Vestibular System
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
[OVERVIEW] of Vestibular System:
Function
Sensors
innervation
Efferent?
Overview
Function:
Detects position + motion of the head
Sensors:
Saccule + Utricle (Otolith Organs)
Detect linear acceleration and head position relative to gravity
Semicircular Canals:
Detect angular acceleration
Innervation:
by neurons in vestibular (Scarpa's) ganqlion
Central Processes → CNVIII (vestibular component)
Efferent from vestibular complex:
Oculomotor Control System
Cerebellum
Spinal cord
Describe the anatomy of the vestibular system
Location
Blood Supply
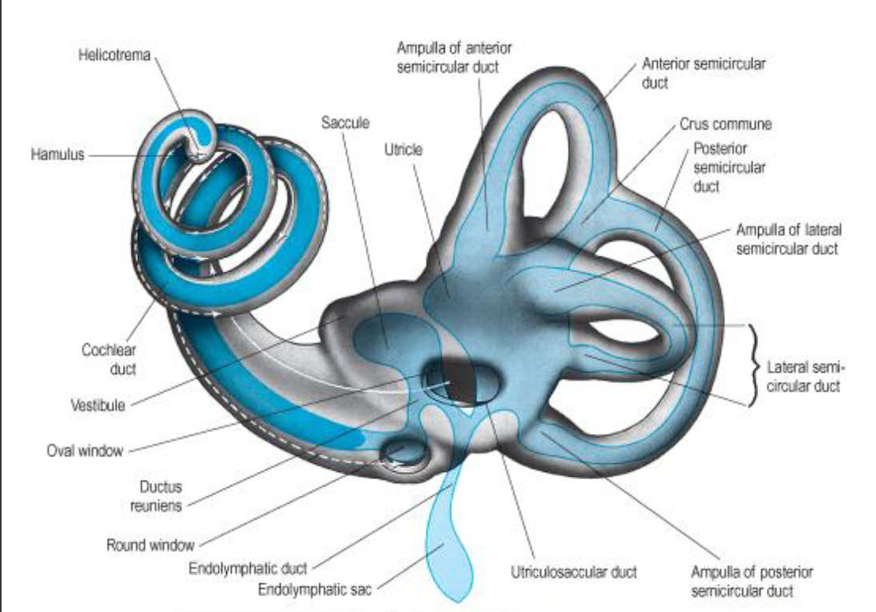
Components of
Outer bony labyrinth
Inner membranous Labyrinth
Location: petrous portion of temporal bone
Blood Supply:
Labyrinthine Artery (from basilar or AICA)
divides into cochlear and Vestibular Branches
Outer bony labyrinth:
vestibule
oval window
semicircular canals
ampullae
cochlea
Inner membranous
Inner Membranous labyrinth
utricle & saccule
semicircular ducts
cochlear duct
endolymphatic sac and duct
utriculosaccular duct
ductus reuniens

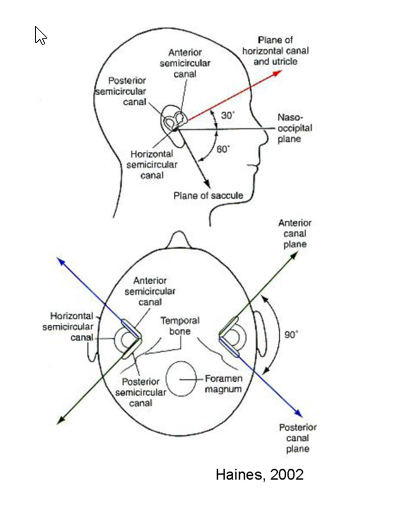
Describe the degrees of the various planes
Plane of horizontal (lateral) canal and utricle
30 degrees from nasooccipital plane
planes of anterior canal and posterior canal
90 degrees apart
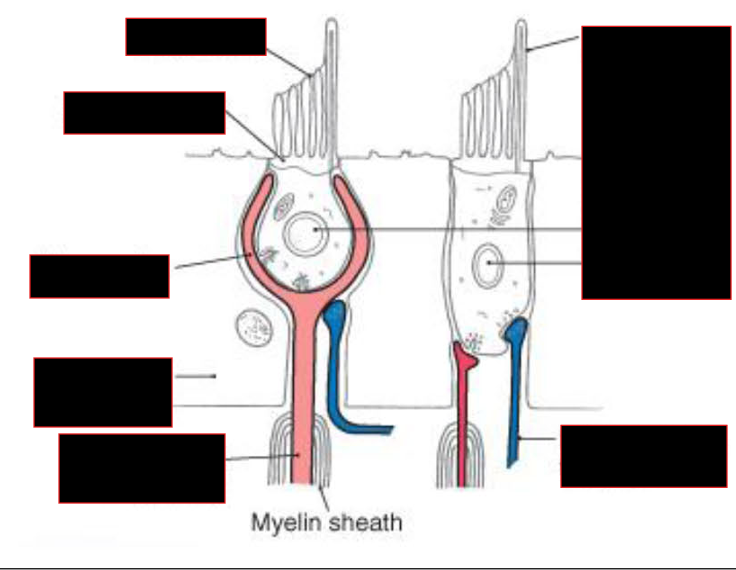
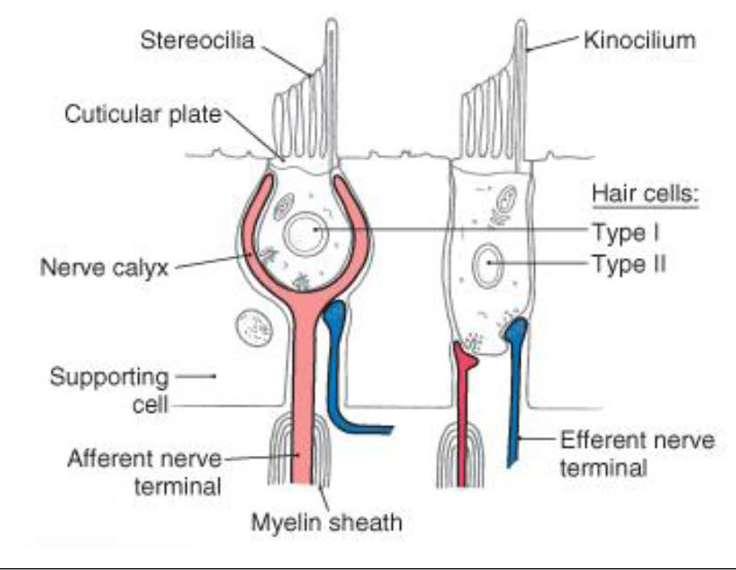
Describe the Hair Cells
Stereocillia vs Kinocillum
Supporting Cell
NTs
Efferent Nerves
Origin
Function
Hair Cells:
Stereocillia vs Kinocilium
Stereocilia: 60-100 hairs project from each cell
progressively increasing in length
Longest cilium = Kinocilium
arises from Centriole
Function: Strain gauges; tranduces mech. stimulis
Supporting Cell: Microvilli
NTs:
Glutamate/Aspartate: Excitatory
Efferent Nerves:
Origin: Reticular Formation
Function:
Releases AcH and CGRP → modulate activity of hair cell or vestibular afferent.
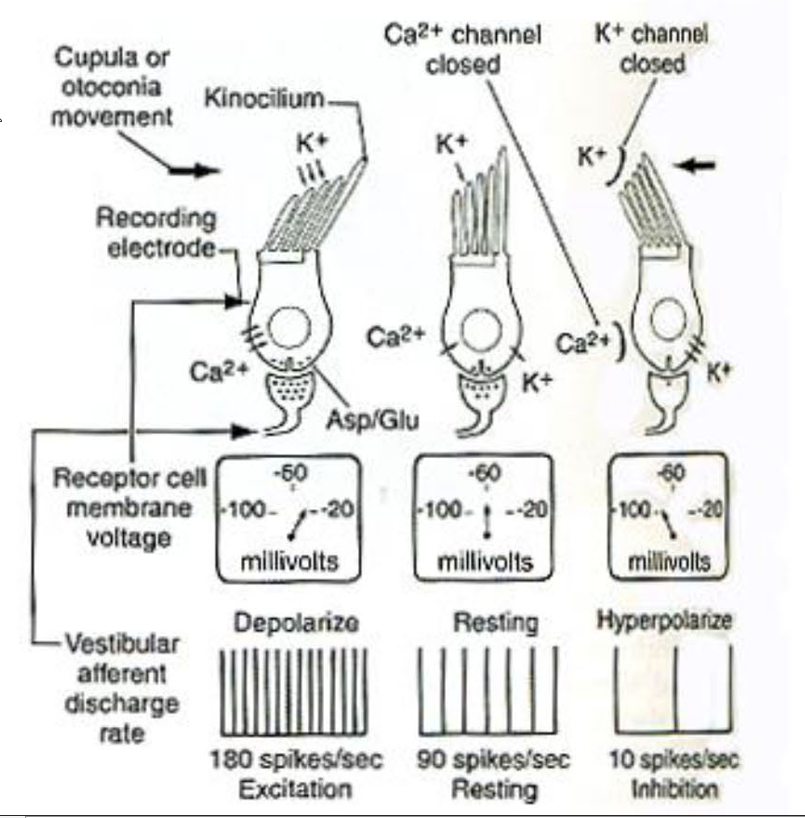
Describe the mechanism for transduction of these hair cells
Transduction:
Sterocilli bends towards kinocilium → Depolarization:
Stereocilia contain K+ channels that open via tip links
K+ rushes in from endolymph
Stereocilia bend away from kinocilium → hyperpolarizes
Describe the Static labyrinth
Composition
Describe the Otolithic Membrane:
What is it?
Function
Describe the Orientation of Macula/Function
Orientation?
Location?
Relation to Striola
Function
Static Labyrinth
Composition:
Utricle and Saccule
Each has Macula: small patch of hair cells
Otolithic Membrane:
What is it?
stereocilia/kinocilia of macula = embedded in membrane containing small calcium carbonate crystals
Function:
creates pull on stereocilia in the direction of gravity
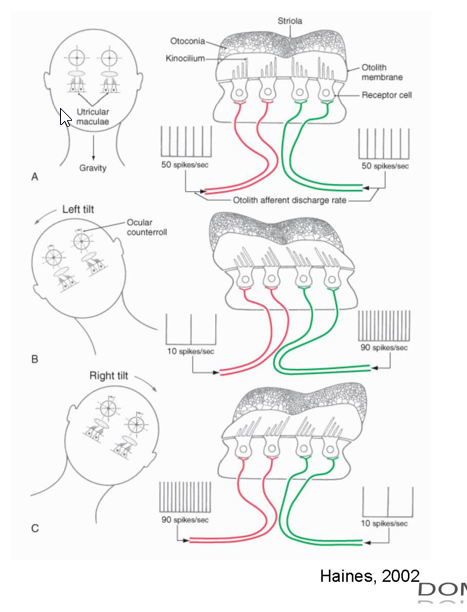
Orientation of Macula/Function:
Utricle Macula: horizontally oriented
Parallel w/ base of the skull
kinocilia faces striola
Saccule Macula: vertically oriented
located on the medial wall
kinocilia face away from striola
Function:
detect static head position relative to gravity and linear acceleration
NOTE: Columnar supporting cells of the maculae are continuous with the cuboidal epithelium lining the utricle and saccule
Describe how the static labyrinth provide Information about head position and linear acceleration
Describe the Kinetic Labyrinth
Content
Function
Kinetic Labyrinth
Content:
Semicircular canals
Crista:
saddle-shaped ridge containing hair cells (3 pathches)
Found in Ampulla of each canal
Function:
Movement of endolymph relative to cristae → detection of angular acceleration/deceleration in all 3 planes
Describe the Mechanism in which the Kinetic labyrinth encodes angular acceleration
Cupula
What is it? Direction of movement in relation to head
Cillia
Horizontal vs A/P Canal:
Kinocilium location
Depolarization event?
Movement/Endolymph
Mech:
Cupula
gelatinous accessory structure attached to epithelial lining.
Hair cells embedded here
Cupula pushed in direction opposite head movement → deflection of cilia.
Cillia;
oriented to respond to movement of endolymph in relations to Utricle
Horizontal Canal:
kinocilium on side of utricle
Depolarization: Endolymph flow towards utricle
A/P Canals:
kinocilium on side away from utricle
Depolarization: Endolymph flow away from utricle
Both hyperpolarized when endolymph flows in the opposite direction mentioned above
Movement and Endolymph:
NOTE: endolymph moves in oppposite direction of head due to inertia
NOTE: for A/P canals; towards utricle of one canal = away from the other canal;
EX: Looking up = Lymph moves Inferior/Anteriorly → Endolymph flows towards the Anterior canal; Endolymph flows away from Posterior canal → Excitation of Posterior/ Inhibition of Anteriorly
NOTE:
anterior and posterior canals are sensitive in the same fashion to roll and pitch movements.
Describe the Vestibular Nerve
Aka?
Location?
Nt?
Ganglia:
vestibular Ganglion = Scarpa’s
Location:
lateral end of the internal acoustic meatus
NT: Glutamate
Describe the Vestibular Nuclear Complex:
Location?
4 main nucleus?
Fate of Ascending vs Descending vestibular Nerve Fibers as it enters?
What about Kinetic vs Static Fibers
Describe the function of commissural connections
Vestibular Nuclear Complex
Location:
dorsally in pons and medulla
btw lateral part of 4th ventricle + inferior cerebellar peduncle
4 Main Nucleus
Lateral (Dieter) vestibular nucleus
Medial (Schwalbe) vestibular nucleus
Superior (Bechterew) vestibular nucleus
Inferior (descending or spinal) vestibular nucleus
Ascending vs Descending Fibers of vestibular nerve:
upon entering vestibular complex:
Ascending: → Superior Nucleus
NOTE: some goes to flocculonodular lobe of cerebellum (vestibulocerebellum)
Descending: → Medial + Inferior Nucleus
NOTE: Lateral nucleus: limited input from kinetic but some from static labvrinth
Kinetic vs Static Labyrinth Fibers:
Kinetic: → superior + medial nuclei
Static: → medial + inferior
commissural connections (vestibulovestibular)
Function:
comparison of information between sides
important for vestibular compensation
Definition: recovery of postural reflexes after unilateral vestibular receptor loss due to trauma or disease
What does the Vestibular Nuclei receive INPUT from:
Cerebellum
SC
Oculomotor System
Describe the Nuclei Output:
Main
Minor
INPUT:
Cerebellum
Flocculonodular lobe: → superior, medial, inferior
Lateral vermis: → lateral
Fastigial (deep cerebellar) nucleus: → lateral and inferior
Spinal cord
from spinovestibular tract
Proprioceptive information
processed information from reticular formation
Oculomotor system
accessory optic system
Output:
Main: → cerebellum (ie., vestibulocerebellum), spinal cord, and oculomotor system
Minor: parietal and insular cortex via thalamus
Describe the Output Systems of the Vestibular Nuclei
Function?
Compare and Contrast Medial/Lateral Vestibulospinal Tracts
Origins/Route
Travels
Innervation
Related to
Function
Describe the Vestibulo-ocular System
Function
Functional Output System:
Function:
Connections w/ cerebellum →
fine control over postural adjustments
eye movernents
Via vestibulospinal + vestibulo-ocular systems
Medial/Lateral Vestibulospinal Tract
Medial:
Origins:
Medially(mostly) + Inferior Nucleus
Bilaterally
Travels:
in MLF (descending component) → Cervical Spine
Innervation:
medial group (axial) of motorneurons in ventral horn
Related to:
flocculonodular lobe
Function:
integration of head and eye movements associated with changes in body position
Lateral:
Origin:
Lateral Nucleus
uncrossed
Travels
Full length of SC
Innervation:
motorneurons medial(majority) and lateral groups in the ventral horn
Related to:
vermis of the cerebellum
Function:
Facilitates (axial extensor musculature)
maintain upright posture and balance
Adjusts trunk position + orientation in response from static + dynamic labyrinths
(balance)
Vestibulo-ocular System
Function:
Provides for maintenance of fixed gaze with on-going head and body movements
Semicircular canal stimulation → conjugate eye movernents in the plane as the canal
EX: (e.g., horizontal canal — horizontal conjugate eye movements)
Describe the Vestibulo-ocular reflex
Components of Reflex Arc
Pathway
X→X
Ipsi vs Contra
Most projections from?
Function/Example
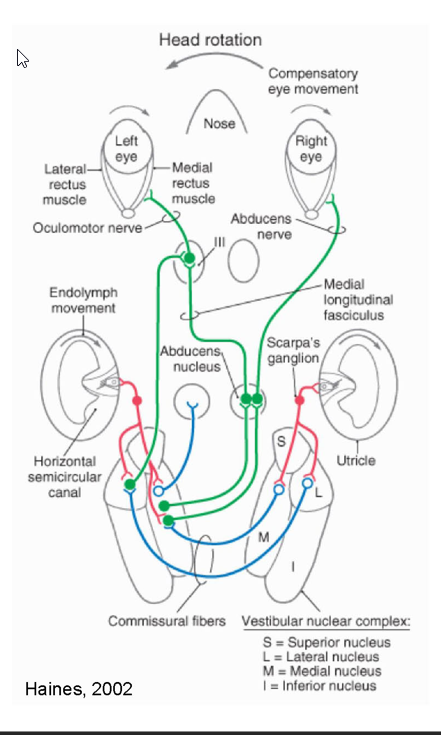
Vestibulo-ocular reflex
3 neuron reflex arc:
primary afferent neuron
vestibular nuclear neuron
oculomotor motorneuron (Ill, IV, and VI)
Pathway:
vestibular nuclear neuron → Oculomotor Nuclei via MLF
Ipsilaterally: Inhibits
Contralterally: Excites
Most projections from Superior + medial nucleus
Lateral → Oculomotor via ascending tract of Dieters
Function:
Co-operate functionally and link pairs of eye muscles
Example:
horizontal semicircular canal input →
excites contra (LR) + Ipsilateral medial rectus (MR);
inhibits ipsi LR + contra MR
Draw out the Vestibulo-ocular reflex
Describe the Thalamocortical System
Function
Pathway
Thalamocortical System
Function:
Allows conscious perception of motion and spatial orientation
Via Combination of info from vestibular, visual and somatosensory systems
Pathway
medial, superior, and inferior nuclei → VP + intralaminar nuclei of the thalamus (BiLat) →
→ somatosensory cortex (BA 3a, 2v)
→ somatosensory association cortex (BA 7)
→ parieto-insular vestibuar cortex
(posterior insula extending into parietal operculum).
Describe Caloric testing
Function
Methodology
Result
Describe Nystagmus
Classifeid based on?
what is COWS
Clinical
What happens in comatose patients
What is the doll’s eye Phenomenon
Caloric Testing
Function: evaluate vestibular pathway
Methodology:
Lateral Semicircular canal= in vertical plane
convection currents induced by irrigating external acoustic meatus w/ warm or cold water
Result:
Warm:
conjugate gaze → opposite side (slow phase)
Then → eyes rapidly reposition to central position (fast phase)
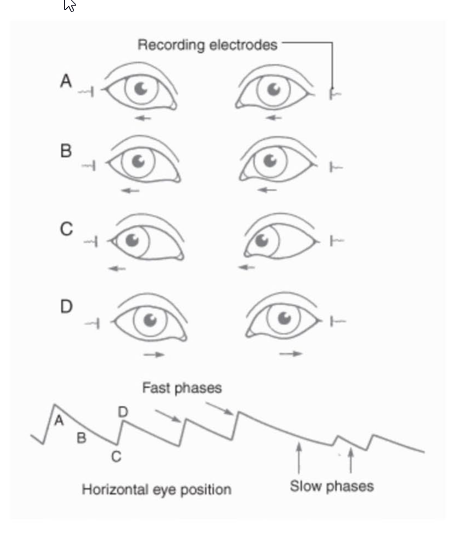
This is called Nystagmus
Cold: Vice Versa
Nystagmus:
Classified based on direction of the fast return phase
COWS
Cold water → Nystagmus to Opposite side
Warm water → Nystagmus to Same side
Clinical Applications:
Comotose Patients:
fast phase (driven by the cortex) is absent
Doll's Eye Phenomenon:
When you turn your head, your eyes should go in opposite direction
If negative:
brainstem = damaged; eyes don’t move
Draw out the the fast/slow phase
What are the clinical signs that the vestibular system is damaged
Clinical manifestations of damage:
V— vertigo — sensation or hallucination of rotation
A — Ataxia —truncal ataxia where body position is difficult to maintain
N— Nystagmus
N— Nausea and Vomiting
(other autonomic signs may include palor and sweating)
NOTE: Signs associated with pathology of both peripheral and central connections.