GI and Urinary Tract
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
63 Terms
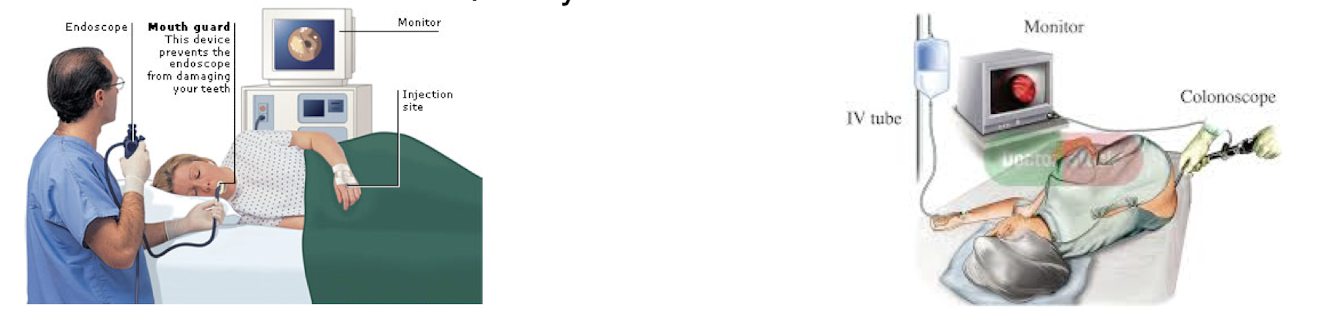
What technical advancements have been made that allows for improved imaging of the GI tract?
The development and perfection of endoscopy
What are the benefits and risks of endoscopy?
Risks: sedation and perforation
Benefits Endoscopy is becoming preferential
direct referrals to GI
safer
biopsy capability
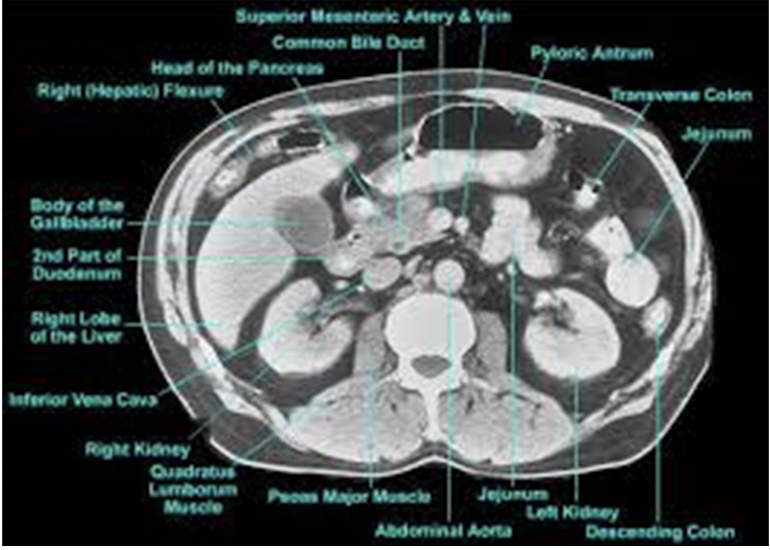
Identify the parts of the GI tract with CT imaging
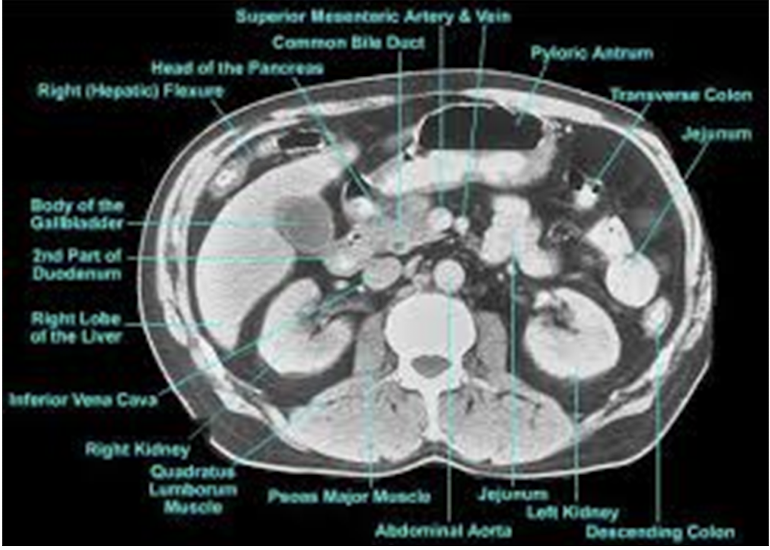

What is occurring in the CT scan?
Acute cholecystitis - enlarged gallbladder
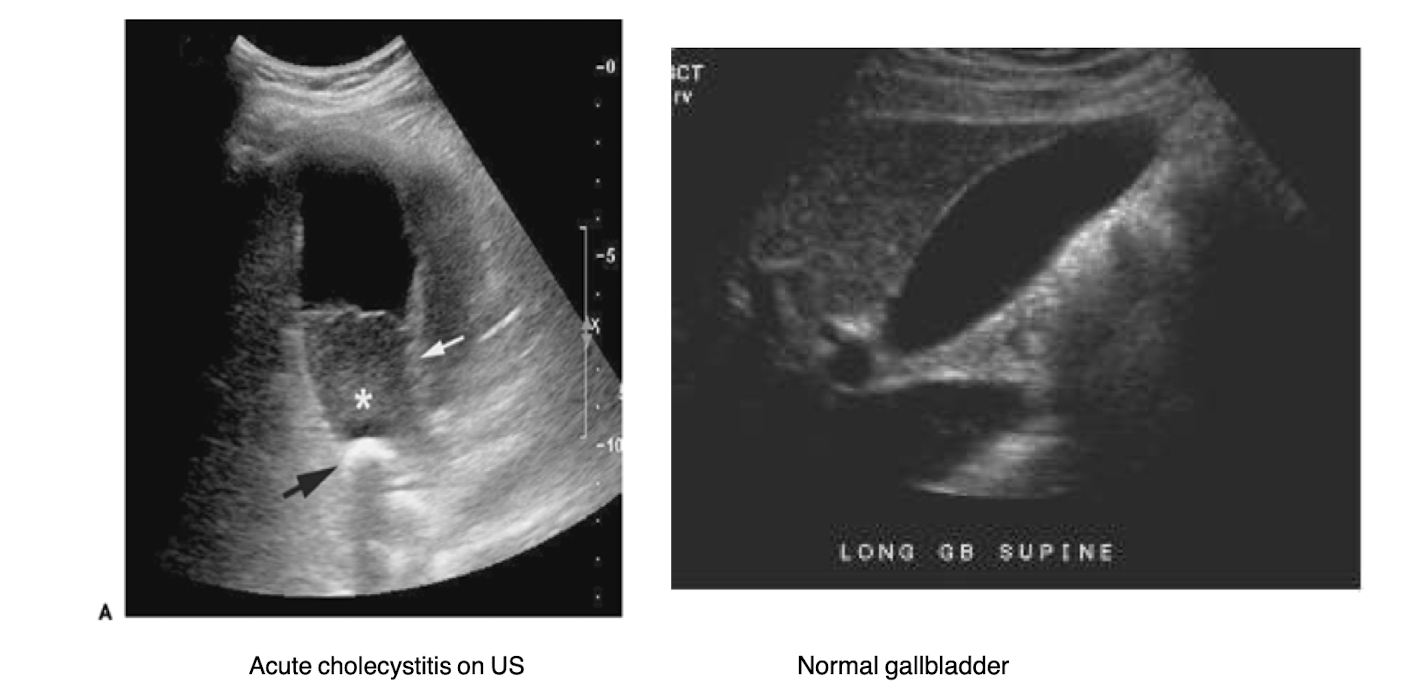
What is the investigative method of choice for evaluating the biliary system?
ultrasound
What do the MRCP and ERCP evaluate? What is the difference between them?
MRCP - magnetic resonance cholangiopancretography
more invasive
ERCP - endoscopic retrograde cholangiopancreatography
Both are used to evalute the biliary tree and pancreatic lesions
When is bowel prep used? When should it not be used?
Bowel prep is used before diagnostic procedures like colonoscopy to clear the intestines.
It should not be used in patients with bowel obstruction or severe inflammatory bowel disease. Not needed for toxic megacolon (extremely dialted colon, acute ulceralitve colitis or for obstruction)
When is abdominal CT preferred?
It is more definitive than U/S and gives more info about internal organs and structures, especially in cases of trauma or complex abdominal pain.
It will indicate inflammatory bowel disease, bowel obstruction, abscesses and fistulas
When is angiography used?
diagnose and therapy for GI bleed
How are nuclear studies used to study the GI tract?
help with hepatobiliary studies and GI bleeding localization
when U/S is inconclusive
more sensitive than angiography
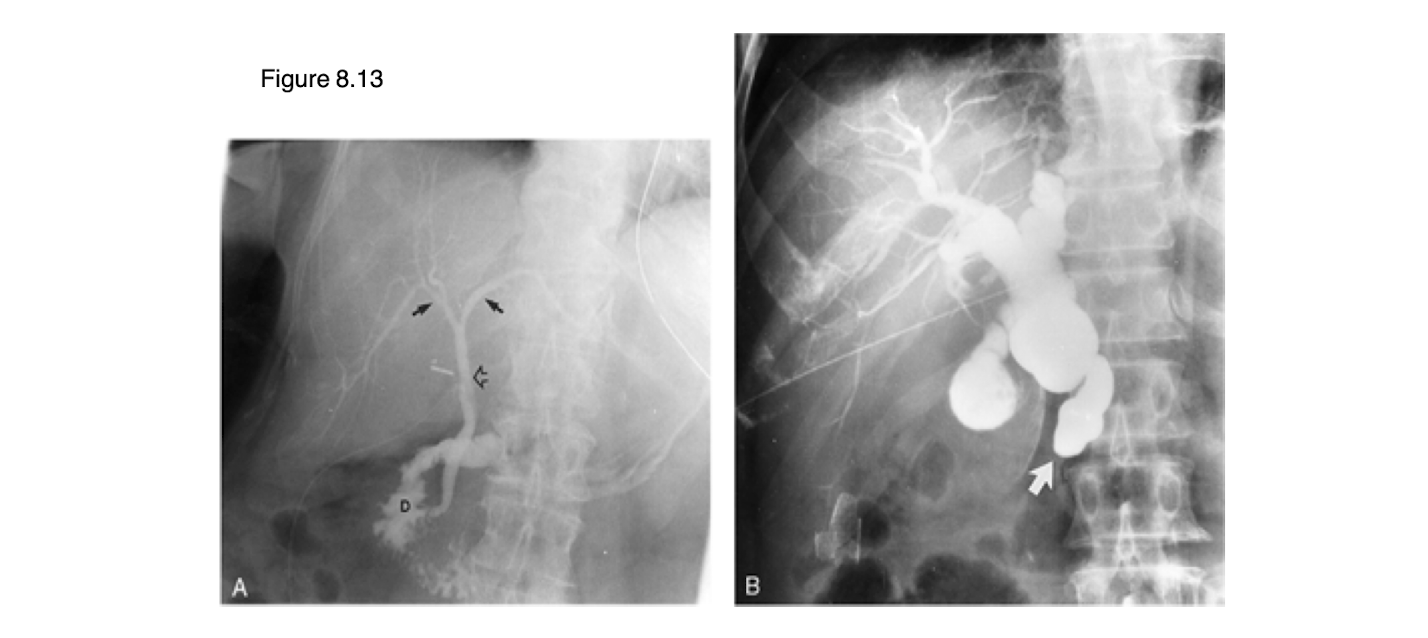
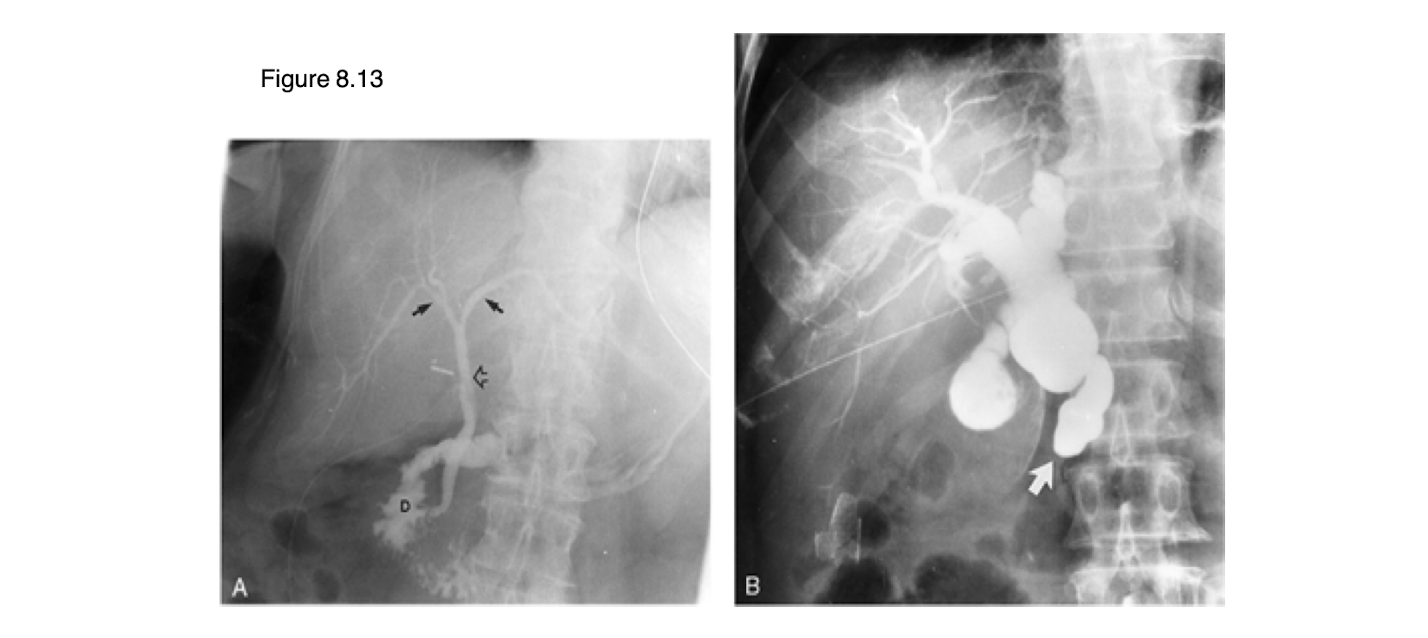
The left image is normal. What is occurring in the right image?
dilated common bile duct
What role does MRI play in GI imaging?
used to evaluate hepatobiliary system and metastases
What is the normal anatomic appearance of the stomach, duodenum, jejunum, and colon?
Pathology: sessile or pedunculated is _____
polypoid lesion
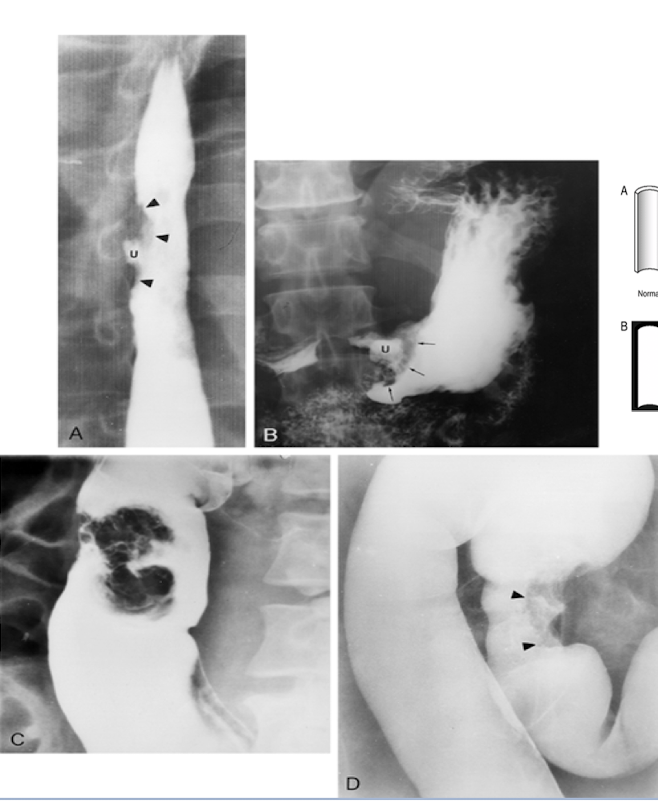
Pathology: tends to look like an “apple core” or “napkin ring”
mucosal mass
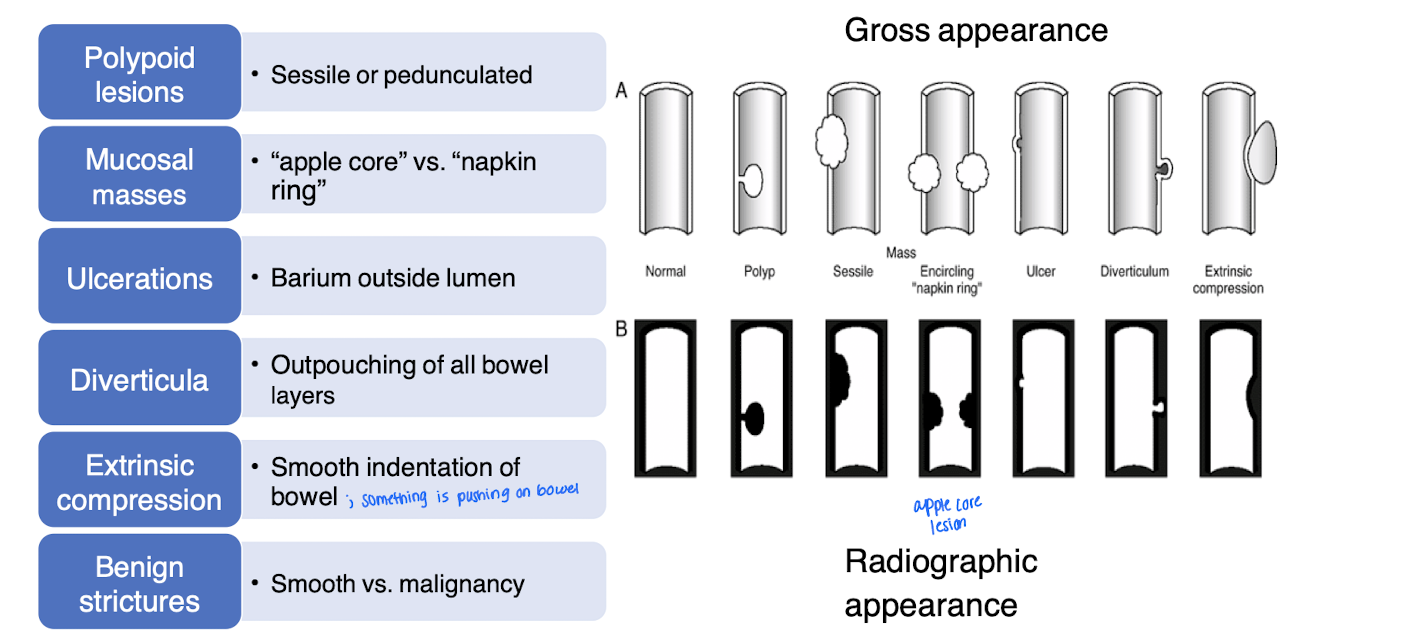
Pathology: on imaging, barium will leak outside the lumen because _____ erodes completely through the intestinal wall
ulcerations
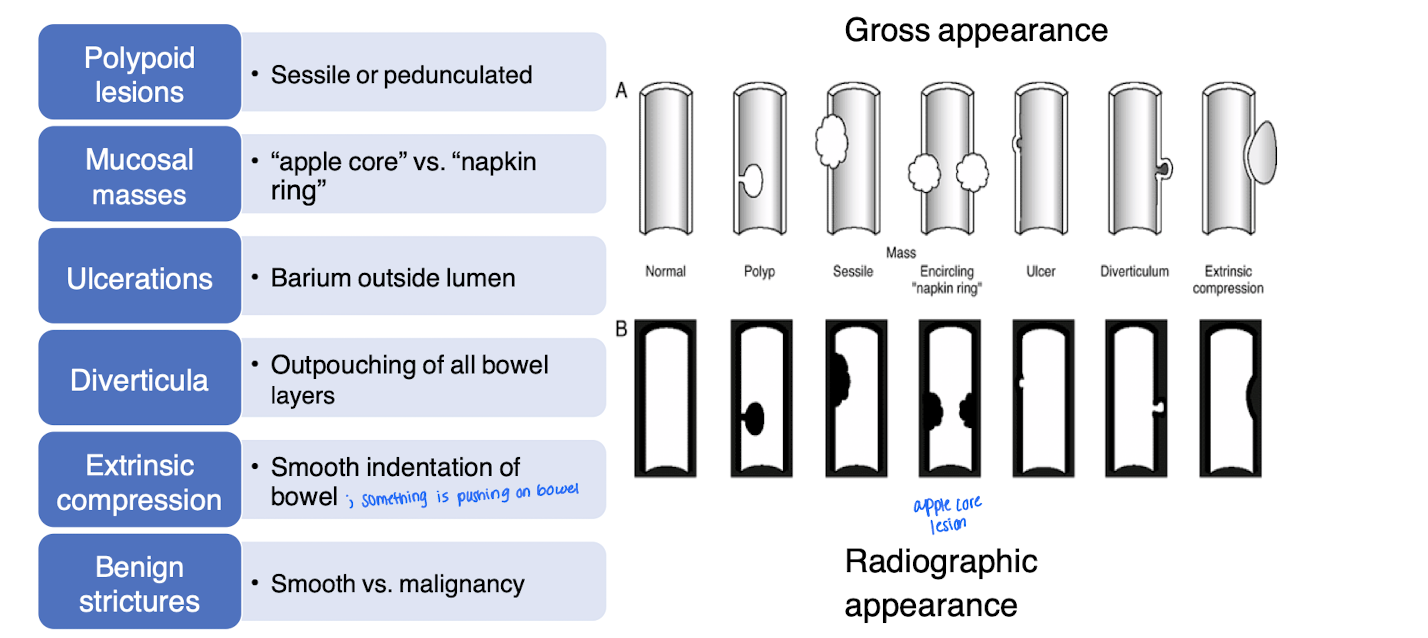
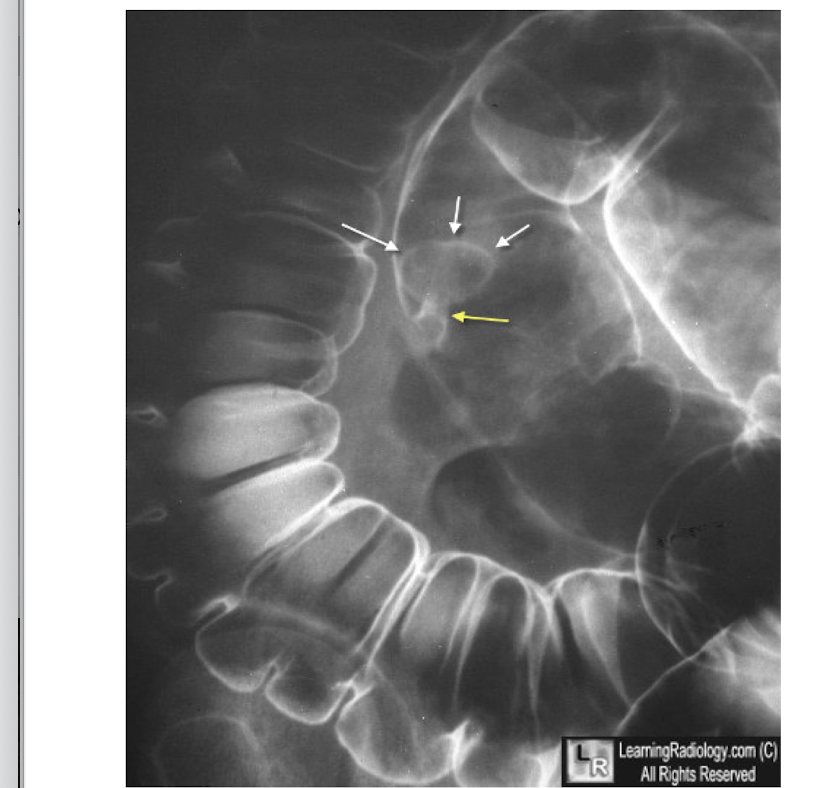
Pathology: outpouching of all bowel layers
diverticulum
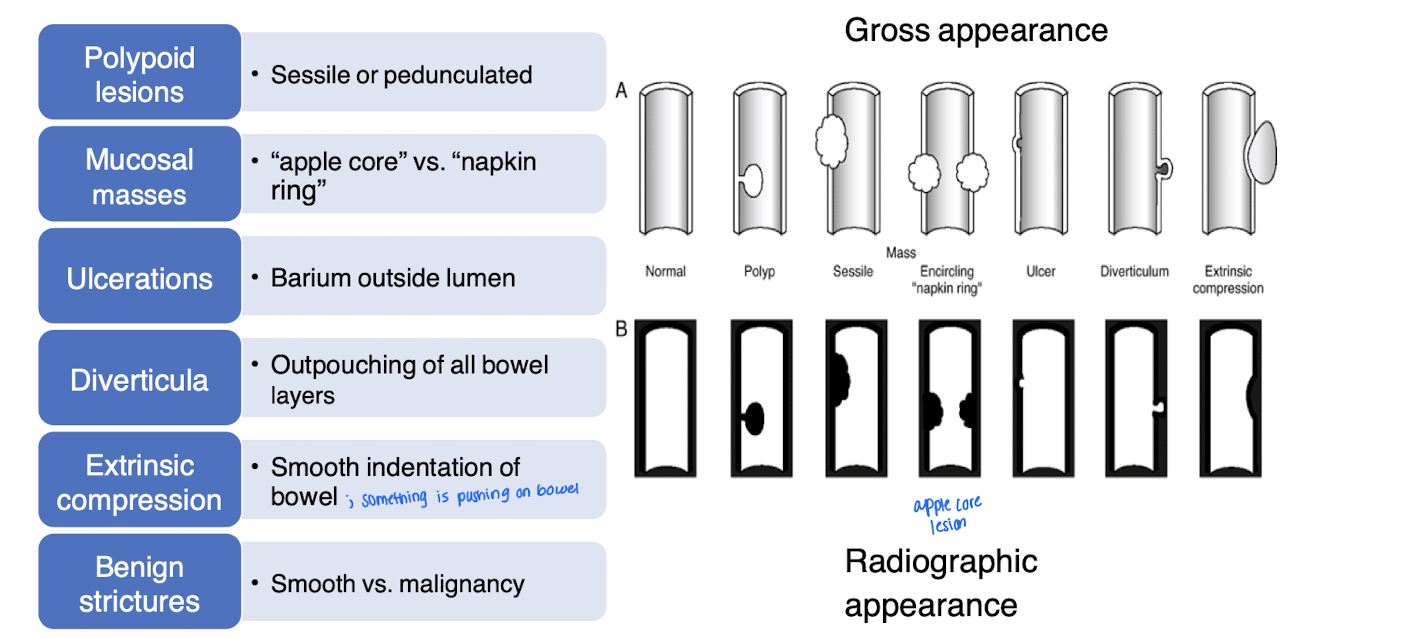
Pathology: smooth indentation of the bowel; looks like something is pushing the bowel
Extrinsic compression
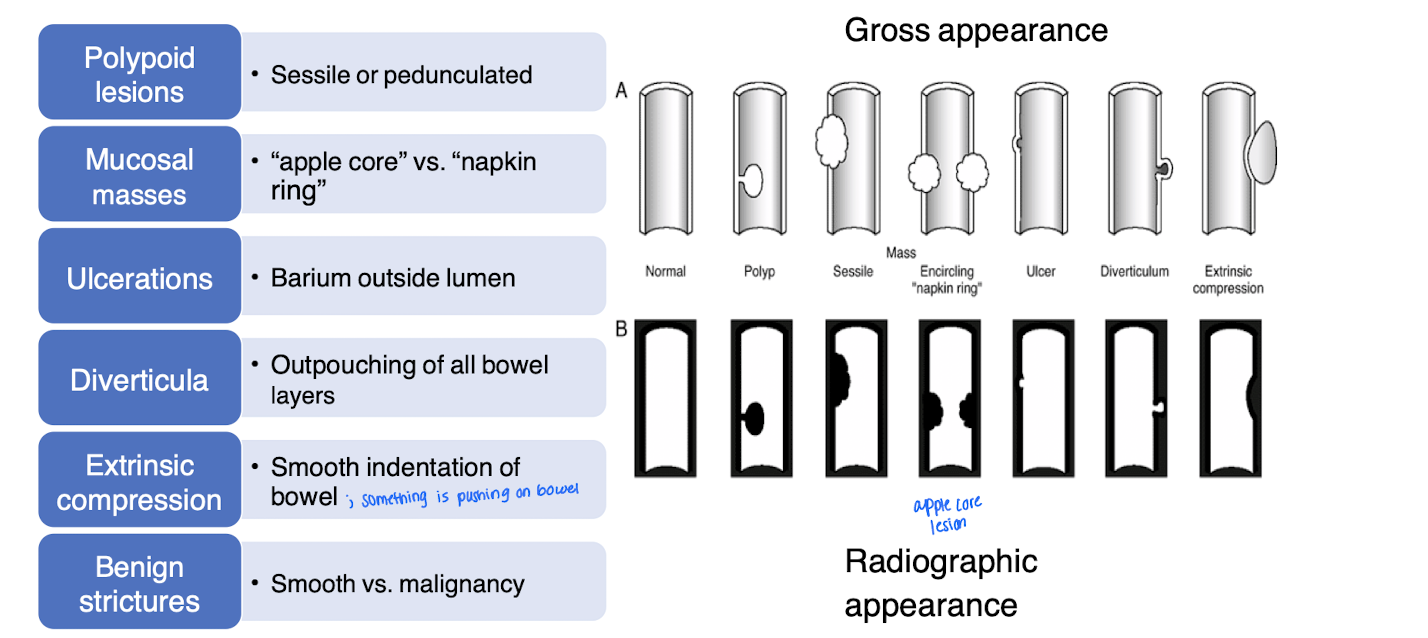
Pathology: described as smooth vs malignancy
a non-cancerous narrowing of a tube-like structure in the body, most commonly the esophagus, which can cause difficulties with swallowing. It is often caused by scar tissue from chronic inflammation, such as that from acid reflux (GERD), and other injuries.
Benign strictures
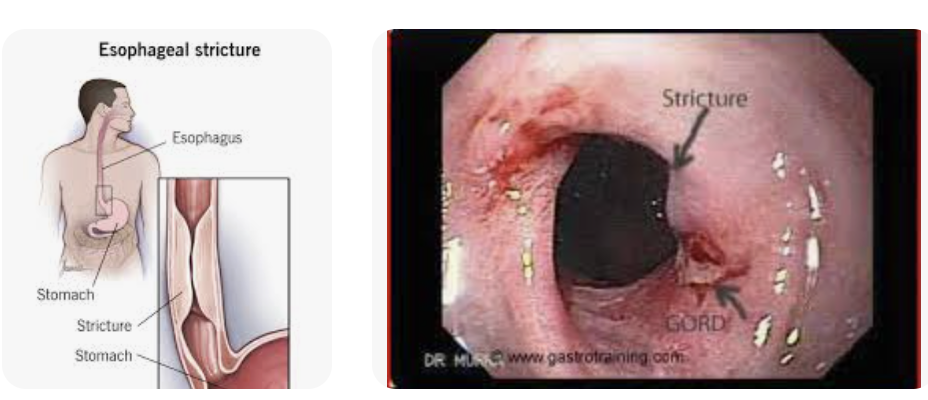
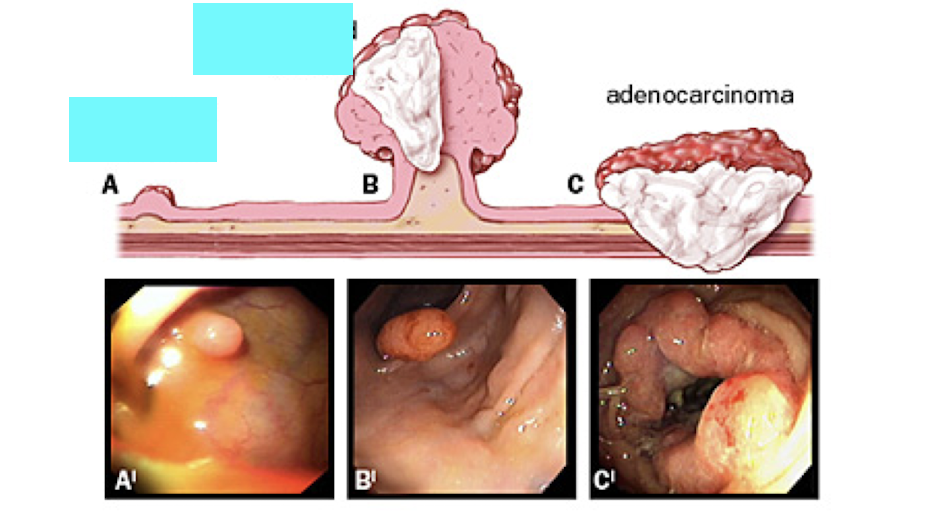
What is A?
sessile polyp - wide base
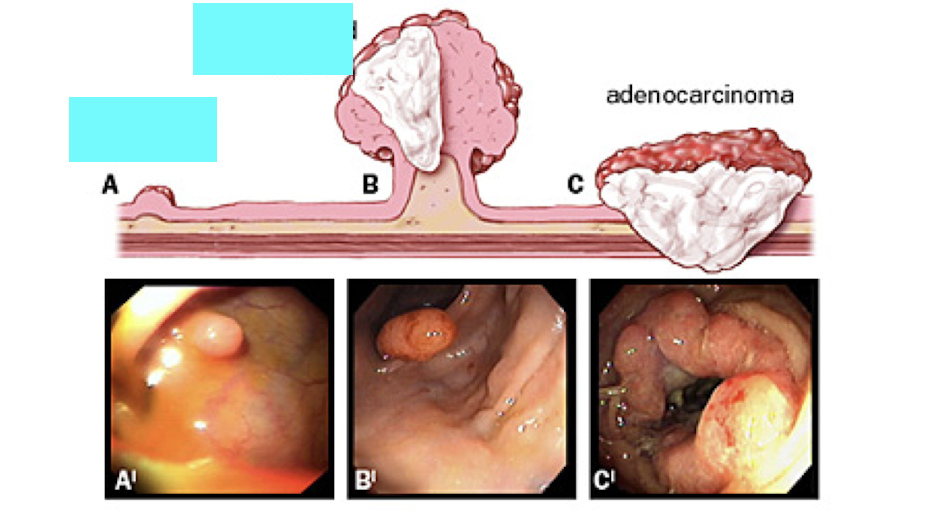
What is B?
Pedunculated polyp - on a stalk
What is observed on the double contrast study in the GI tract?
a. Mucosal mass
b. Diverticula
c. Pedunculated polyp
d. Sessile polyp
c. Pedunculated polyp - wide stalk

What is shown on the imaging?
a. Mucosal mass
b. Diverticula
c. Pedunculated polyp
d. Sessile polyp
a. Mucosal mass - apple core or napkin ring
What is D?
a. Mucosal mass
b. Diverticula
c. Pedunculated polyp
d. Sessile polyp
d. Sessile polyp
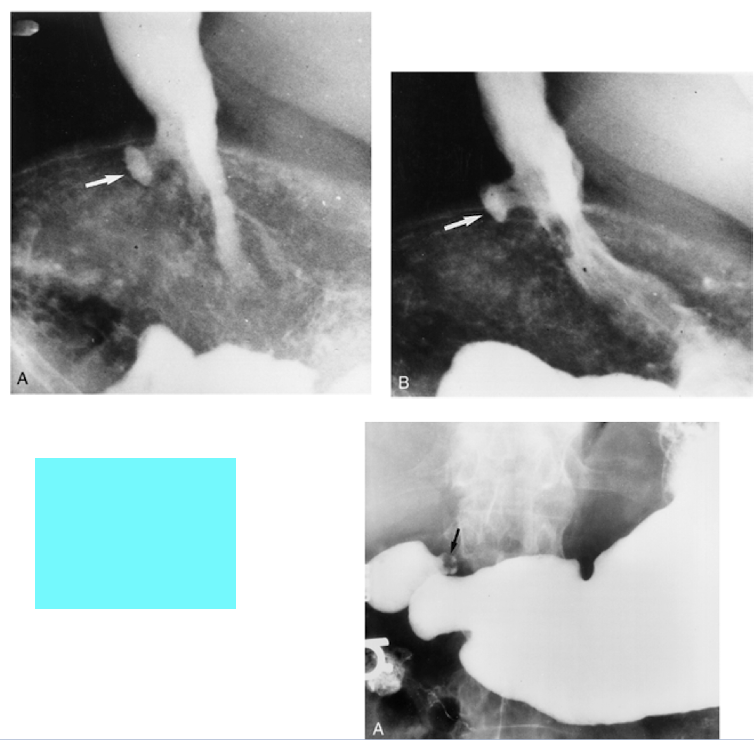
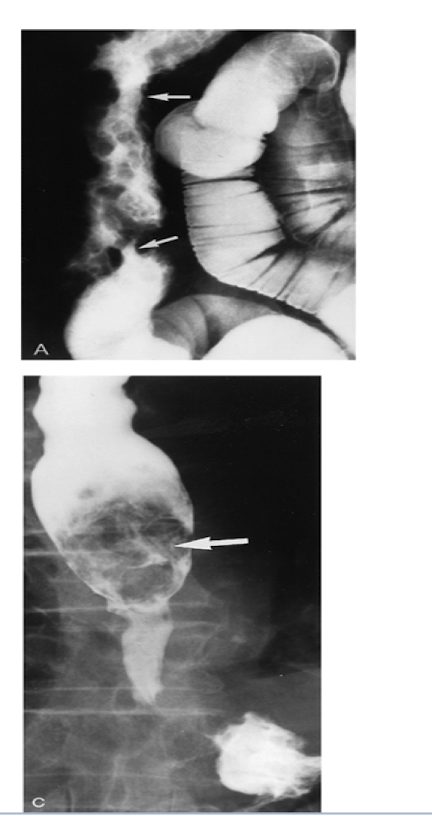
What are the images showing?
Duodenal ulcers
What is shown on the image?
Diverticulum
What are the images showing?
strictures
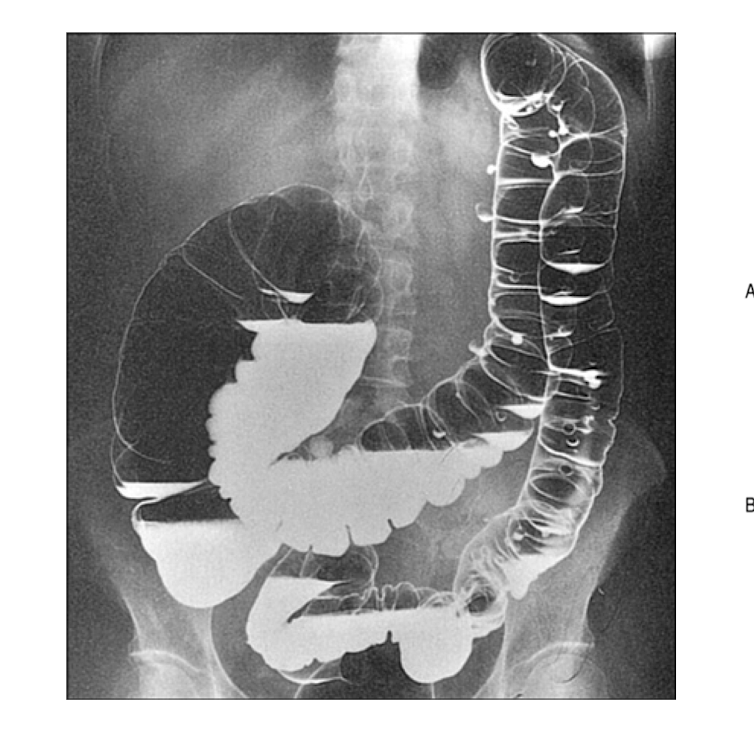
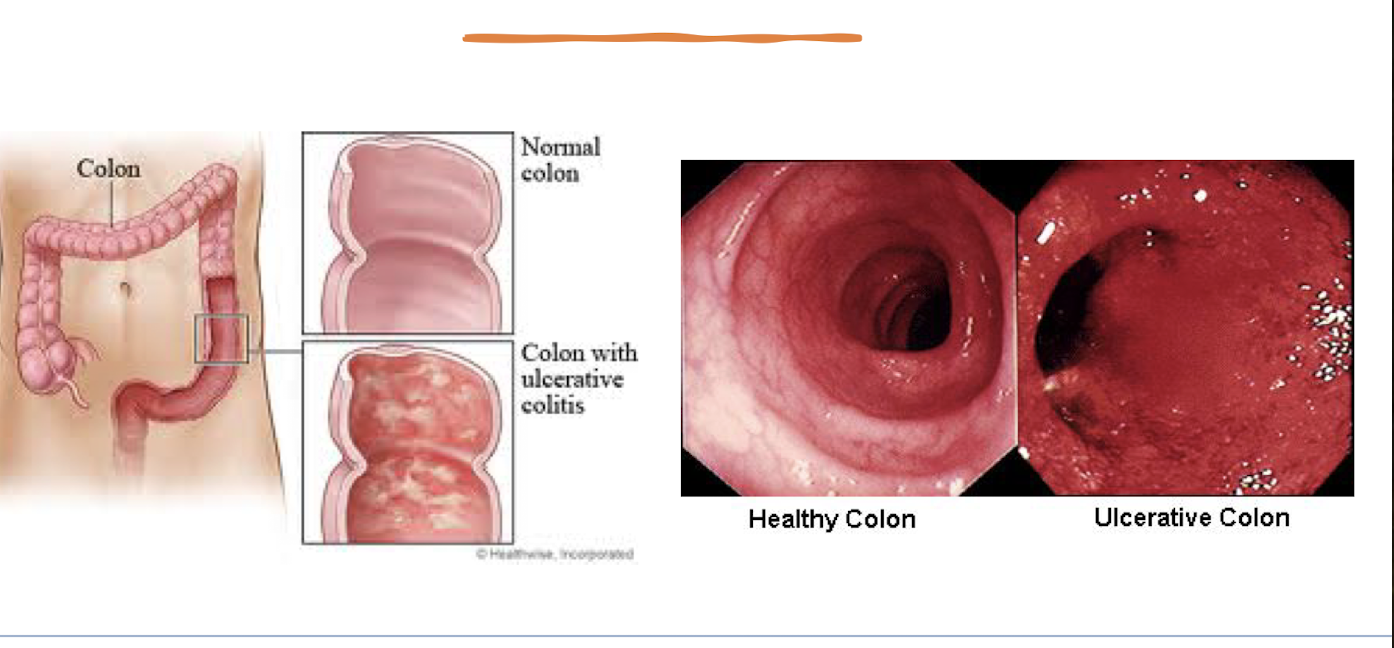
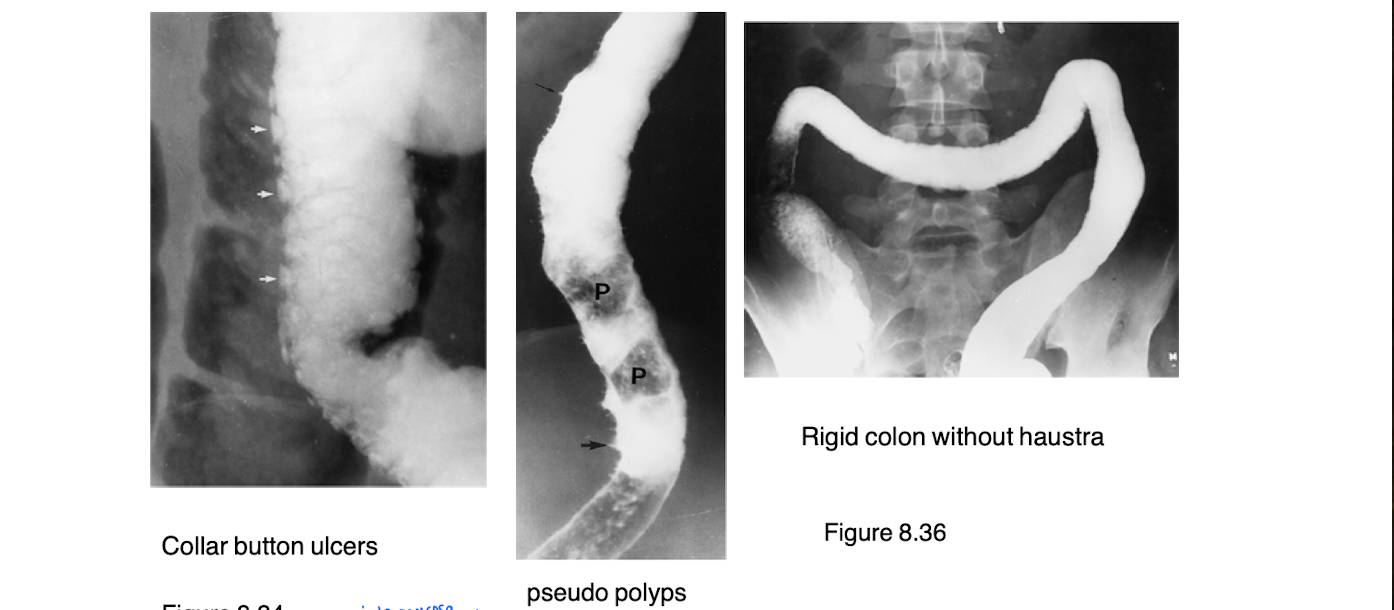
What is ulcerative colitis?
type of inflammatory bowel disease (progressive inflammatory movement)
bowel wall edema
shallow, coalescent ulcerations: pseudopolyps
prone to undergo malignant change
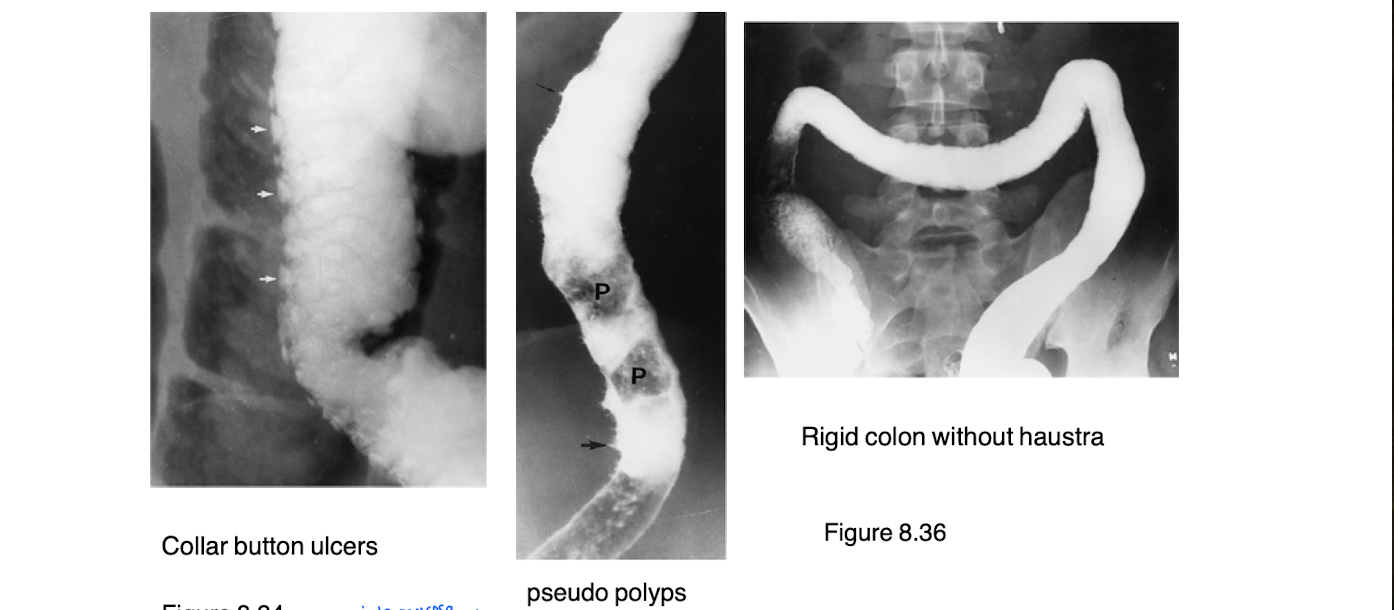
What is this diagnosis?
Ulcerative colitis
What are a hallmark to ulcerative colitis
No haustra
Collar button ulcers
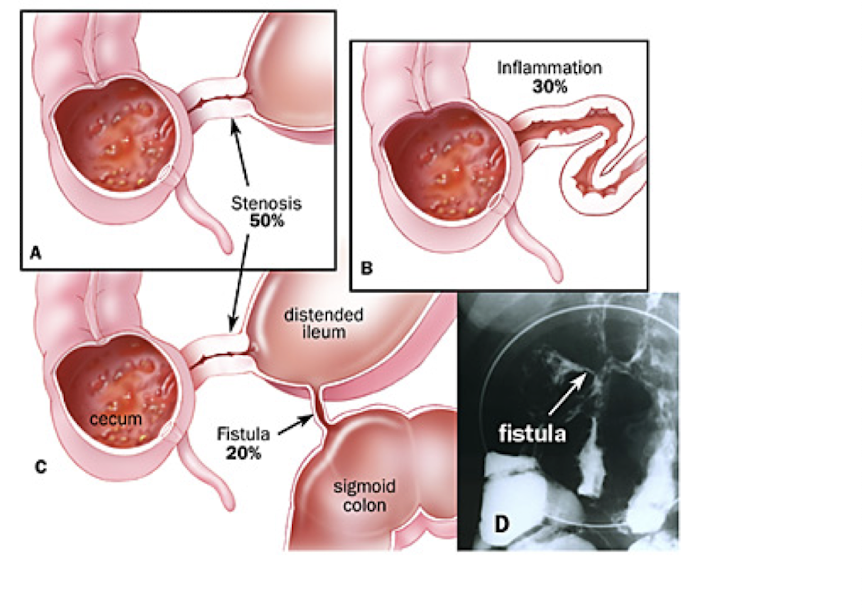
Describe Crohn’s Disease
type of inflammatory bowel disease
strictures, obstruction, and fistulas are seen
skin lesions
cobblestone created by skip lesions
increased risk of colon cancer
Which type of IBS has an increased risk of colon cancer?
Crohn's Disease

What can be seen in the image?
Cobblestoning for Crohn’s disease
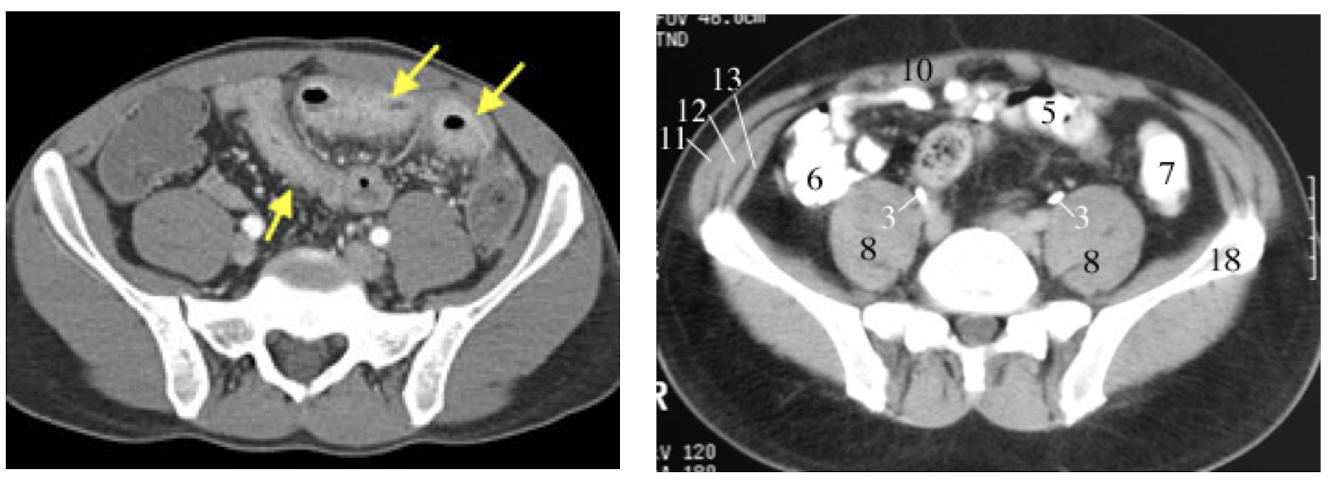
What is shown in the CT (left)?
small bowel inflammation
What are the more common GI tract abnormalities of the pediatric population?
Foreign body
Pyloric stenosis - common in boys and presents around 3 weeks of age with projectile vomiting because food is backing up
Hirschsprung disease
Intussusception
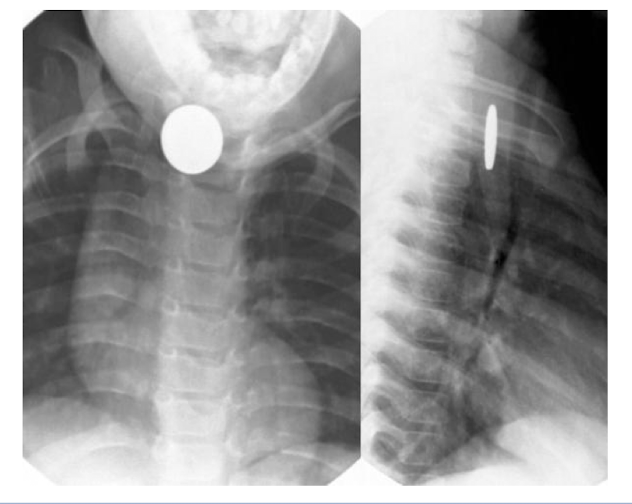
What is shown on the pediatric imaging?
Esophageal Foregin body
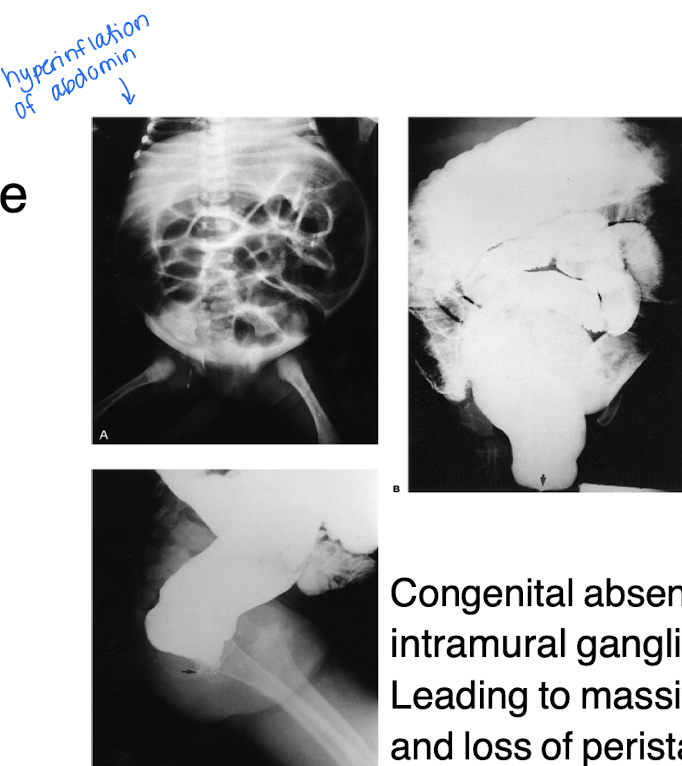
What is Hirschsprung disease?
A congenital absence of intramural ganglion leading to massive dilation, and loss of peristalsis
What is intussusception
A condition where a part of the intestine telescopes into an adjacent segment, causing obstruction and potential ischemia.
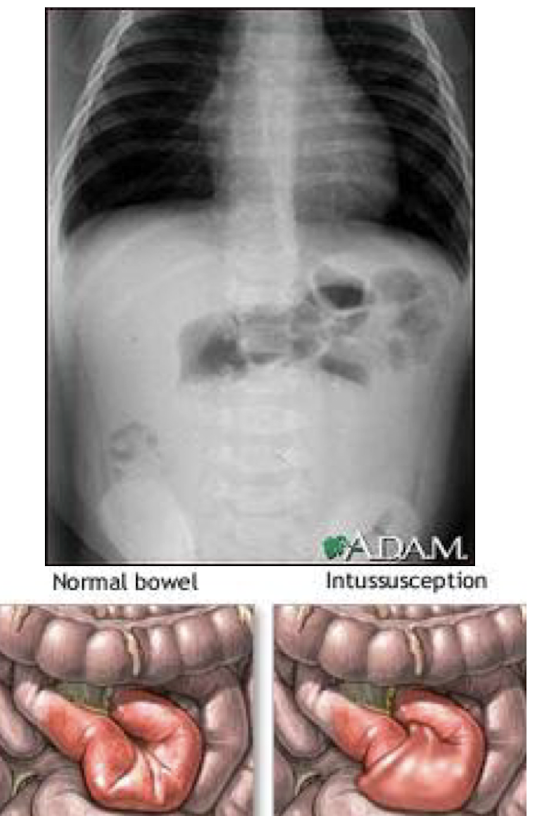
How is the diagnosis of intussusception confirmed and treated at the same time?
Diagnosis is typically confirmed through an abdominal ultrasound or CT scan, and treatment is performed via an air contrast enema or surgical intervention.
What are the studies used to evaluate the urinary tract, how are they performed and what are the indications of each?
Intravenous urogram (IVU) aka IVP uses contrast dye to visualize the urinary tract, assessing kidney function and identifying obstructions, stones, or abnormalities.
Retrograde examinations - contrast via small catheter
Cystogram/voiding cystourethrogram - imaging while voiding
Check for vesicoureteral reflex in kids
Nephrostogram uses contrast dye to visualize the kidneys and renal pelvis, often performed when urine flow is obstructed or to assess kidney anatomy.
U/S
CT
MRI
Isotope study
What is the initial study of the urinary tract imaging?
Ultrasound
eval kidney shape and size
determine if mass is solid vs cystic
transrectal for prostate
When is CT used in the urinary tract?
renal trauma
calculi
When is MRI used in the urinary tract?
masses
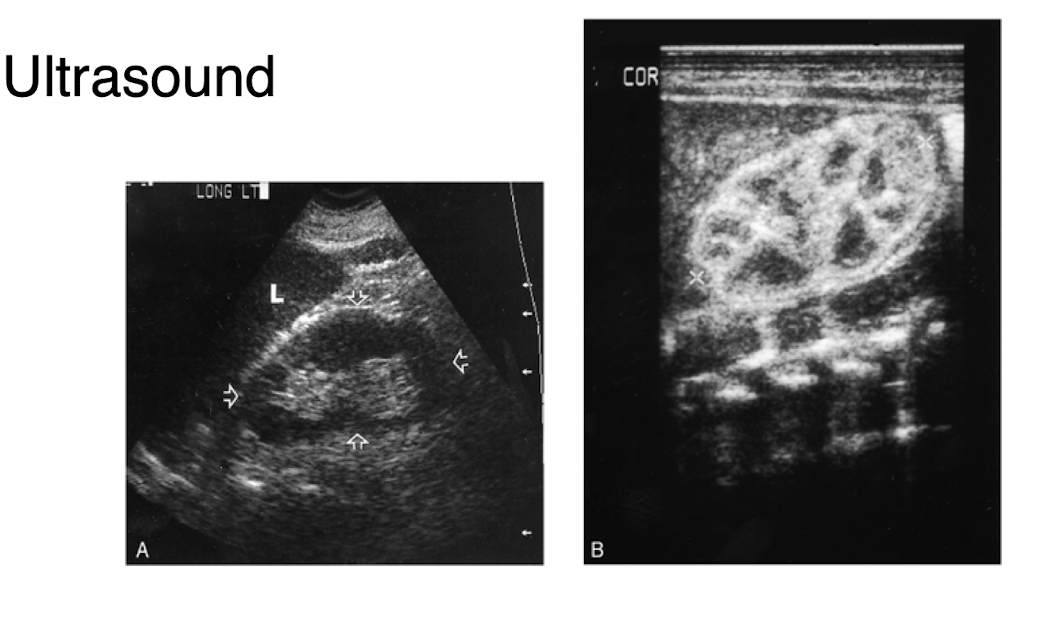
What is shown in this ultrasound of the urinary system?
normal renal ultrasound with the right image being the kidneys
Describe the appearance of "normal" collecting system, ureters, bladder, and prostate
The normal collecting system appears smooth and well-defined,
ureters displaying no obstruction or dilation
the bladder shows uniform thickness without wall irregularities
prostate gland is of normal size and echogenicity, free of lesions or abnormalities.
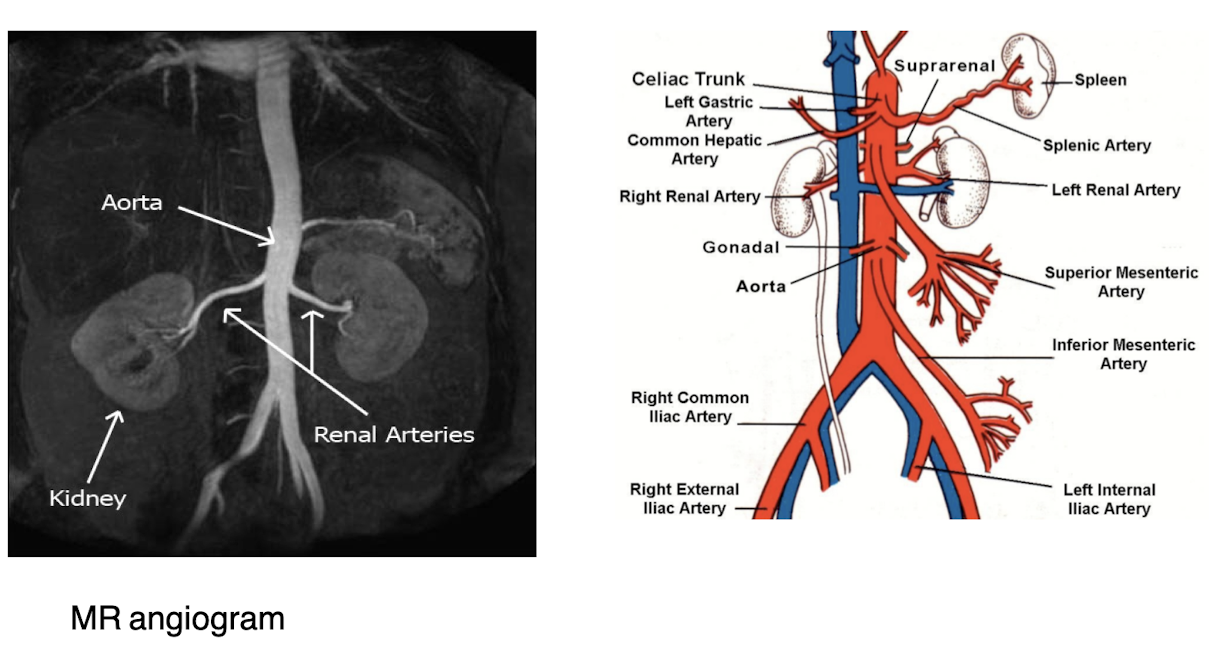
What is the "normal" vascularity of the kidneys?
The kidneys have a highly vascular structure, with renal arteries supplying blood and a rich network of capillaries, ensuring adequate perfusion for filtration and waste removal.
What is a duplication of the collecting system?
A congenital anomaly where there are two ureters and renal pelvises associated with a single kidney, leading to potential drainage issues.

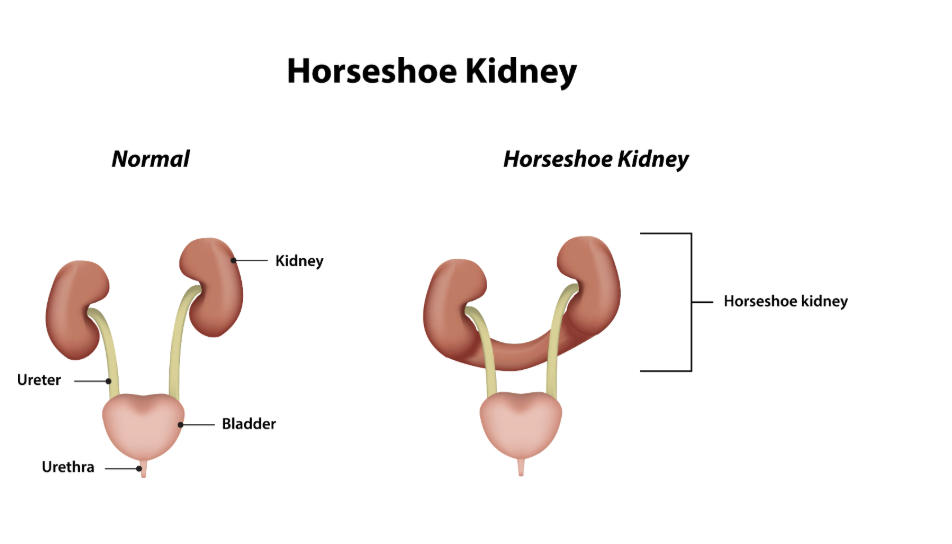
What is a horseshoe kidney?
A congenital abnormalitiy where the two kidneys are fused together at their lower ends, forming a "U" shape, which can affect their function and position.
What are posterior urethral valves and how are they diagnosed?
Most common cause of urethral obstruction in male children. They are abnormal folds of tissue in the urethra that obstruct urine flow, diagnosed through ultrasonography or cystoscopy.
What is ureterocele?
congenital abnormality with a dilated distal end of ureter
What is renal ectopia?
Congenital condition where the kidneys are not in the appropriate spots
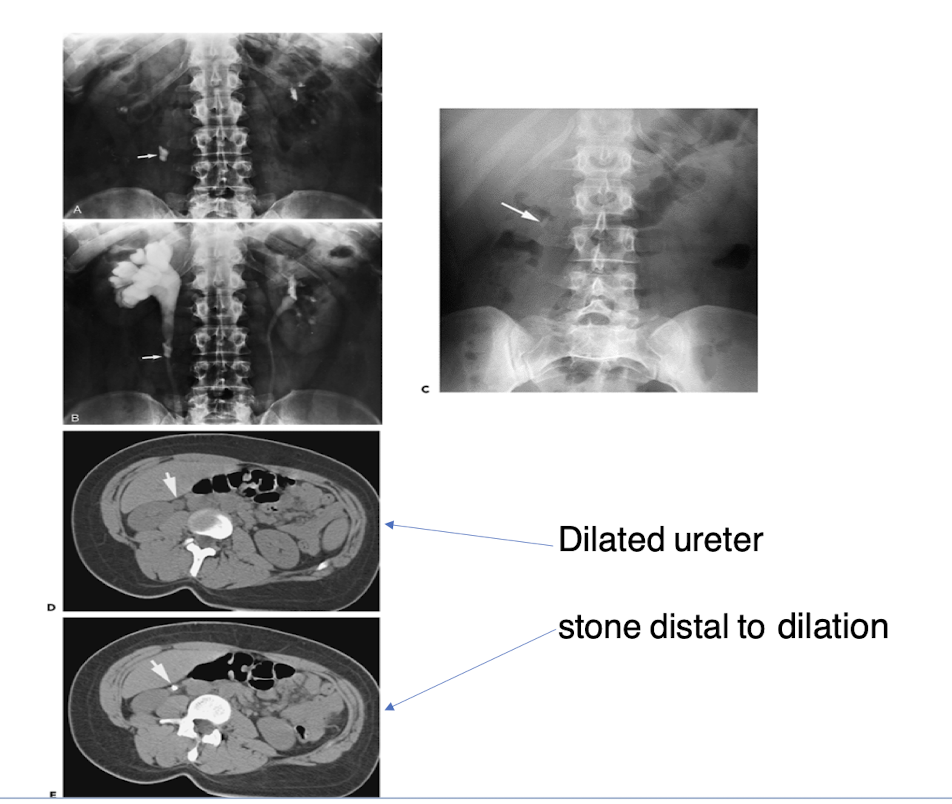
What are common causes of urinary obstruction?
Congenital or acquired
Stones - common cause of acquired obstruction
tumor
operative manipulation
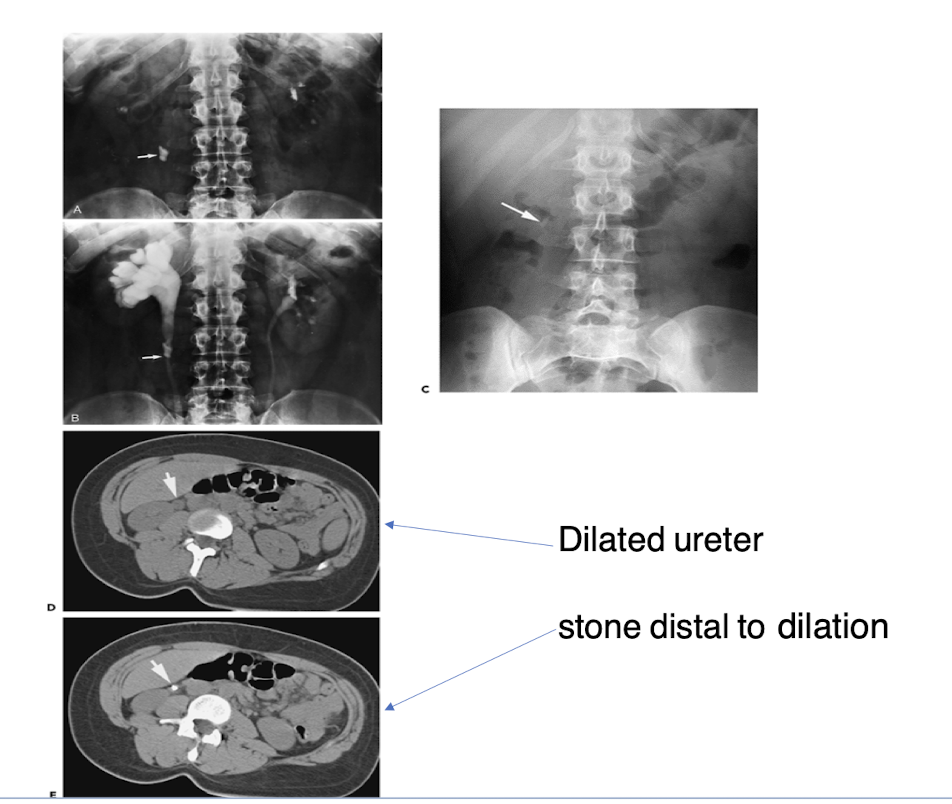
What changes will you see when imaging an acute obstruction?
Dilated renal collecting system, hydronephrosis, or hypofunction of the affected kidney.
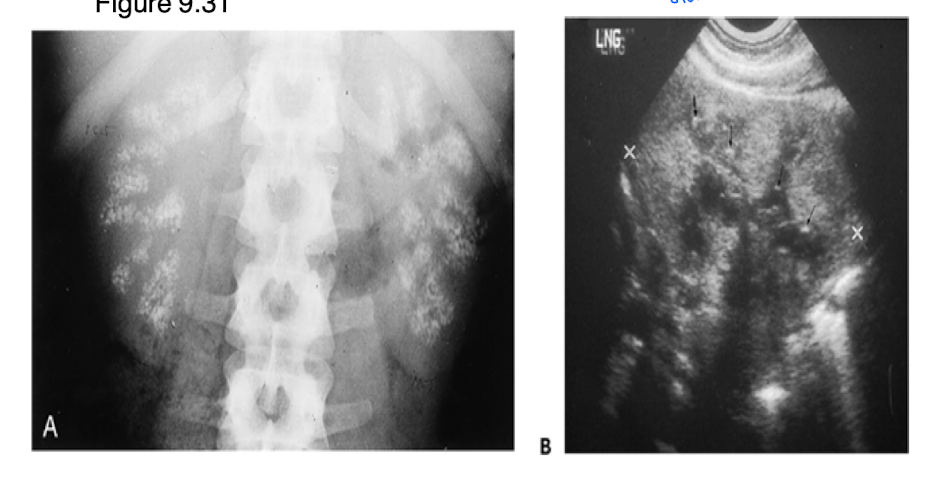
What is nephrocalcinosis? How does it appear on film?
calcium deposits in renal tissue due to increased serum calcium
Uniform opacity, bilateral, and stone is clear, and precise
When is imaging indicated in a patient with pyelonephritis?
pyelonephritis is a severe urinary tract obstruction when there is suspicion of abscess, obstruction, or complications.
An infection that can be difficult to dx on CT if patient is not responsive to treatment
After a renal mass is detected, what is the next logical step?
Further imaging including CT
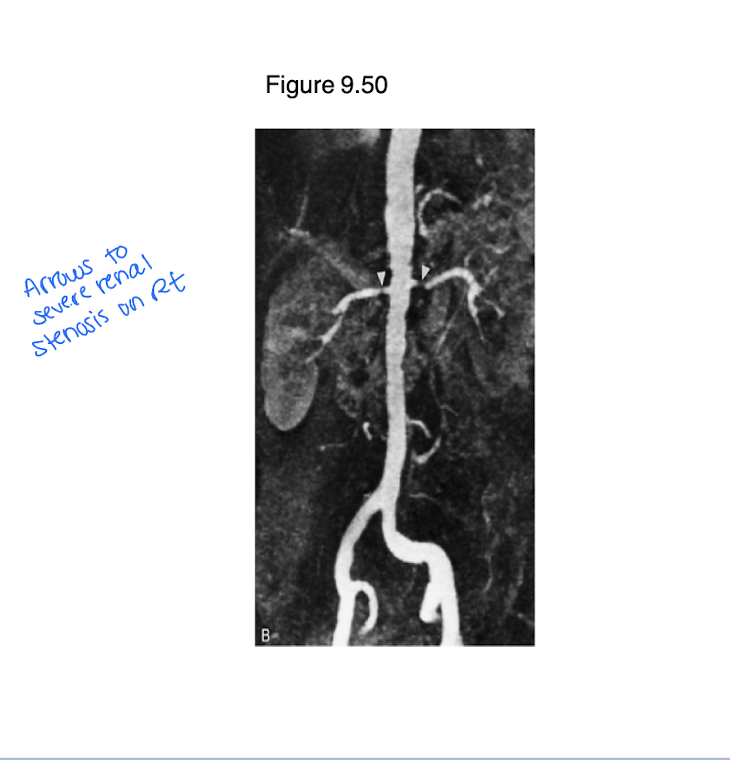
Vascular lesions can lead to renal artery occlusion. What diagnostic tool would be used to evaluate?
Doppler u/s
Angiography
Why would we do a CT of the abd and pelvis when there is injury to the urinary tract?
evaluate kidney function
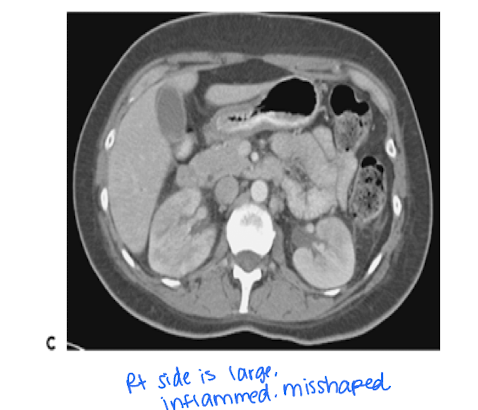
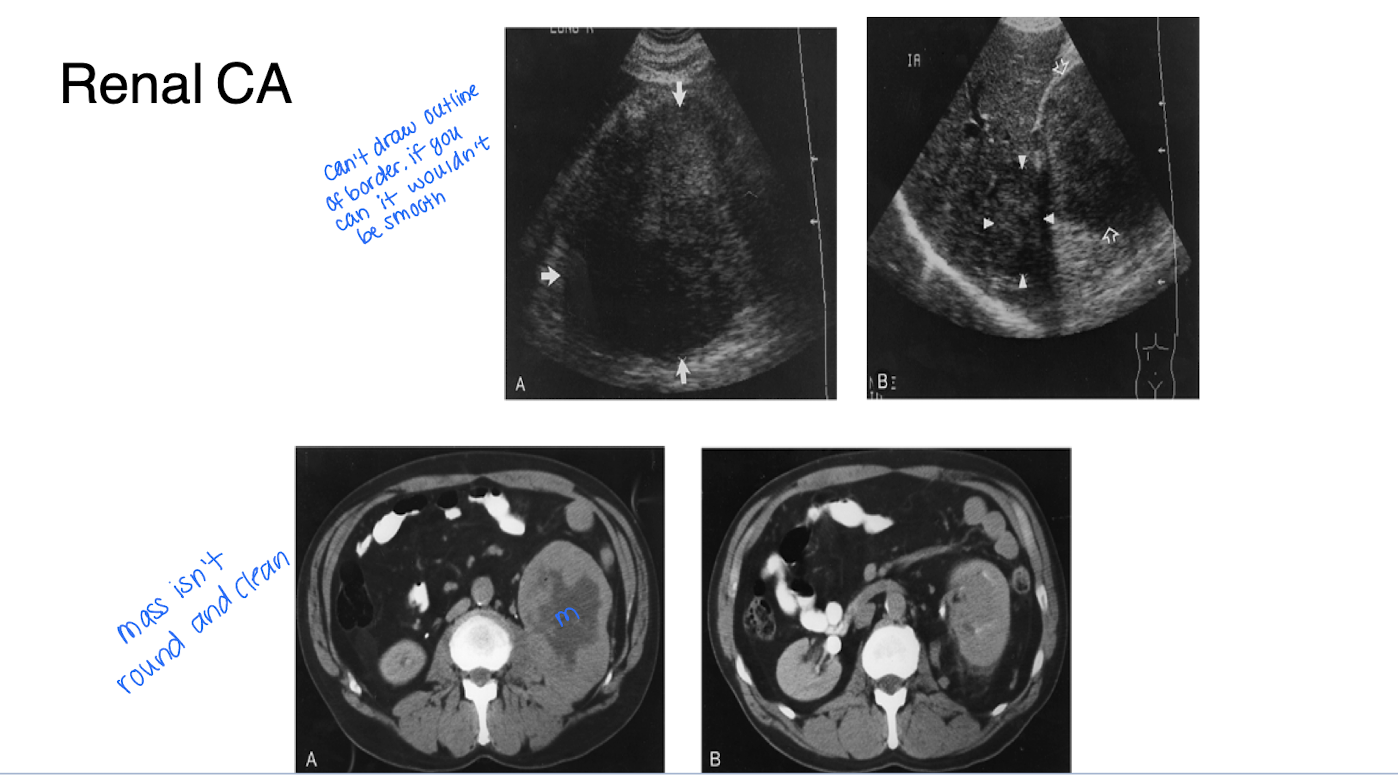
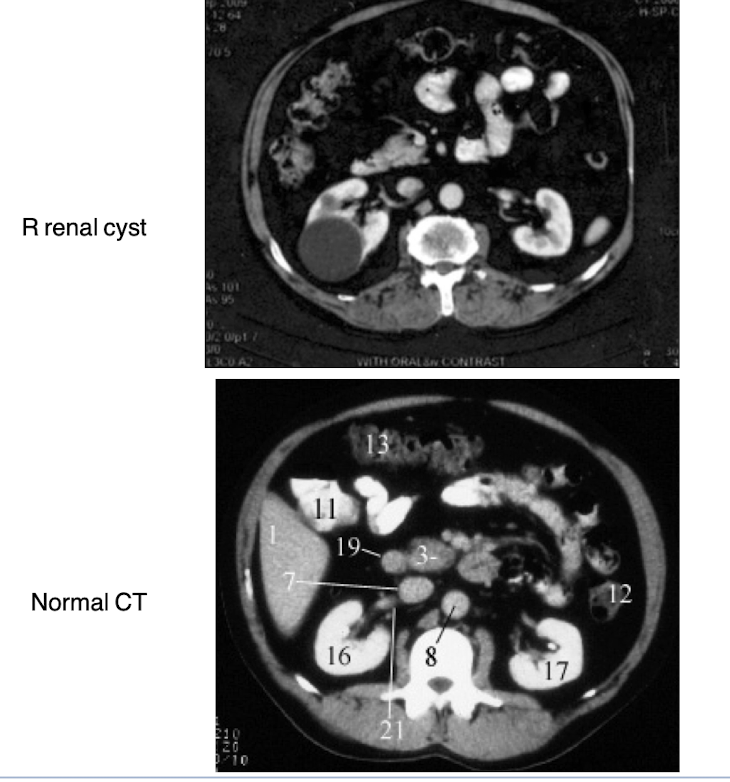
Differentiate between renal cysts and renal carcinoma including characteristics, how they appear when imaged.
Renal cysts are typically simple, fluid-filled sacs that are asymptomatic and have thin walls, while renal carcinoma presents as a solid mass with irregular borders and may show enhancement on imaging studies. Cysts appear anechoic on ultrasound, whereas carcinomas are often hypoechoic and may display vascularity on Doppler imaging.
What is extrinsic compression?
A condition where external structures apply pressure on the urinary tract or kidneys, potentially causing obstruction or dysfunction.
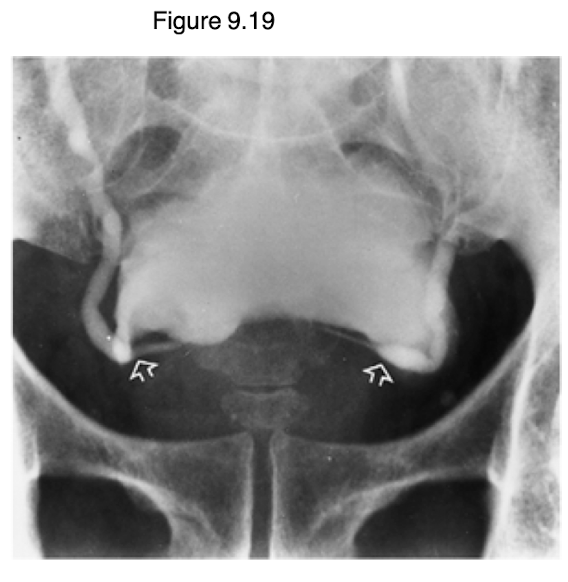
The image does the bladder having an abnormal shape and elevation. This is secondary to an enlarged prostate. What would this be called?
Extrinsic compression
What is vesicoureteral reflux and how is it diagnosed?
Vesicoureteral reflux (VUR) is a condition where urine flows backward from the bladder into the ureters and kidneys, often due to a malfunctioning valve at the ureter-bladder junction.
Juse Cystogram/voiding cystourethrogram
A 42 y/o white female presents with colicky (gassy) pain in her left flank for 4 hours. Patient was working at her desk when the pain began. Nothing makes the pain better or worse. It radiates to the left groin. The patient has never had pain like this before. She rates it 9/10.
On exam she is diaphoretic and in acute distress. CV and lung exam is normal. Abd exam reveals CVA tenderness and no other abnormalities.
Vitals:
T: 36.8C
P: 90 bpm
R: 28
BP: 128/76
What tests would be ordered?
What do you expect to find?
She has kidney stones
Order CT of abd/pelvis
Should see radiopaque mass and dilation of ureter too