DSA24/25L - OMM: Upper Respiratory: Otalgia and Sinusitis + Lab
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
36 Terms
-Eustachian tubes are FLAT (flattened angle) & SMALLER in proportion to the cranium
-Tubes are less stiff/more easily compressible
Why are children more predisposed to getting Otitis Media (Middle/Inner Ear Infex)?
In the petrous portion of the Temporal Bone & close to the TMJ
Describe the location of the Eustachian Tube
Mandibular drainage technique via relaxing medial pterygoid mm -> tensor veli palatini m open eustachian tube (used in acute otitis media; drain otitis media into eustachian tube)
Describe the "Galbreath Technique"
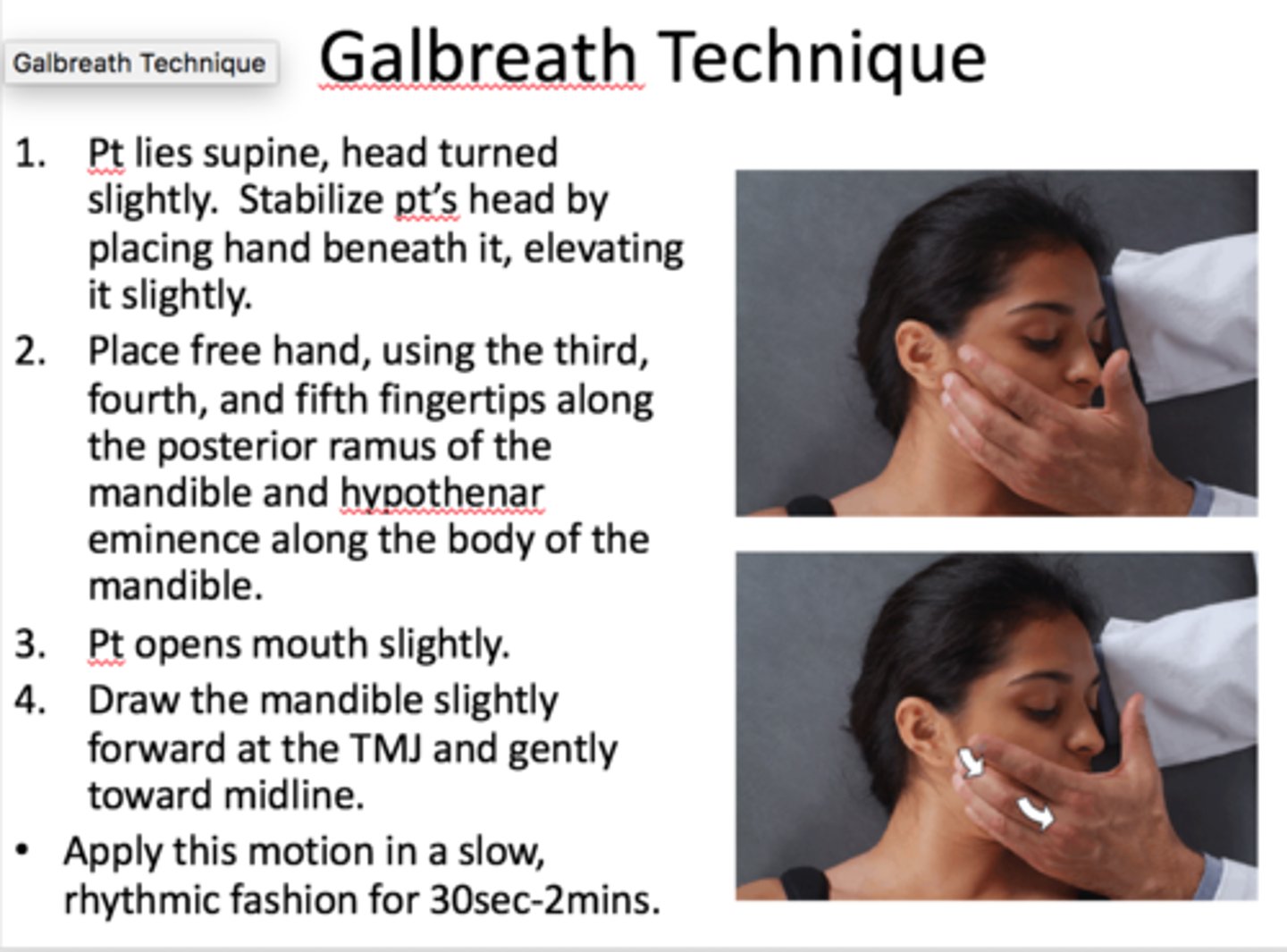
Have pt sit up or supine --> Turn pt's head with affected ear facing AWAY from you --> Take your opposite hand and contact pt's mandible on affected side & APPLY DOWNWARD AND TRANSVERSE MILD FORCE on mandible, so you cross the face --> Repeat in slow, rhythmic application (3-5 sec per round) fro 30-60 seconds
How is the "Galbreath Technique" performed?
B/c it's protecting in the nasopharynx (less potential for pathogens to enter Eustachian tube itself)
Why are the SURROUNDING STRUCTURES of the Eustachian tube preferred locations for OMT for Infex?
-Condylar decompression
-BMT
-VSD
-Parietal Lift/Frontal Lift/OM Suture release
-Tx Ant Cervical Fascia
What cranial OMT can be used to protect the surrounding structures of the Eustachian tube?
Opens the Eustachian tube during swallowing/yawning - helps equalize pressure btwn nasopharynx & middle ear
How does the Tensor Veli Palatini affect the Eustachian tube?
Elevates pharynx + assists opening Eustachian tube w/ swallowing
How does the Salpingopharyngeus affect the Eustachian tube?
When Tensor veli palatini muscle attachment pulls wall of tube laterally during swallowing
What OPENS the Eustachian Tube?
Elastic recoil of cartilage, tissue turgidity, and tension of the Salpingopharyngeus muscle
What CLOSES the Eustachian Tube?
Lacrimal gland, Submandibular gland, Nasopharyngeal Mucosa
What glands are innervated by the Facial Nerve (CNVII)?
Parotid Gland
What glands are innervated by the Glossopharyngeal Nerve (CNIX)?
Eardrum bulges outward as middle ear fills w/ fluid --> Tube Narrows/closes
What anatomical changes occur with Otitis Media (inner ear infex)?
Canal becomes swollen & drains pus
What anatomical changes occur with Otitis Externa (outer ear canal infex)?
-Suboccipital Area
-Supraclavicular Area
What are common sites of lymphatic congestion in Upper Airway mucosa infex (aka areas to CHECK during Resp-Circ Exam)?
The effectiveness of a child's immune system in response to the bacterial and viral insults of the upper airway and middle ear during early childhood
According to the R-C Model, what is the most important factor in determining which children are prone to OM?
-Results in release of cytokines and inflammatory mediators, some of which may cause Eustachian tube dysfunction
-Respiratory viruses also may enhance nasopharyngeal bacterial colonization and adherence and impair host immune defenses against bacterial infection
Why do viral pathogens causing URIs often lead to OM (acc to the R-C Model)?
Offers objective evidence of the presence/absence of OM based on how STIFF the TM is (can be stiffened by scarring, fluid, etc)
What can Tympanometry (acoustic immittance testing) tell us about who is more prone to OMs?
-To identify the offending organism/its sensitivity
-For some pain relief
-For sepsis work-up
When is a Tympanocentesis indicated for AOM Tx in children?
-Severe, refractory pain
-Hyperpyrexia
-Facial Paralysis/Mastoiditis/Labyrinthitis, CNS Infex From AOM
-Immunological compromise
(AKA Third-line Therapy if Pts failed 2 courses of Abx)
When is Myringotomy (incision into the eardrum) indicated for AOM Tx in children?
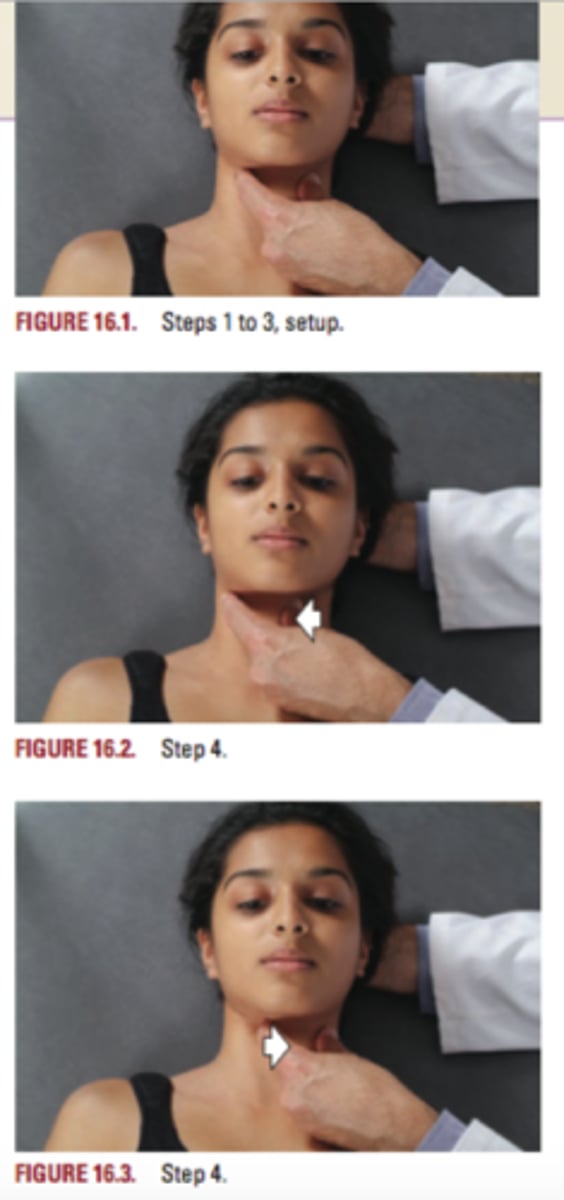
Anterior Cervical Arches:
Stabilizes pt head with one hand; opposite hand's thumb and index finger form a horseshoe shape over anterior cervical arches, making alternating contact with lateral aspects of hyoid bone, thyroid cartilages, then cricoid cartilage, gently pushing them side-to-side for 30 seconds-2 minutes
What is this R-C OMT technique?
Submandibular Release:
DO index and 3rd fingertips placed immediately below the inferior rim of the mandible directed superiorly into submandibular fascia; determine ease --> bind asymmetry and apply a gentle direct or indirect treatment until a release is palpated (30 sec- 2 min)
What is this R-C OMT technique?
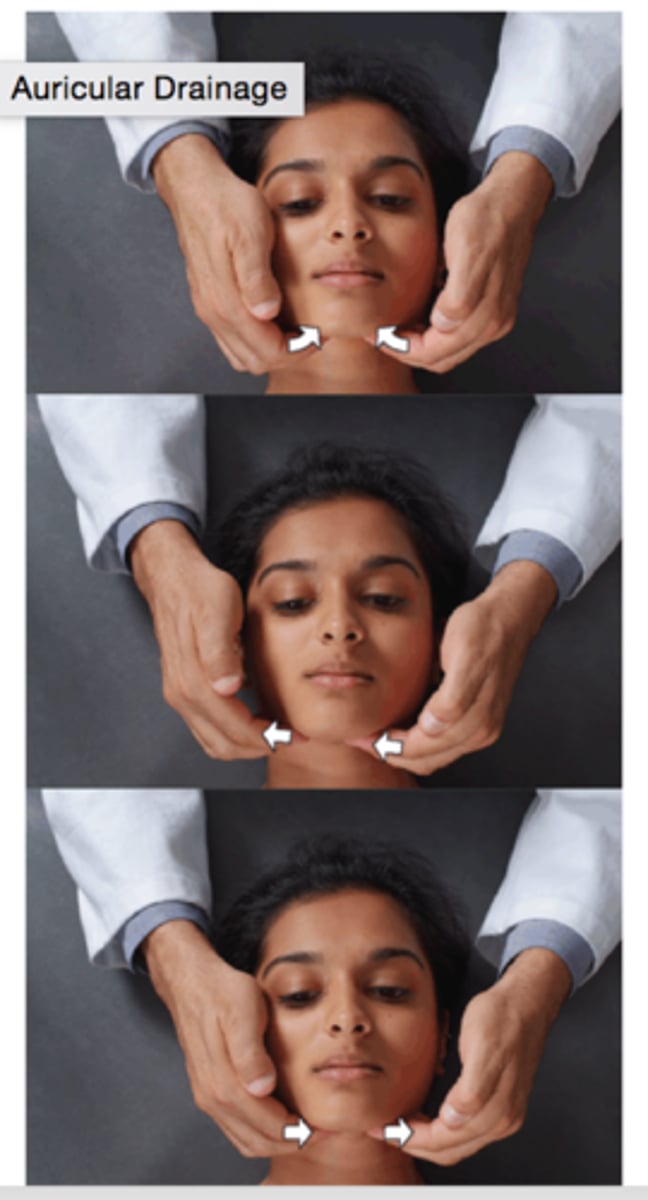
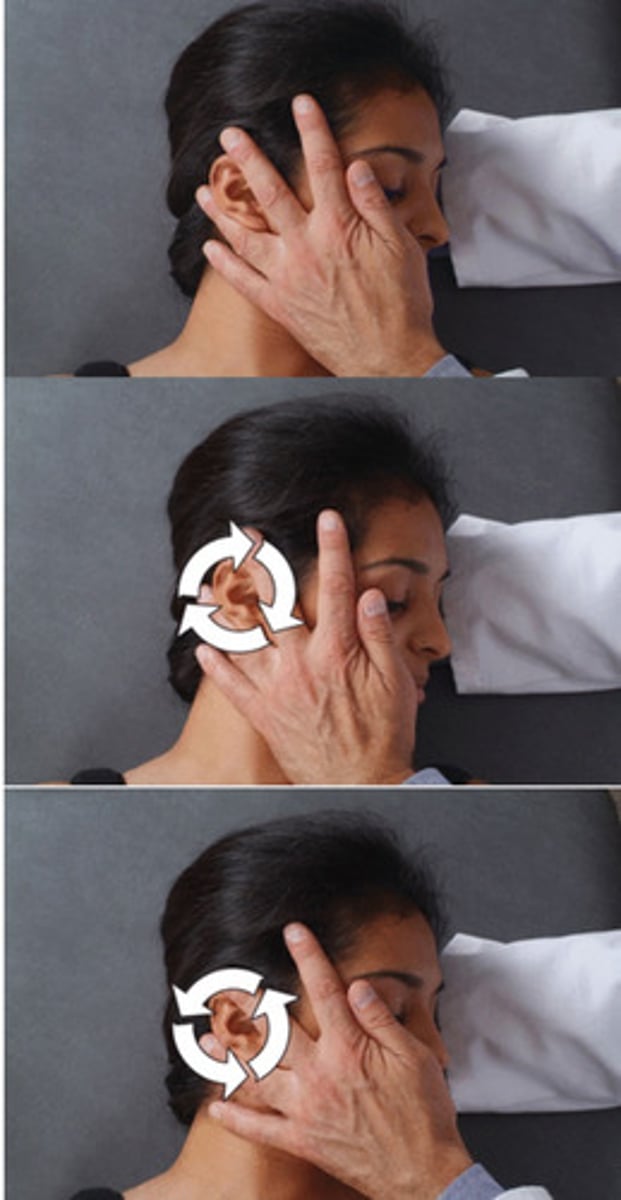
Auricular Drainage:
Pt supine with head turned towards DO seated near head of table; DO stabilizes pt head with cephalad hand beneath the head to elevate it slightly; DO places caudad hand flat against side of pt head with fingers pointing cephalad and the ear between 3rd and 4th fingers; DO hand makes clockwise and counterclockwise circular motions, moving the skin and fascia over the surface of the skull for 30 sec-2 min
What is this R-C OMT technique?
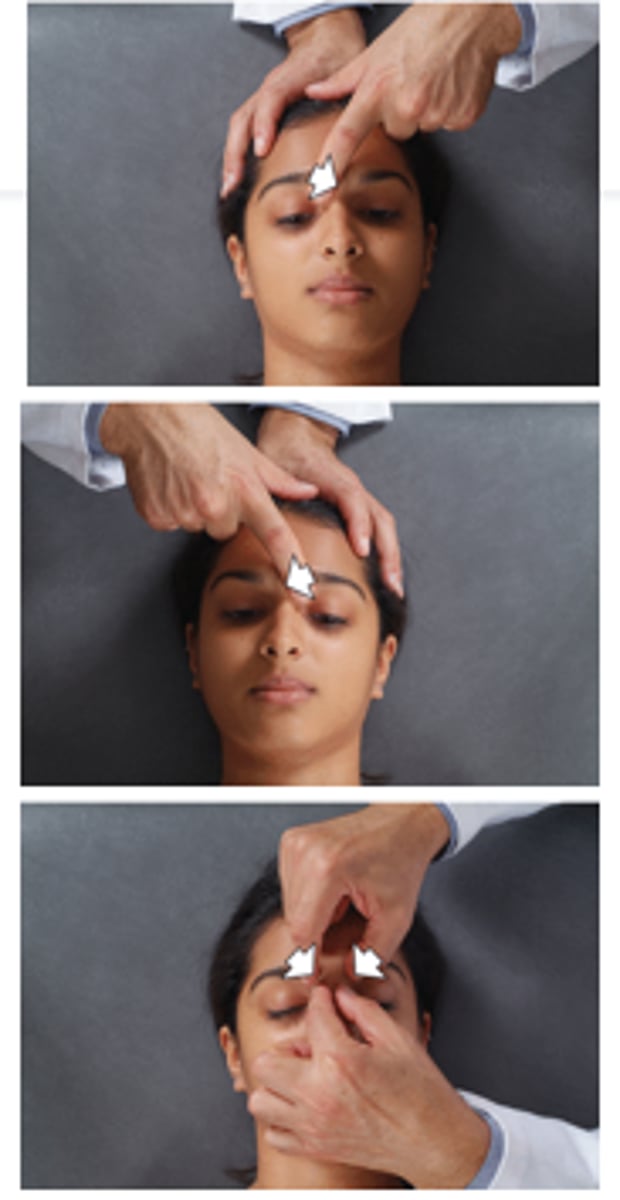
Alternating Nasal pressure:
Pt supine with DO seated at head of table; DO uses index finger to press on a diagonal into the junction of nasal and frontal bones, first in one direction and then the other, for 30 sec-2 min
What is this R-C OMT technique?
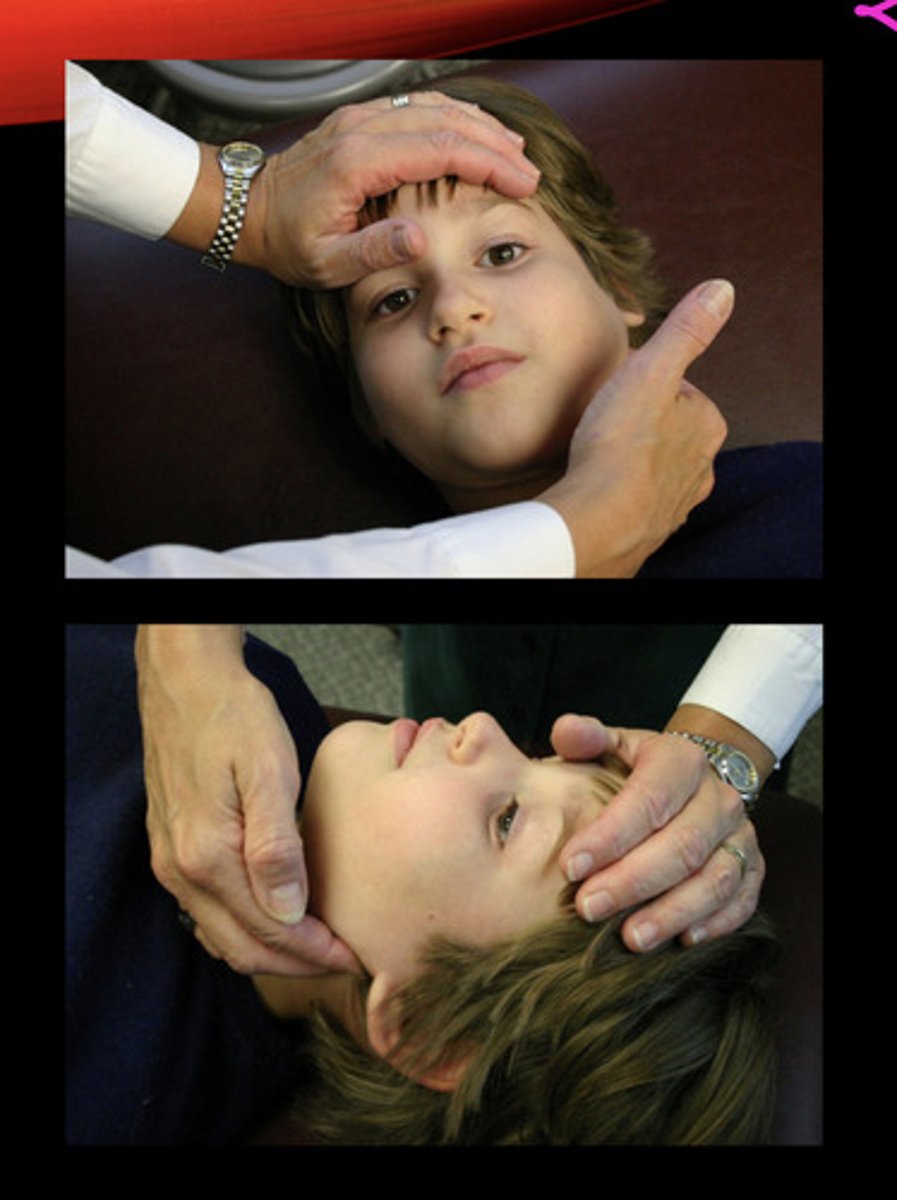
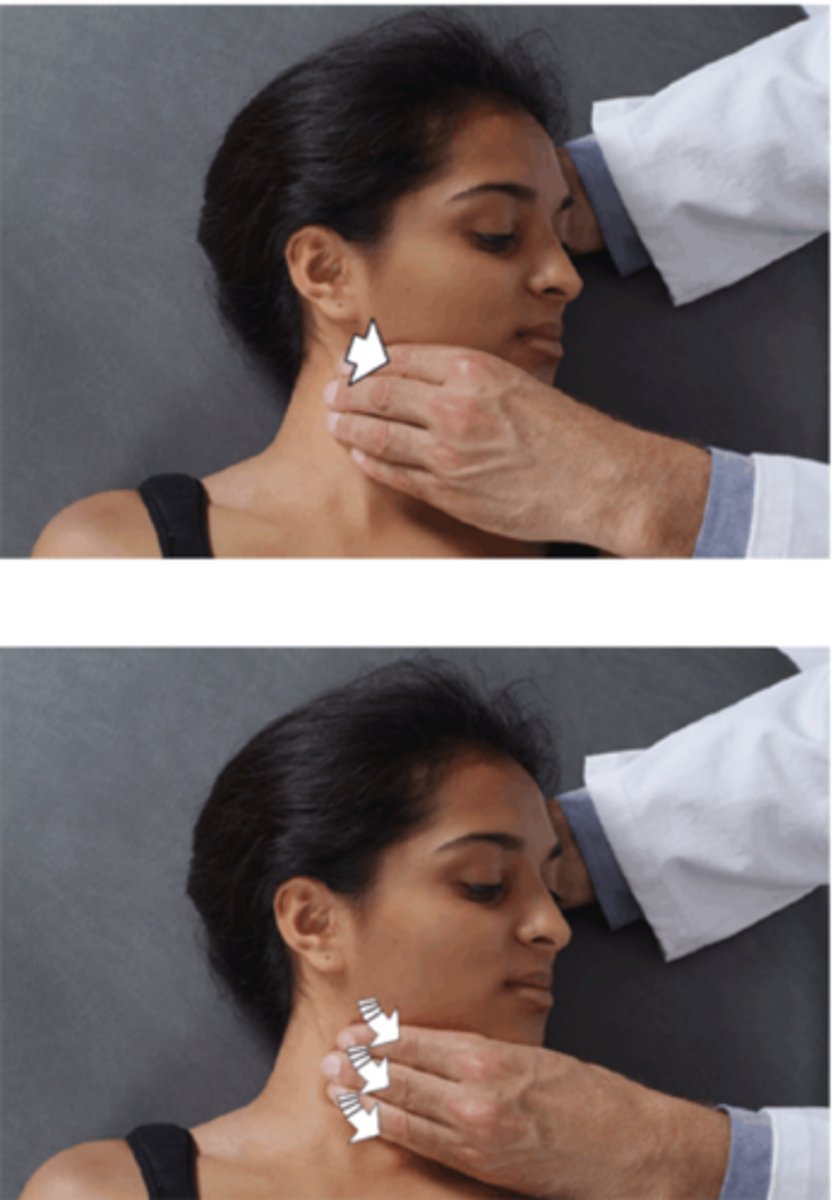
Cervical Chain Drainage:
Pt supine with head turned towards DO seated near head of table; DO stabilizes pt head with cephalad hand beneath the head to elevate it slightly; or by gently grasping pt forehead; DO caudad hand (palmar aspect of fingers) makes broad contact over SCM muscle near angle of the mandible; from cephalad to caudad (OR caudad to cephalad), fingers roll along the muscle in a milking fashion; procedure is repeated anterior and posterior to SCM in order to affect both anterior and posterior cervical lymphatic chains
What is this R-C OMT technique?
Frontal Sinus Effleurage:
DO index finger pads placed immediately superior and medial to pt eye brows to begin slow, gentle stroking (effleurage) laterally that takes them immediately parallel to the supraorbital ridge until they meet the area of the pterion; fingers continue inferiorly in a continuous gentle motion toward the TMJ and inferiorly over the mandible for 30 sec-2 min
What is this R-C OMT technique?

Maxillary Sinus Effleurage:
DO index finger pads placed inferior to infraorbital foramina to begin a slow, gentle stroking (effleurage) over pt's skin immediately parallel to lateral aspect of the nose until meeting dental ridge; fingers continue laterally in a continuous gentle motion toward alar aspect of zygoma for 30 sec-2 min
What is this R-C OMT technique?

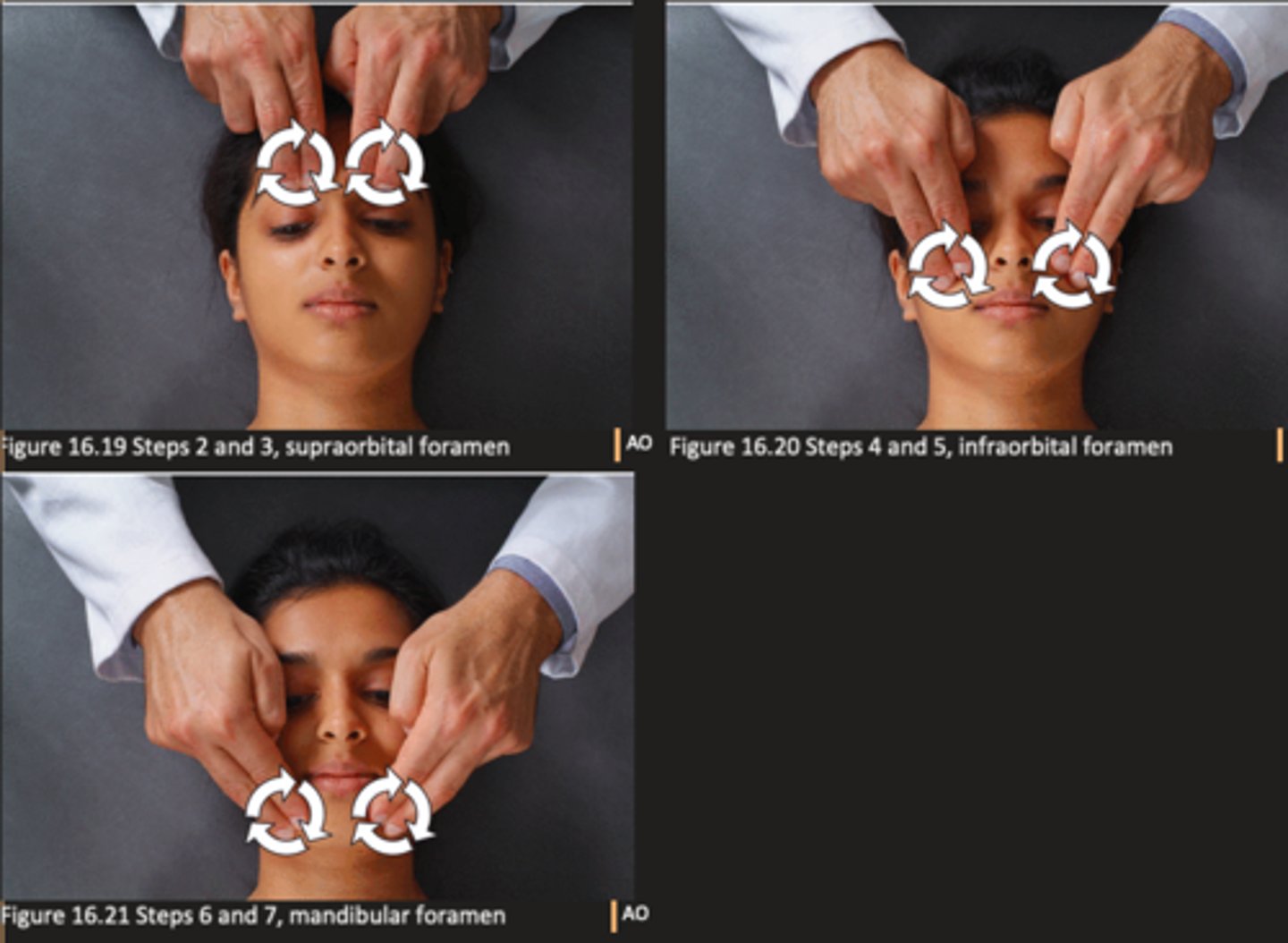
Trigeminal Nerve Decongestion:
Pt supine with DO seated at head of table; DO palpates along superior orbital ridge to ID the supraorbital foramen; DO places index finger pads just inferior to orbital ridge and produces circular motion bilaterally; these steps are repeated at infraorbital foramen and submental foramen for 30 sec-2 min at each of the (3) locations
What is this R-C/Neuro OMT technique?
-Second-hand smoke
-Formula/bottle feeding
-Giving antihistamines/Decongestants too often
What behaviors make children more suscepitble to AOM?
-Fewer episodes
-Fewer surgeries
-More normal Tympanograms
Overall, both pediatric and adult pts with Recurrent AOM experienced what benefits post OMT (according to the studies mentioned)?
Inflammation/Viruses can reduce ciliary motion
Why are 1-2% of colds complicated by bacterial sinusitis?
-Purulent Drainage
-Face Pain
-Fever
-Hearing Loss/Ear Pain
-Issues with smelling
-Halitosis
What are the signs/sx of Sinusitis?
-Viral = Decongestants (Sx), Seroids, Saline
-Tx allergic component w/ Antihistamiens
-Bacterial = Abx (if Fever + Sx > 7 days & worsened)
What is the Usual Tx for Sinusitis?
•Insure proper cranial motion to pump sinuses
•Treat OA if nothing else
•Direct nasal sinus treatment
What is the Biomechanical Tx for Sinusitis?
•Trigeminal Stimulation of sinuses
•Treat upper thoracics T1-T4 (Sympathetics)
•Tx the Pterygopalatine ganglion (PNS)
What is the Neurologic Tx for Sinusitis?
•Target Thoracic Inlet & Anterior Cervical Fascia
•Effleurage to Sinuses
What is the R-C Tx for Sinusitis?