Looks like no one added any tags here yet for you.
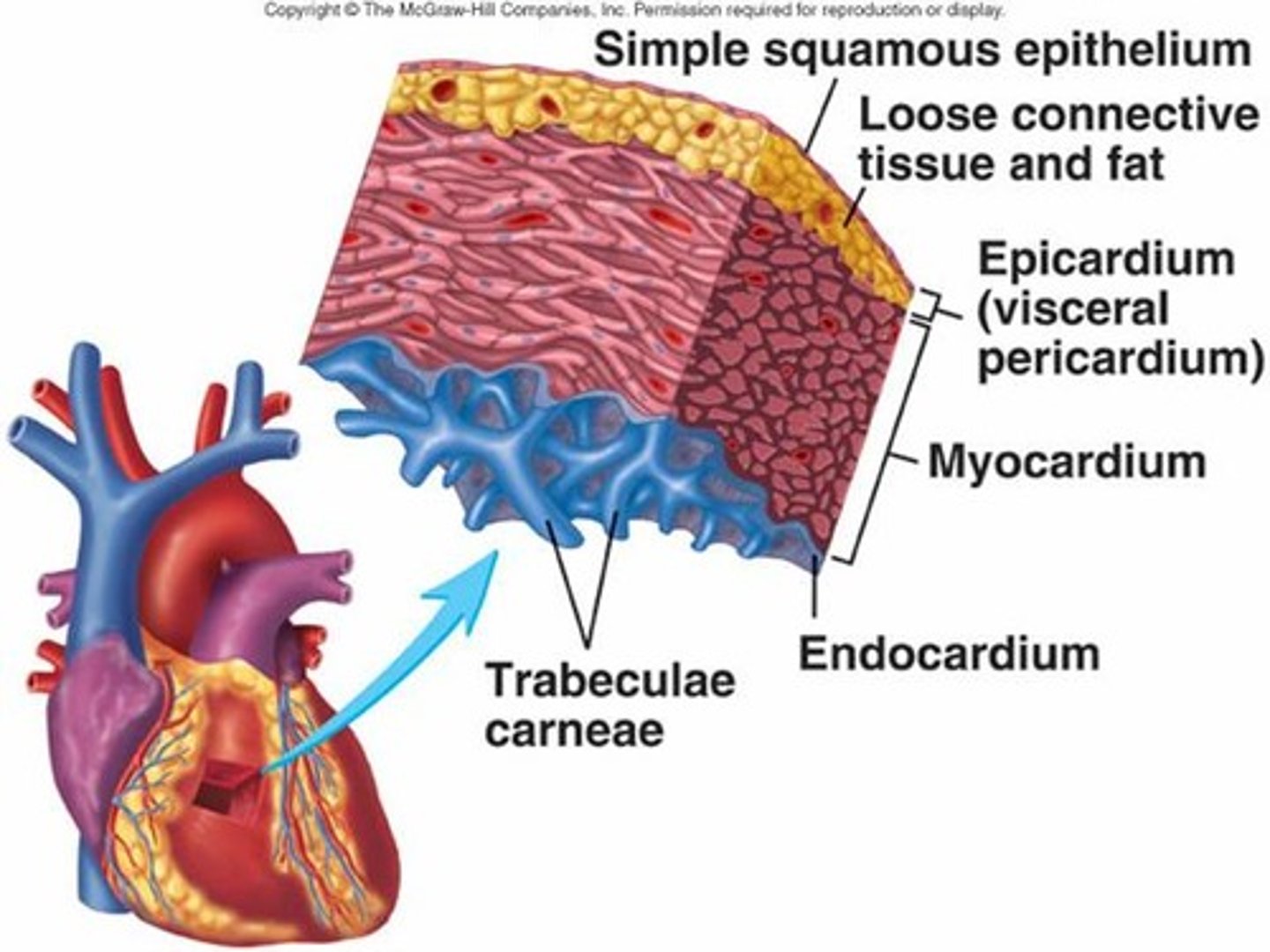
heart wall has 3 layers...
epicardium, myocardium, and endocardium
characteristics of the myocardium
-thickest layer
-cardiomyocytes provide contractile force
-contains coronary arteries & veins
what is the function of the coronary arteries? what happens if occluded?
2 main coronary arteries (RCA and LCA) that supply blood to different areas of the heart ; occlusion of either can cause left ventricular damage
right vs left coronary artery
right
-supplies right atrium & right ventricle, portion of posterior wall of left ventricle, SA & AV nodes & bundle of His
left
-supplies left atrium & left ventricle
what is collateral circulation?
assists in supplying blood & O2 to myocardium that has become ischemic
-formation of collateral arteries can restore circulation following arterial occlusion (CAD)
new collateral vessels are formed through two processes....
-arteriogenesis (new artery growth branching from preexisting arteries)
-angiogenesis (growth of new capillaries within a tissue)
review: progression of atherosclerosis
1. endothelium injury and inflammation
2. cytokines released (amplify inflamm.)
3. cellular proliferation
4. macrophage migration
5. LDL oxidation (trapped LDL engulfed by macrophages + oxidative stress) = foam cell formation
6. fatty streak (many foam cells; forms lesions)
7. fibrous plaque (smooth muscle cells cover streak)
8. complicated plaque (cell death degrades matrix, risk of rupture)
atherosclerosis is a precursor for....?
CAD as it narrows or occludes coronary arteries
dyslipidemia
abnormal concentrations of lipoproteins; can be likned to CAD (indicator of coronary risk)
modifiable risk factors for CAD
-dyslipidemia
-HTN
-cigarette smoking
-excessive alcohol consumption
-diabetes and insulin resistance (hyperglycemia)
-obesity
-diet (atherogenic
-physical inactivity / sedentary lifestyle
nonmodifiable risk factors for CAD
-advanced age
-family history (genetics and shared environmental exposures)
-male gender or female after menopause
nontraditional risk factors for CAD
-markers for inflammation, ischemia, thrombosis → C-reactive protein
-adipokines → adiponectin and leptin
-CKD
-air pollution and ionizing radiation
-medications
-coronary artery calcification, carotid wall thickness
-microbiome
what is CAD?
narrowing of coronary arteries, usually d/t atherosclerotic plaques
-reduces myocardial oxygen supply
-responsible for both angina & myocardial infarction (MI)
CAD is divided into 2 types of disorders....
1. chronic ischemic heart disease
2. acute coronary syndrome (ACS)
what is chronic ischemic heart disease?
narrowing of coronary artery lumen d/t atherosclerosis and/or vasospasm
-episodes of myocardial cell ischemia
-stable plaque → stable angina
what is acute coronary syndrome (ACS)?
disruption of atherosclerotic plaque which obstructs coronary lumen
-unstable plaque → unstable angina (UA)
-MI (NSTEMI, STEMI)
most common complications for ACS
dysrhythmias (v fib), heart failure, sudden cardiac death
stable plaque
produces obstruction of coronary blood flow → myocardial ischemia (stable angina)
-stable angina may progress to unstable angina
unstable plaque
-large lipid-rich core, thin fibrous cap, inflammation, lack of smooth muscle cells
-tend to fissure or rupture
-rupture causes platelet aggregation/adhesion & thrombus formation!!!
-myocardial ischemia leads to ACSs (unstable angina & MI (NSTEMI & STEMI))
oxygen supply depends on....? oxygen demand depends on.....?
-blood flow to myocardium → impacted by coronary artery disease (CAD), atherosclerosis, vasospasm
-oxygenation of blood reaching myocardium → impacted by anemia, respiratory disease
-sympathetic activity, physical activity etc.
3 types of transient myocardial ischemia
1. silent ischemia
2. prinzmetal angina
3. stable angina
what is silent ischemia?
myocardial ischemia that does not cause detectable symptoms
what is prinzmetal angina?
abnormal vasospasm of coronary vessels → unpredictable chest pain
what is stable angina?
chest pain occurring intermittently (recurrent)
-stable plaque
-caused by myocardial ischemia
-predictable frequency, intensity, duration of pain
**may develop into unstable angina
stable angina occurs with.... and is relieved by.....
-over exertion during activity, increasing O2 demand, stress, exposure to cold
- rest and nitrates → blood flow restored and no necrosis of myocardial cells results
what is unstable angina (UA)?
chest pain with worsening pattern and is unpredictable
-pain is not relieved with rest
form of ACS = transient episodes of thrombotic vessel occlusion
-unstable atherosclerotic plaque has ruptured and thrombus can form → may cause prolonged ischemia → myocyte death → MI
UA occurs with...
increasing frequency, during sleep, at rest or with minimum exertion
signs and symptoms of UA
increased dyspnea, diaphoresis, anxiety as angina worsens
evaluation of UA
-serum cardiac biomarkers (troponins, creatine phosphokinase-myocardial bound [CPK-MB])
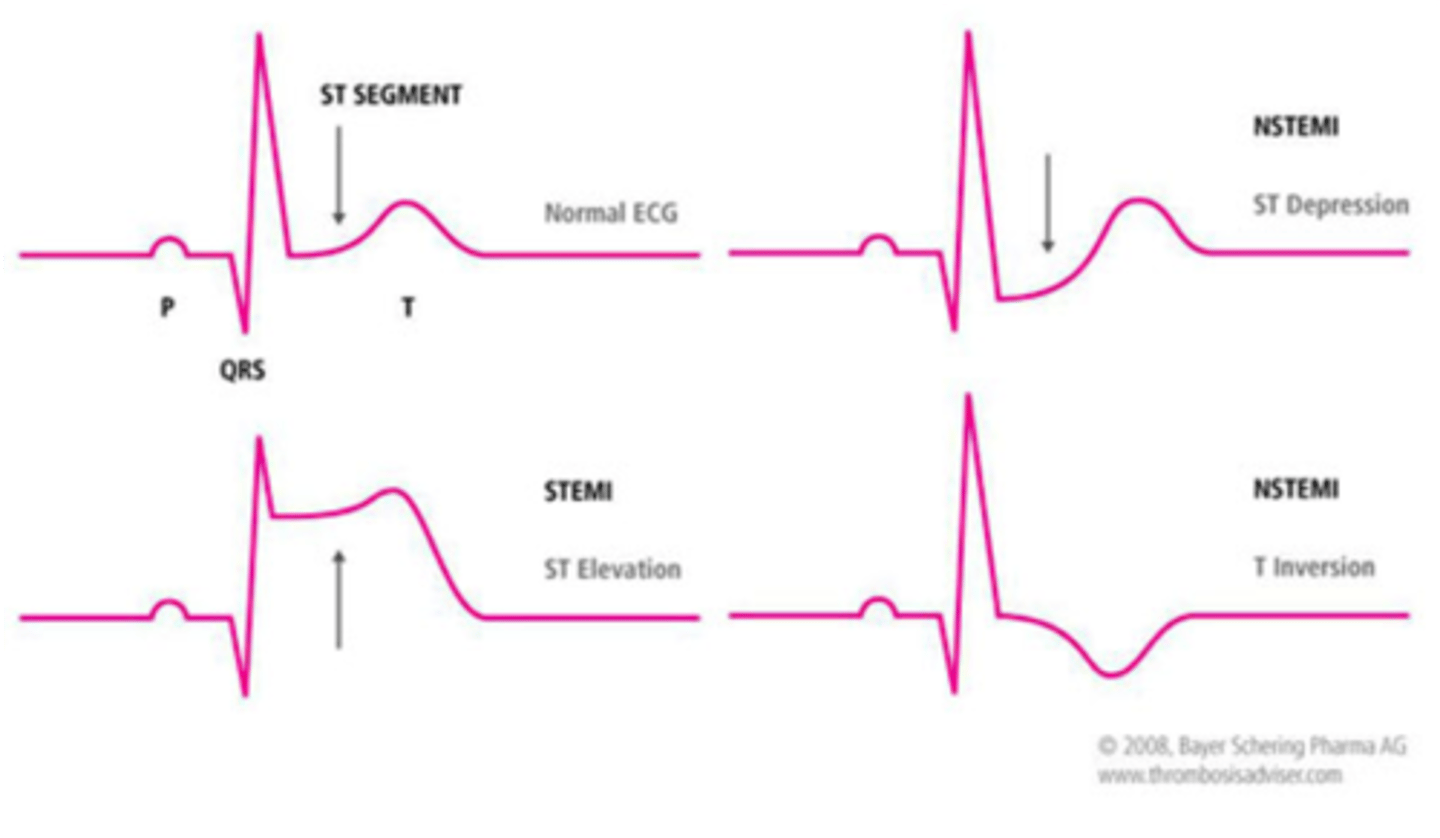
-ECG reveals ST-segment depression and T-wave inversion during pain
treatment of UA
-immediate hospitalization for administration of nitrates, antithrombotics, & anticoagulants
-once stabilized provide beta blockers, ACE inhibitors
-emergency PCI performed if condition does not improve
what is myocardial infarction (MI)?
prolonged ischemia causes irreversible damage to the heart muscle (myocyte necrosis)
-cellular injury, leading to cellular death
list the 2 types of MI
1. subendocardial infarction
2. transmural infarction
subendocardial infarction
-transient thrombosis or incomplete coronary artery occlusion (partial)
-partial wall thickness damage
-ST-segment depression
-called a Non ST-Segment Elevation MI (NSTEMI)
transmural infarction
-more extensive MI associated with prolonged and complete coronary occlusion (total)
-full wall thickness damage
-elevation of ST-segment on ECG
-called a ST-Segment Elevation MI (STEMI)
what causes cellular injury?
-↓ O2 & nutrients
-glycogen stores used up (leads to acidosis)
-acidosis may make myocardium more vulnerable to damaging effect of lysosomal enzymes → HF
-failure of Na+/K+ pump (lose K+, Ca+, Mg+ from cells → loss of contractility → ↓ pumping action)
-angiotensin II (1. vasoconstriction & fluid retention, ↓ contractility, ↑ myocardial work; 2. promotes catecholamine release & causes coronary artery spasm)
-stress (release of catecholamines → imbalances of sympathetic and parasympathetic function, irregular heartbeat & HF)
-NE elevates blood glucose levels, also suppresses beta cell activity which reduces insulin secretion → hyperglycemia
what is cellular death?
after about 20 minutes of myocardial ischemia, irreversible hypoxic injury causes cellular death & tissue necrosis
-necrosis releases intracellular enzymes through damaged cell mem where lymphatics pick up and transport to blood (to be detected by serologic tests)
structural & functional changes associated with myocardial ischemia: myocardial stunning
temporary loss of contractile function that persists for hours to days after perfusion has been restored
structural & functional changes associated with myocardial ischemia: hibernating myocardium
tissue that is persistently ischemic undergoes metabolic adaptation to prolong myocyte survival
structural & functional changes associated with myocardial ischemia: myocardial remodeling
process occurring in myocardium after MI
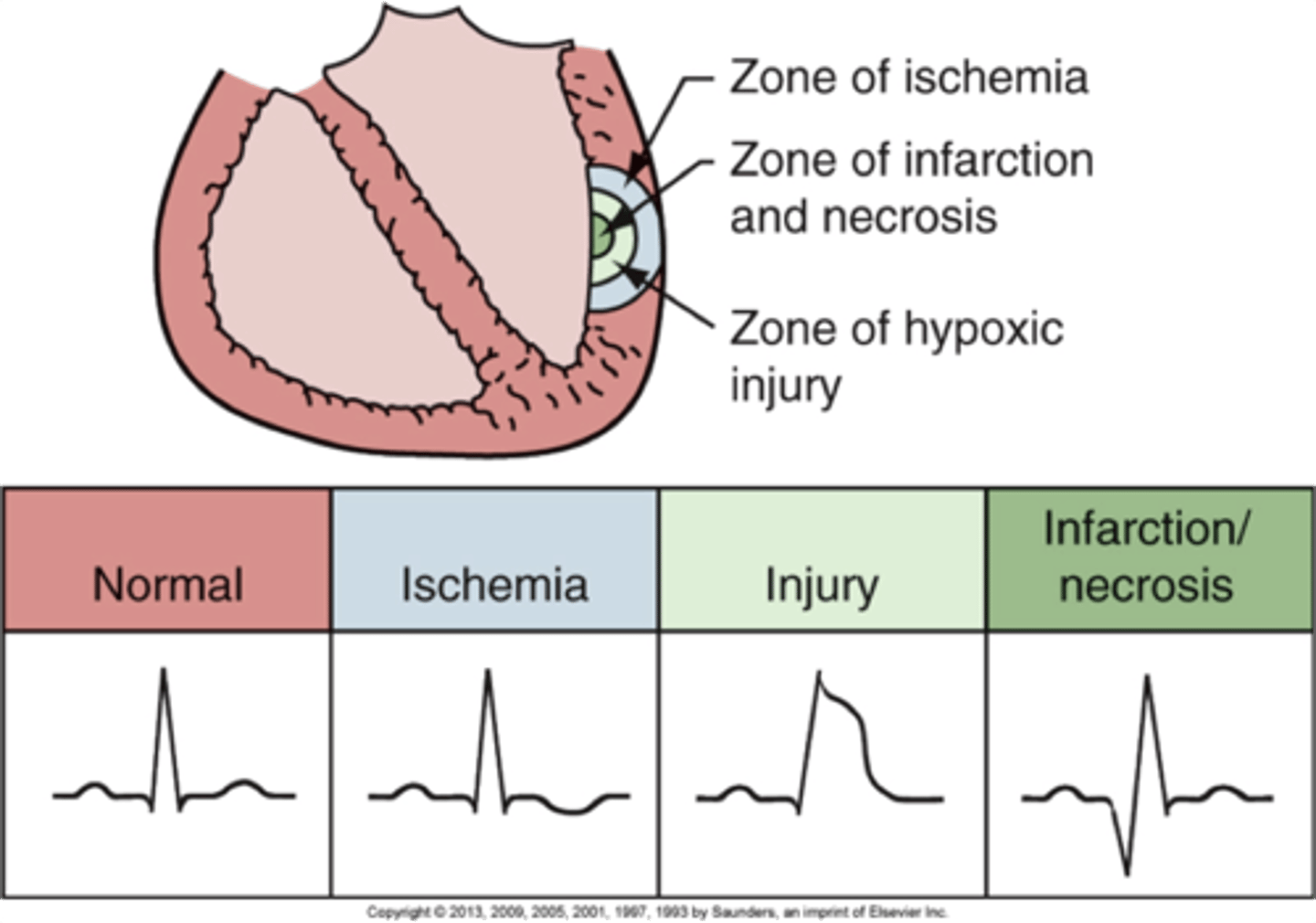
infarcted myocardium is surrounded by a zone of hypoxic injury, which may...
-progress to necrosis
-undergo remodeling (scarring)
-or return to normal
what is reperfusion injury?
reperfusion of ischemic myocardium
-involves release of toxic oxygen free radicals, calcium flux, and pH changes which contribute to cellular death
-also cause damage to the coronary circulation through endothelial injury, platelet activation, inflammation, and vasoconstriction
how does repair of tissue from MI occur in...
-24 hours
-10 to 14 days
-6 weeks
-24 hours: leukocytes infiltrate necrotic area & proteolytic enzymes from scavenger neutrophils degrade necrotic tissue
-10 to 14 days: collagen matrix is deposited & is initially weak, mushy, & vulnerable to reinjury
-6 weeks: necrotic area is completely replaced by scar tissue (strong but unable to contract & relax)
complications of MI
-decreased contractility with abnormal wall motion
-altered left ventricular compliance
-decreased SV
-decreased ejection fraction
-increased left ventricular end-diastolic pressure and volume
-sinoatrial node malfunction (life-threatening dysrhythmias)
-HF
-cardiogenic shock
diganostics for MI: ECG
affected area can be identified on a 12-lead ECG (ST-segment depression (NSTEMI) or ST-segment elevation (STEMI))
ECG changes depend on....
-duration of ischemic event (acute vs evolving MI)
-extent (partial/subendocardial vs entire wall thickness/transmural)
-location
diganostics for MI: serum biomarkers
-cardiac troponin I (cTnI)
-creatine phosphokinase-MB (CPK-MB)
-lactate dehydrogenase (LDH)
-myoglobin
how are biomarkers released into the blood?
cardiac muscle damage → myocardial cells necrose & die → release their contents including enzymes (biomarkers) into blood
cardiac specific serum biomarkers: cardiac troponin I (cTnI)
have high specificity for myocardial tissue
-primary biomarker for dx of MI
-rise within 2-4 hours after onset of symptoms
when would you see elevated cTnI? UA or NSTEMI?
NSTEMI !! bc myocardial injury has occurred (which causes the release) whereas UA does not have myocardial injury
but still, UA and NSTEMI both occur d/t myocardial ischemia; one gets damaged, the other doesn't
**injury = released biomarkers
cardiac specific serum biomarkers: creatine phosphokinase-MB (CPK-MB)
released by myocardial cells but is also in other muscle cells
-used as 2nd-line biomarker d/t ↓ sensitivity and ↓ specificity
-levels exceed normal ranges within 4-8 hours of injury
non-cardiac specific serum biomarkers: lactate dehydrogenase (LDH)
LDH is an enzyme found in almost all body tissues including heart
non-cardiac specific serum biomarkers: myoglobin
present in cardiac and skeletal muscle
-released into circulation with any damage to muscle tissue including myocardial necrosis
-released quickly from infarcted myocardial tissue
-elevated within 1 hour after myocardial cell death
-peak levels reached within 4-8 hours
additional labs for MI
-leukocytosis
-elevated CRP
-hyperglycemia
symptoms / assessment for MI
-sudden, severe chest pain (heavy/crushing; radiates to neck, jaw, back shoulder, left arm; pain severe and prolonged; NOT relieved by nitroglycerin or rest)
-sensation of indigestion
-N&V
-tachycardia
-HTN
-hypotension with severe myocardial damage
-skin is cool and clammy
-atypical symptoms → silent MI (different symptoms or no symptoms)
treatments for MI
-hospitalization
-immediate administration of supplemental O2 and aspirin (or clopidogrel)
-morphine
-bed rest
-NSTEMI → same as UA, including antithrombotics, anticoagulation or PCI, or both
-STEMI → best managed with emergency PCI & antithrombotics
-hyperglycemia treated with insulin
-stool softeners
-once stabilized, further management includes ACE inhibitors, beta-blockers, and statins
non-pharmacological treatment for ACS
-percutaneous coronary intervention (PCI)
-coronary artery bypass graft (CABG)
-minimally invasive direct coronary artery bypass (MIDCAB)
-gene & stem therapy for myocardial angiogenesis and spinal cord stimulation
nursing implications for practice with thrombolytic therapy
-careful monitoring of the client's condition and providing education
-assess for conditions that would be contraindicated (recent trauma or surgery/biopsy, GI bleeding, postpartum, cerebral hemorrhage, bleeding disorders, thrombocytopenia)
-in septic thrombophlebitis, favourable clot is in place that would be dissolved, which is contraindicated
-used with caution in any condition where bleeding could be a significant hazard, such as severe renal or liver disease