Cauda Equina Syndrome
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
• The Cauda Equina is comprised of the “bundle-like” structure of nerve
fibers that extend distally from the terminus of the spinal cord.
• Spinal cord ends between T12-L3 depending on anatomic variations
• Cauda Equina provides motor and sensory innervation to:
-LEs
-Bladder
-Anus
-Perineum
anatomy
(cauda equina)

1.) Herniation of Lower Lumbar Disc-most common
(Often Central Herniation)
2.) Epidural Hematoma
3.) Infections
4.) Neoplasms (Primary & Metastatic)
5.) Trauma
etiology
(cauda equina)

-rare condition
-most common in younger men (18-26)
-Occurs in 3% of all disc herniations
• Prevalence:
- 1 in 30,000-100,000 people/year
epidemiology
(cauda equina)
1. Acute Onset:
2. Gradual Onset:
onset
(2)
Can happen rapidly
• Acute disc herniation
• Trauma
Acute Onset
(cauda equina)
May develop over several months
• Lumbar stenosis
• Neoplasm
Gradual Onset
(cauda equina)
• Severe Low Back Pain (97% of patients)
• Bilateral Lumbar radiculopathy symptoms
-LE weakness and/or paresthesia
-Most often from L5-S1
• Bladder Dysfunction (92% of patients)
-Incontinence vs. Retention
• Bowel Dysfunction (72% of patients)
-Incontinence vs. constipation
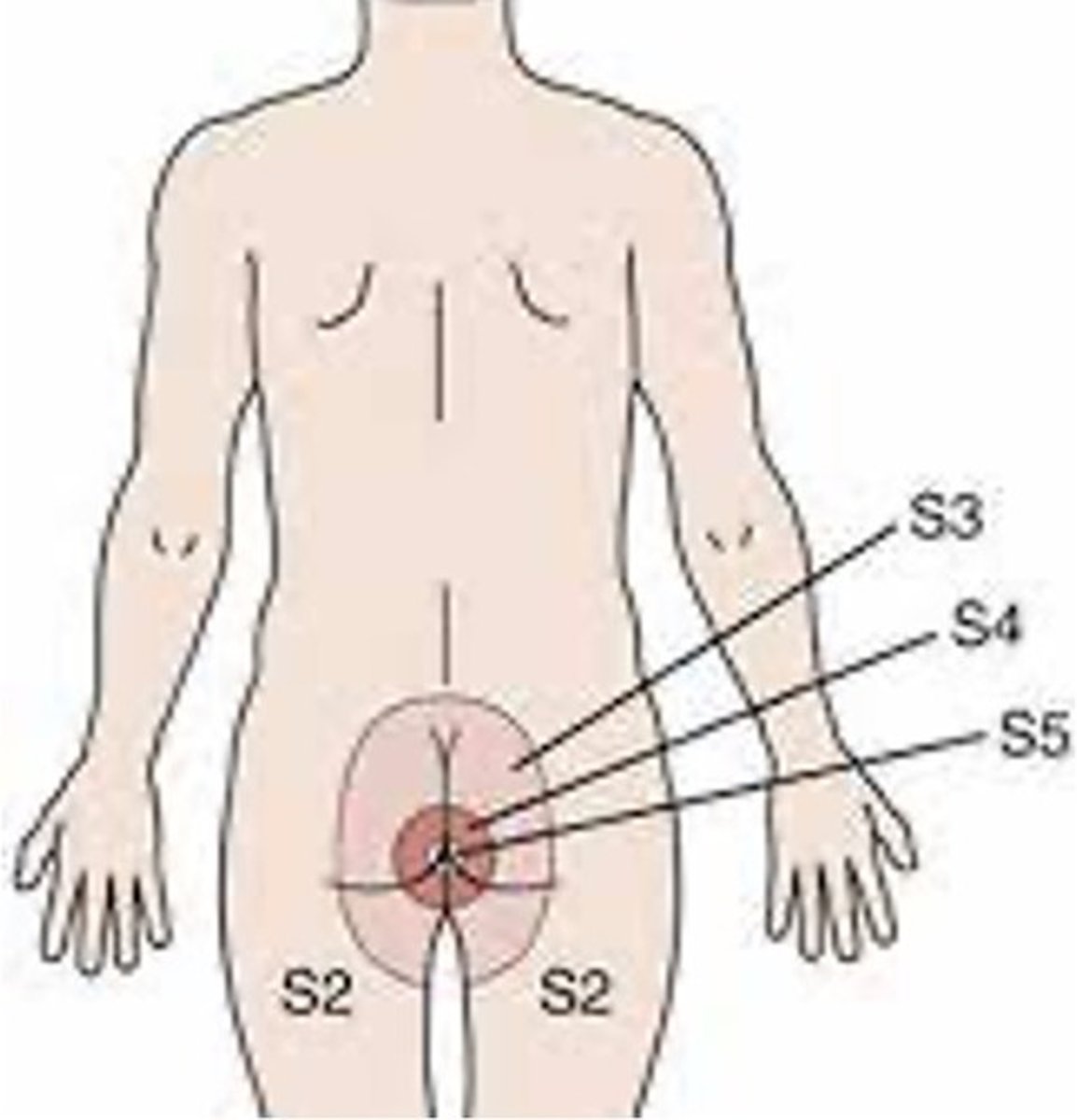
• Saddle Anesthesia or loss of sensation around anus (93% of patients)
• Sexual Dysfunction
*Perineal Anesthesia & Bladder Dysfunction are often the first
symptoms*
Clinical Presentation
(cauda equina)
-Diminished DTR's
-Bilateral LE Weakness
-L3-S1 affected
LMN Symptom Presentation
(MOST common)
-Increased DTR's
-Spasticity
-Babinski, Clonus, can be present
-T12-L3 affected
UMN Symptom Presentation
(less common)
• Patients who present to PT with signs and symptoms consistent with
Cauda Equina need to be referred immediately to the ER for imaging
and likely surgery!
• Timing of medical intervention after onset of symptoms is crucial
• _ is the window to prevent lasting damage?
<48 hours
• Recommended that PT calls physician ahead of patient arriving to ER
to expedite the process
Emergency Referral
(cauda equina)
_ is Gold Standard for Diagnosis
MRI
_ _ is another option if MRI not available
• CT Myelogram
• Most patients undergo immediate decompression surgery
-including laminectomy and possible discectomy at the level involved.
Treatment
(cauda equina)
• If early decompression (<48 hours), prognosis is more favorable
Early Prognosis
(<48 hours)
• If medically treated >48 hours after onset of symptoms, prognosis is
much less favorable and often results in permanent neurological
damage including:
-Self-catherization due to urinary dysfunction
-Colostomy bags due to bowel dysfunction
-Sexual Dysfunction
-Motor and sensory deficits in the LEs
Late Prognosis
(>48 hours)
• Several factors can lead to delay of recognition of treatment:
1.) Patient must recognize symptoms and seek medical care very
quickly
2.) Medical provider must be able to recognize symptoms, diagnose as
CAS, and refer to ER.
3.) ER staff must be able to route patient to provider immediately. Diagnosis must be made immediately.
4.) MRI must be available immediately, and surgeon must be able to
perform emergency surgery.
• If any of these steps are delayed, it can negatively impact the time
before decompression surgery
Medicolegal Considerations
(4)