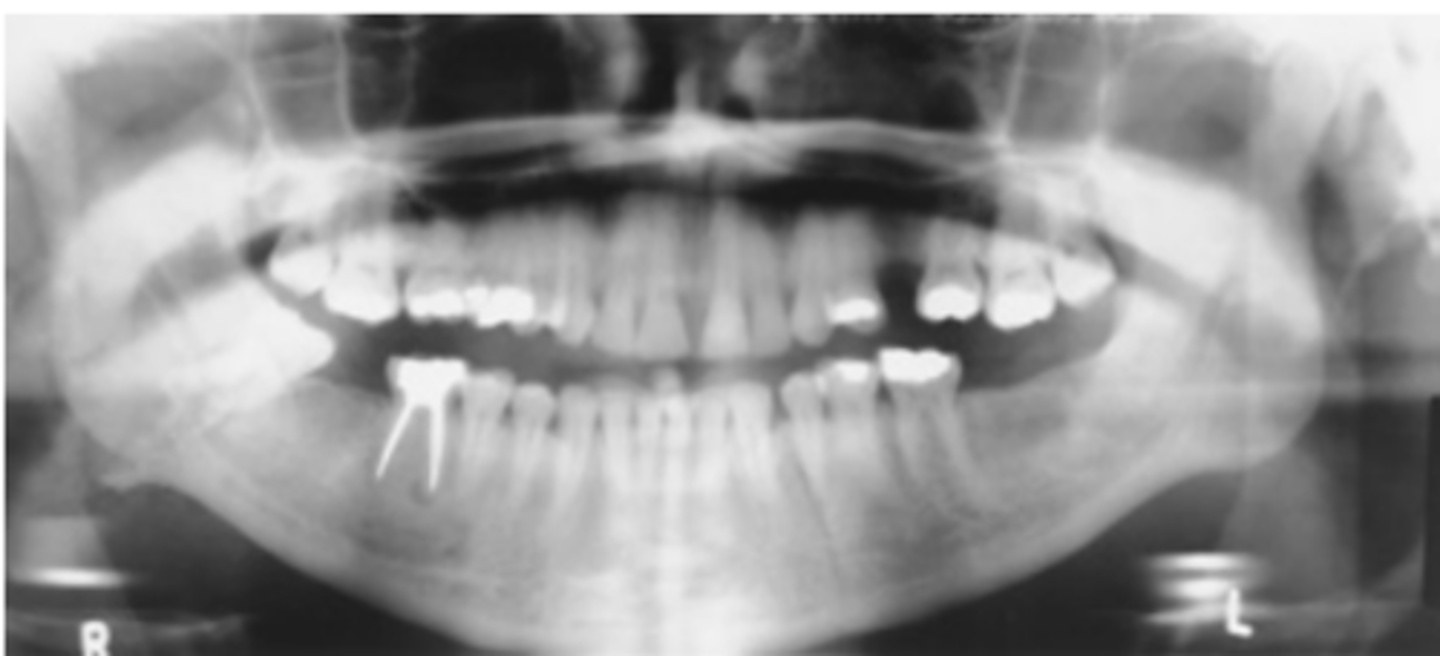
Panorex
-Position: The mandible visualized without rotation or tilting is indicated by the following: TMJs on the same horizontal plane in the image; rami and posterior teeth equally magnified on each side of the image; anterior and posterior teeth sharply visualized with uniform magnification
TMJ Routine
-AP Axial (Modified Towne)
-Axiolateral 15° oblique (Modified Law)
OR
-Axiolateral (Schuller)
AP Axial Projection (Modified Towne) TMJ
-Position: Correctly positioned patient, with no rotation, is indicated by the following: condyloid processes visualized symmetrically, lateral to the cervical spine; clear visualization of condyle and TM fossae relationship.
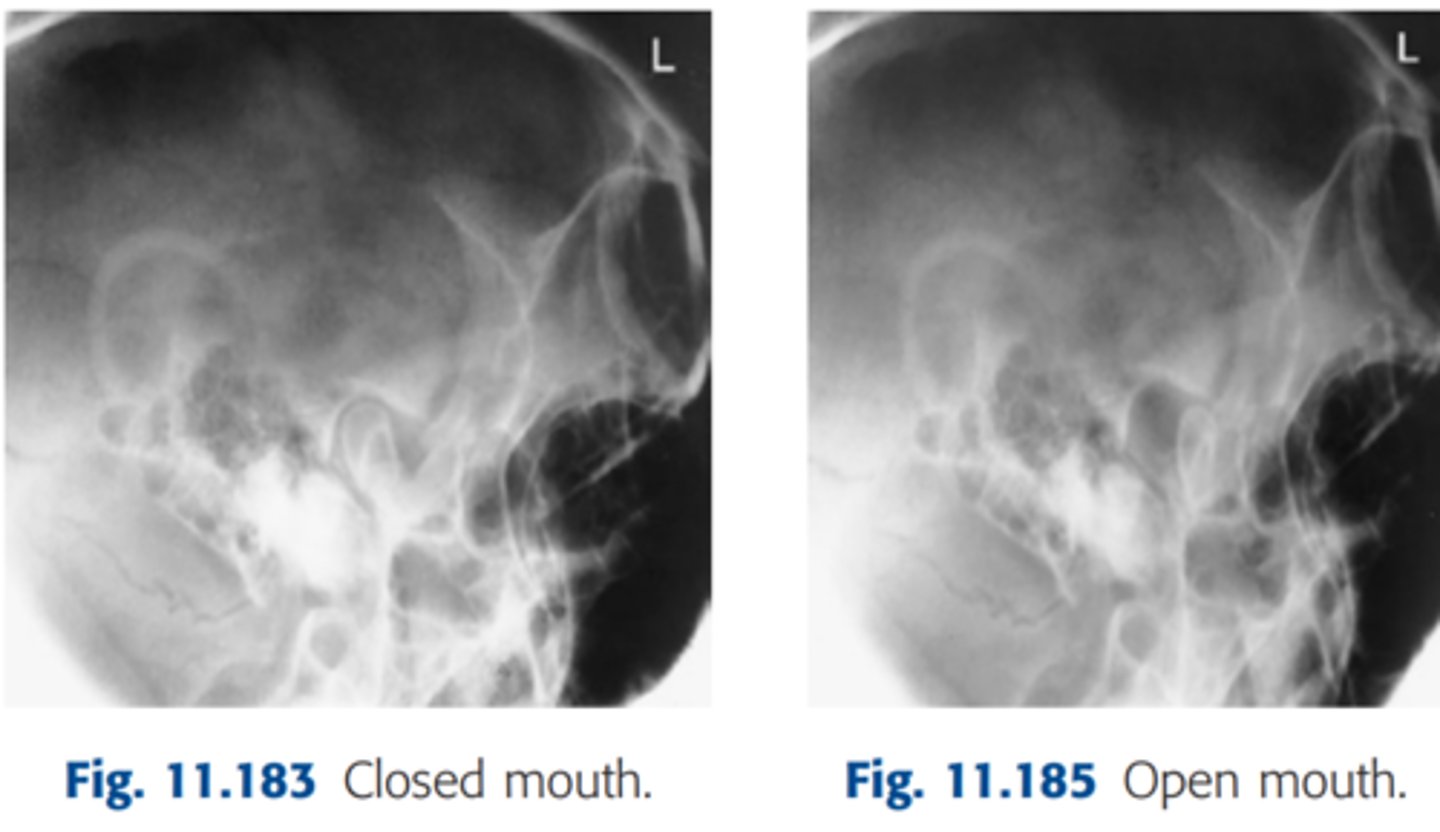
Axiolateral Oblique (Modified Law) TMJ
-Position: Correctly positioned images demonstrate TMJ closest to IR clearly, without superimposition of opposite TMJ (15° rotation prevents superimposition).
• TMJ of interest is not superimposed by cervical spine
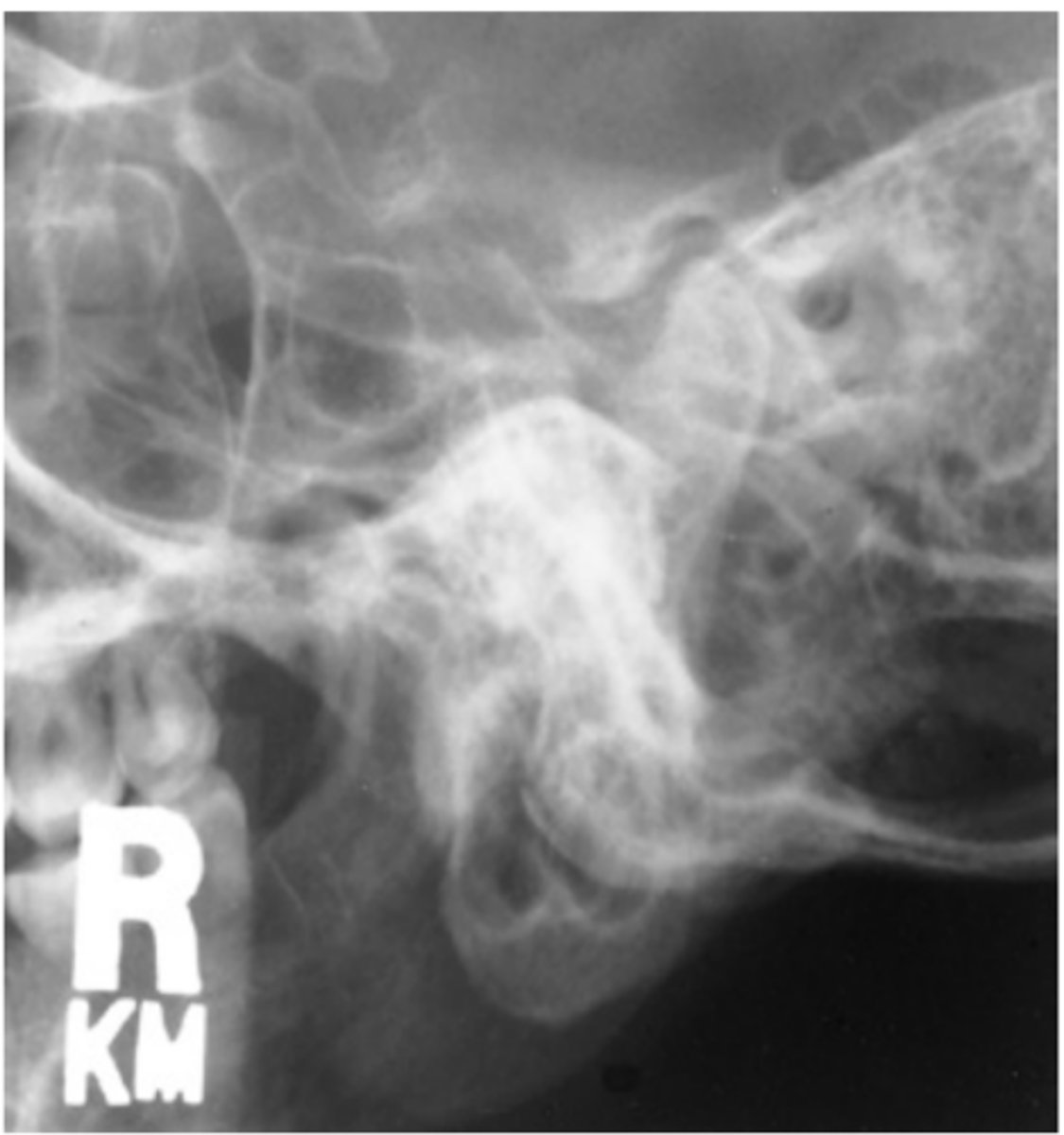
Axiolateral Projection (Schuller Method) TMJ
-Position: TMJs are demonstrated without rotation, as evidenced by superimposed lateral margins
Lateral Sinuses
-Position:
• Accurately positioned cranium without rotation or tilt.
• Rotation is evident by anterior and posterior separation of symmetric bilateral vertical structures such as the mandibular rami and greater wings of the sphenoid.
• Tilt is evident by superior and inferior separation of symmetric horizontal structures such as the orbital roofs (plates) and greater wings of sphenoid
PA Caldwell Sinuses
-Position: no rotation or tilt is indicated by the following: equal distance from the lateral margin of the orbit to the lateral cortex of the cranium on both sides; equal distance from the MSP (identified by the crista galli) to the lateral orbital margin on both sides; superior orbital fissures symmetrically visualized within the orbits.

Parietocanthial Waters Sinuses
-Position: No rotation of the cranium is indicated by the following: equal distance from MSP (identified by the bony nasal septum) to lateral orbital margin on both sides; equal distance from the lateral orbital margin to the lateral cortex of the cranium on both sides.
• Adequate extension of neck demonstrates petrous ridges just inferior to the maxillary sinuses
SMV Sinuses
-Position:
• Accurate IOML and CR relationship is demonstrated by the following: correct extension of neck and relationship between IOML and CR as indicated by mandibular mentum anterior to ethmoid sinuses.
• No rotation evidenced by MSP parallel to edge of IR.
• No tilt evidenced by equal distance between mandibular ramus and lateral cranial cortex

Parietoacanthial Transoral (Open-Mouth Waters) Sinuses
-Position: No rotation of the cranium is indicated by the following: equal distance from the MSP (identified by the bony nasal septum) to the lateral orbital margin on both sides; equal distance from the lateral orbital margin to the lateral cortex of the cranium on both sides; accurate extension of the neck demonstrating petrous ridges just inferior to the maxillary sinuses
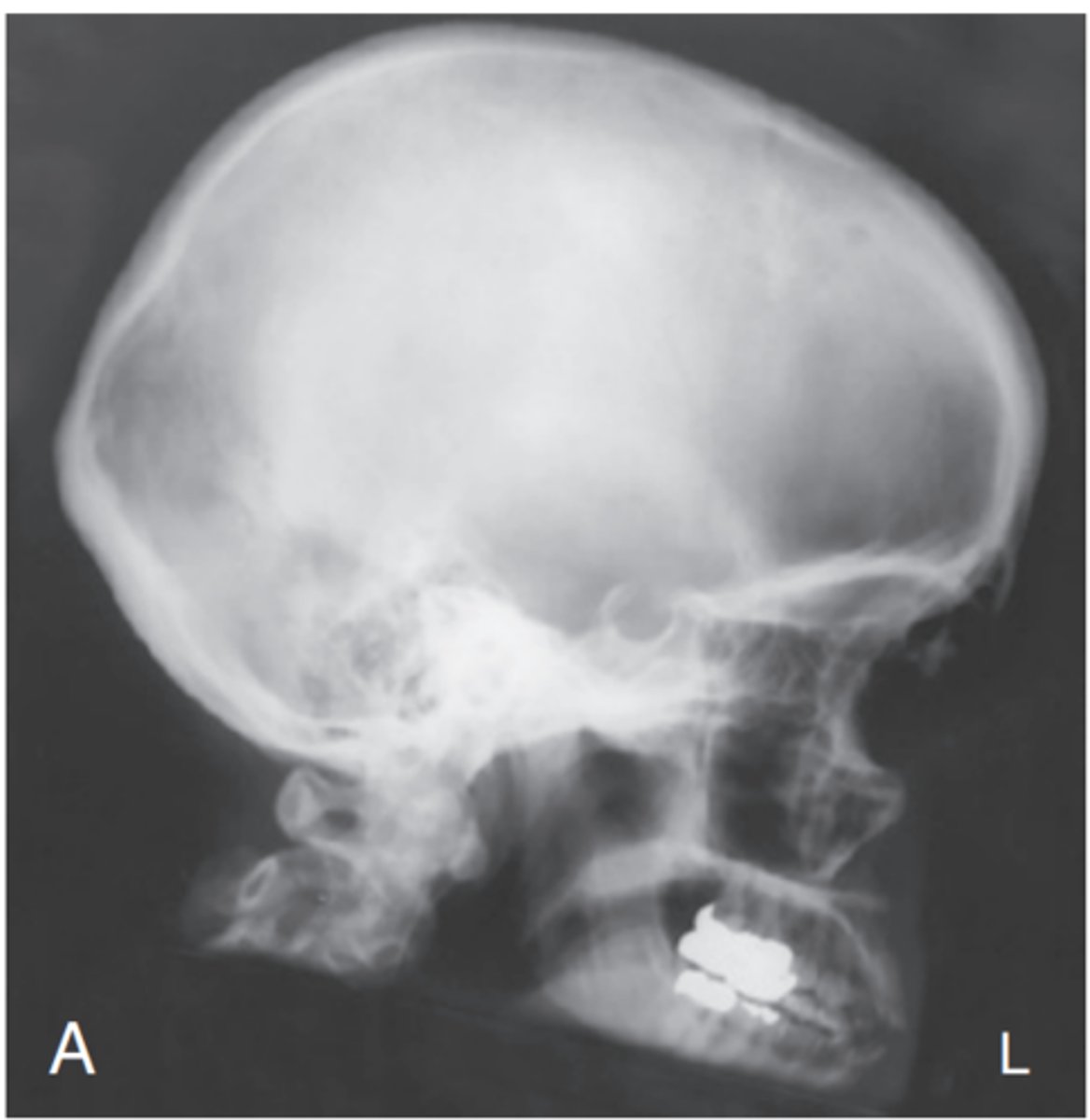
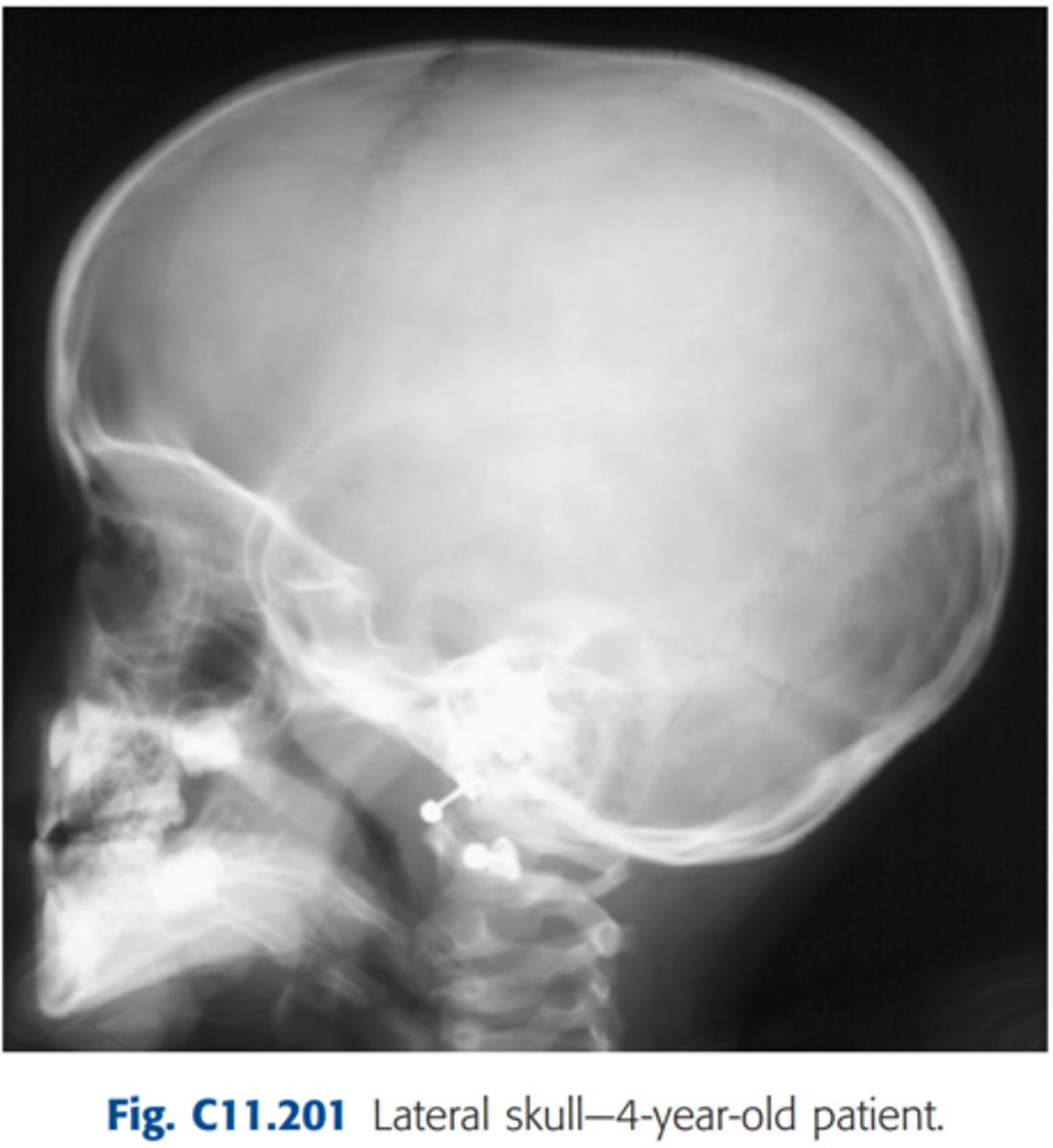
Critique Lateral Skull (Fig.201)
Repeatable errors (three)—
Criterion 1: Anatomy demonstrated: Foreign bodies (earrings) obscure essential anatomy.
Criterion 4: Exposure: In most departments, this would be sufficiently underexposed to be repeatable.
Criterion 5: Anatomic side markers: No anatomic side marker is visible.
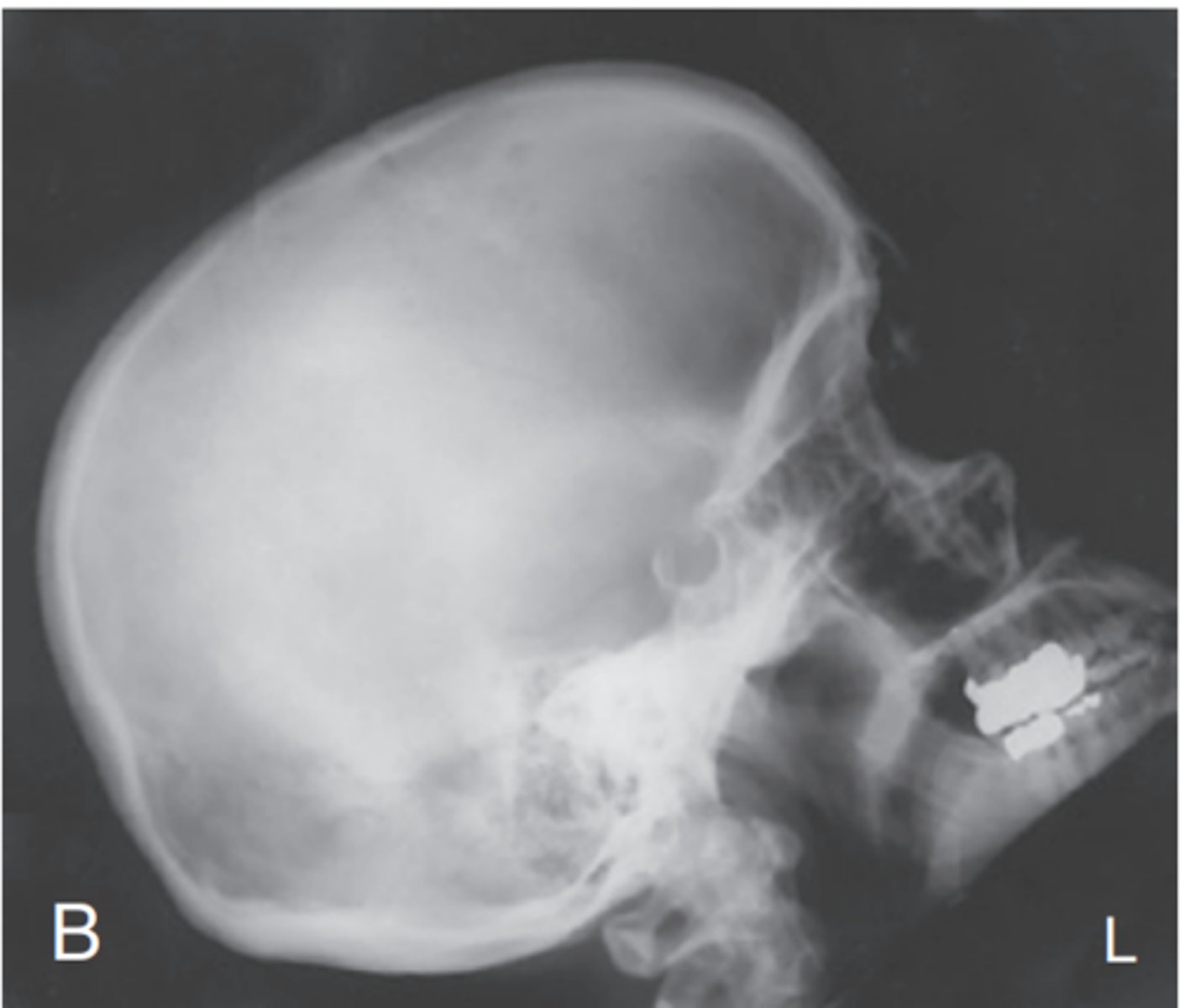
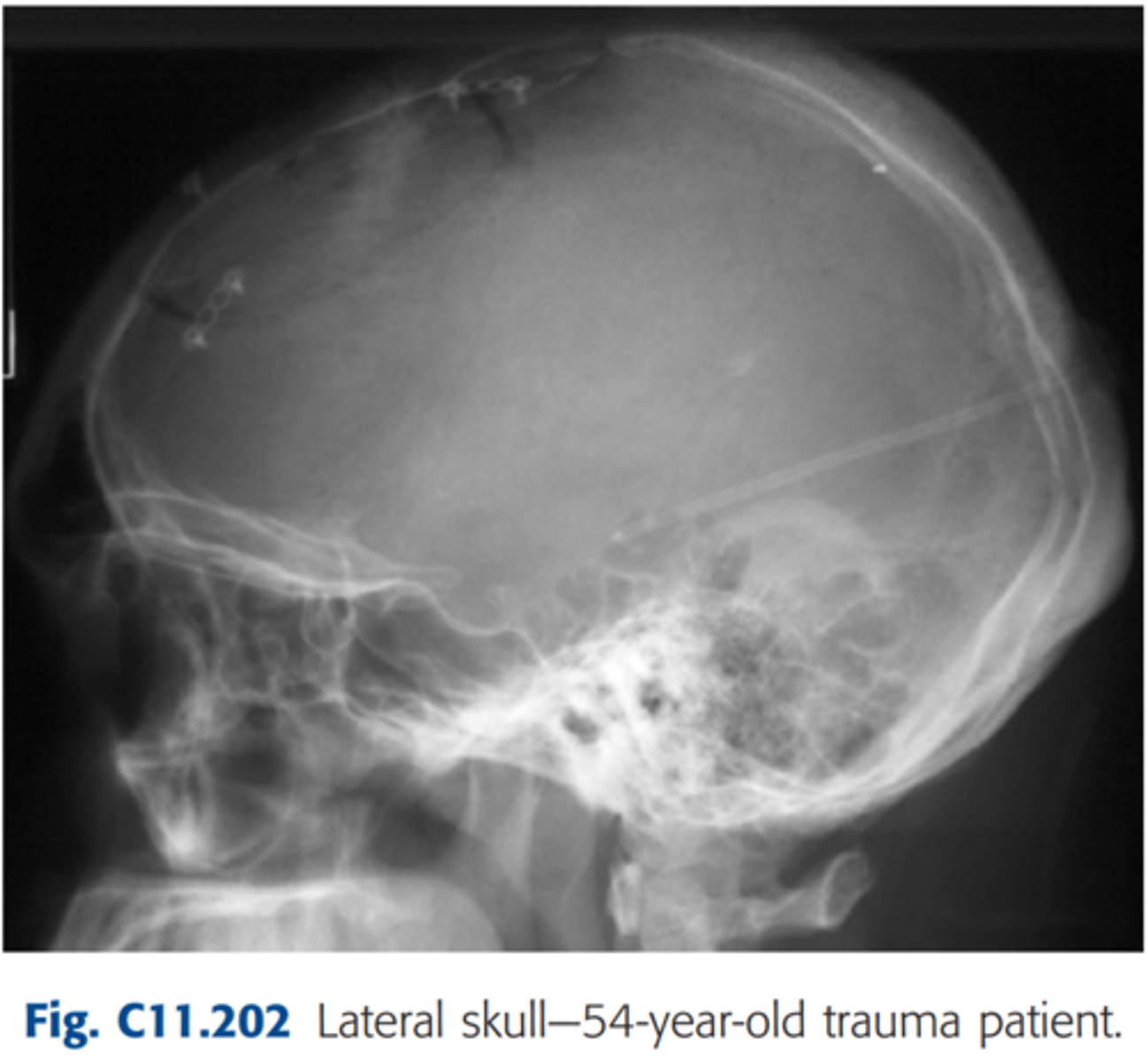
Critique Lateral Skull (Fig.202)
Repeatable errors (four)—
Criterion 1: Anatomy demonstrated: The vertex (region of skull trauma) and posterior aspect of the skull appears to be just slightly cut off (region of skull trauma).
Criterion 2: Positioning: The skull is tilted and rotated. (Note the separation of the orbital plates from the tilt and separation of the greater wings of the sphenoid, the rami of the mandible, and the EAMs, indicating rotation and tilt).
Criterion 3: Collimation and CR: CR centered too anterior to skull.
Criterion 5: Anatomic side markers: Anatomic side marker is partially demonstrated.
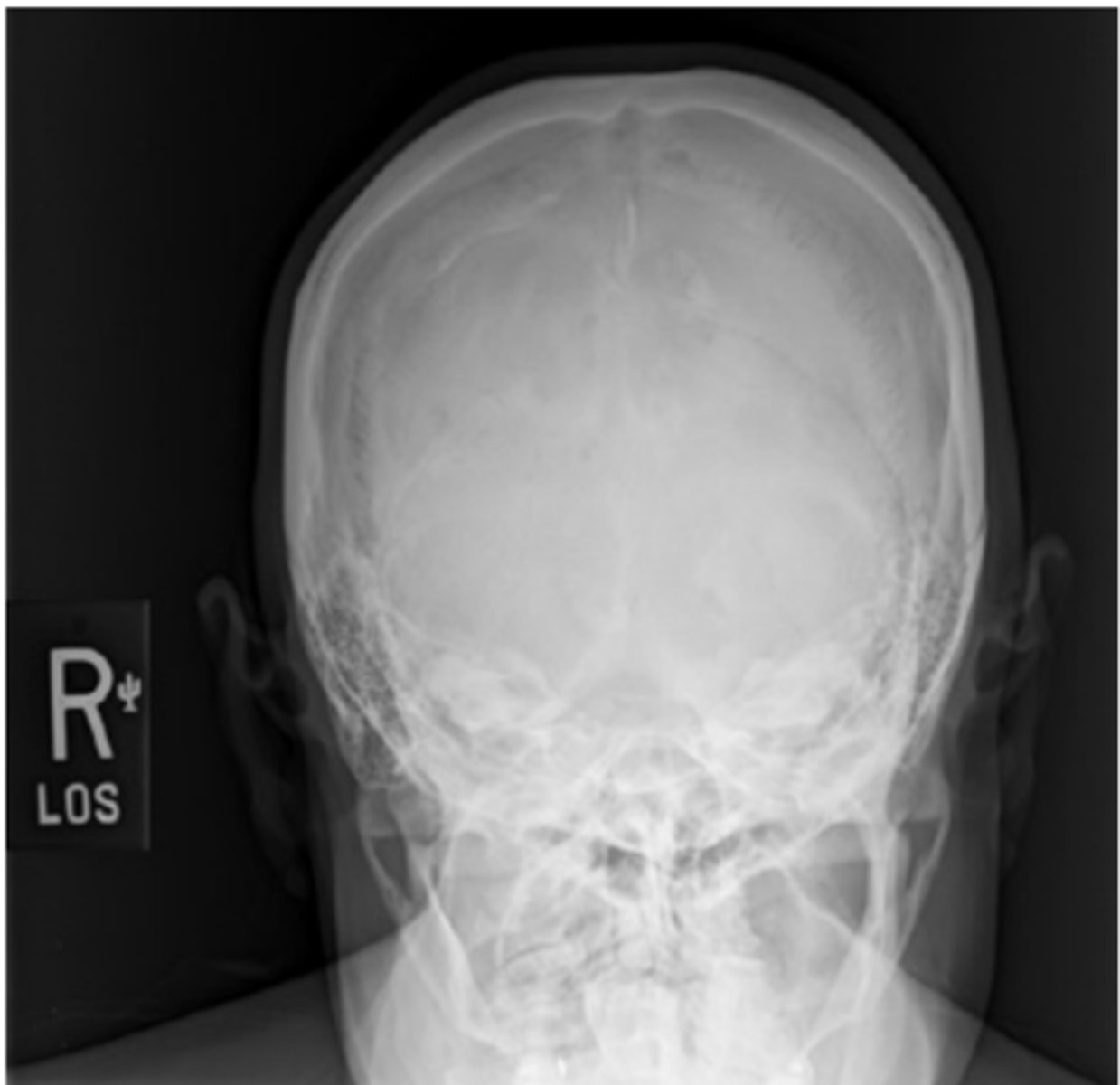
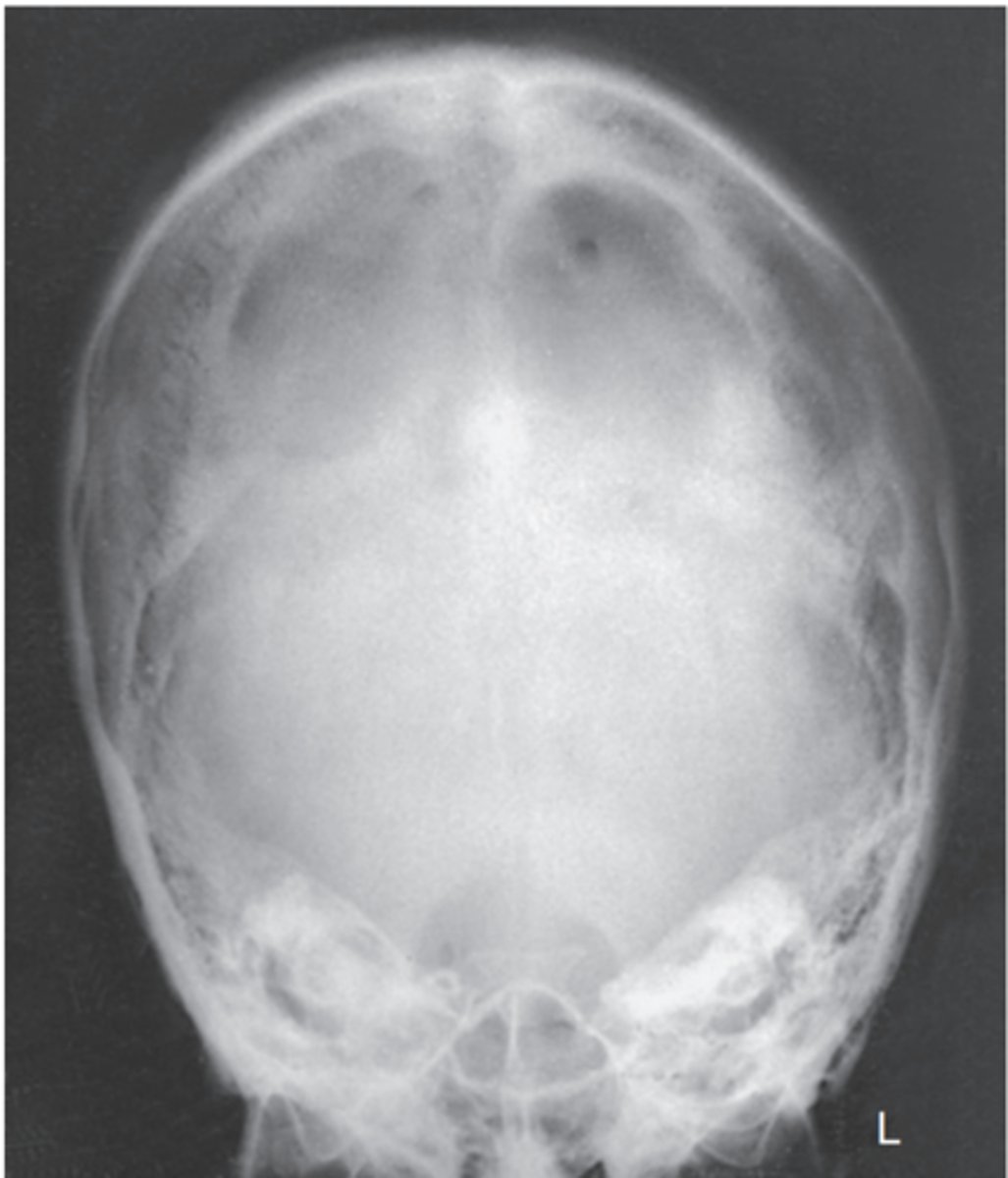
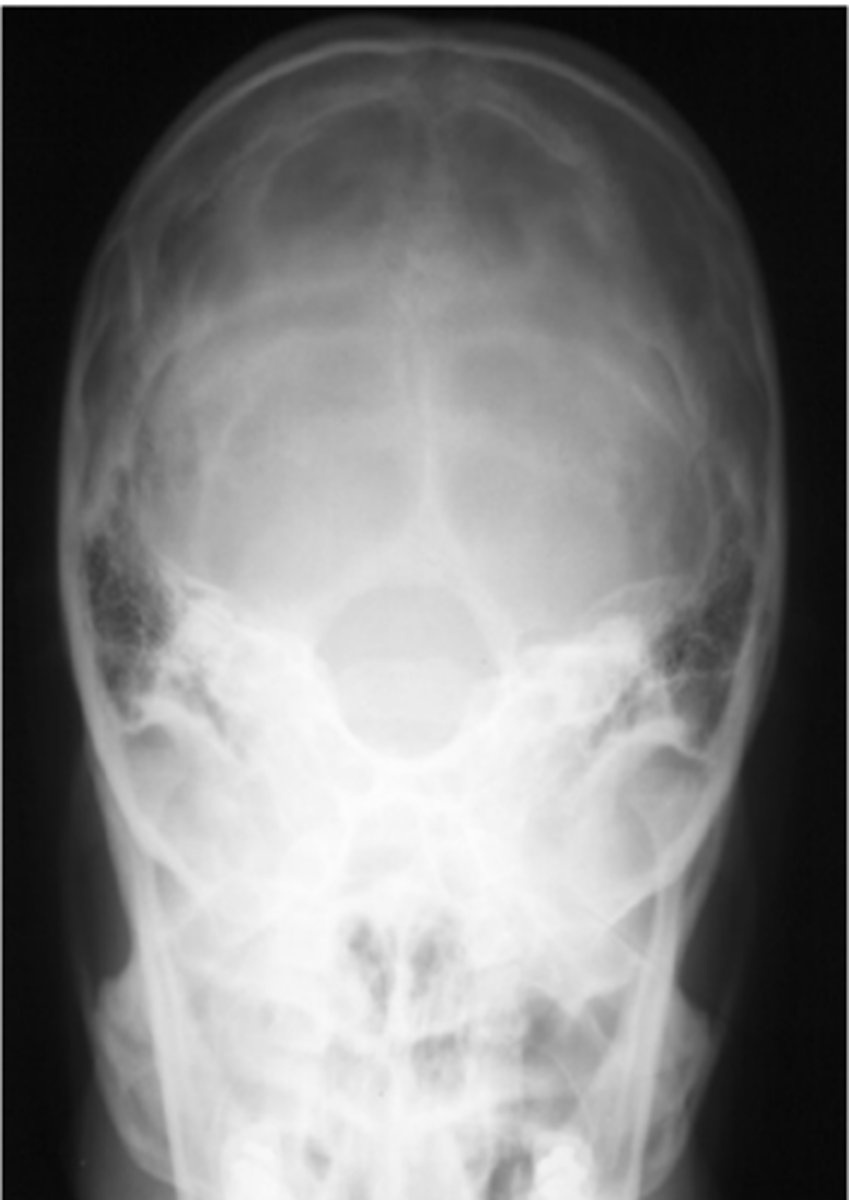
Critique AP Axial (Towne) Skull
Repeatable errors (three)—
Criterion 3: Collimation and CR: CR is overangled.* The anterior arch of C1 (rather than the dorsum sellae) is projected into the foramen magnum.
Criterion 4: Exposure: Mid/lower aspect of skull underexposed (analogy).
Criterion 5: Anatomic side markers: There is no evidence of side marker.
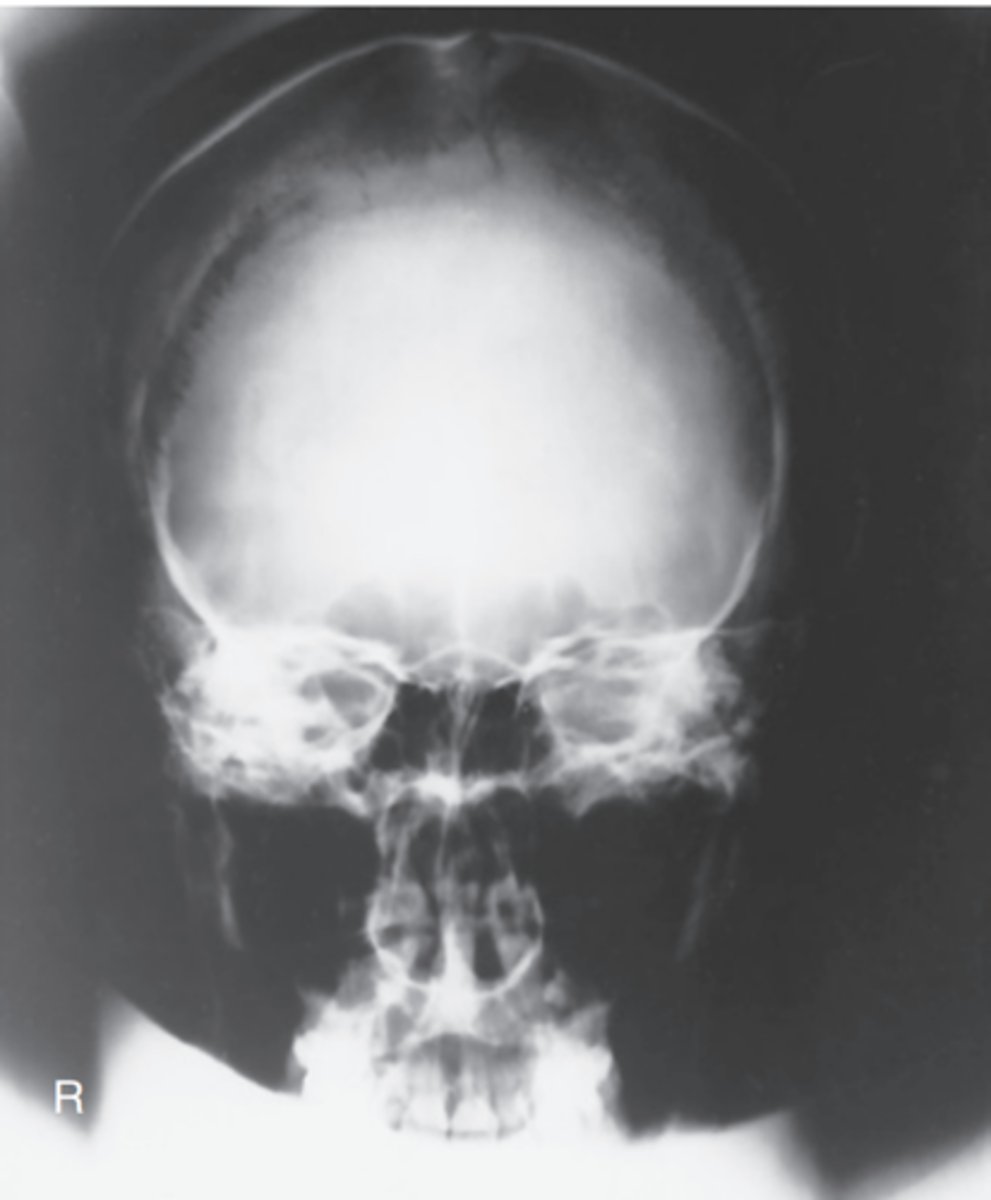
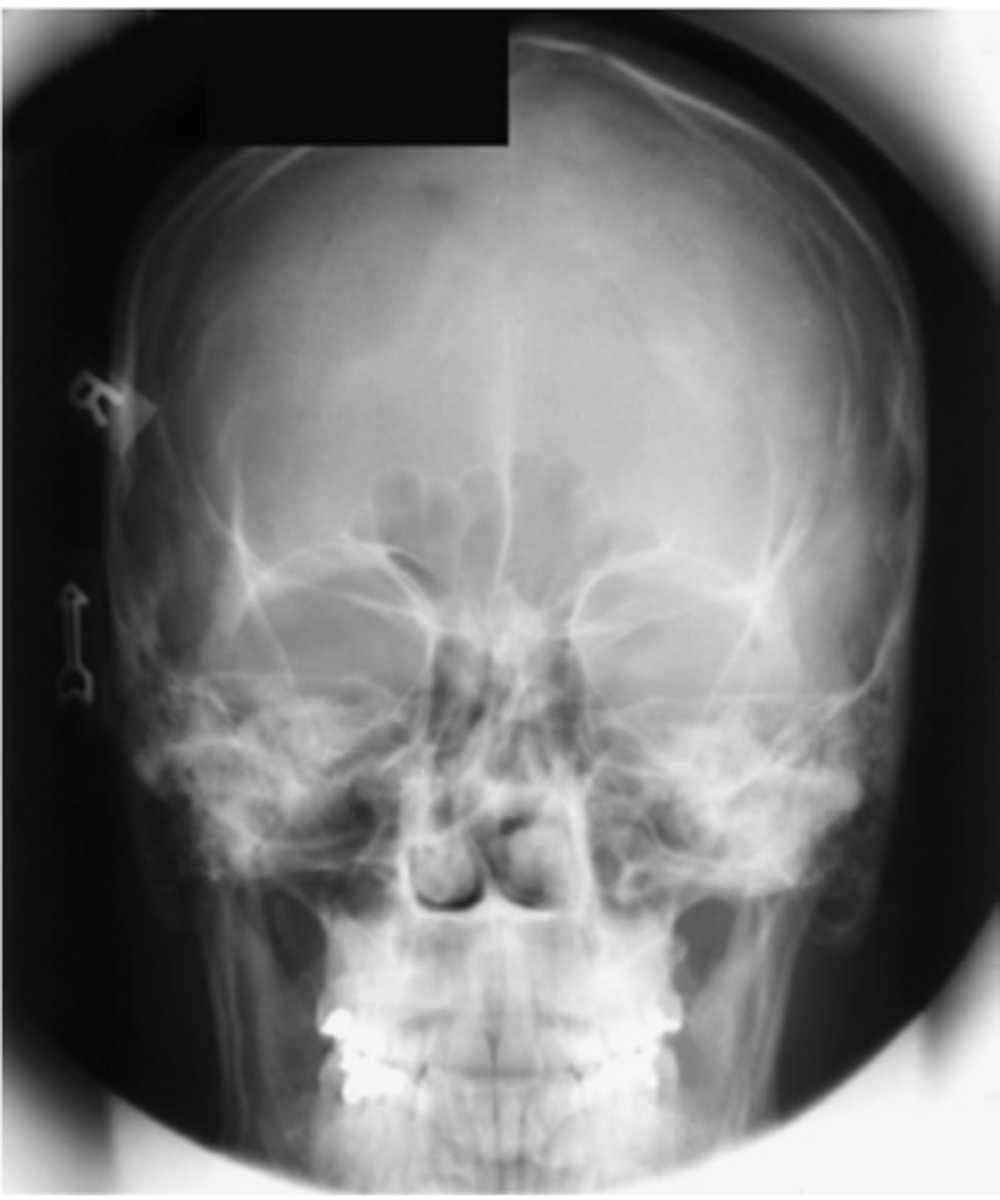
Is this a PA or AP projection? are there any errors?
-This is an AP 15° cephalad projection, as evidenced by the large size of the orbits resulting from magnification caused by increased OID
Repeatable errors (three)—
Criterion 2: Positioning
Criterion 3: Collimation and CR: The petrous ridges are not projected into the lower one-third of orbits. More flexion of neck or less CR angulation is required. The skull also is slightly rotated (note distance between orbits and lateral margins of skull) and tilted.
Criterion 5: Anatomic side markers: Anatomic side marker is missing.

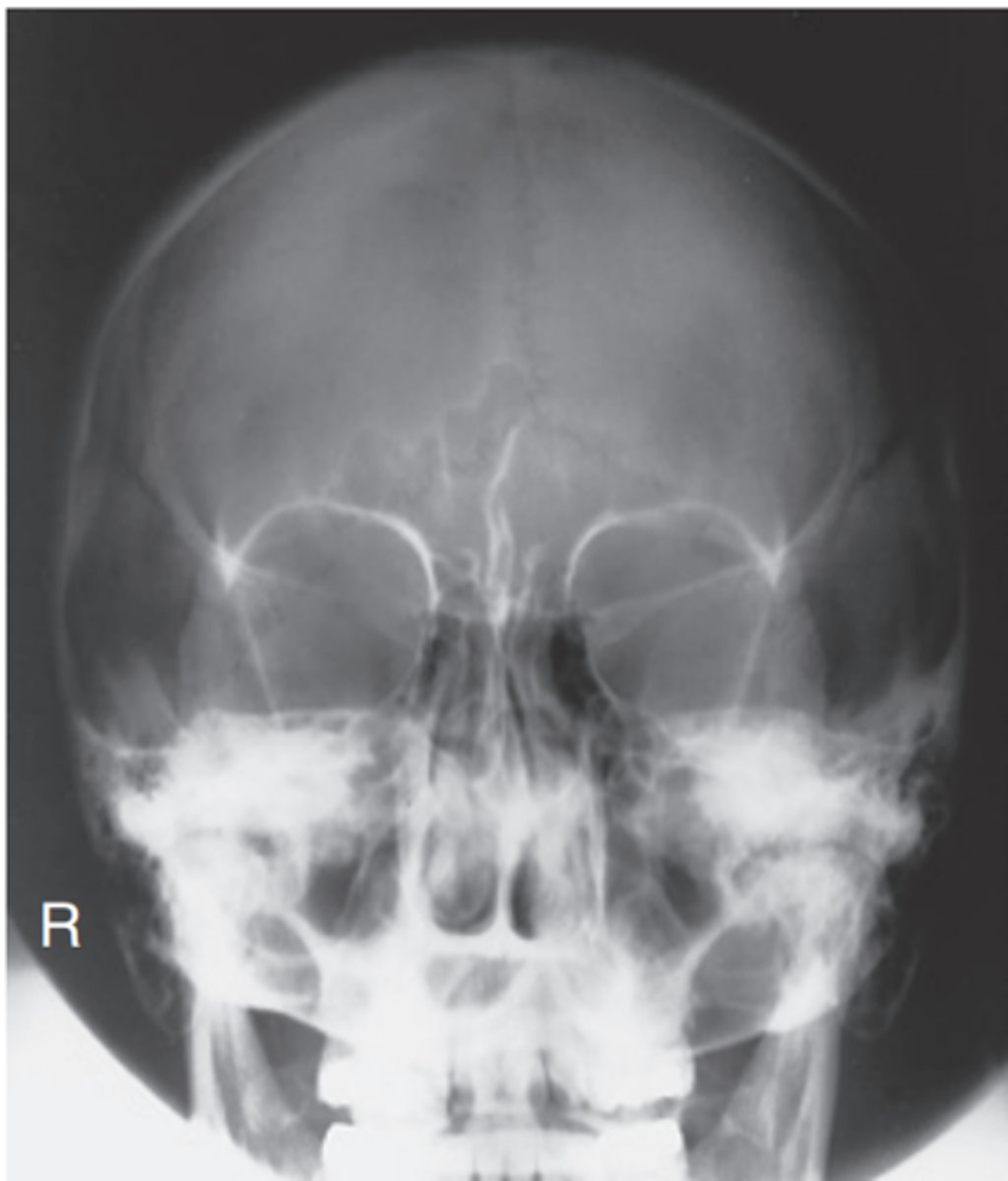
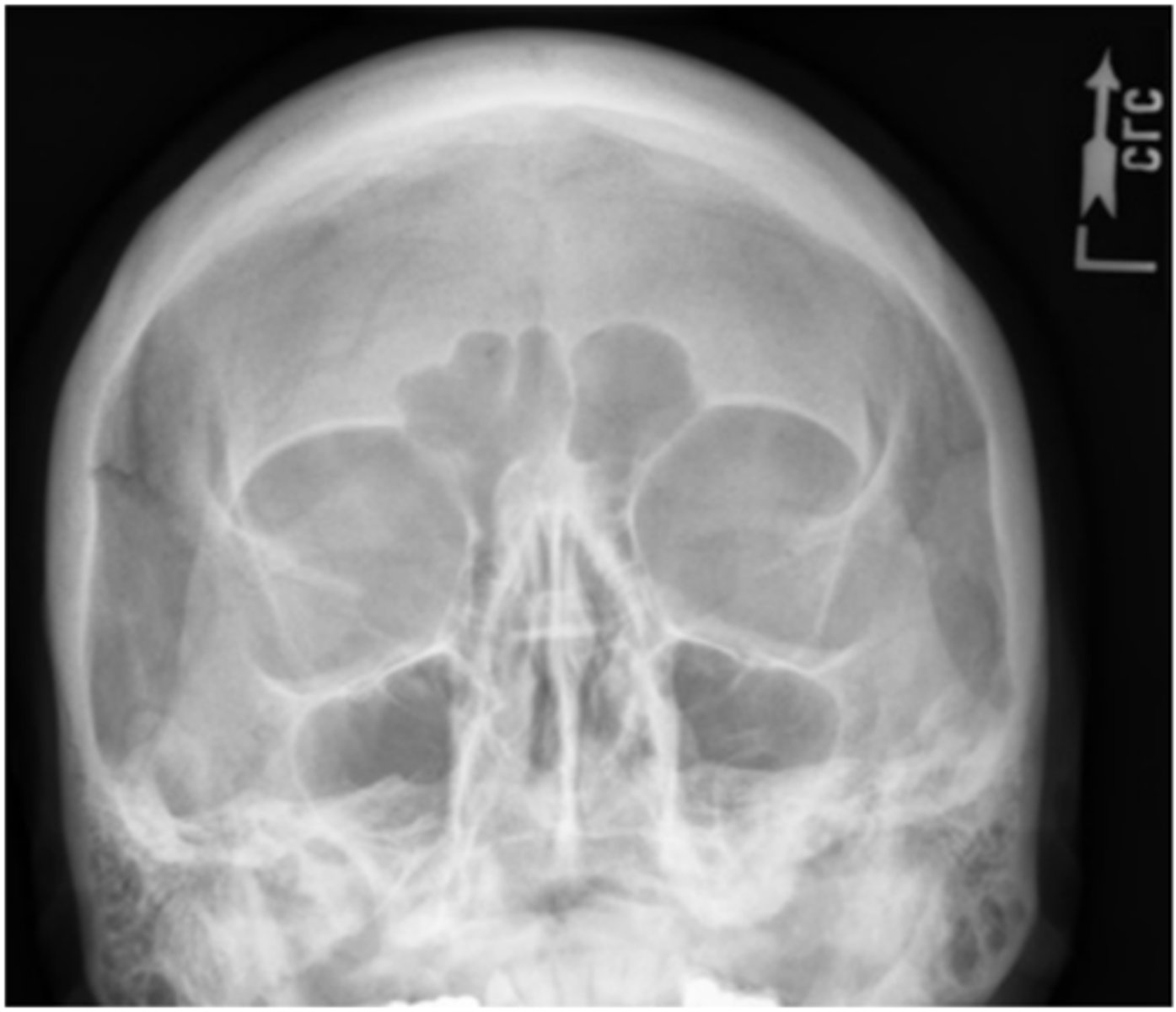
Is this Caldwell projection PA or AP Axial? are there any errors?
This is a PA 15° Caldwell projection.
Repeatable errors (two)—
Criterion 1: Anatomy demonstrated: Patient identification marker (analog cassette) and side marker are obscuring skull.
Criterion 5: Anatomic side markers: Anatomic side marker is evident but placed over skull; patient identification marker is over upper right cranium.
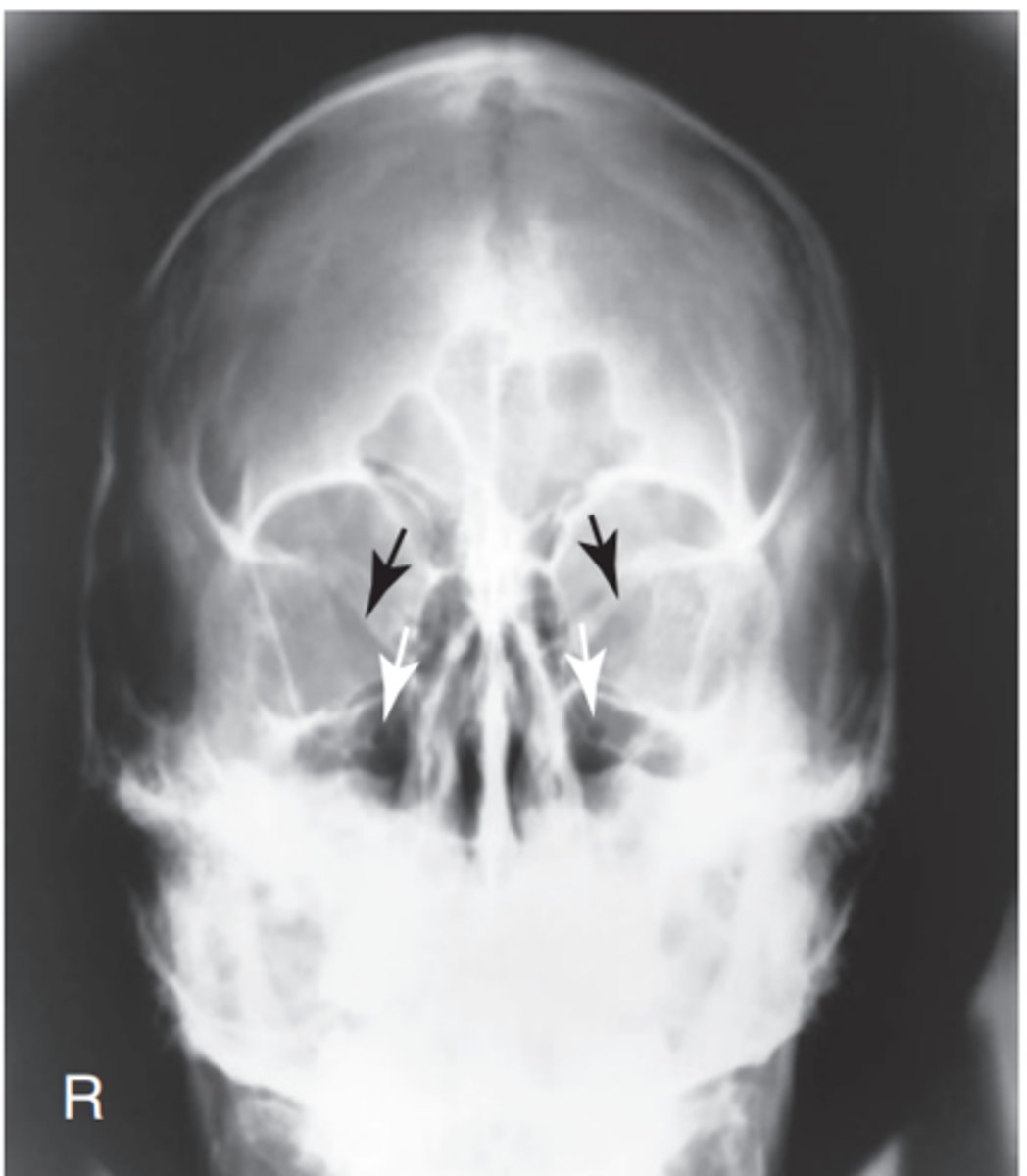
Critique this Parietocanthial Waters
Repeatable errors (three)—
Criterion 2: Positioning: Skull and neck are underextended, as evidenced by projection of petrous ridges into lower portion of maxillary sinuses. There is a slight tilt to the left.
Possibly Criterion 3: Collimation and CR: Collimation can be increased to minimize exposure to skull and neck region. CR is centered slightly too high.

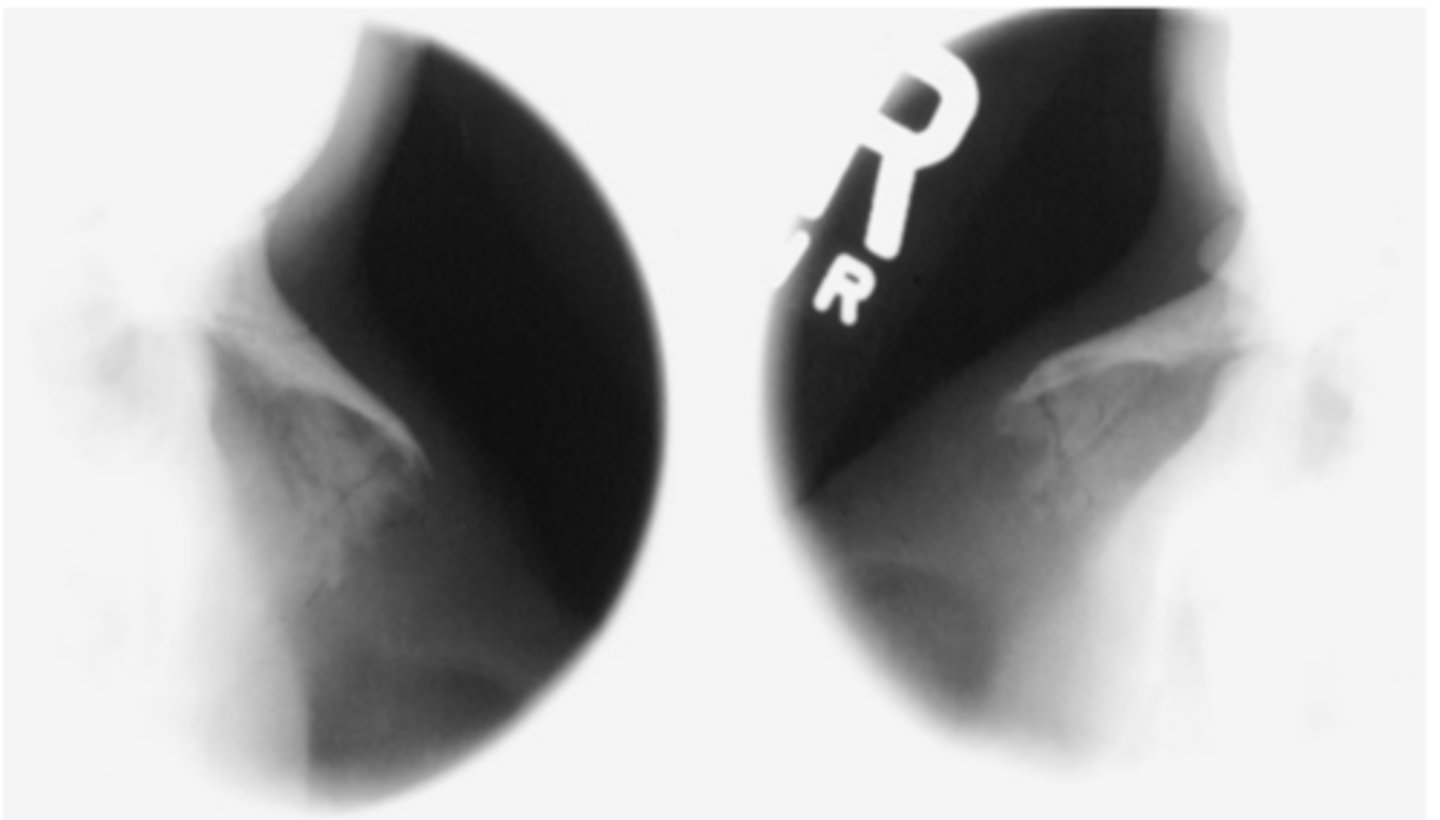
Critique this SMV Mandible
Repeatable errors (two)—
Criterion 2: Positioning: Skull is underextended (IOML was not parallel to IR and was not perpendicular to CR). Mandible is foreshortened, and rami are projected into temporal bone.
Criterion 5: Anatomic side markers: No anatomic side marker is visible
Critique this Optic Foramina Rhese Method (Fig.208)
Repeatable errors (two)—
Criterion 2: Positioning: Skull is rotated excessively toward a PA. The skull is rotated greater than 53° from the lateral position toward PA. This results in projection of the optic foramina into the middle lower aspect of the orbit. (for correctly positioned parieto-orbital, oblique Rhese method radiographs with the optic foramina projected into lower outer quadrants of orbits.)
Criterion 5: Anatomic side markers: No anatomic side marker is visible.
Critique this Optic Foramina Rhese Method (Fig.209)
Repeatable errors (three)—
Criterion 1: Anatomy demonstrated: Optic foramen is distorted and into lateral orbital wall due to poor positioning.
Criterion 2: Positioning: Skull appears to be overextended. (The AML was not perpendicular.) This projects the optic foramina into the infraorbital rim structure. The skull also appears to be under-rotated, toward a lateral position.
Criterion 5: Anatomic side markers: There is no evidence of anatomic side markers
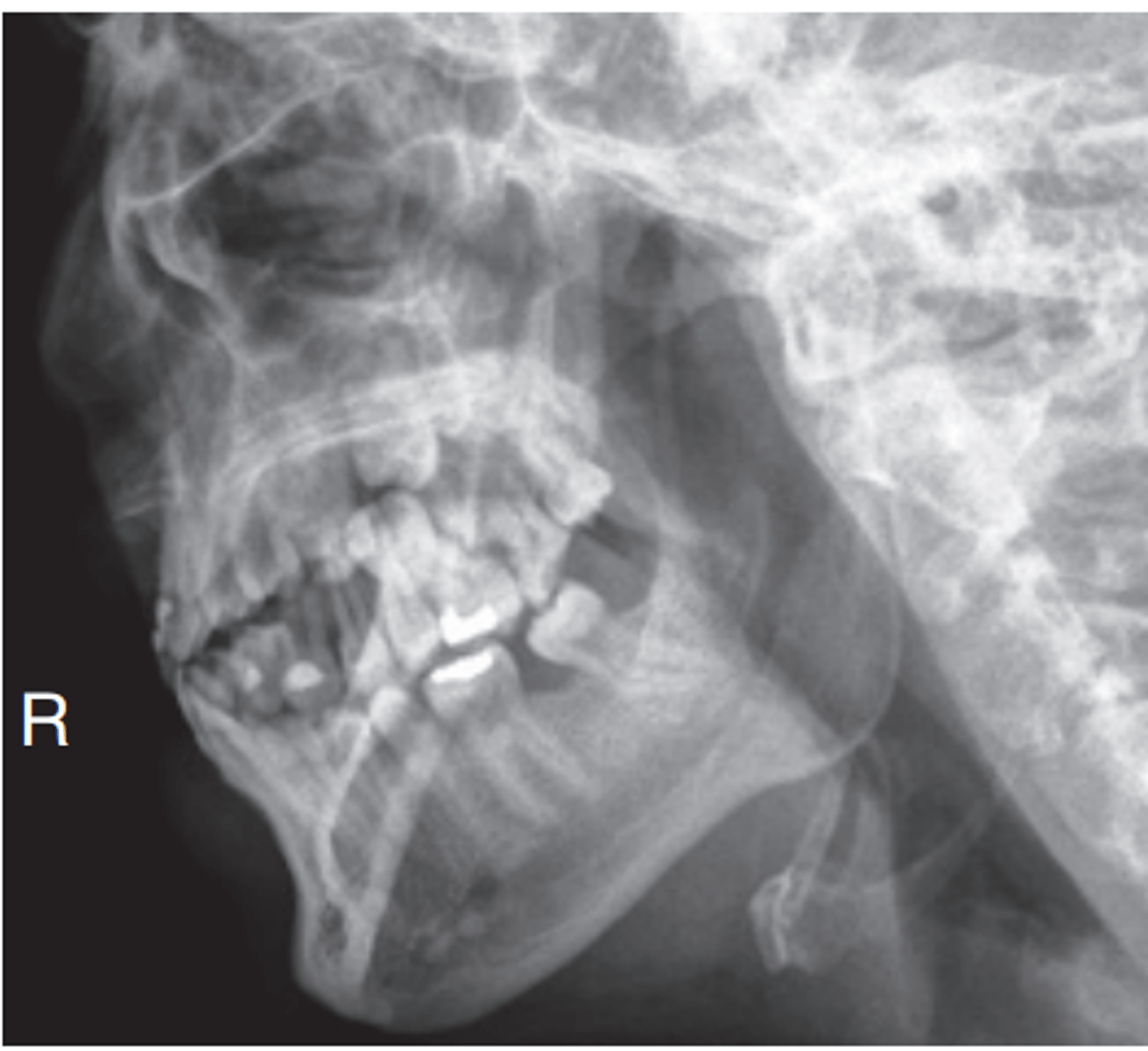
Critique this Lateral Facial Bones
Repeatable errors (two)—
Criterion 2: Positioning: Skull is rotated. (Note the separation of rami of mandible, greater wings of sphenoid, and orbits.)
Criterion 5: Anatomic side markers: No anatomic side marker is visible

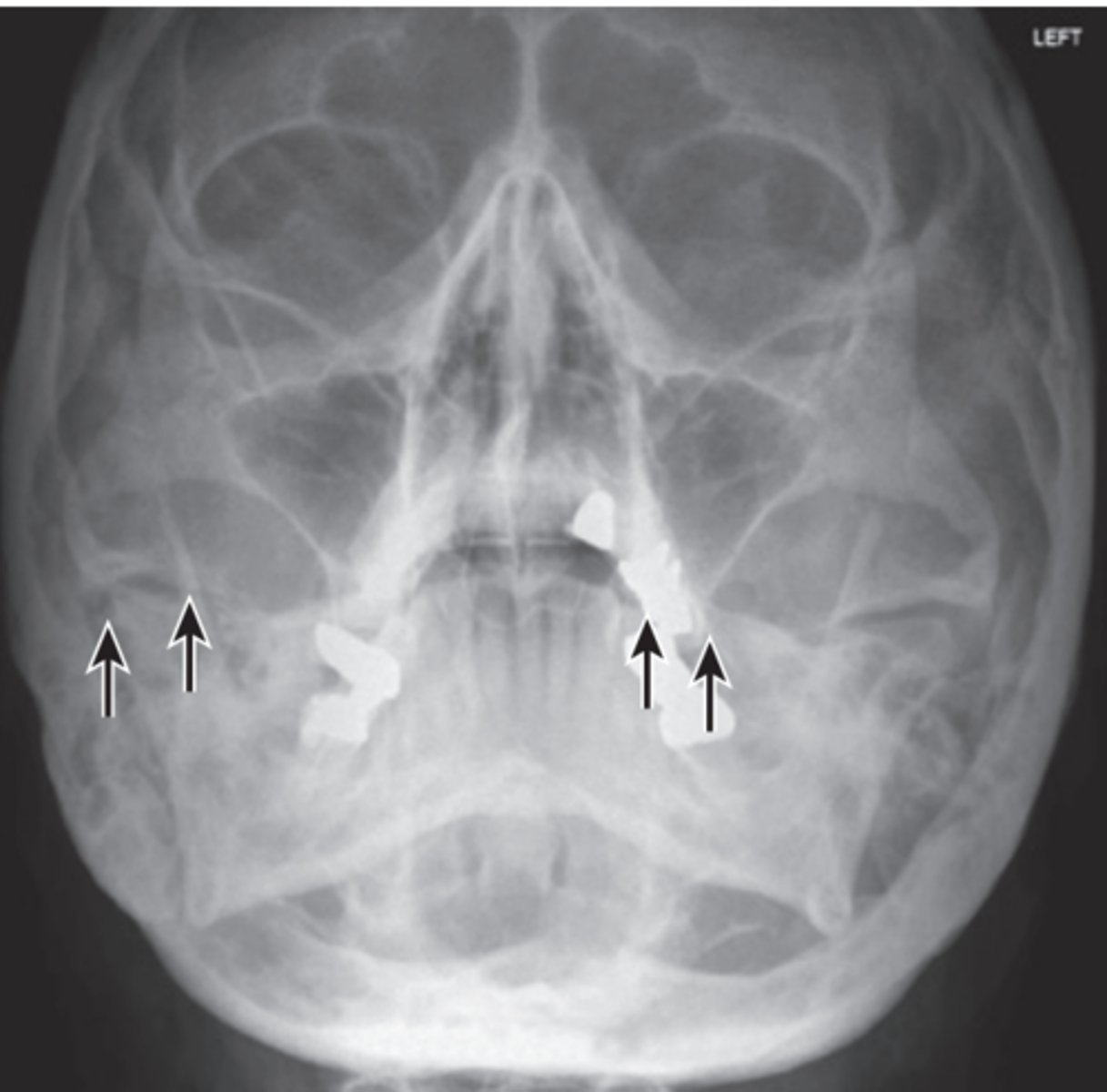
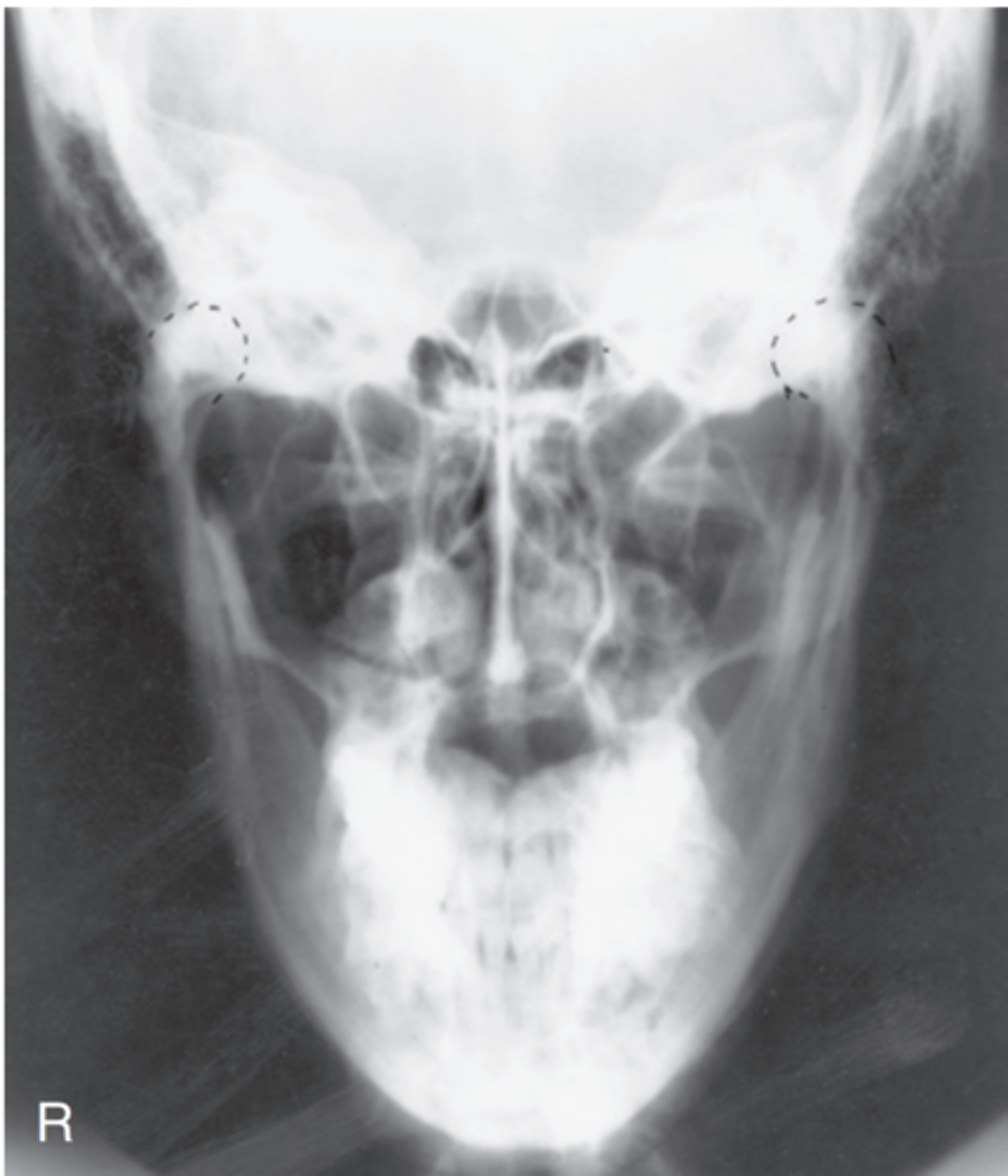
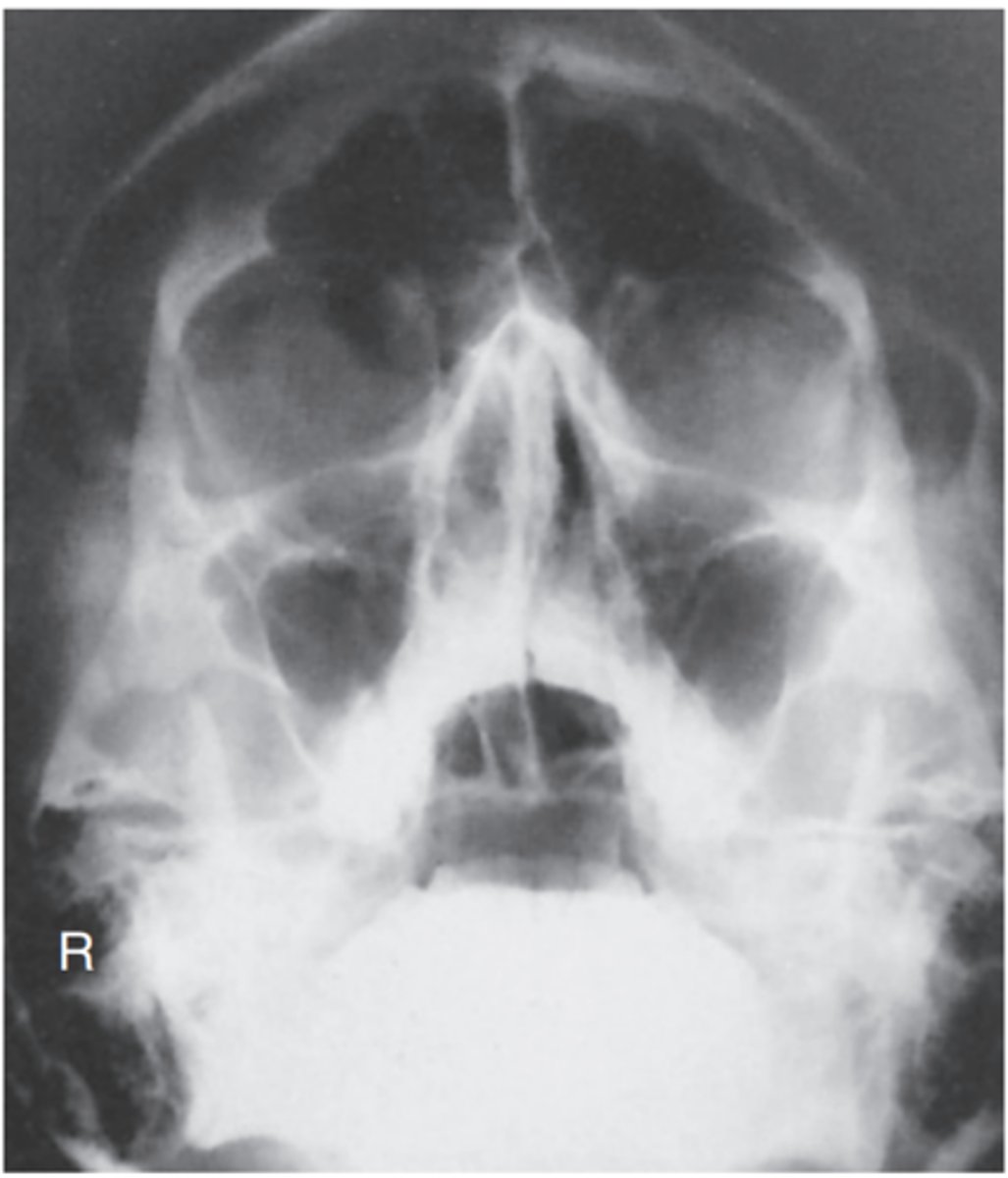
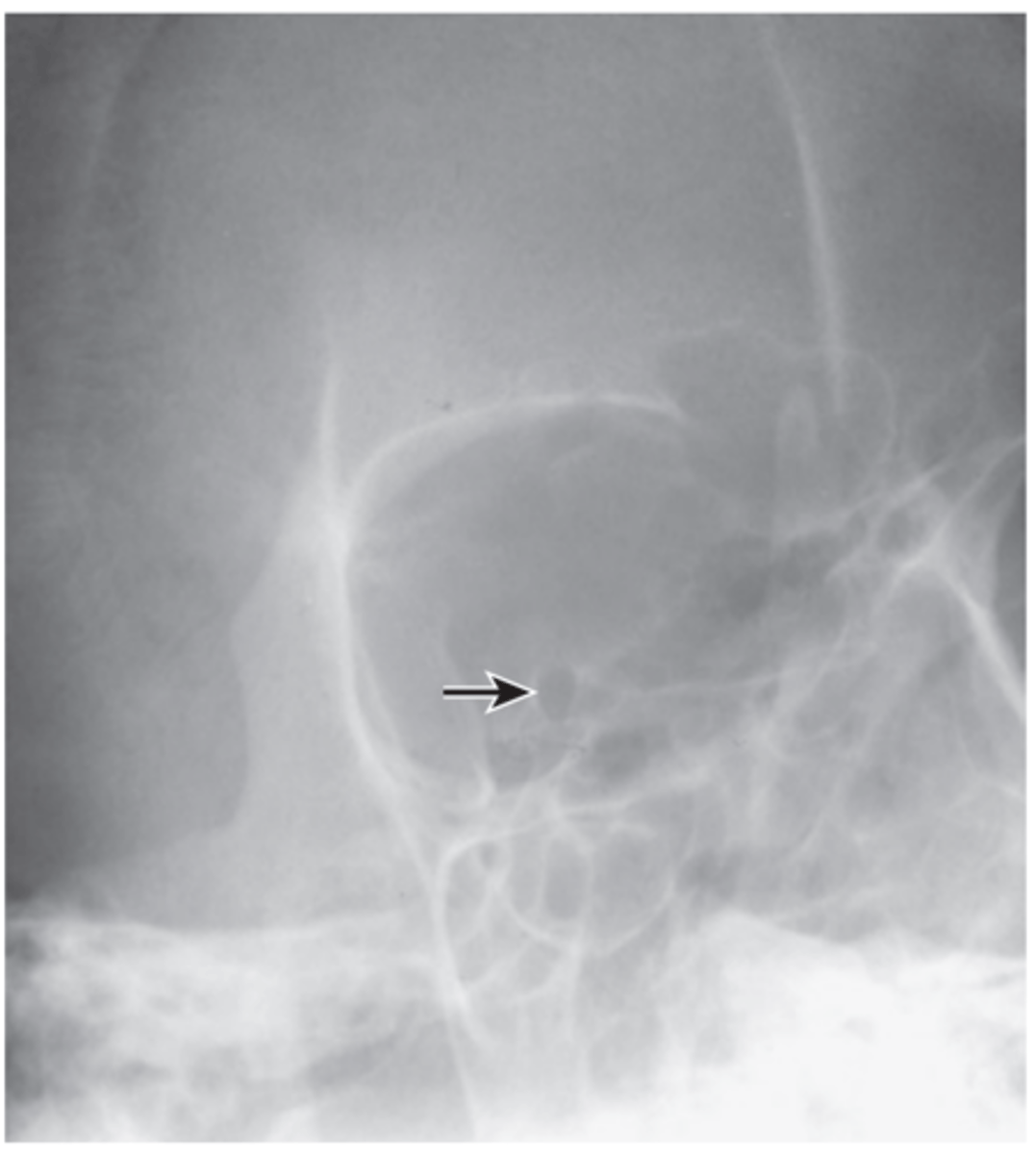
Critique parietoacanthial transoral projection (open-mouth Waters)
Repeatable errors (three)—
Criterion 1: Anatomy demonstrated: Sphenoid and maxillary sinuses are not well demonstrated. Petrous ridges are projected into lower aspect of maxillary sinuses.
Criterion 2: Positioning: Skull is underextended (chin not elevated sufficiently), leading to projection of petrous ridges into the lower aspect of maxillary sinuses. The base of the skull is superimposed over the sphenoid sinus.
Criterion 5: Anatomic side markers: No anatomic side marker is visible.
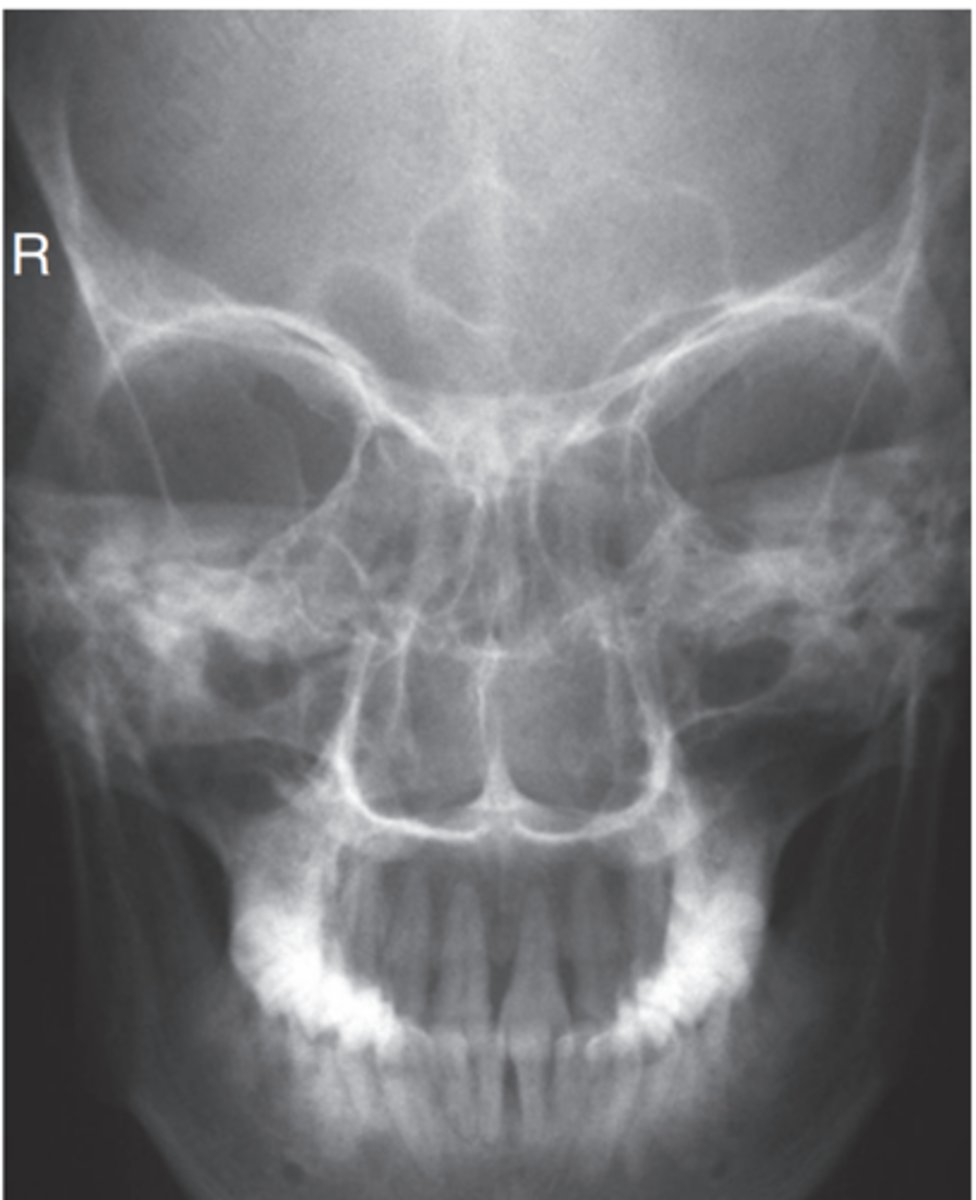
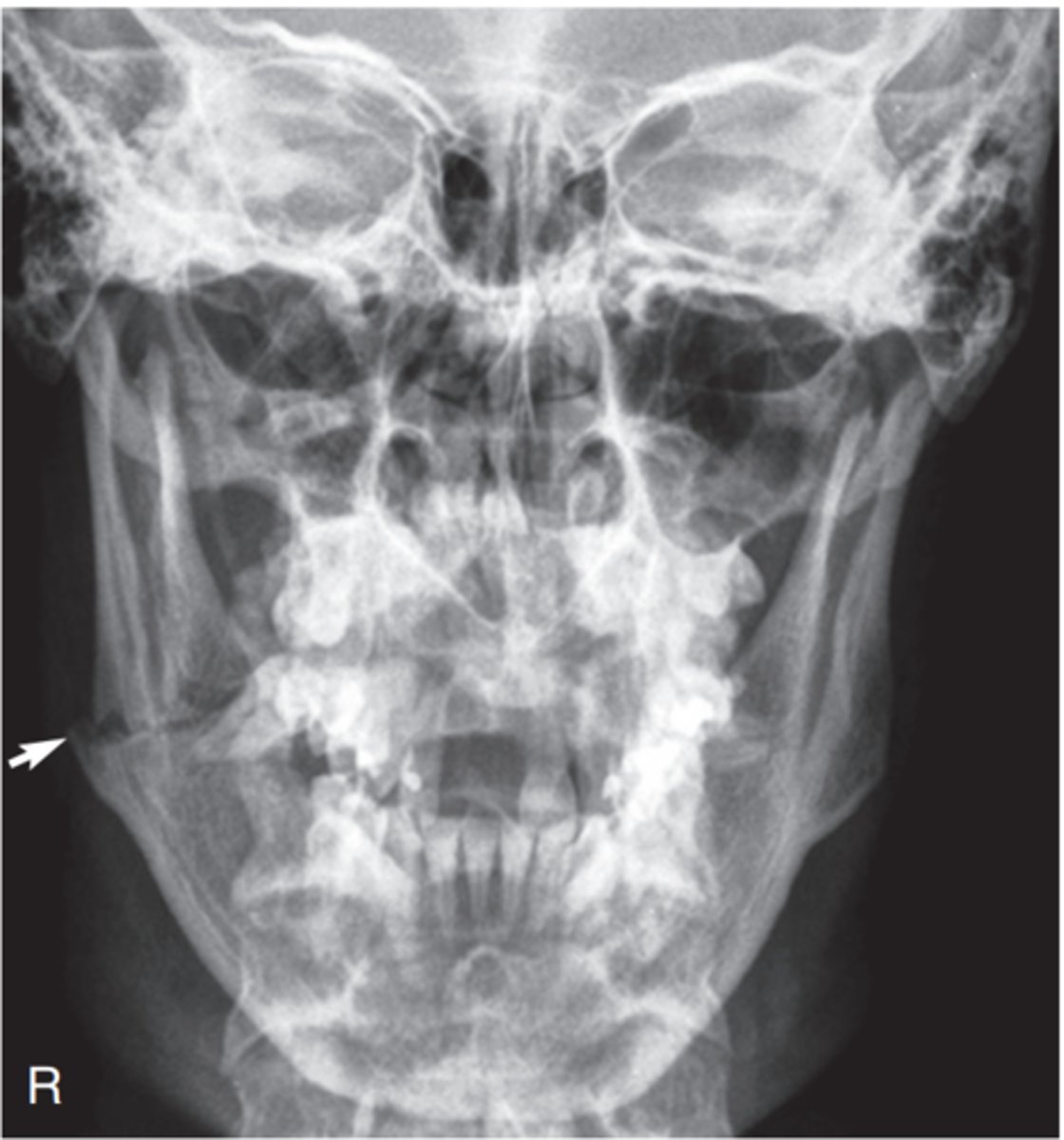
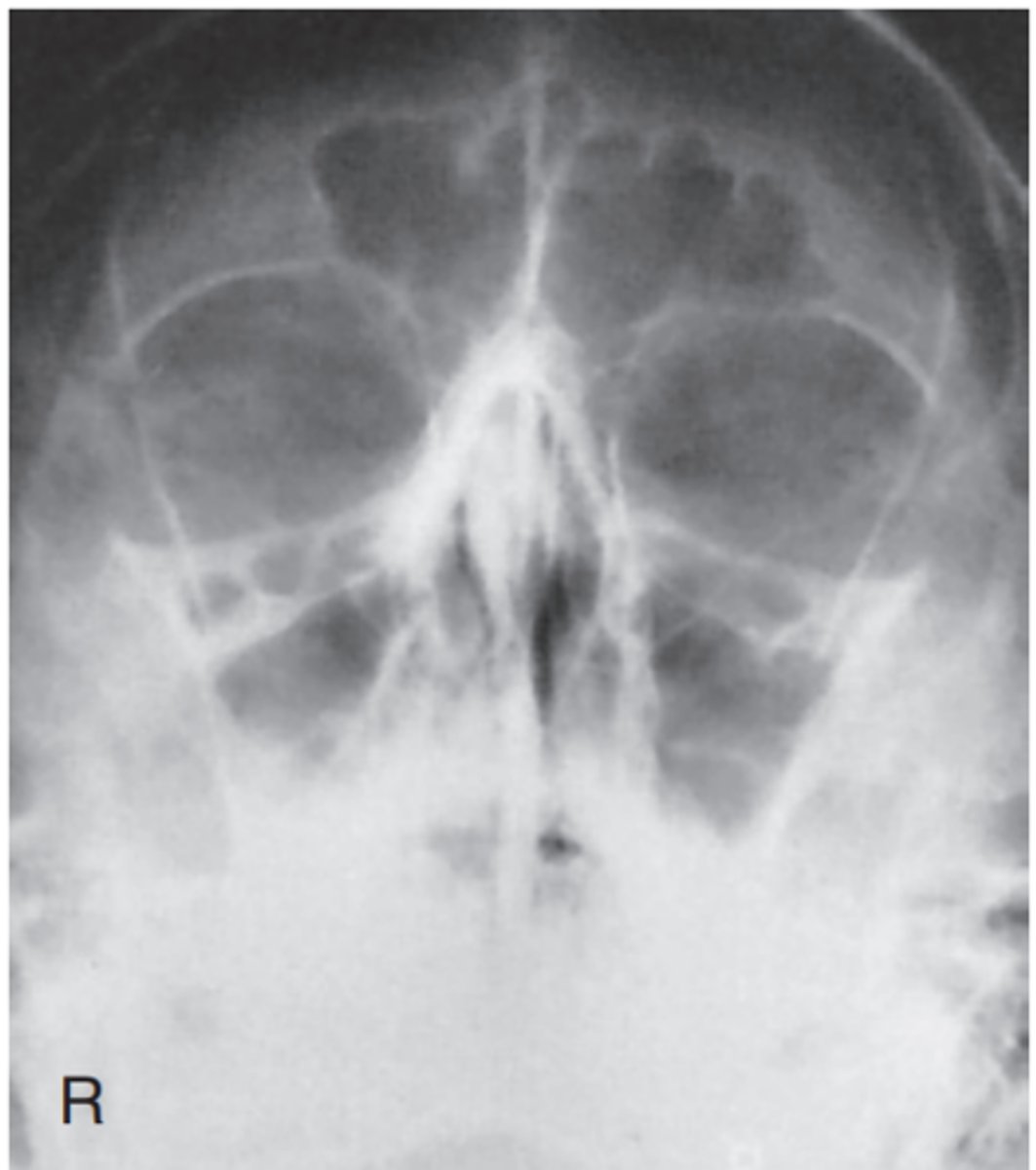
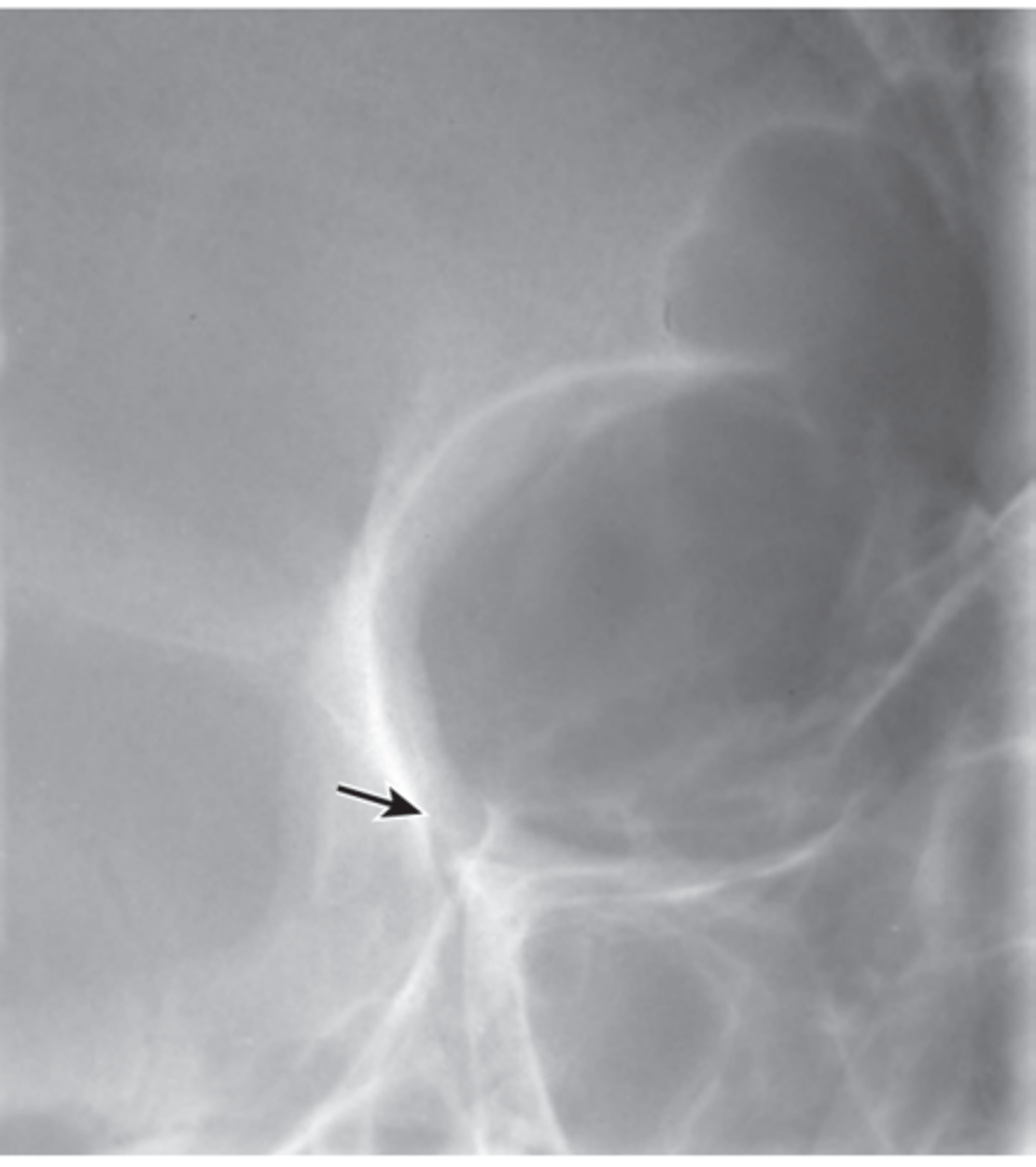
Critique parietoacanthial (Waters) projection.
Repeatable errors (three)—
Criterion 1: Anatomy demonstrated: Maxillary sinuses are not well demonstrated. Petrous ridges are projected into the lower aspect of maxillary sinuses. Artifacts appear to be both surgical clips and devices (acceptable) and external hair pins and clips (not acceptable).
Criterion 2: Positioning: The skull is underextended and severely rotated. This results in projection of petrous ridges into the lower aspect of the maxillary sinuses. Artifacts appear to be external hair pins or clips
Criterion 5: Anatomic side markers: No anatomic side marker is visible.

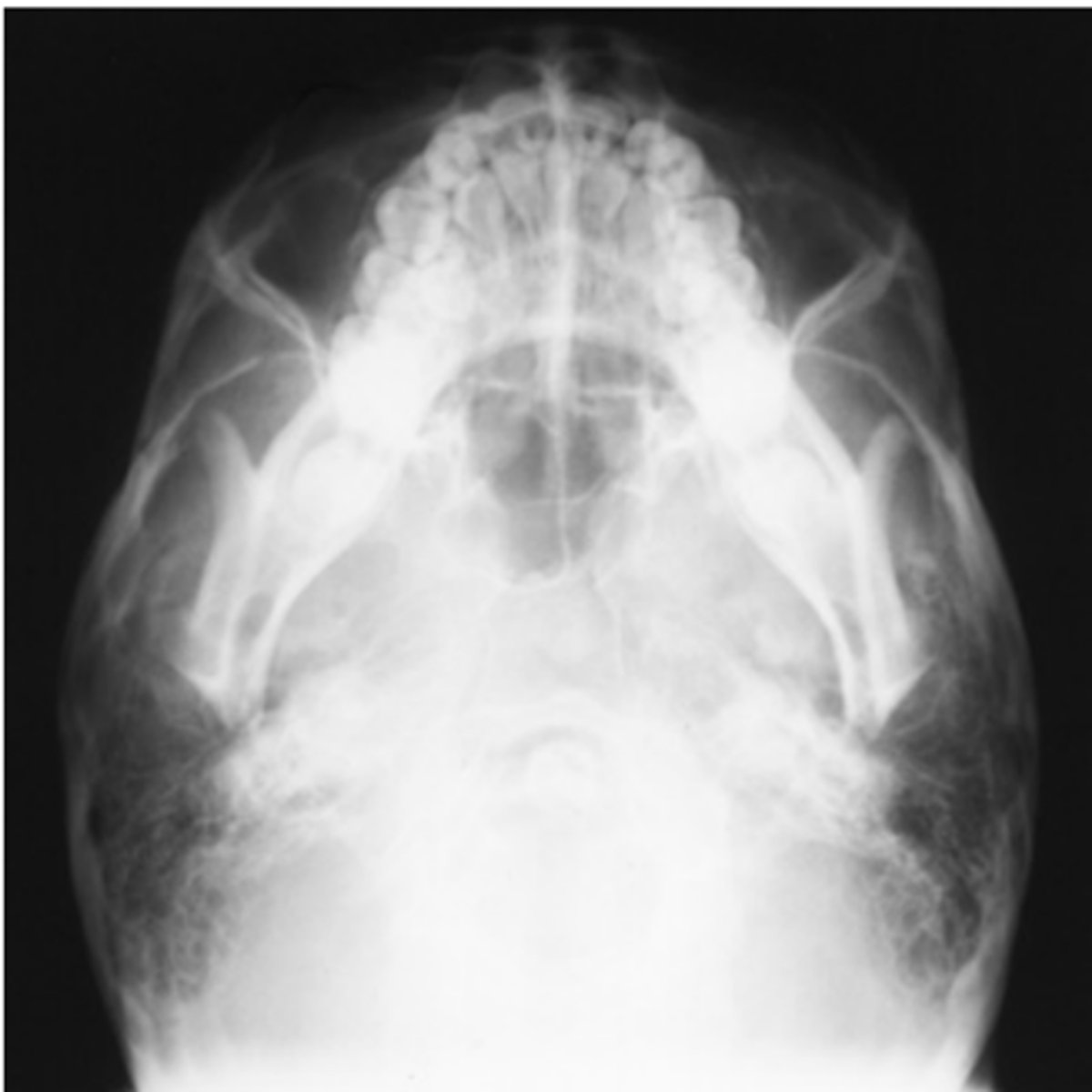
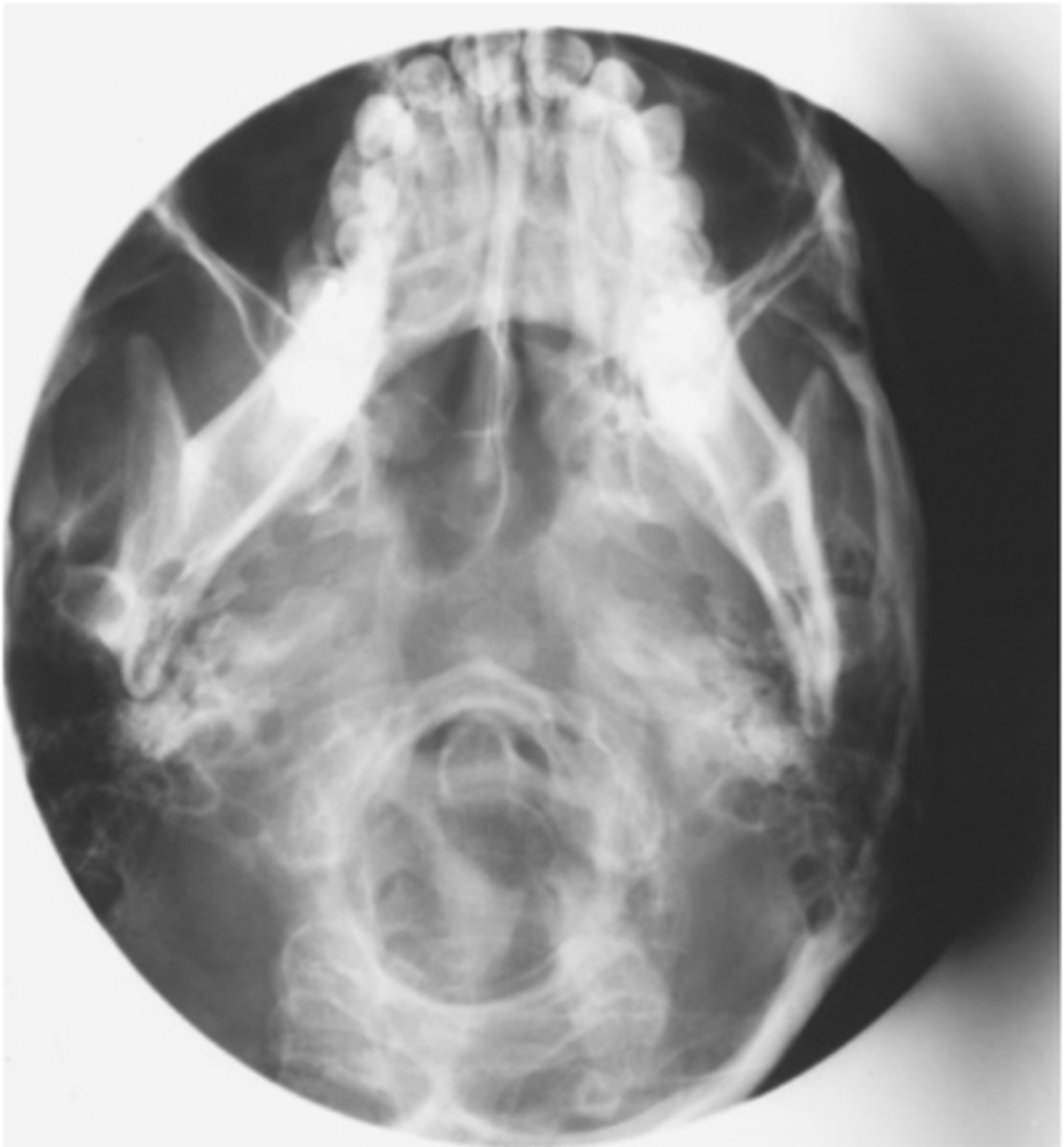
Critique SMV
Repeatable errors (four)—
Criterion 1: Anatomy demonstrated: Maxillary and ethmoid sinuses are not well demonstrated because of superimposition of mandible.
Criterion 2: Positioning: The skull is grossly underextended and tilted (also slight rotation).
Criterion 3: Collimation and CR: Collimation would have been adequate if centering had been correct. CR centering is off laterally, leading to cutting off of the anatomy. Mandible is superimposed over sinuses.
Criterion 5: Anatomic side markers: No anatomic side marker is visible.
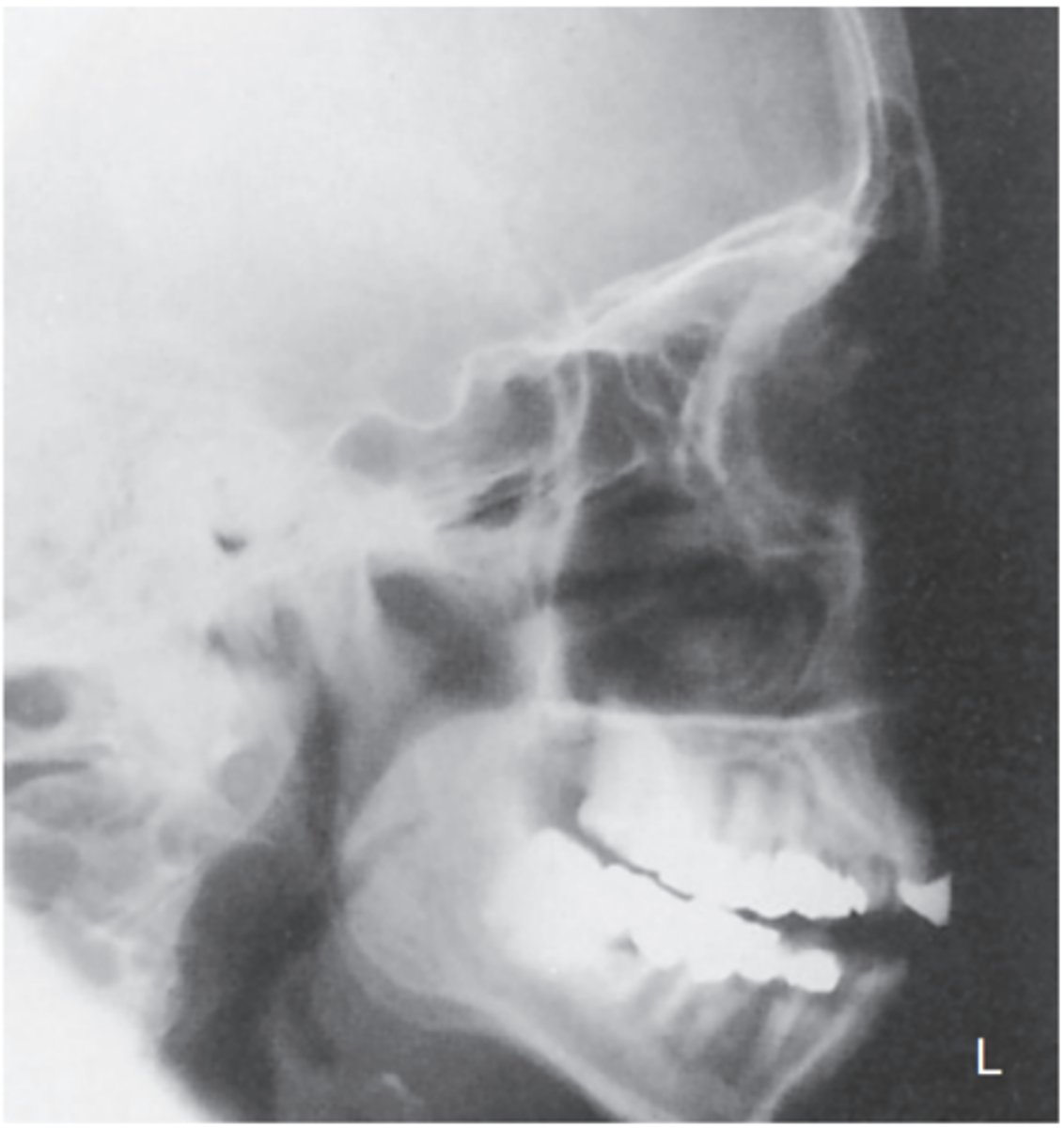
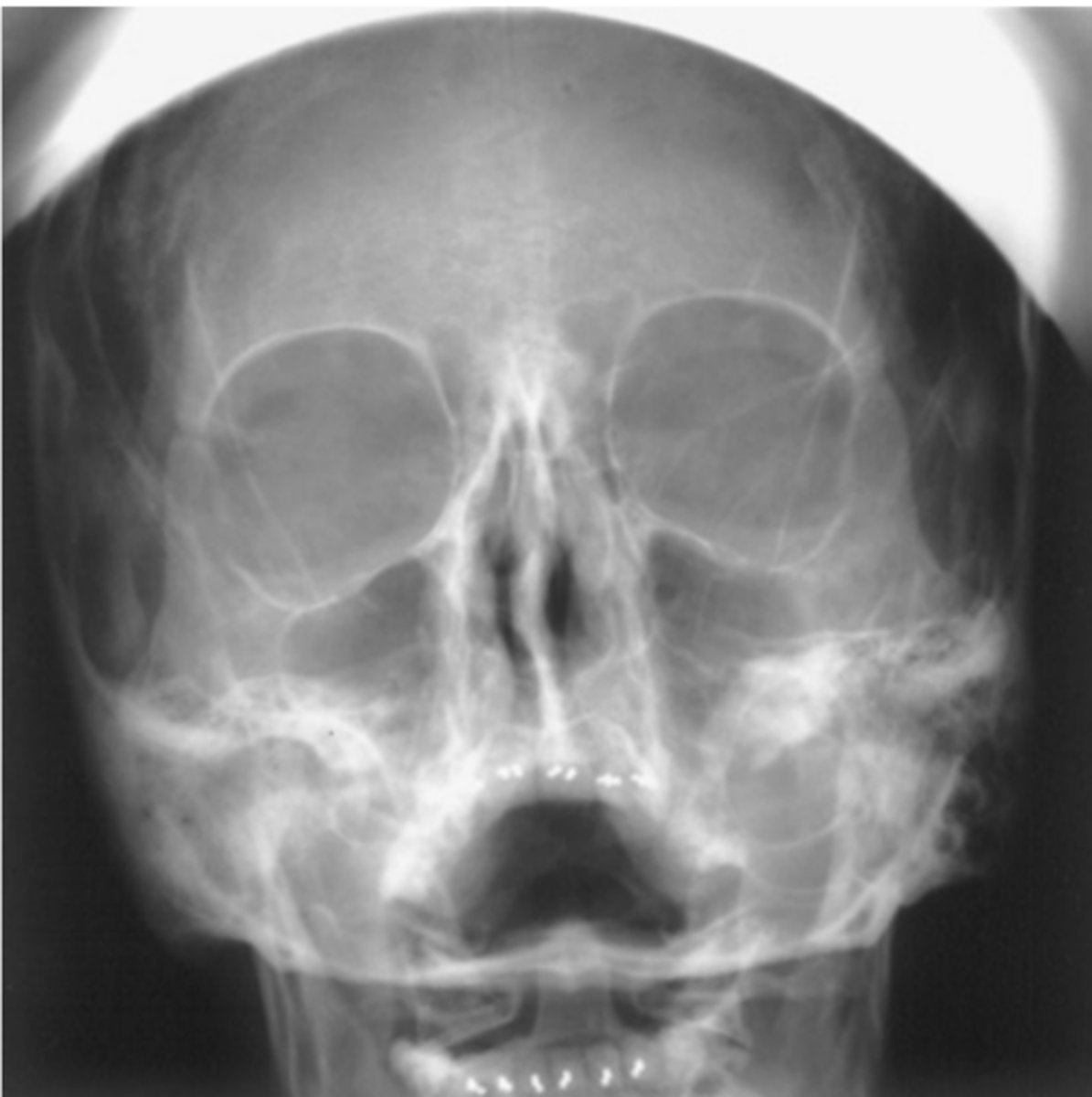
Critique Sinuses Lateral Projection
Repeatable errors (three)—
Criterion 1: Anatomy demonstrated: Aspects of the ethmoid and maxillary sinuses are not well demonstrated because of rotation of the skull.
Criterion 2: Positioning: Tilt of the skull is evidenced by lack of superimposition of orbital plates of the frontal bone. Note: Rotation of skull is evidenced by lack of superimposition of greater wings of sphenoid bones. CR centering is slightly anterior.
Criterion 5: Anatomic side markers: No anatomic side marker is visible.
