Module 3 - Abdominal Radiography Flashcards
1/61
Earn XP
Description and Tags
Flashcards for Abdominal Radiography Review
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
62 Terms
Why is knowledge of abdominal body habitus important in radiography?
It helps with proper centering, inclusion of necessary structures, and determining the need for additional images.
What should a technologist do if a patient’s stature is too large for one IR?
Use multiple IRs to ensure complete inclusion of required abdominal structures.
What is the typical instruction for including abdominal anatomy?
"Pubic symphysis up" or "diaphragm down" to include as much of the abdomen as possible.

What structures must be included bilaterally on an abdominal image?
Flank stripes.
What anatomy should be included on a supine abdomen image?
From T11/T12 to the pubic symphysis, including bilateral flank stripes.

What anatomy should be included on an upright/decubitus abdomen image?
From T8 (including diaphragms) to the sacrum, including bilateral flank stripes.
How should supplementary projections show coverage?
They should clearly demonstrate overlap to ensure continuity.
What is a single view abdominal exam often called, and what is it used for?
Scout or preliminary image; used to assess line placement, fecal loading, or before contrast studies.
What structures must be included in a single supine abdominal image?
Same as in a routine supine abdominal image: T11/T12 to pubic symphysis.
What is included in a typical multiview abdomen (ABM) exam?
Supine AXR, PA/AP upright AXR, and sometimes PA chest X-ray.
Why is a PA chest sometimes included in an abdomen series?
To rule out air under the diaphragm and assess thoracic causes of abdominal symptoms.
What is the purpose of an upright abdominal projection?
To assess for air-fluid levels and free air in the abdominal cavity.
What anatomy must be included in an upright abdomen image?
Diaphragms and vertebral level T8.
When is a lateral decubitus abdomen projection used?
When the patient cannot stand for an erect image; to detect free air.

Why is the left lateral decubitus preferred for detecting free air?
Free air contrasts best against the liver on the right side.
How long should a patient remain in position before taking a decubitus image for free air?
Approximately 5–10 minutes.
Where should the decubitus marker be placed?
On the downside (side in contact with the table).
Where will free air accumulate in wide-hipped patients during a decubitus?
At the iliac bone, which is the highest point in the peritoneal cavity.
Why are male and female pelvises different radiographically?
Female pelvises are wider to accommodate fetal development and childbirth.
How can recognizing pelvic differences assist in abdomen imaging?
Helps determine if the projection is AP or PA and interpret anatomical variation.
What is a benefit of doing a PA upright abdomen instead of AP?
Reduces gonadal dose and allows unstable patients to hold onto the bucky.
How do AP and PA projections differ in pelvis appearance?
Differences in ala shape and pelvic inlet, though some differences may stem from gender, not projection.
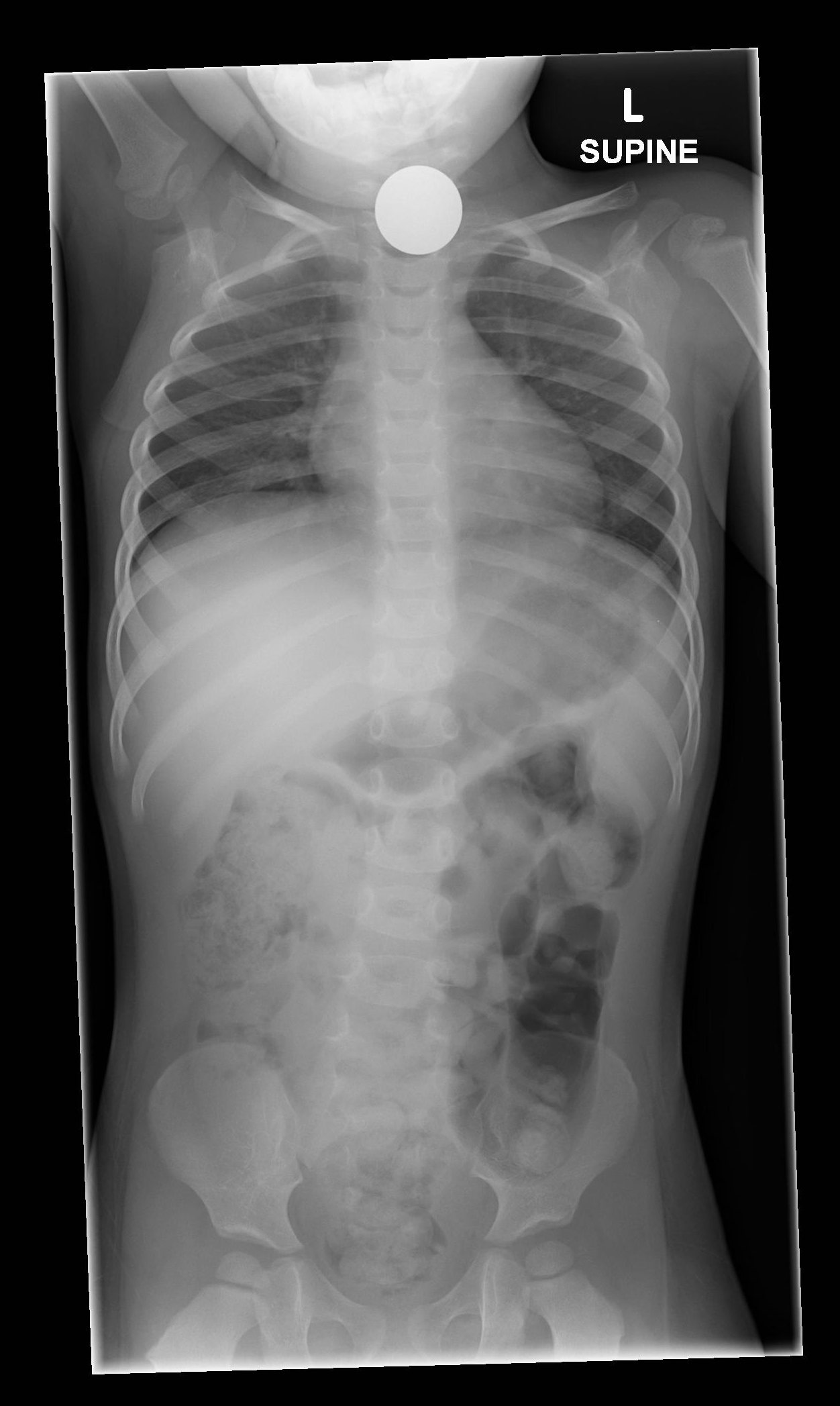
What anatomy is included when imaging for foreign body (FB) ingestion in children?
From nasopharynx to anus.
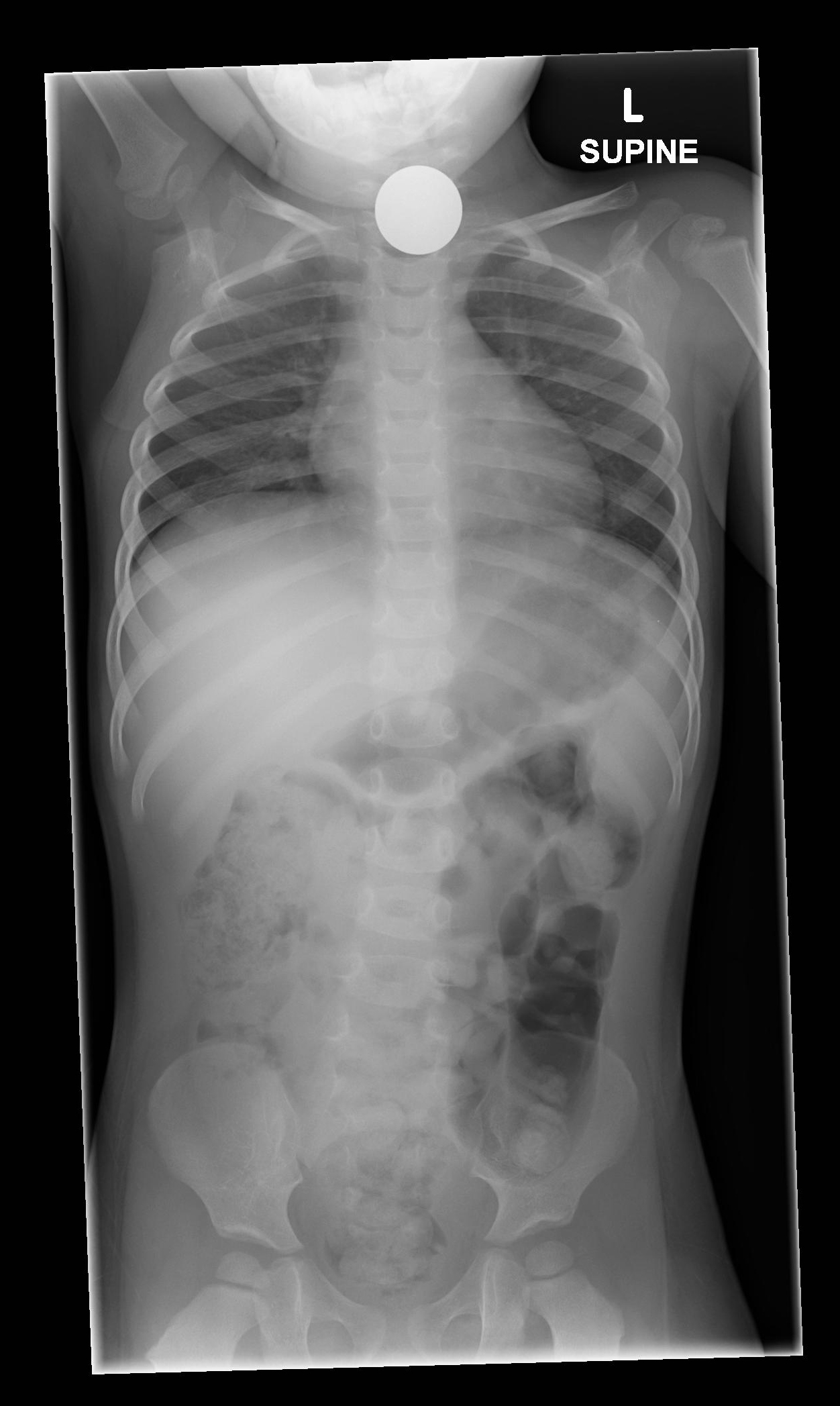
Why is full coverage important in pediatric FB imaging?
To identify if the FB is in the airway or gastrointestinal tract for appropriate treatment.
What are criteria for good abdominal image quality (IQ)?
Sharp gas outlines, Visible thoracic spine through heart shadow, Defined psoas muscles, kidneys, liver, Uniform density, Sharp cortical outlines (spine/ribs/pelvis), No motion artifacts
Why should abdominal images be taken on full expiration?
To elevate the diaphragm, reduce compression, and provide uniform density.

What causes voluntary motion in abdominal imaging?
Patient movement or breathing; preventable with proper instruction and short exposure time.
What causes non-voluntary motion, and how is it managed?
Peristalsis; minimized using reduced exposure time but not completely preventable.

What is assessed for alignment in abdominal images?
Lumbar spine parallel to IR, No torso or pelvic tilt, LCM and ala on the same transverse plane
What indicates rotation on an abdominal radiograph?
Spinous processes not midline, Unequal iliac wings or obturators, Sacrum not aligned to pubic symphysis
Why is reviewing site protocol and the patient requisition important before imaging?
To determine proper centering, structures required, and the number and type of projections needed.
When might a supplementary abdominal projection be required?
When the primary image doesn’t fully include necessary anatomy or when patient size/history indicates additional coverage is needed.
What is a KUB image?
A focused abdominal X-ray to assess the kidneys, ureters, and bladder.
How is collimation adjusted for a KUB image?
Lateral margins are not required; collimation should extend medially to the ASIS to avoid clipping.
How can you prepare a patient for a decubitus abdomen exam to improve efficiency and image quality?
Place them in the lateral position early (e.g., during room setup) to allow air to rise to diagnostic areas.
What is a common workflow strategy in busy departments for decubitus views?
Perform supine and chest X-rays first, then let the patient rest in lateral decubitus before imaging.
What are the main advantages of a decubitus abdomen over an upright one?
More comfortable for ill patients, and it still allows visualization of free air.
In which direction does free air move in the left lateral decubitus position?
Toward the right upper quadrant, below the diaphragm, between the liver and abdominal wall.
Why is expiration preferred for abdominal imaging?
It elevates the diaphragm, reduces compression of abdominal contents, and improves visibility of structures.
How can you confirm full expiration on an upright image?
The dome of the diaphragm should be seen at or above the level of the 9th posterior ribs.
What features indicate poor image quality in abdominal imaging?
Blurred gas outlines, Uneven density
Why must radiographers strive for high image quality despite digital post- processing capabilities?
Because post-processing reduces the radiologist’s ability to manipulate the image and interpret subtle pathology.
How do you tell the difference between voluntary and non-voluntary motion artifacts?
Voluntary motion causes more noticeable blurring and streaking; non-voluntary motion is subtler and often localized to the bowel.
Can peristalsis be stopped during abdominal imaging?
No, but its effects can be minimized by shortening exposure time.
Why is abdominal imaging considered “easier” to critique?
Because many criteria from other body regions (e.g., alignment, rotation, respiration) are transferable.
What are some criteria transferable from chest to abdominal imaging?
Spine straight and centered, Symmetrical rib/pelvis structures, Full expiration, Clear, sharp anatomical outlines
What vertebral level indicates inclusion of the diaphragm on an upright abdomen?
T8
What vertebral level typically aligns with the lower poles of the kidneys on a supine image?
L3 transverse processes
What landmark helps ensure inclusion of inferior abdominal contents?
Pubic symphysis
What landmark helps guide lateral collimation for KUB?
ASIS (Anterior Superior Iliac Spine)

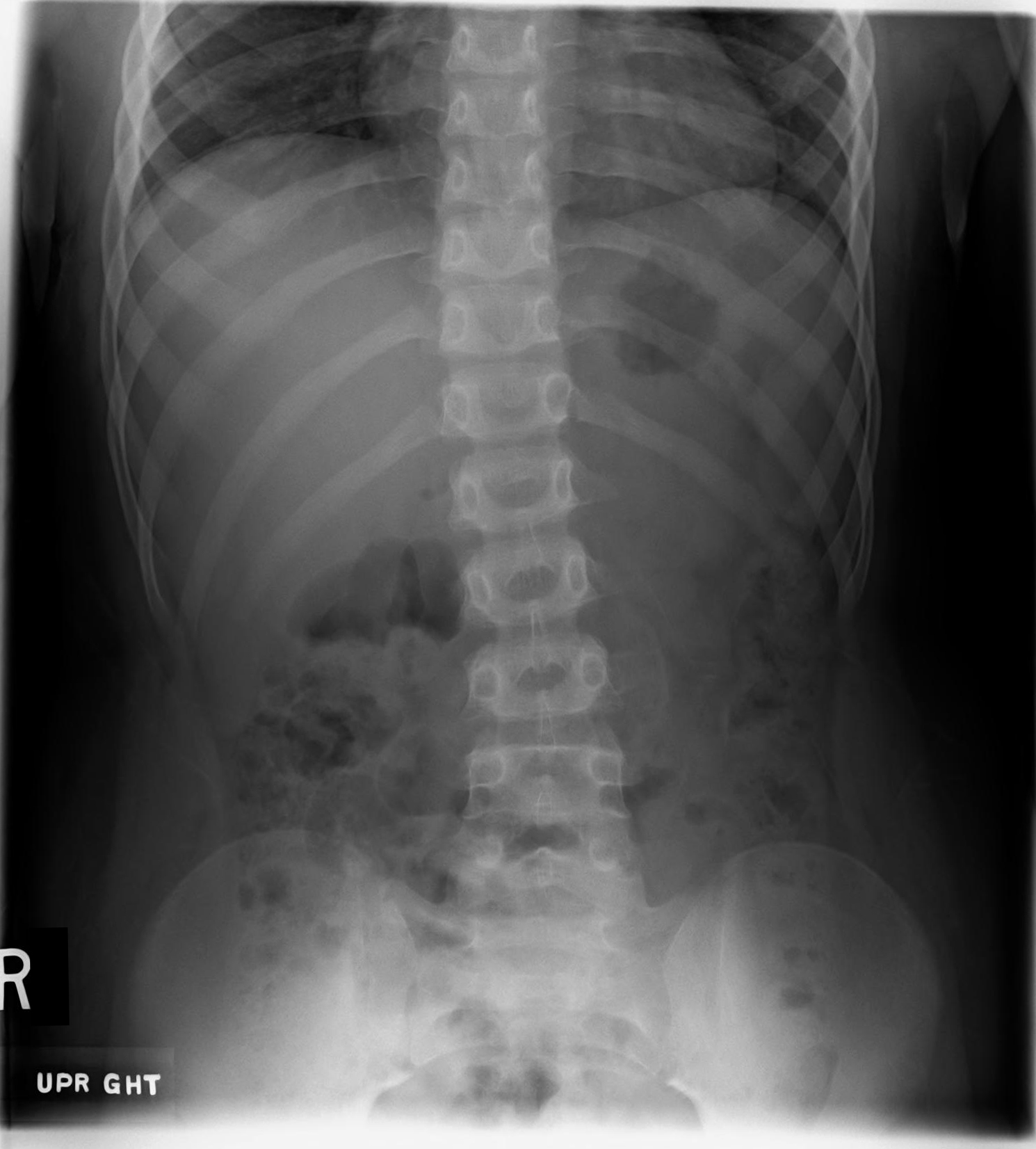
What phase of respiration has been captured for this projection? What is seen radiographically to support the assessment?
Expiration; lower poles of kidneys are at the transverse processes of L3


25 y/o a multi-abdomen series. c/o lower abdomen pain. The req states "? hernia". Assess the structures included?
Superior-inferiorly most of T12 to the pubic symphysis; bilaterally both flanks have been included. Though not all of T12 is seen, the upper pole of the left kidney has been demonstrated.
Minimal exposed space lateral to the left ala.

25 y/o a multi-abdomen series. c/o lower abdomen pain. The req states "? hernia". Assess the structures included? Assess the phase of respiration
Inferior poles of kidneys are located superior to the L3 transverse processes = good expiration

What are notable image flaws?
RPO pelvic rotation; Wider right ala and SP's of lower spine deviating towards the left
Tilt towards the left in the shoulders and hips - left LCM and ala more inferior than the right side
Collimation - one-sided on the right (patient's right). Unable to accurately determine excess or CP.
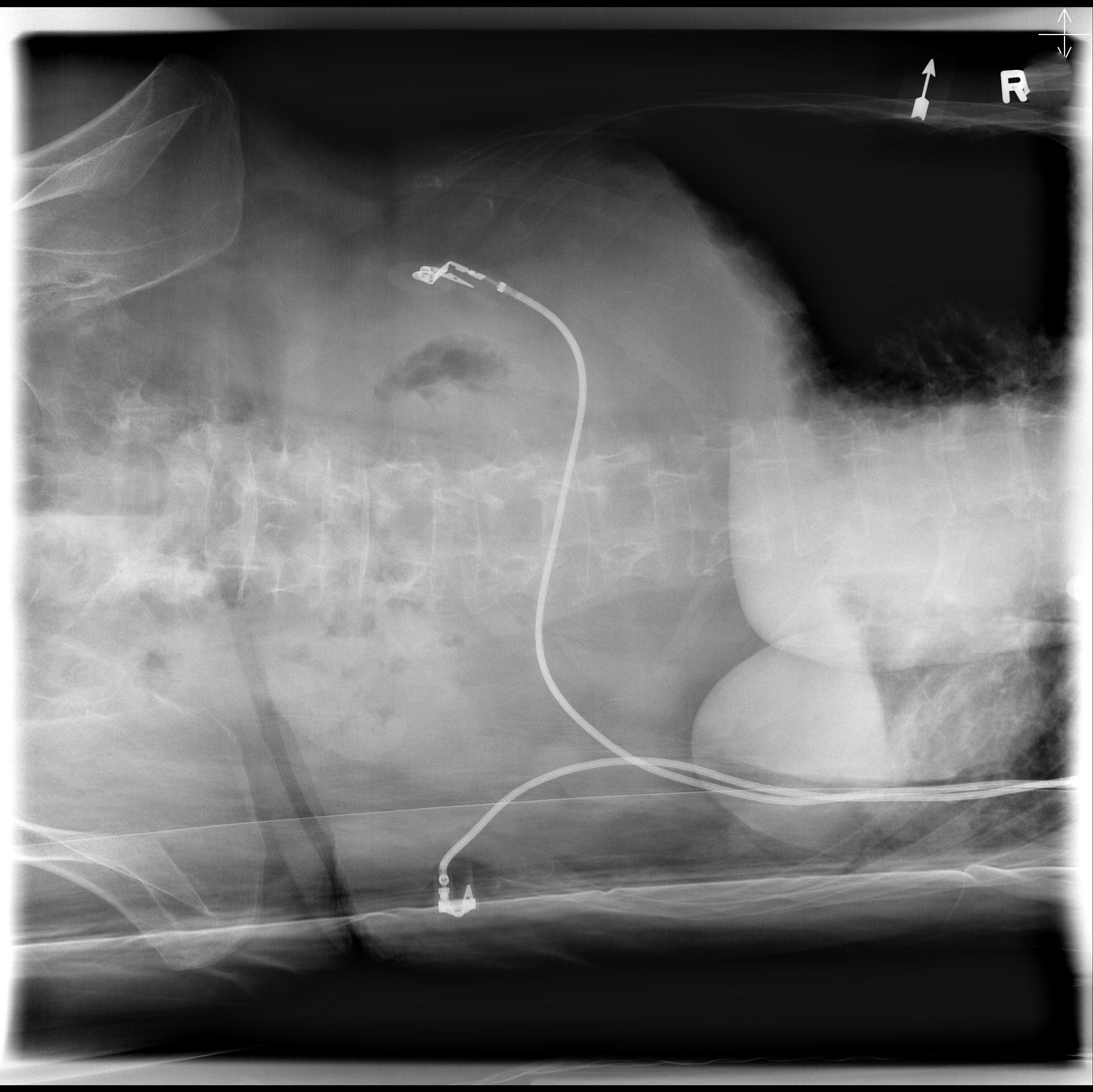
Name the projection title?
PA Left Decub
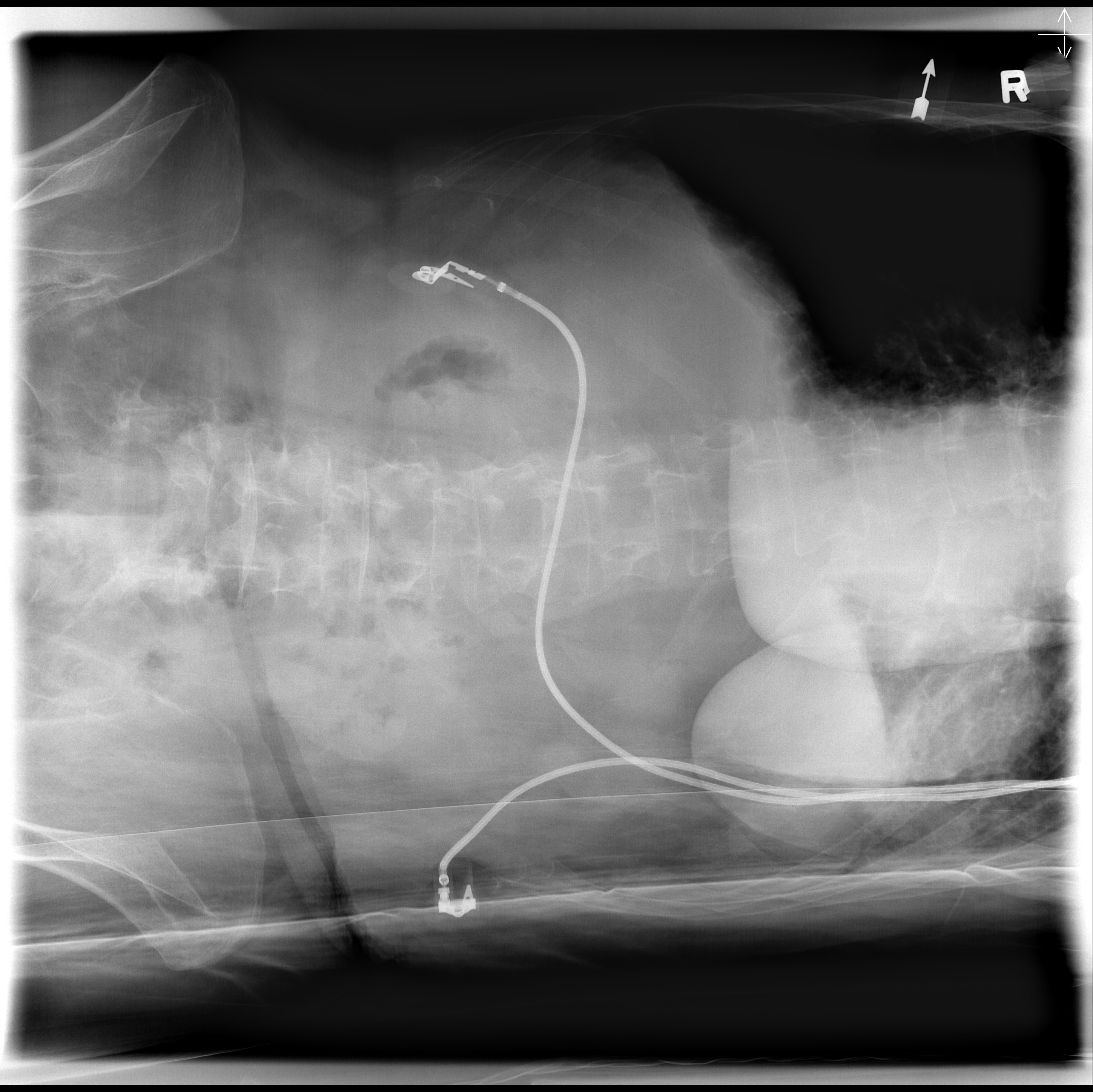
Assess Structures included?
Good sup-inf; Excess bilaterally
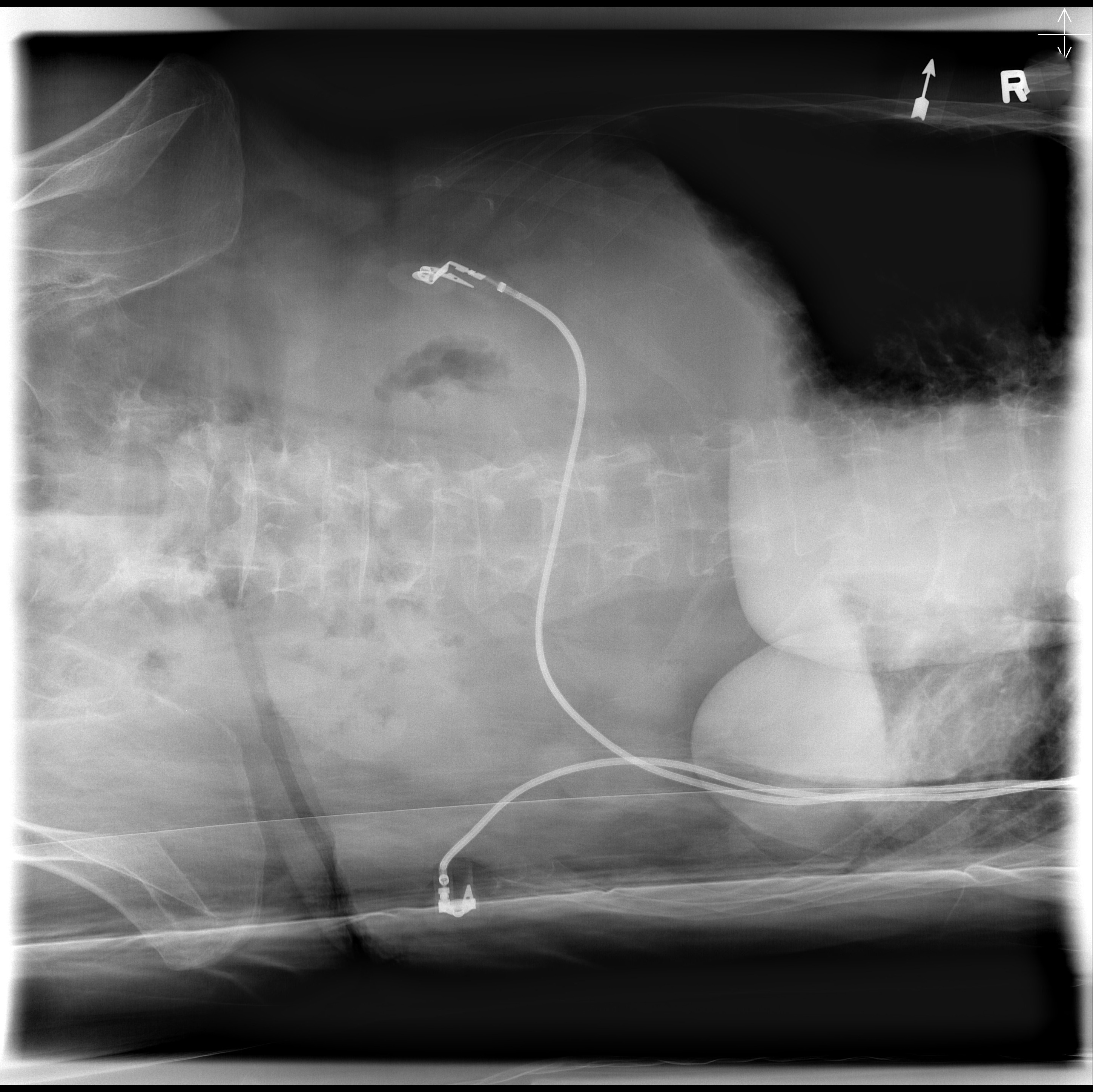
Assess pelvic rotation?
Pt is PA; Left ala is wider = RAO
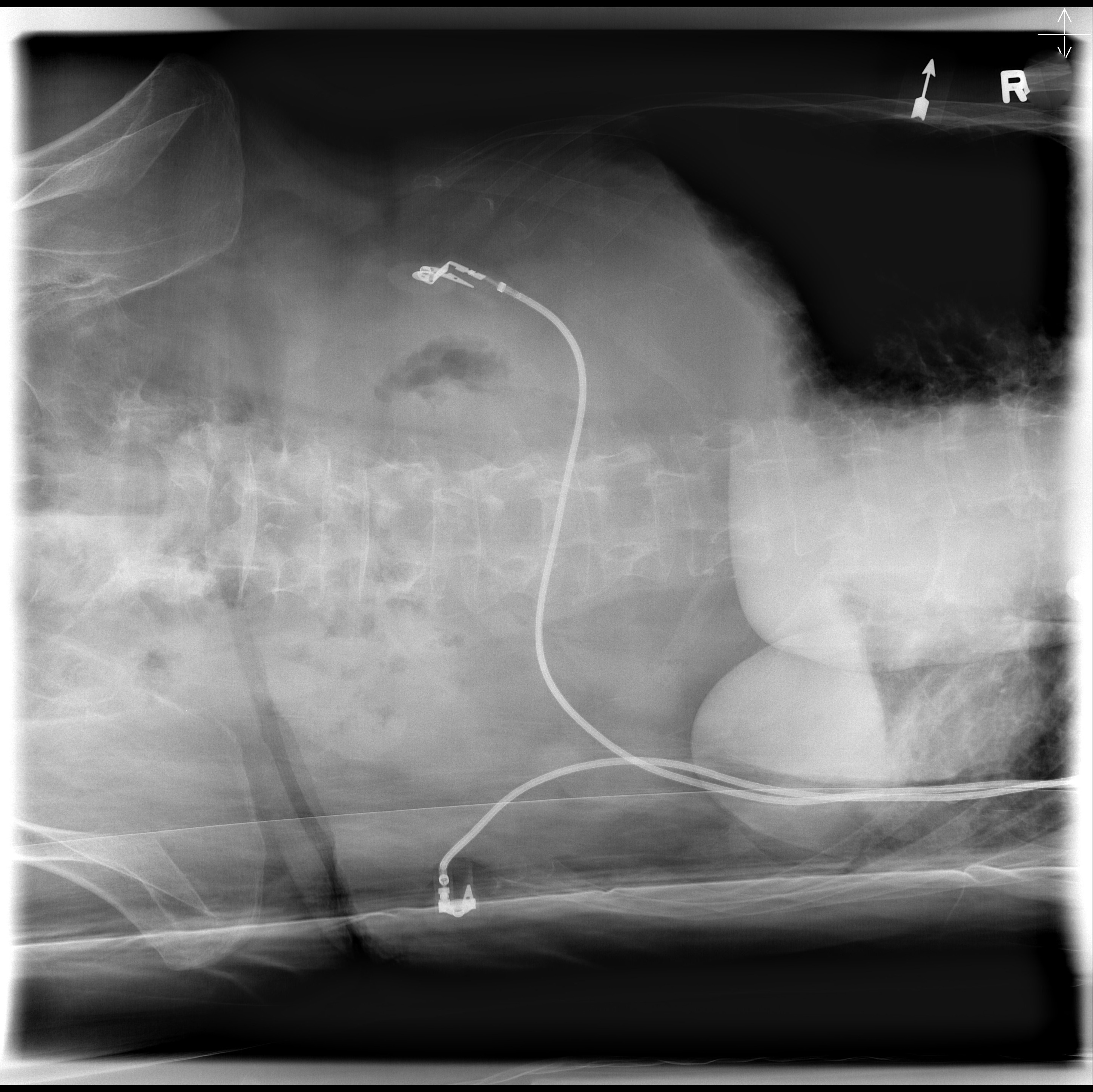
Assess thorax rotation
Pt is PA; SP's not midline and moving towards the RT pedicle = RAO
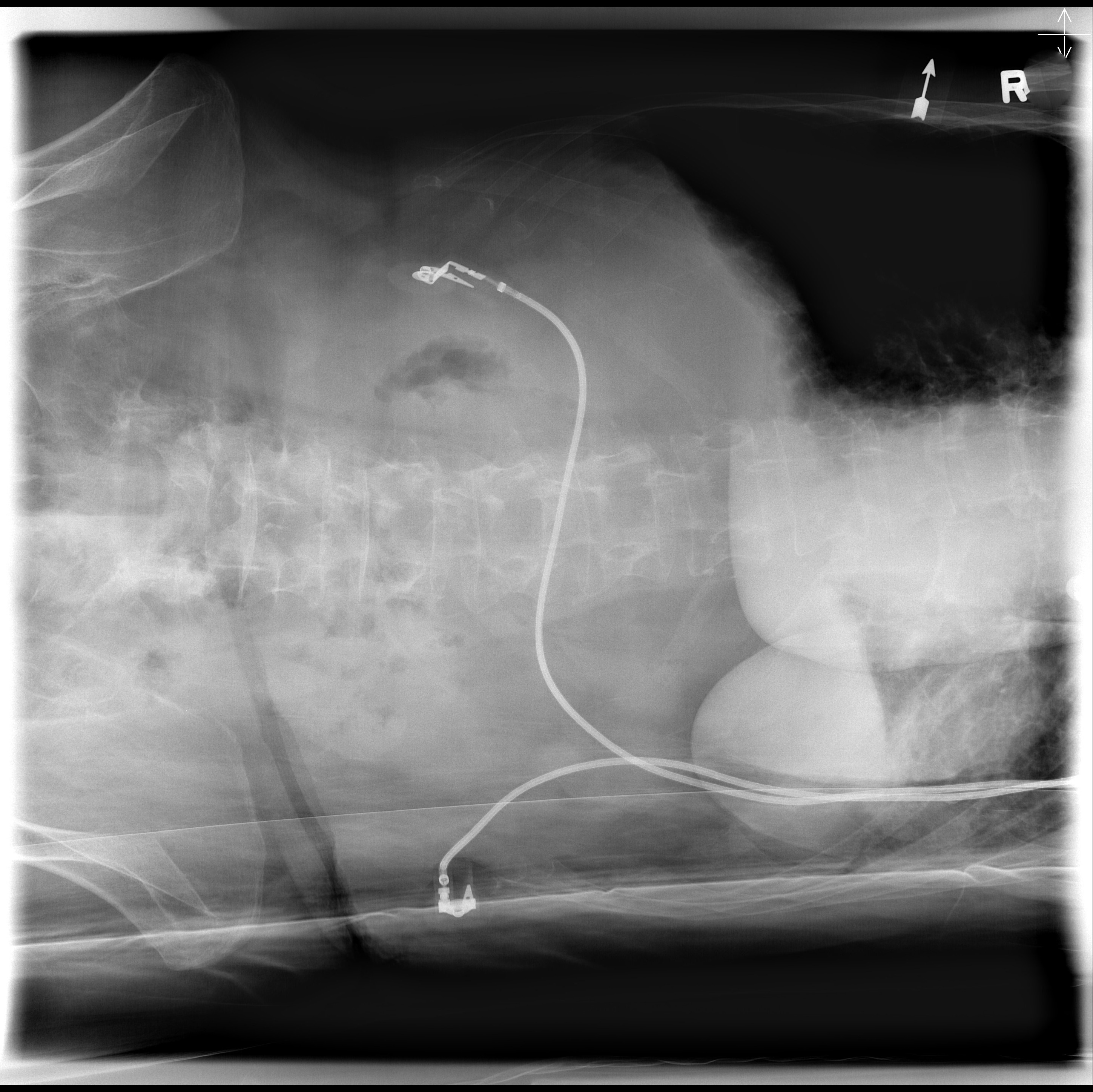
Assess tilt
Pelvic and thorax tilted to the right
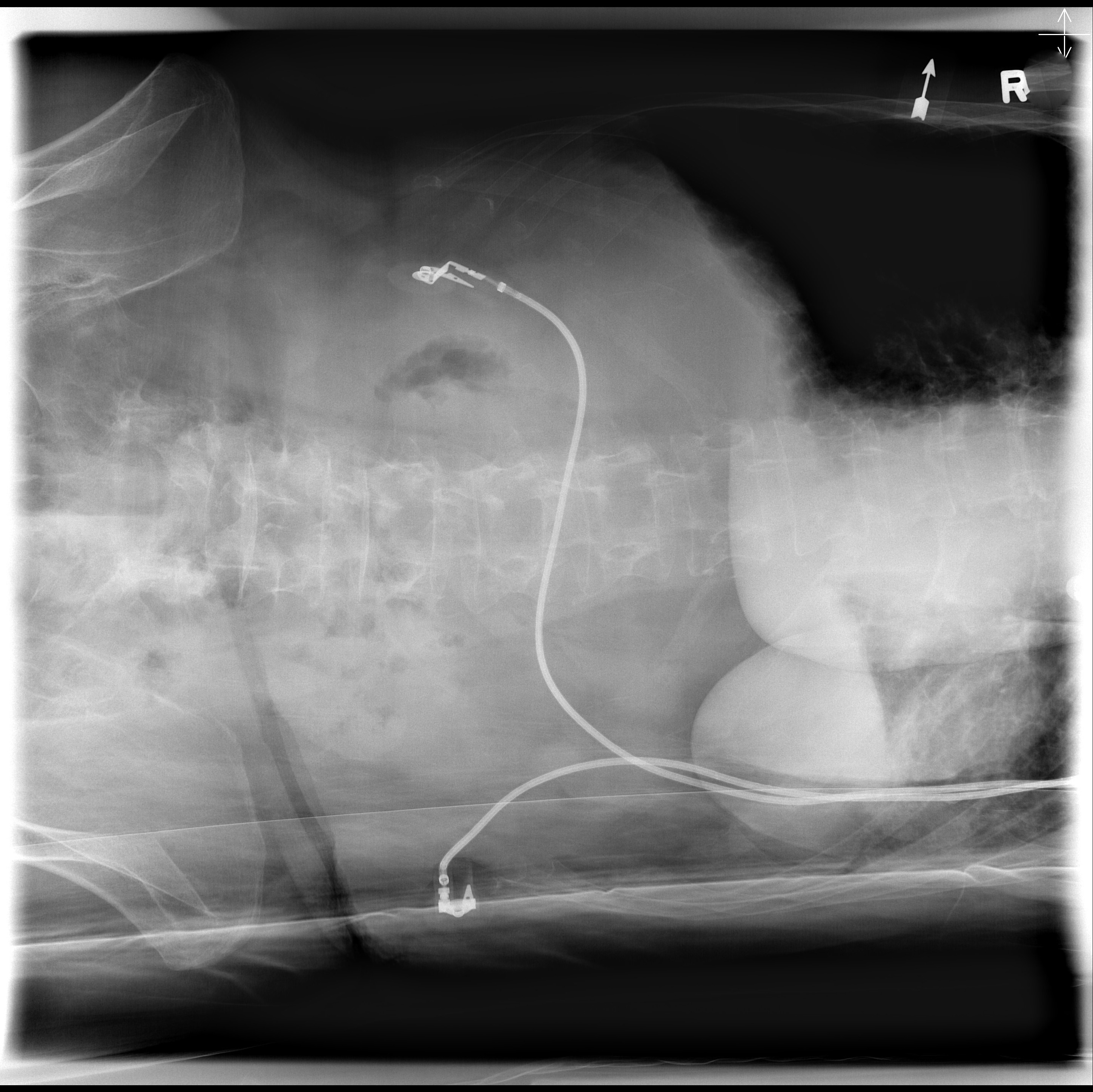
Assess the phase of respiration captured. What is seen radiographically?
Inspiration; domes of the diaphragms above T12
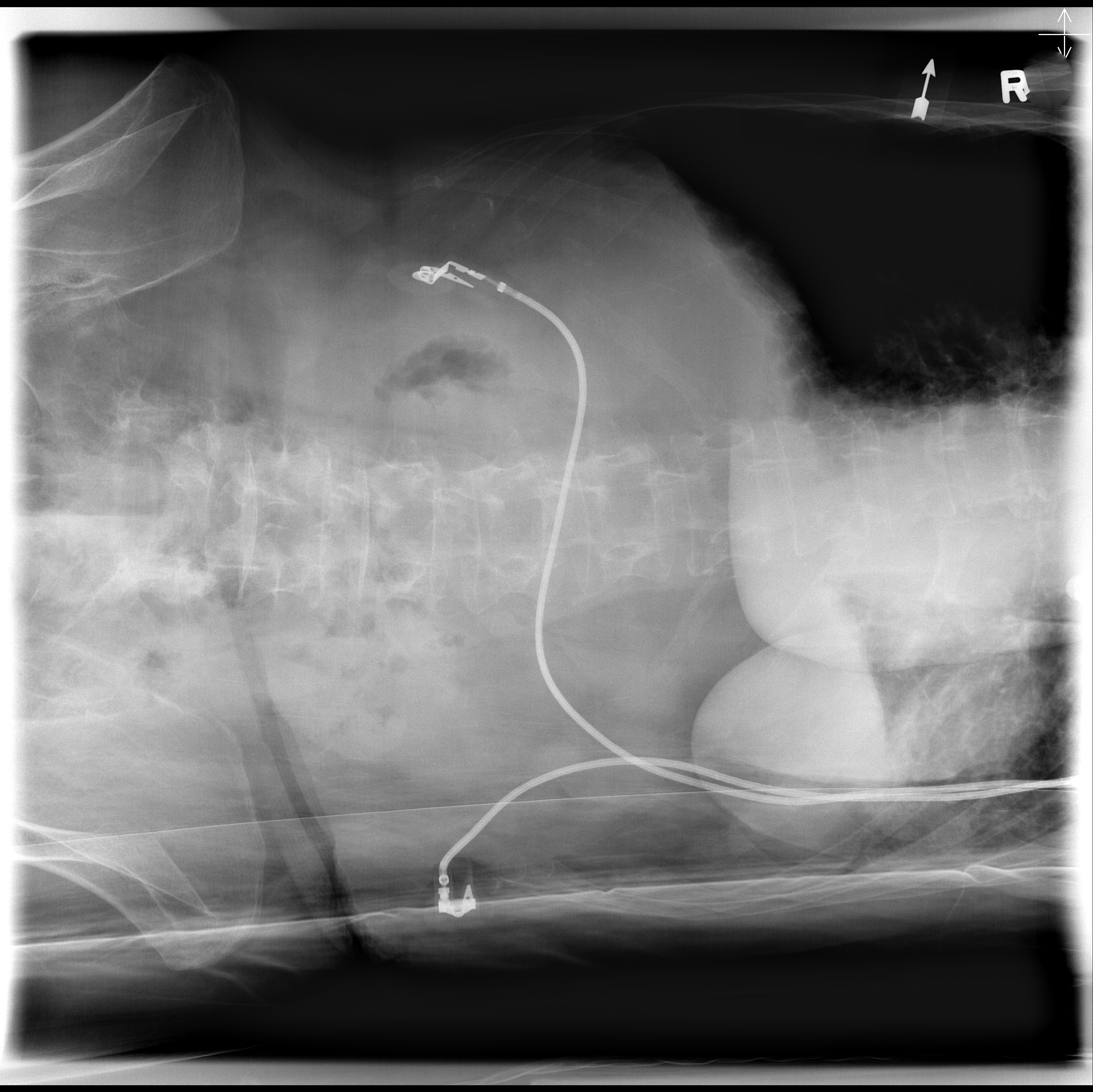
Assess for voluntary/involuntary motion
No voluntary motion (sharp left hemidiaphragm); Possible involuntary motion (bowels near pelvis)
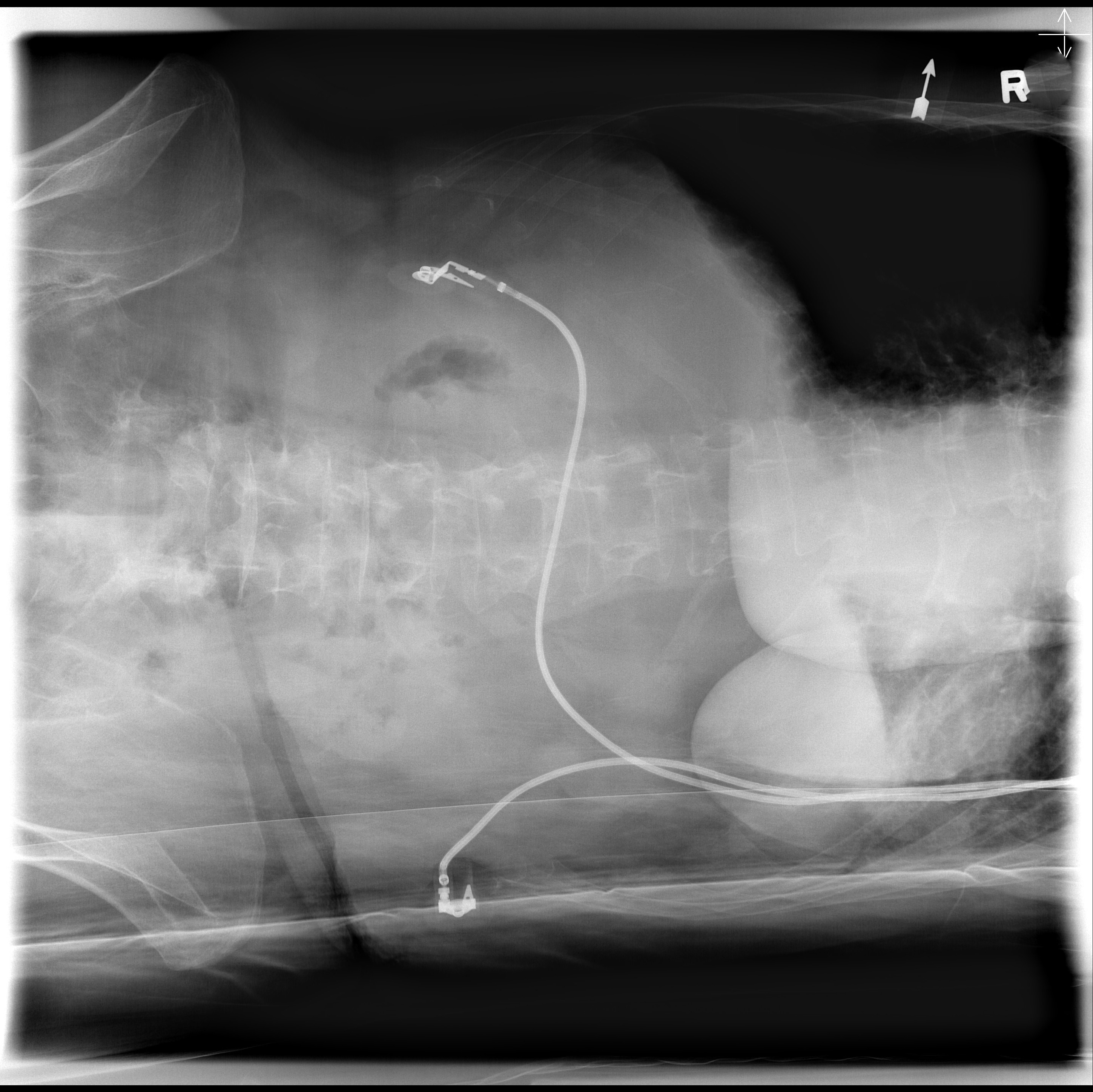
Assess for optimal IQ. What adjustment is needed?
Satisfactory; uniform density and bowel outlines seen. Gas not too dark. Could use a filter and capture on expiration.