Introduction & Epidemiology
1/23
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
24 Terms
dental caries
-localized, chemical destruction of tooth structure as a result of metabolic activities in the microbial deposits (dental biofilm) covering the tooth surface at any given site (enamel/dentin/cementum)
-lesions emerge when there is an imbalance in the physiological equilibrium between the tooth mineral and the biofilm fluid
-carious lesions represent the s/s of multiple de- and remineralization processes accrued over time
dental biofilm (plaque)
-complex microbial community on the tooth surface
-caries develop at specific sites where biofilm accumulates
-great variability in biofilm characteristics such as composition and functionality seen throughout biofilm maturation, between biofilm sites, and between individuals
-biofilm formation on tooth surface is prerequisite for caries- necessary, not sufficient for clinically visible caries lesions
metabolic events in biofilm
-very active
-consistently metabolizing saliva proteins and other energy sources to grow and evolve
-acid produced as a metabolic by-product resulting in minute fluctuations in the biofilm fluid pH (normal process)
-metabolic activity can greatly increase when an energy source is introduced & can result in dramatic fluctuations in biofilm and fluid pH
-any factor that influences the metabolic process (diet, biofilm composition and structure, salivary secretion rate, saliva composition, fluoride availability) will contribute to balance between net loss or gain of mineral (and the rate)
demineralization and remineralization
-driving force for ion exchange = degree of saturation of mineral in surrounding solution
-any shift in biofilm pH will influence the chemical composition of the biofilm fluid and the relative degree of saturation of fluid with respect to tooth mineral
-from time of eruption, tooth will be subject to chemical modifications on innumerable occasions
-modifications are mostly very subtle
-tooth surface is in a state of dynamic equilibrium with the surrounding oral fluid (saliva and biofilm fluid)- most sequences of metabolic events “cancel each other out”
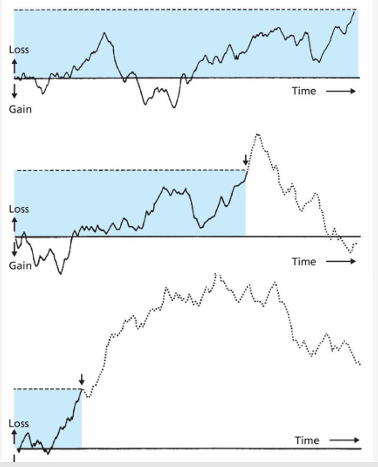
carious lesion scale
-initial loss of mineral at a nano-level to total tooth destruction
-demineralization progresses very slowly in most individuals
-demineralization is kept active when there is a disturbance in the physiological equilibrium in the biofilm covering the affected site
-anything that influences the equilibrium will influence the development and progression of caries
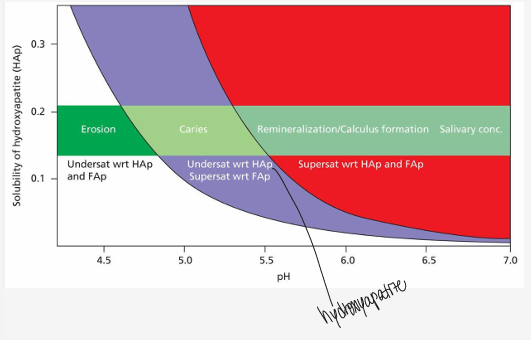
caries continuum
-net mineral loss or gain
-dental caries develops along a spectrum of changes in tooth mineral over time
-caries: progressive, dynamic disease rather than a single event or a binary condition (healthy v. decayed)
-can be controlled
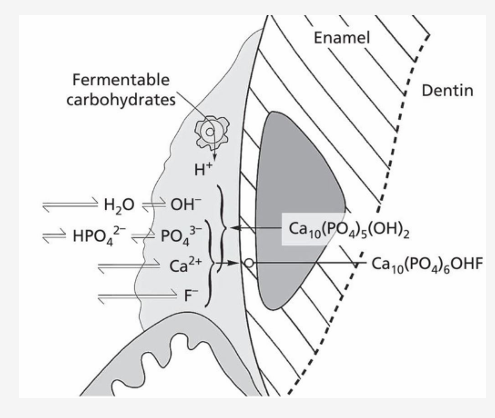
lesion formation
-when the pH falls below a certain level (critical pH), dissolution of hydroxyapatite = demineralization
-due to differences in stability, fluoridated apatite is simultaneously formed in the partially dissolved surface layers of enamel
-carious lesion can form under these conditions
ions in biofilm
-contribute to rough texture
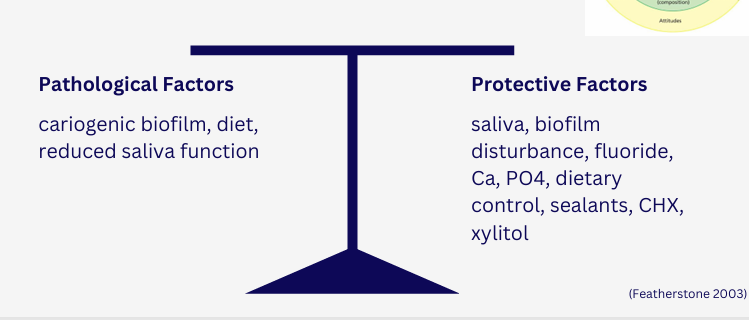
caries balance model
epidemiology
-requires that diseases (and other factors) be measured quantitatively
-measures must be standardized and objective
caries measurement- DMF
-graduated, numerical scale used to measure specific entities
-used as an indicator, not an absolute measure
measurement- DMF score
-can do by surfaces or by teeth
-permanent teeth: DMFS/T (decayed, missing, filled, surfaces, teeth)
-primary teeth: def (decayed, indicated extraction, filled)
DMF index- limitations/inconsistencies
-decayed: what do we classify as decay?
-missing: was tooth lost to caries? or perio/ortho/cosmetics?
-filled: why was tooth filled or not filled?, aesthetic direct/indirect restorations, fissure sealants
the “caries decline”
-fluoride exposure: community water fluoridation (starting in the 1940s, expanding rapidly in the 50s and 60s), widespread fluoride toothpaste use by the 1960s-70s
-improved oral hygiene practices: increased awareness of oral health
-preventive public health programs: school-based fluoride programs, dental sealants (research in 60s, in 80s widespread use)
-prevalence measurement overestimated decline- non-cavitated lesions, life-long disease, shift in age distribution
“caries decline” consequences
-reduced emphasis on cariology in dental curricula and research funding- direct result of perception that caries was a vanquished disease, closure of dental schools
-underestimation of early and active disease
-delayed recognition of ECCs and root caries among certain populations- distribution
“caries decline” trends
-low decayed and missing components
-most of disease is made up of filled components
-although the total number of new carious lesions dropped, the characteristics of new lesions changed with the proportion made up of pit and fissure lesions growing
-has implications for preventive modalities
“caries decline” misconception
-misconception that caries was a disease of the past
-in the US, caries still ranks among the most common chronic diseases of childhood with approximately 1 in 4 preschool children experiencing dental caries in their primary dentition
-among US older adults aged 65+, DMFT is >95%
polarization of dental caries
-late 20th century to 21st century: stabilization of dental caries in many high-income countries
-concentrated in high-risk individuals and underserved populations
-persistent or even increasing caries burden in many areas
-national preventive dentistry demonstration project (NPDDP): despite an overall decline in caries, there is a significant minority of children with severe caries (DMFS of 7+)
-NIDR: “50% of the disease is found in 12% of children”- led to concept of targeting preventive services, increase in prediction research
risk factors
-specific behavior, exposure, biological characteristic, or social condition that is associated with a health condition- exposure to a risk factor increases the probability of a given outcome
-assess individual caries risk
-guide caries control decisions (preventive and therapeutic)
-tailor individualized caries management plans
determinants of health
-broader, interconnected biological, environmental, commercial, or social factors which determine health
-can be positive or negative
-health status influenced by these determinants
-determine who is more likely to be exposed to risk factors
-tailor caries management plans
-explain caries disparities and polarization
-upstream opportunities to promote a state of health
caries risk factors and determinants
-age
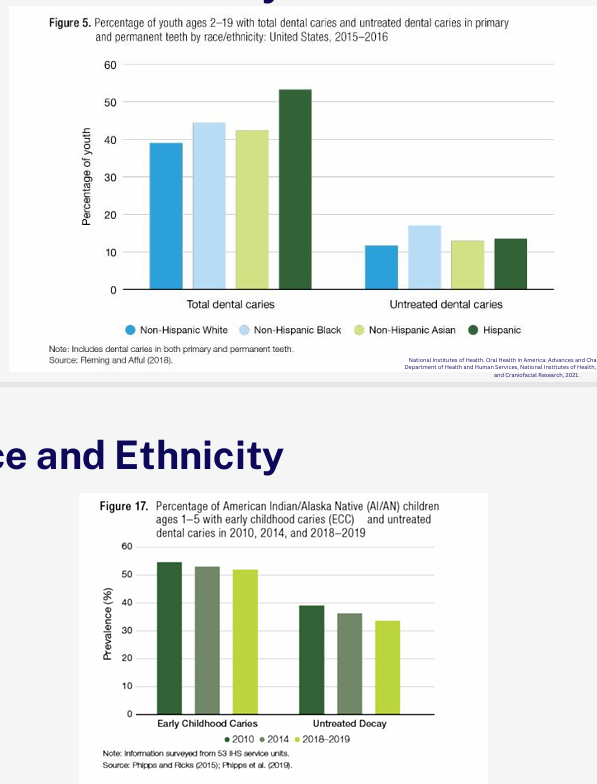
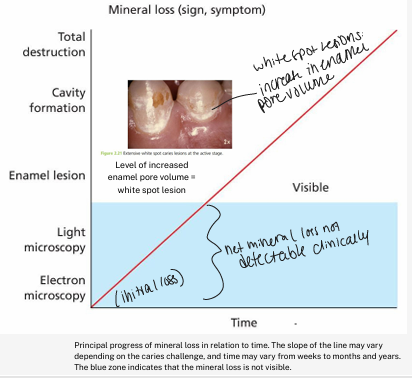
-race and ethnicity
-SES
-diet and nutrition
age
-caries once considered a disease of childhood
-evident that adults are susceptible
-more children are reaching adulthood with intact surfaces, and the caries “attach” is spread over a lifetime
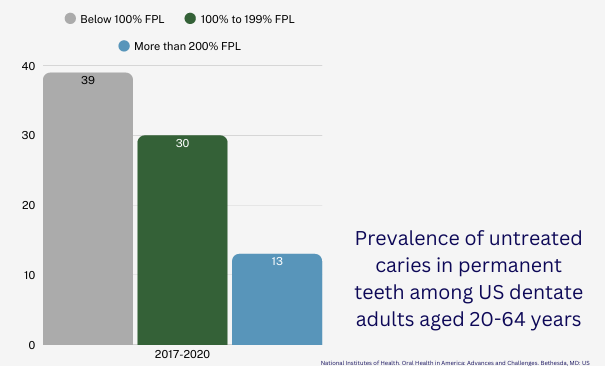
poverty status
race and ethnicity