7 - Telencephalon
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
what is the telencephalon? what is on the outer and inner surface?
two large hemispheres separated by the longitudinal fissure
outer surface is cerebral cortex containing layers of cells and gyri and sulci
inner surface contains subcortical white matter and gray matter
how many layers are in the neocortex? what % of our cerebral cortex?
6 layers
90% of our cerebral cortex
how many layers are in the paleocortex? what function does it contribute to?
3-5 layers
parts of the olfactory cortex - parahippocampal gyrus and uncus
how many layers are in the archicortex? what part of brain does it contribute to?
max 3 cell layers
parts of the limbic cortex - hippocampal formation and dentate gyrus
what are the primary efferent neuron of the cortex?
pyramidal cells - long axons and apical dendritic trees
what are the types of cortical interneurons and local circuit neurons? what is their primary transmitter? what do they do?
spiny cells, aspiny stellate cells, basket cells
GABA (inhibitory)
they receive afferent signals and talk to each other to create a signal to send down efferent chain
(much is not known about them)
what are the 6 lamellar organization of the neocortex?
I - molecular: most superficial, few neuron cell bodies, mesh of axons running parallel to surface and apical dendrites
II - external granular layer: small/medium size, cortical circuits
III - external pyramidal layer: small/medium size, cortical circuits
IV - internal granular layer: primary receptive layer, contains spiny and aspiny cells. afferent neurons are mostly thalamocortical that synapse here and efferent neurons go from here to nearby cortex in other gyri
V - internal pyramidal layer: medium and large pyramidal cells, principle efferent layer from cerebral cortex, mainly connects to subcortical regions and less to thalamus (go out of hemisphere into brainstem, spinal cord, striatum)
VI - multiform layer: primarily pyramidal cells and has primary corticothalamic projections from this layer
what is the sequence of afferent and efferent neurons to/from the cortex?
cortex receives input —> processes it —> disseminates output to other areas
corticocortical fibers like commissural and association fibers relay from one gyrus to another gyrus
thalamocortical neurons go from specific nuclei in thalamus to layer IV
projection fibers like cortico (spinal, bulbar, striate) and corticothalamic fibers travel from layer V and VI respectively
what is homotypical cortex? what are heterotypical cortex?
homotypical: all 6 layers are clearly definable and roughly equal
heterotypical: some layers are not well defined, related to the function of that area of cortex
what is an example of granular heterotypical cortex? agranular heterotypical cortex?
granular heterotypical: layer IV is well developed, layer V indistinct, where terminations of sensory specific thalamic nuclei. ex: primary visual, auditory, somatosensory areas
agranular heterotypical: layer V is well developed, layer IV indistinct, origin of many long projection fibers and predominantly pyramidal cells. ex: primary motor cortex
most regions of the cerebral cortex receive information from ___ levels of the neural axis via the ____ and project to the ______.
specific regions of the ______ are associated with specific regions of the _______.
lower, diencephalon, diencephalon
diencephalon, telencephalon
what NT are within the cerebrum? what cells use what NT?
GABA, glutamate, neuropeptides/neuromodulators
pyramidal - glutamate (excitatory to post-synaptic cells)
thalamocortical projections - glutamate (sensory and motor control is processed in the thalamus before being sent to the cerebral cortex)
T/F the cerebral cortex receives afferent fibers from the thalamus only.
F, receives afferent fibers from other subcortical regions but these are mostly modulatory
where does the cortex receive most of its modulatory signals? what are the NT that these pathways use?
extrathalamic subcortical regions
5HT (seratonin), NA, Ach, DA, Hist
what are the mechanism of action of these neuromodulatory systems?
enhance/suppress, depending on receptor, can excite or inhibit cortical activity
general arousal state
attention/readiness to attend stimuli - signal to noise ratio
alter motivational state
what is the significance of the neuromodulatory systems?
important for neural plasticity
dysfunction/imbalance in neuromodulatory system can result in?
mood disorders, anxiety disorders, schizophrenia, attention disorders, Alzheimer’s cognitive aspects of Parkinson’s
what is an example of an extra-thalamic neuromodulatory pathway to cortex?
ACh cholinergic pathway that travels from basal forebrain in cerebrum
lack of Ach causes Alzheimer’s and is involved in many other activities like learning, memory, mood, and sleep
what is the noradrenergic system?
a neuromodulatory system that travels from the locus ceruleus of pontine RF. the locus ceruleus responds to changes in sensory input such as enhancing signal to noise ratio
what is the serotonergic system?
a neuromodulatory system from the Raphe Nucleus of the pons and midbrain and uses the NT 5-HT. it enhances or suppresses neuronal activity
what does dysfunction of 5-HT or 5-HT combined with NA cause?
depression, anxiety, aggressive behavior, ED’s, OCD
what is the dopaminergic system?
from ventral tegmentum of midbrain and pars compacta in the substantia nigra. have several receptor types that have differing actions (D1-D5)
dysfunction can cause hallucination in Schizophrenia, cognitive dysfunction of Parkinson’s, Alzheimer’s
what are histaminergic neuromodulatory pathways?
from the hypothalamus and have a role in wakefulness. inhibition is associated with sleep
what are the functions of the primary motor cortex (M1)? where is it and its Brodmann’s area?
control of specific, well-defined movement in distal muscles, connections to areas of thalamus related to motor and sensory information
precentral gyrus, Brodmann’s area 4
what are the subcortical afferent pathways to the the primary motor area (M1)? does it have a somatotopic arrangement?
cerebellum → VL → M1
somatic sensory → VPL → M1
yes
what happens with a lesion to the primary motor area?
contralateral motor deficit (corticospinal tracts cross over)
what consists of the secondary motor areas? what are its functions? what do the secondary motor areas receive from?
supplementary motor area and premotor area
control of proximal muscles, initial phases of movement, planning of movements, interlimb coordination, movements guided by visual and tactile sensory info
has few thalamic connections
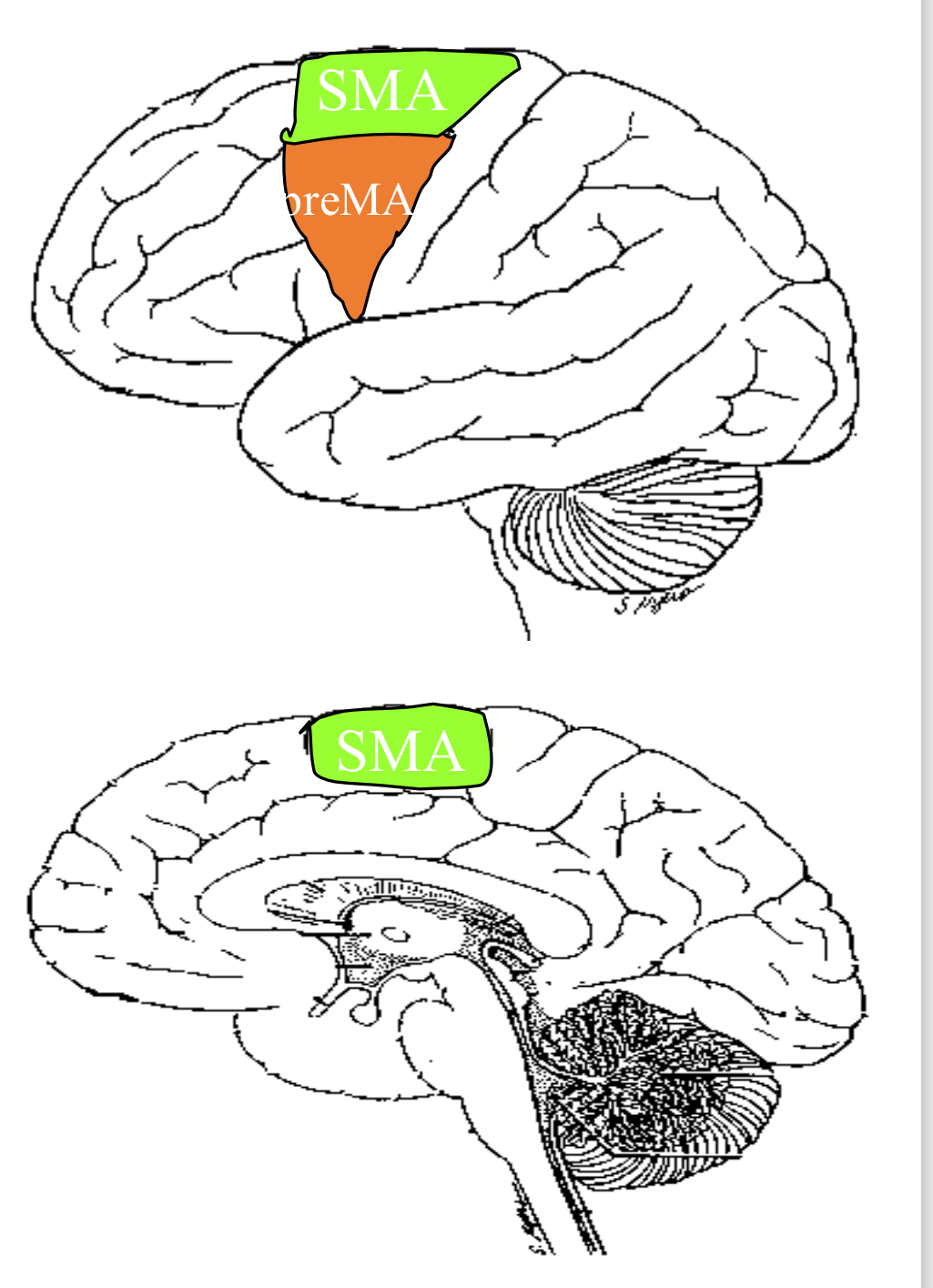
where is the secondary motor area located?
frontal to the precentral gyrus (M1)
what is the pathway to the secondary motor areas?
receive subcortical afferents
globus pallidus and substantia nigra → VA/VL → SMA
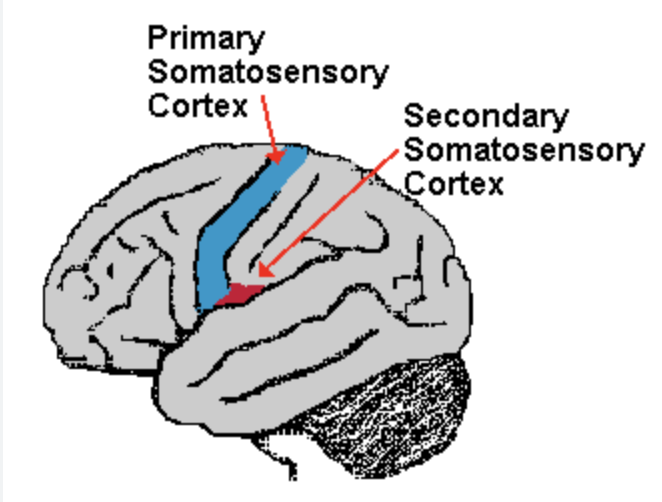
what is Brodmann’s area for the primary somatosensory area? what information does it process?
Brodmann’s 3,1, 2
processes somatic info - non discriminative touch, discriminative touch and pain, position, vibration
what is the afferent pathway to the primary somatosensory area (S1)? does it have a somatotopic arrangement?
ascending sensory pathways → VPL&VPM → S1
yes
what happens if there is a lesion to S1?
contralateral sensory deficits (spinothalamic and PCML tracts cross over)
what is the secondary somatosensory area? what is its function? what region of the thalamus does it come from?
on the dorsal wall of the lateral sulcus
has less discriminative aspects of sensation like processing pain information
comes from VPL or VPM from the thalamic nuclei (somatosensory pain)
ventral posterolateral nucleus in the thalamus (VPL)
ventral posteromedial nucleus in the thalamus (VPM)
VPL: where all the body’s information comes from
VPM: where information from the head comes from
where is the primary language processing area found?
dominant hemisphere, left 95% of the time (L-handed individuals 70%)
what hemisphere is responsible for motor movement of contralateral limbs?
both dominant and non-dominant
what hemisphere is responsible for comprehension and production of written and spoken language? what hemisphere is responsible for prosody of language production and comprehension?
dominant
non-dominant
what hemisphere is responsible for visual-spatial analysis and spatial attention only to the contralateral space? what hemisphere is responsible for visual-spatial analysis and attention in the bilateral space and integrated visuospatial gestalt?
dominant
non-dominant
what hemisphere is responsible for sequential and analytical calculating skills? what hemisphere is responsible for ability to line up columns of numbers on page?
dominant
non-dominant
what hemisphere is responsible for 3D recognition and recognition of faces?
non-dominant hemisphere
what hemisphere is responsible for following a set of written directions in sequence, analytical thinking, decision/problem solving based on analytical data? what hemisphere is responsible for finding one’s way by overall sense of spatial orientation, intuitive thought, creative/artistic abilities
dominant
non-dominant
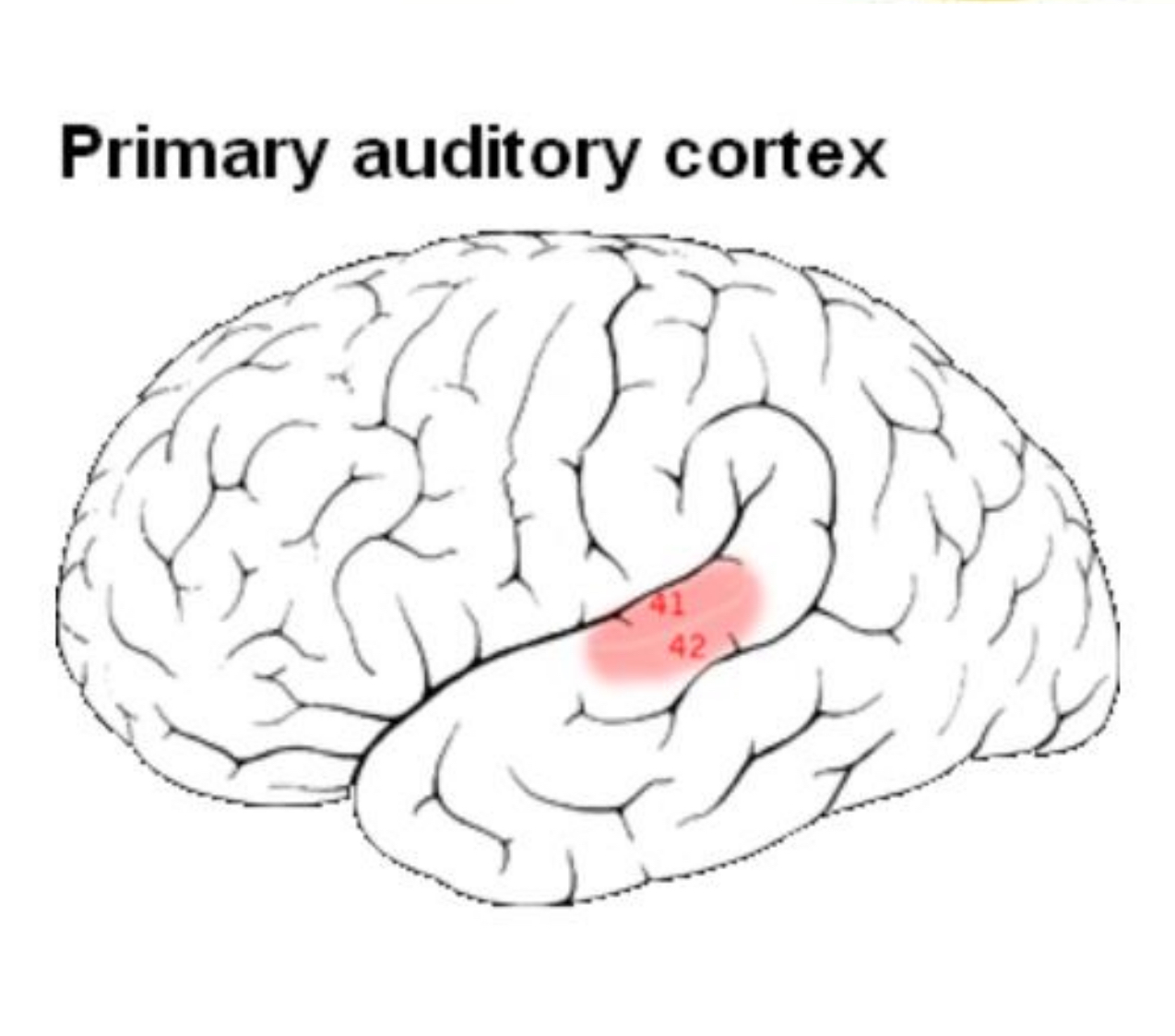
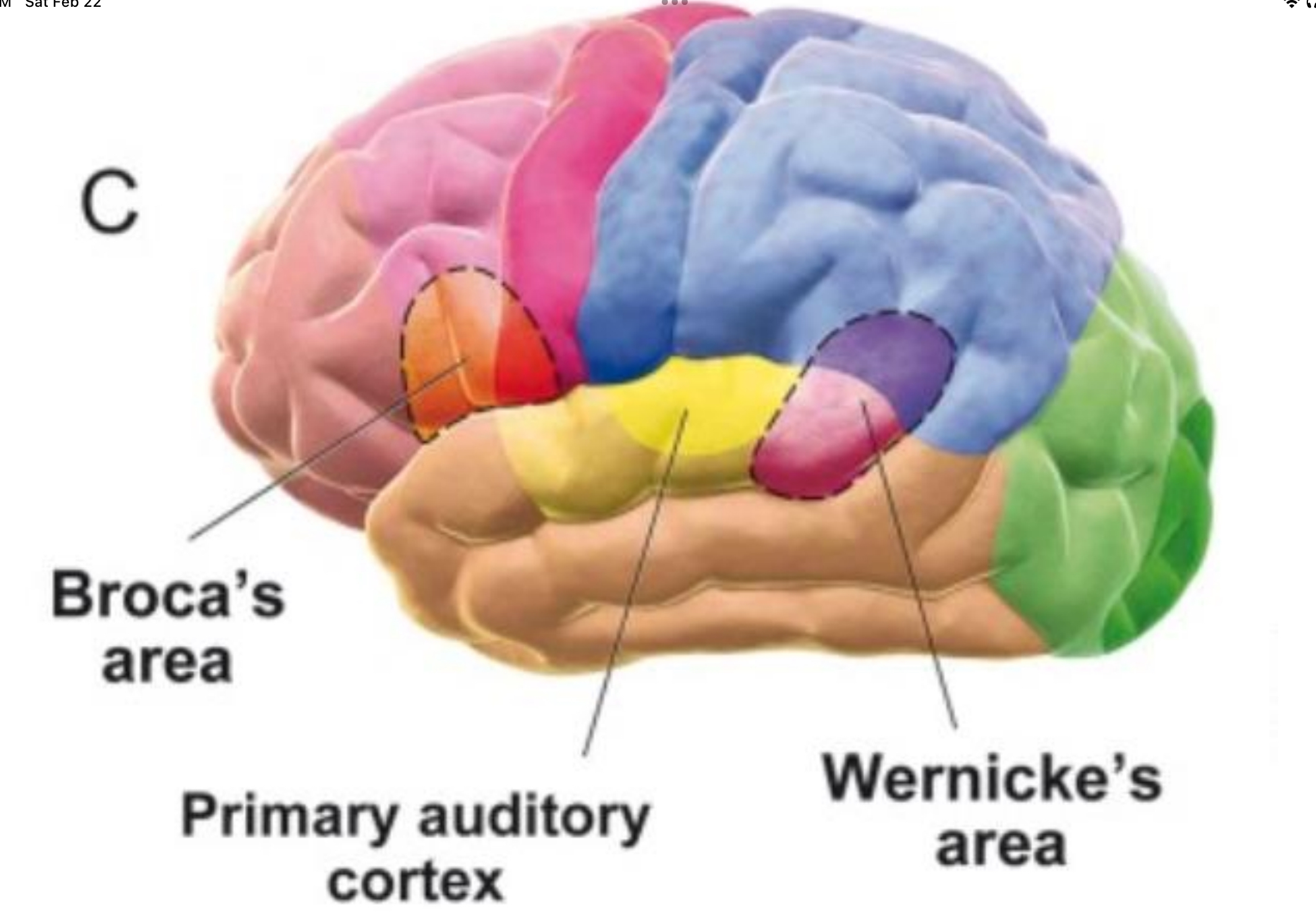
what is Brodmann’s area for primary auditory area? what part of the thalamus do its afferent neurons come from? what happens if a lesion occurs?
Brodmann’s 41&42 (transverse temporal gyri)
thalamic afferents from the medial geniculate body
lesion: difficulty in interpreting or localizing a sound, but not deafness
where is Wernicke’s area? Brodmann’s? what is its function?
in dominant hemisphere in superior temporal gyrus (auditory) and supramarginal and angular gyri (written)
Brodmann’s area 22, 40, 39 respectively
associates auditory information with speech qualities in Broca so we respond correctly
associates this auditory input with memories to allow comprehension
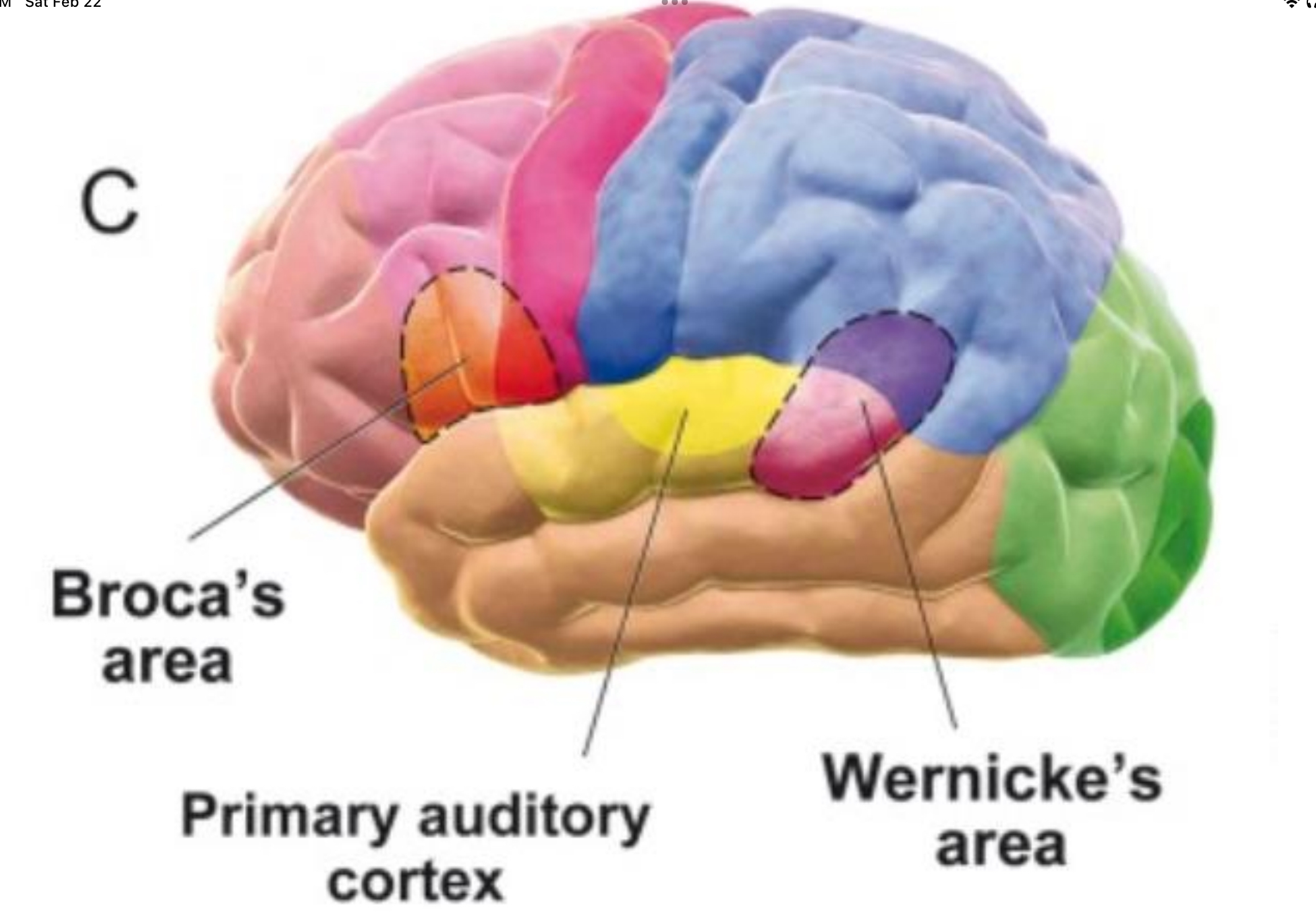
what is Broca’s area? Brodmann’s? function?
speech production in dominant hemisphere, inferior frontal gyrus
Brodmann’s area 44 & 45
brings together information begin process of creating motor production and speech, also has role in detecting inappropriate word use (semantics)
what is the pathway for the ability to hear and repeat words?
primary auditory cortex —> Wernicke’s —> arcuate fasciculus —> Broca’s —> Motor areas
what is the non-dominant hemisphere’s role in speech?
comprehension and production of affective elements of speech, prosody
temporoparietal does comprehension and inferior frontal does production
also decodes non-standard meanings, processes metaphors, understands themes
what is Broca’s aphasia and sx? where is the lesion?
difficulty turning concept or thought into meaningful sounds
decreased fluency of spontaneous speech, often halting, short phrases, content words, severe cases results in mute
comprehension is okay
repetition and naming is impaired. often accompanied by agraphia which is the inability to express thoughts in writing
lesion in superior division of MCA (middle cerebral a.)
what is Wernicke’s aphasia and sx? where is the lesion?
impaired comprehension of auditory and written language
spontaneous speech - normal fluency and prosody, but makes no sense. paraphasic errors - unintended syllables or words. neologisms - made up words
inferior division of MCA
if a pt is aware of their speech deficit and is frustrated and upset, they most likely have?
if pt is unaware of deficit, they most likely have?
Broca’s
Wernicke’s
what is agraphia and alexia?
language deficit - disruption in the ability to write and read respectively
can be simultaneous or isolated. often due to lesion at the junction of parietal, occipital, temporal lobes (angular and supramarginal gyri)
what is Brodmann’s area in the posterior and parietal association cortex? function? what happens with a lesion?
Brodmann’s 5&7
does higher order processing, integration of sensory information - visual, auditory, tactile, vestibular, formation of perceptions. attention to the spatial aspects of sensation. motor planning is based on sensory input
important for the initiation on movement
lesion is most impacting on non-dominant hemisphere
what parts of the brain are most important for integrated sensory-spatial gestalt? what hemisphere of brain is more important for attention?
parietal (over frontal) and non-dominant hemisphere (over dominant)
non-dominant
what happens with a lesion in the non-dominant hemisphere?
difficulty with tasks requiring visual-spatial analysis
decreased constructional abilities (most severe R parietal lesions). R side lesion causes errors in overall organization
decreased attention and alertness
personality/emotional changes - bland, apathetic, irritable
difficulty using/interpreting prosody of speech
hemi-neglect syndrome (because dominant side only has contralateral awareness)
what is contralateral neglect and where is it? types?
typically R parietal (or frontal) lesion in non-dominant side
types include sensory (ignore sensory stimuli), motor-intentional (fewer movements in contralateral hemispace), combined sensory and motor and conceptual (deny body part is theirs)
what is agnosia? what are the types?
inability to interpret sensation, often lesion is in a modality specific area of sensory association cortex
types:
tactile agnosia/astereognosis
visual agnosia includes prosopagnosia which is inability to recognize faces (lesion in bilateral inferior occipitotemporal assoc cortex), color agnosia
auditory, gustatory, olfactory agnosia
what is a lesion in the prefrontal region? result?
all of frontal lobe in front of supplementary motor area and premotor cortex is affected by lesion
restraint, initiative, and order functions are impaired
prefrontal is important for learning new material, selective attention, integration of information in decision making
what are common signs and behaviors in prefrontal lesions?
abulia - lifelessness and delayed responses
disinhibition - inability to suppress inappropriate responses, silly, aggressive, inappropriate
confabulation - fill in memory gaps by fabricating
inability to maintain attention
perseveration: continued or repetition of activity beyond app end point
reduced abstract reasoning
diminished ability to generate lists
incontinence
frontal release signs - primitive reflexes such as grasp
gait abnormalities - shuffling, unsteady, magnetic
what is disconnection syndrome? sx?
dysfunction caused by damage to association or commissural pathways
b/w hemispheres (corpus callosum lesion) - R hemisphere is unable to access language functions in L hemisphere - can’t name objects placed in L hand, inability to write w/L hand, inability to read material in L hemi-field, difficulty with bimanual coordination
what are the types of fiber pathways?
association - within lobe
commissural - lobe to lobe
projection - up and down
what are examples of long association fasciculi? short association fibers? commissure fibers? projection fibers?
cingulum, superior longitudinal fasciculus, uncinate fasciculus, inferior fronto-occipital fasciculus, arcuate fasciculus
arcuate fibers
corpus callosum, anterior commissure
corona radiata (between cortex and internal capsule), internal capsule (cortex to subcortical structures)