3 Spinal Cord Pt 2
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
Ascending Pathway
What does the ascending (sensory) system carry?
Carries:
Exteroceptive – from outside body (pain, temp, touch)
Proprioceptive – from inside body (muscles and joints)
helps brain know where body is in space
Ascending Pathway
Diff types of sensory info comes from diff types of receptors and is carried on diff types of nerve fibers. List the type of sensory information carried.
Touch (light touch vs. deep pressure; crude/gross vs. 2-point tactile discrimination, vibration)
Proprioception – conscious or unconscious
Pain
Temp
Ascending Pathway
What is the general organization of ascending (sensory) pathways? Mention the location of the cell bodies
Posterior Column (ML) Pathway
What information is carried in the Posterior Column (Medial Lemniscus) Pathway?
2-point touch discrimination
conscious proprioception
vibration
**only pathway that travels in the posterior column
Posterior Column (ML) Pathway
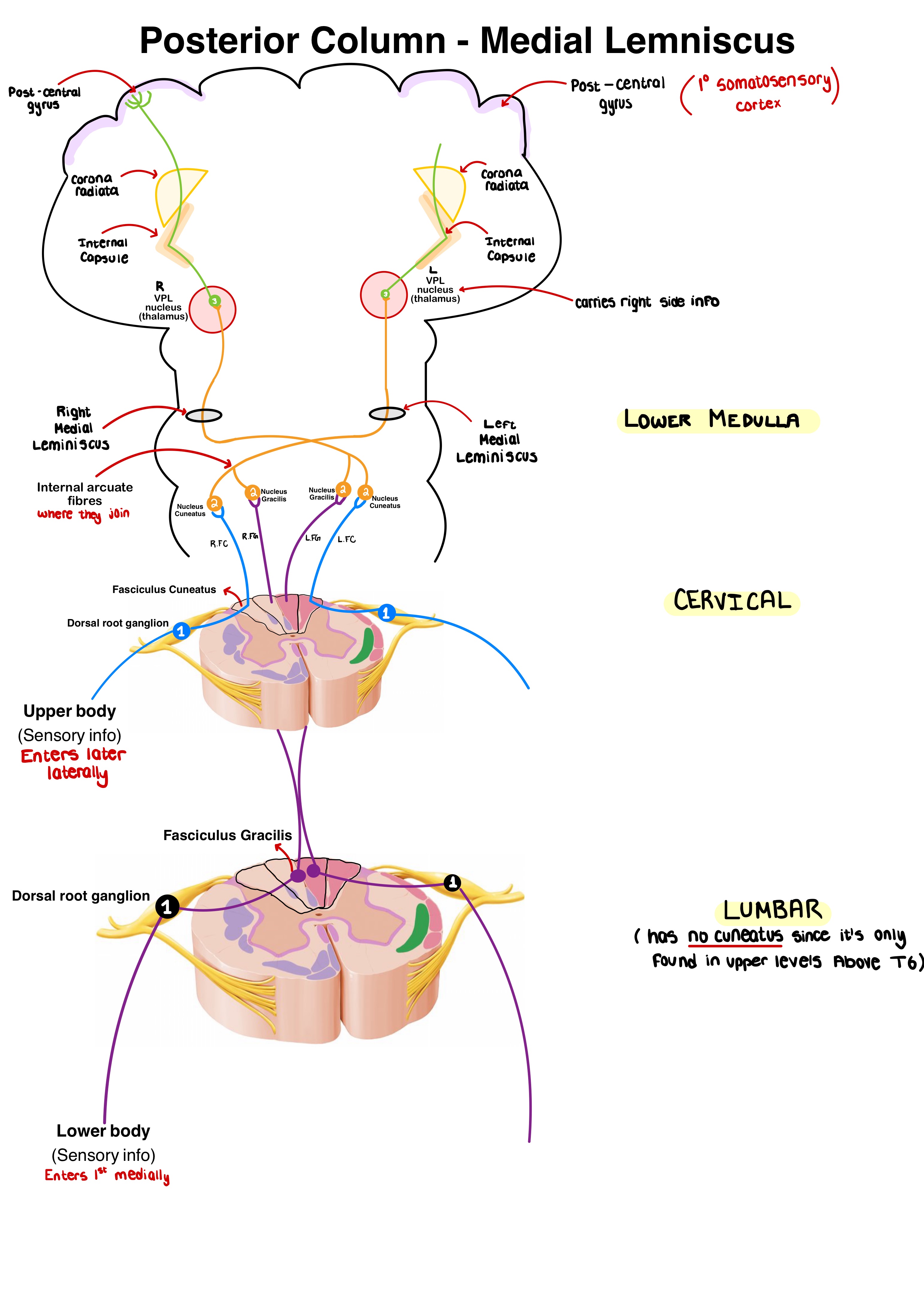
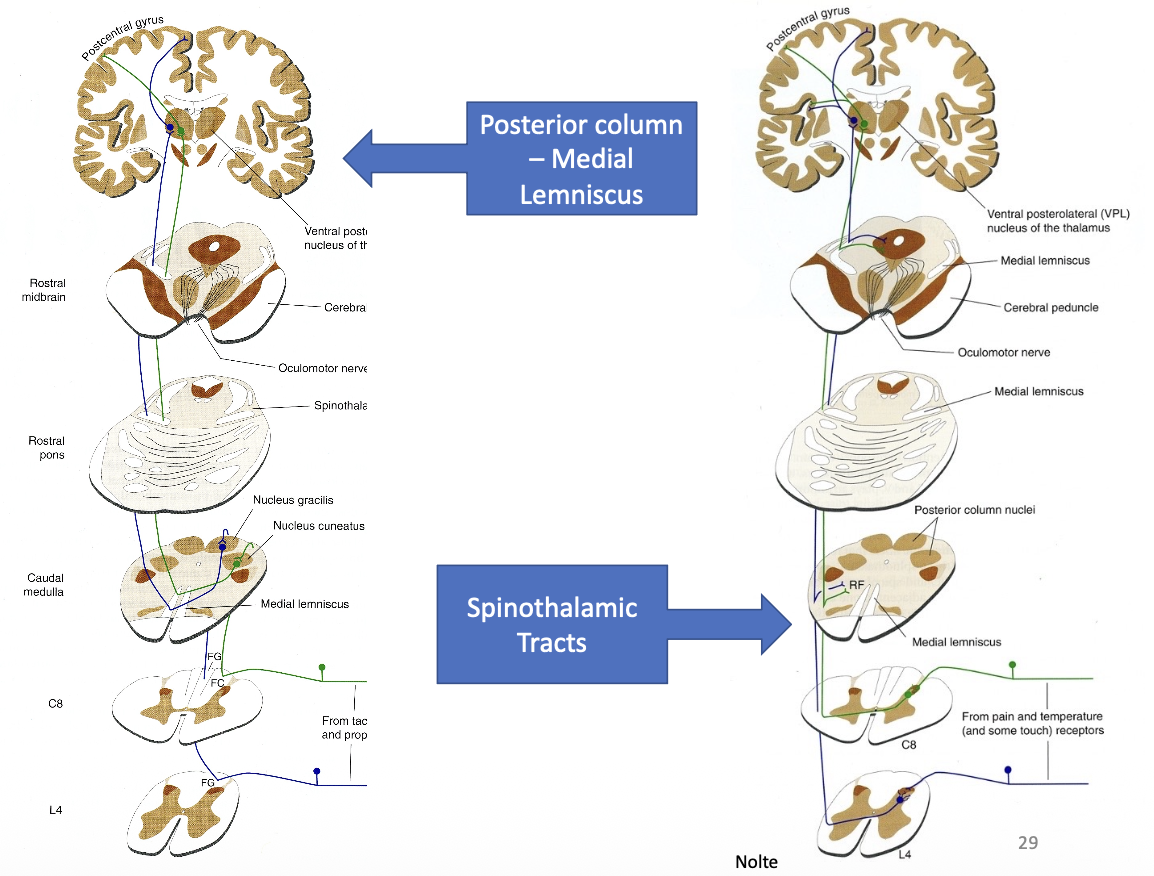
Outline the Posterior Column (ML) Pathway.
1st order neuron (spinal cord)
Cell body: dorsal root ganglion
travels through Fasciculus gracilis medially (lower body) or fasciculus cuneatus (upper body) laterally
ends at medulla
2nd order neuron (medulla/brainstem)
Cell body: nucleus gracilis (lower body) & nucleus cuneatus (upper body)
Axons of nucleus gracilis and cuneatus join at internal arcuates and CROSS in sensory decussation
Travel up as medial lemniscus (tract of lots of 2nd order neurons)
ends at VPL thalamus
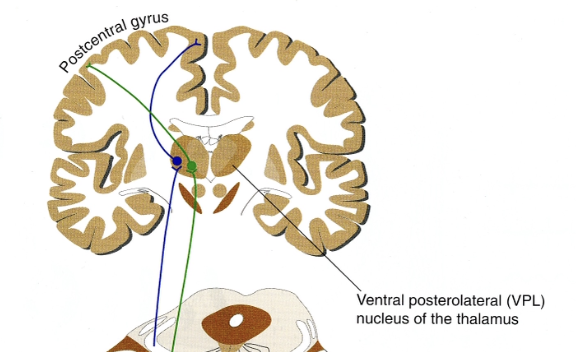
3rd order neuron (cortex)
Cell body: VPL thalamus
Travel through internal capsule → corona radiata → post-central gyrus (parietal lobe)
For the posterior columns-medial lemniscus tract:
Which order neuron is ascending in the white columns?
Which order neuron is ascending in the brainstem?
Which white columns do you find them in and where in the brainstem?
White column = 1st-order neuron (dorsal columns)
Brainstem = 2nd-order neuron (Medial lemniscus)
Posterior Column (ML) Pathway
How is the Posterior Column (Medial Lemniscus) Pathway organized? Where does the last synapse occur?
→ somatosensory organization is maintained at ALL levels
Postcentral gyrus = 1st (primary) somatosensory cortex in parietal lobe
contains the sensory homunculus
Posterior Column (ML) Pathway
What sensory modalities are affected when there’s damage to Posterior Column (ML) Pathway.
Completely lost:
Conscious proprioception
Kinesthesia
Severely affected:
Complex (fine) tactile discrimination
Minimally affected / reduced (not completely lost):
Pressure
Vibration
→ b/c these sensations have alternative pathways
What symptoms arise when there’s a lesion ABOVE vs BELOW the sensory decussation?
ABOVE = contralateral
BELOW = ipsilateral
Posterior Column (ML) Pathway
What would occur if there’s damage at:
Left posterior column at C8
Left posterior column at L4
Left pons in ML
Right Postcentral gyrus
Left C8 = left UPPER and LOWER extremity sensory loss
Left L4 = lose conscious proprioception and tactile discrimination (↓ pressure and vibratory sense) in left LOWER extremity
Left ML = right sensory loss (above sensory decussation)
Right Postcentral gyrus = left sensory loss
Posterior Column (ML) Pathway
What is a motor coordination defect that can occur due to damage to PCML pathway?
Sensory Atraxia - incoordination of movement due to loss of sensory feedback about current position of body part
most pronounced with eyes closed since lose visual feedback about body position
Romberg test: pt stands upright and closes eyes, where loss of balance indicates (+) Romberg = impaired posterior column function

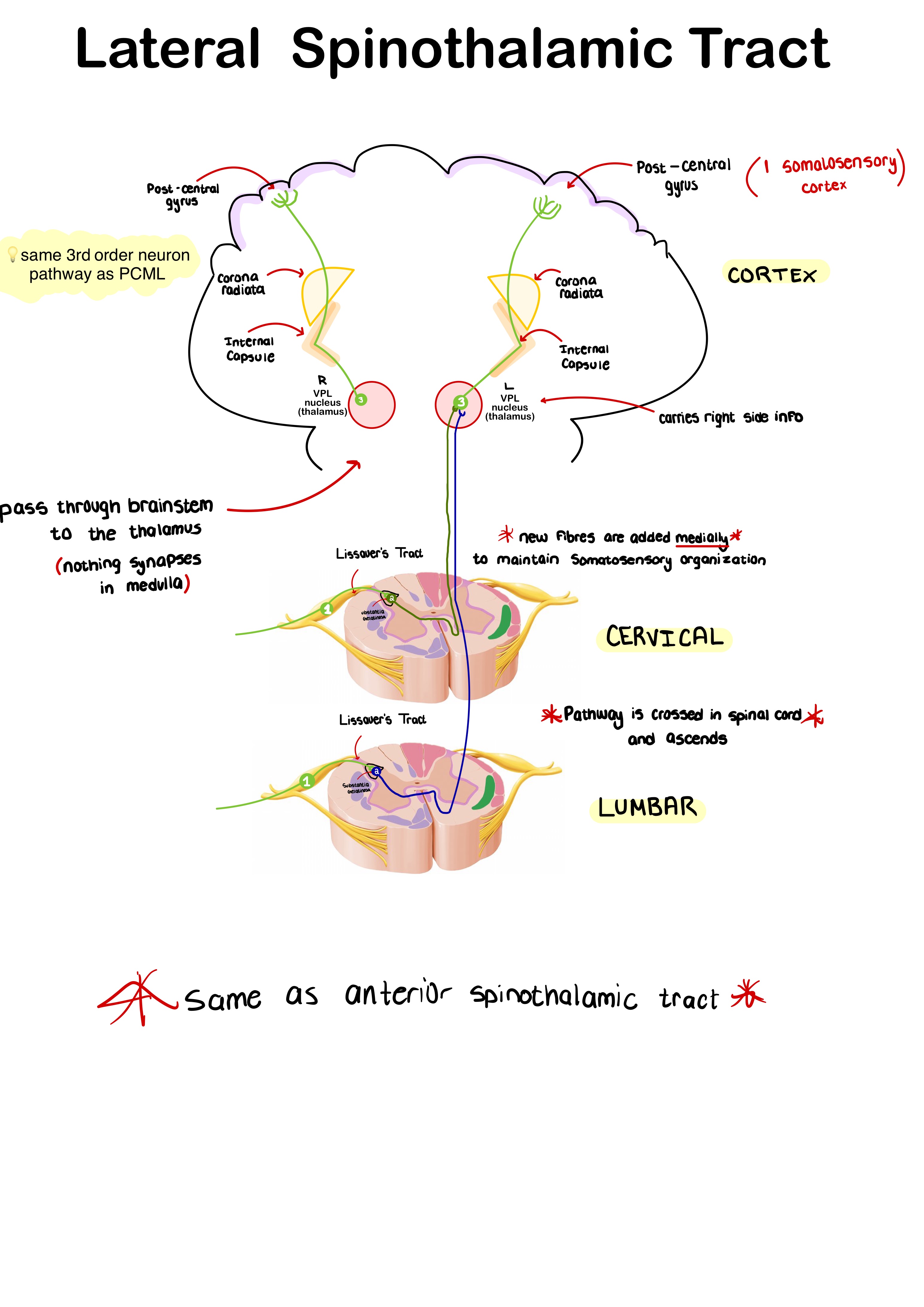
Lateral Spinothalamic Tract
What information is carried in the Lateral Spinothalamic Tract Pathway?
Conscious pain and temp (awareness and localization)
Lateral Spinothalamic Tract
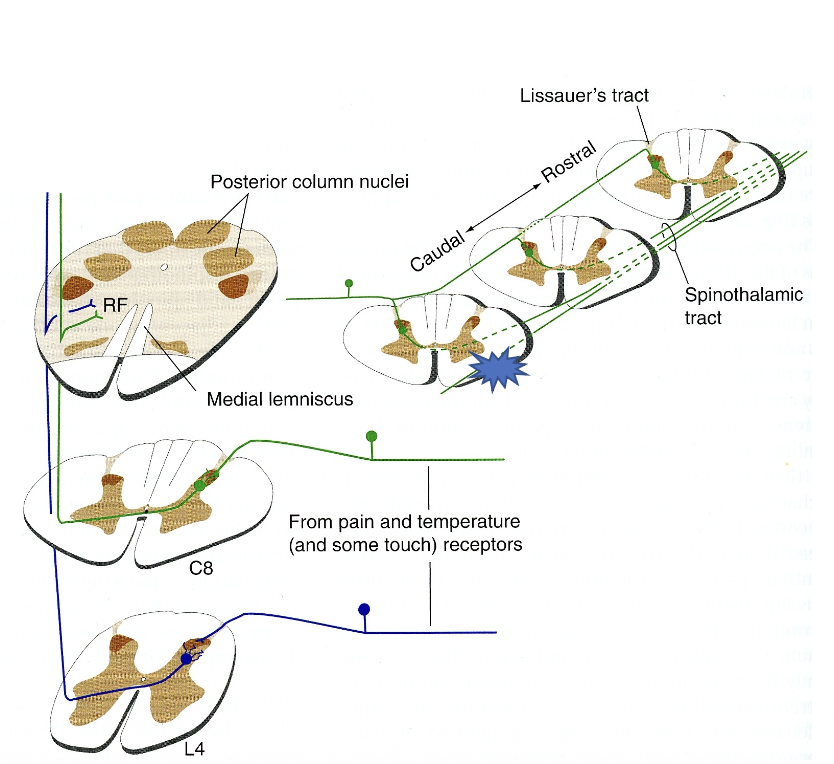
Outline the Lateral Spinothalamic Tract.
1st order neuron (spinal cord)
Cell body: dorsal root ganglion
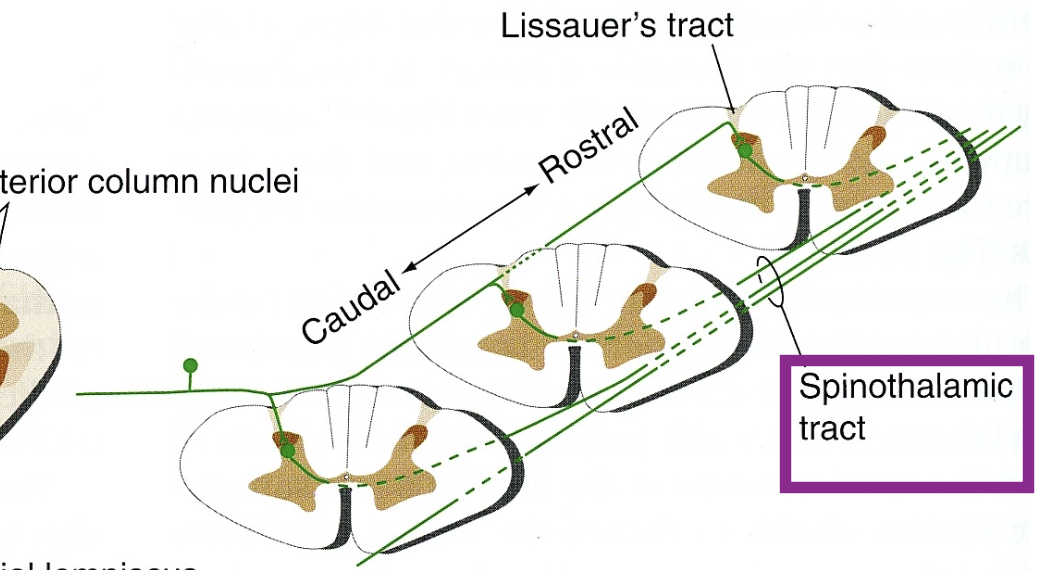
travels through Lissauer’s tract
ends at substantia gelatinosa
2nd order neuron (spinal cord)
Cell body: Substantia gelatinosa
axon crosses obliquely in anterior white commissure, then ascends in the contralateral white column as the “lateral spinothalamic tract" (bunch of 2er neurons)
spinal cord → brainstem → thalamus
ends in VPL nucleus
3rd order neuron (thalamus)
Cell body: VPL nucleus
Travel through posterior limb internal capsule → corona radiata → post-central gyrus (parietal lobe)
For the Lateral Spinothalamic Tract:
Which order neuron is ascending in the white columns?
Which order neuron is ascending in the brainstem?
Which white columns do you find them in and where in the brainstem?
White column = 2nd-order neuron (contralateral white columns)
Brainstem = 2nd-order neuron (spinal lemniscus)
Lateral Spinothalamic Tract
How is somatosensory organization maintained here?
as lateral Spinothalamic tract ascends, new fibers are added medially → somatosensory organization is maintained
Lateral Spinothalamic Tract
What does a lesion to the spinothalamic tract cause?
→ loss of conscious pain and temp on OPPOSITE side of body beginning 1-2 spinal segments BELOW the lesion level …. due to oblique rise
e.g., lesion to the LEFT lateral spinothalamic tract at T1 would cause loss of pain and temp sensation on the RIGHT side at T3 and below
Lateral Spinothalamic Tract
Why is lateral cordotomy performed on some patients with intractable pain?
destroys lateral spinothalamic tract 1-2 segments ABOVE level of pain, preserving tactile sensation (which is carried in posterior column)

Lateral Spinothalamic Tract
What occurs if there’s a lesion to the anterior white commissure?
BILATERAL loss of pain and temp 1-2 segments BELOW
Fibers already in and entering Lateral spinothalamic tract and higher are unaffected
Damage at T8 → loss of pain & temp at T9-T10
Spared → below T10 + at & above T8
Anterior Spinothalamic Tract
What information is carried in the Anterior Spinothalamic Tract Pathway?
Light/crude touch
Pressure
Poorly localized/discriminated sensation
How do the anterior and lateral spinothalamic pathways travel in the CNS?
remain separate in spinal cord
Travel together in brainstem
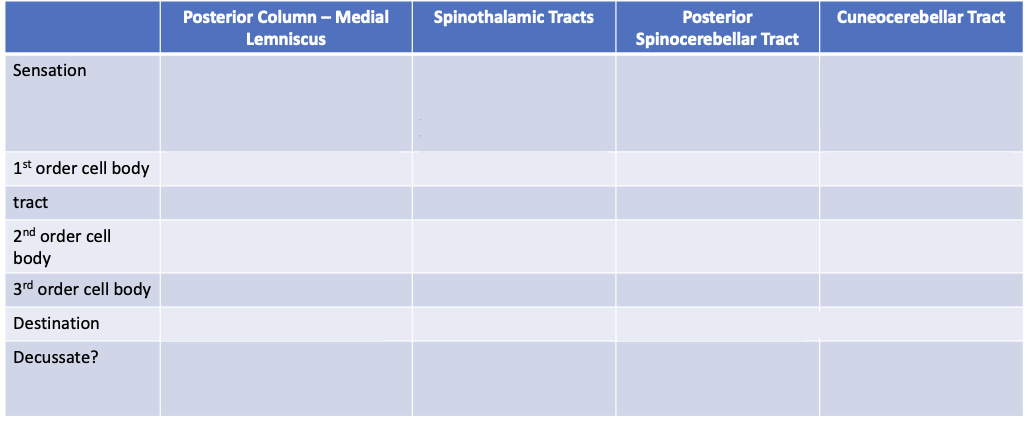
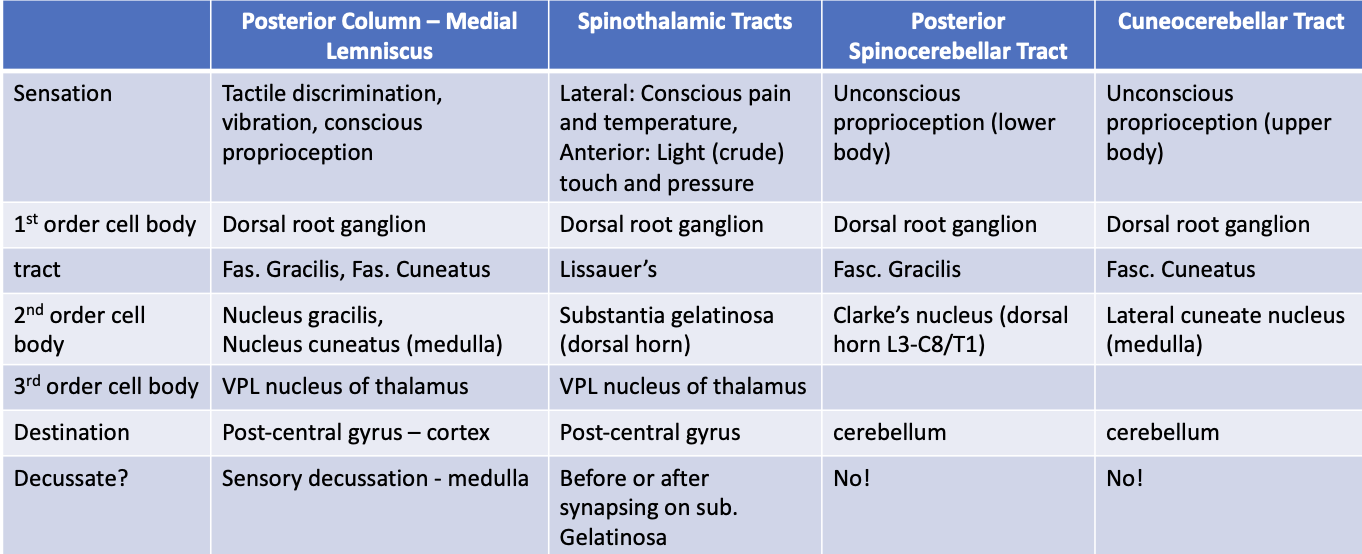
Fill out this table.
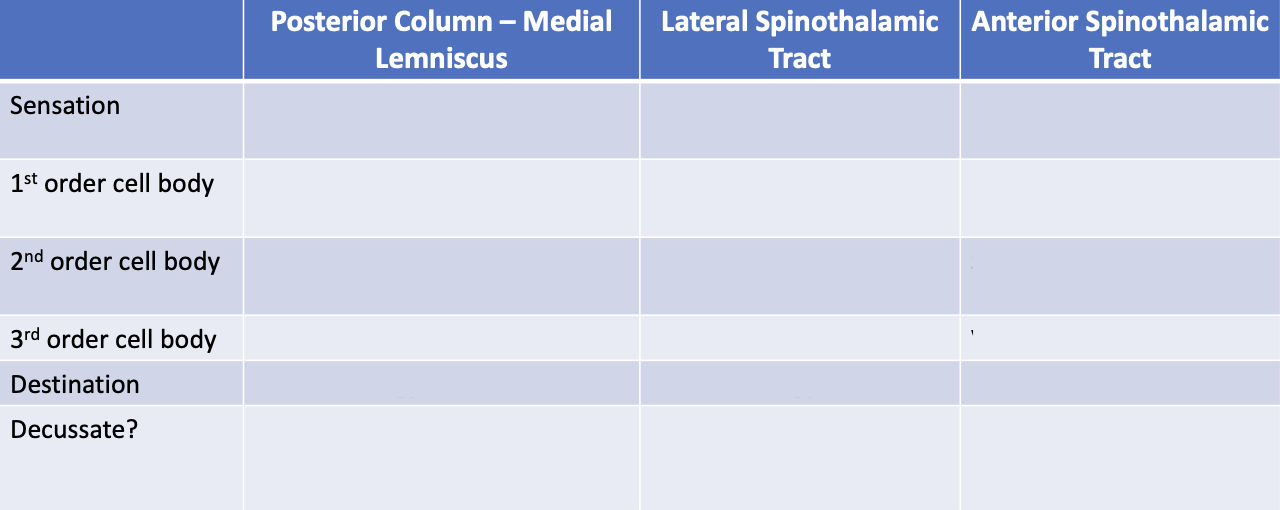
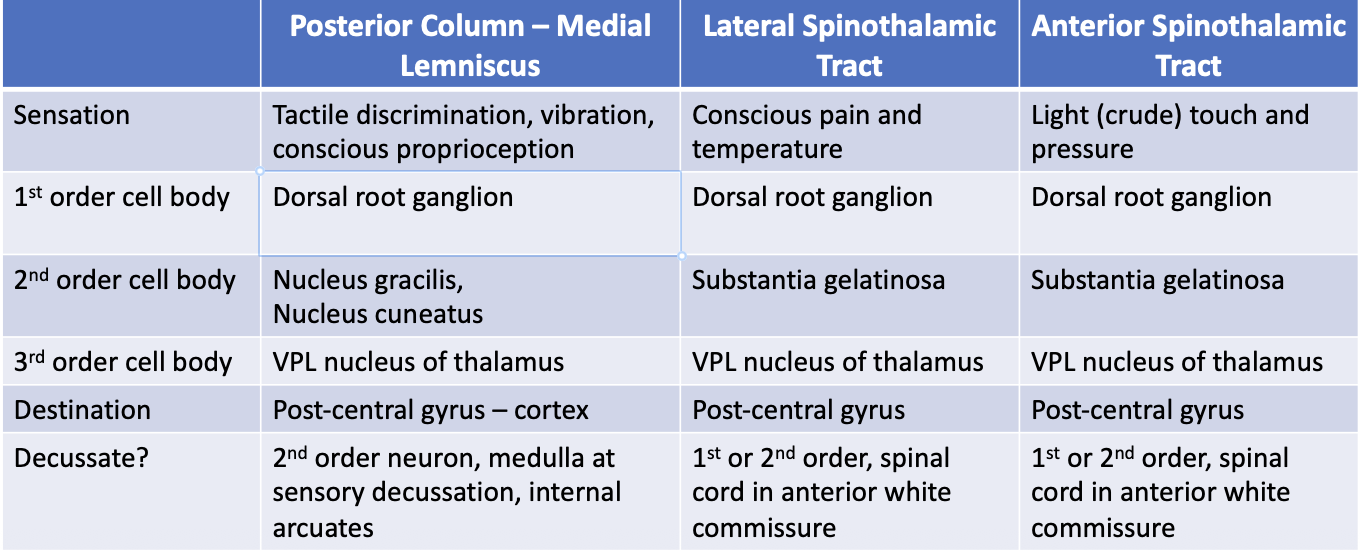
The Posterior Column – Medial Lemniscus, Lateral and Anterior Spinothalamic Tract are all _______ sensory pathways.
The Posterior Column – Medial Lemniscus, Lateral and Anterior Spinothalamic Tract are all concious sensory pathways
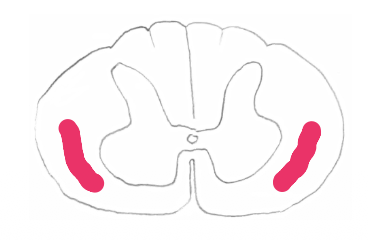
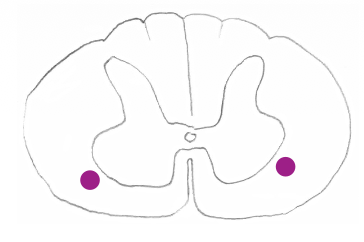
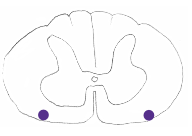
The axons travelling in the blue dot area are carrying what type of information for which side of the body?
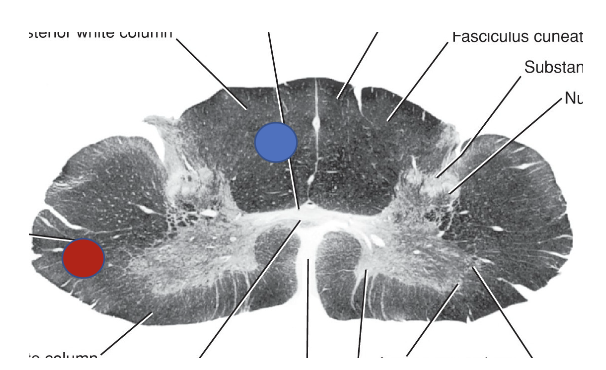
Blue dot = Posterior white column: carrying conscious proprioception, 2-point tactile and vibratory sense from the RIGHT side of the body
Red dot = 2nd order neuron carrying pain and temp sensation from the LEFT side of the body
What information do Spinocerebellar Tracts carry in general?
→ Unconscious proprioception for coordination of movement of limbs and posture
Unconscious = doesn’t go to thalamus and cortex – goes to cerebellum instead
How do typical ascending pathways and Spinocerebellar pathways vary?
Ascending = 3 neuron pathways
Spinocerebellar = tracts are uncrossed (usual for cerebellum)
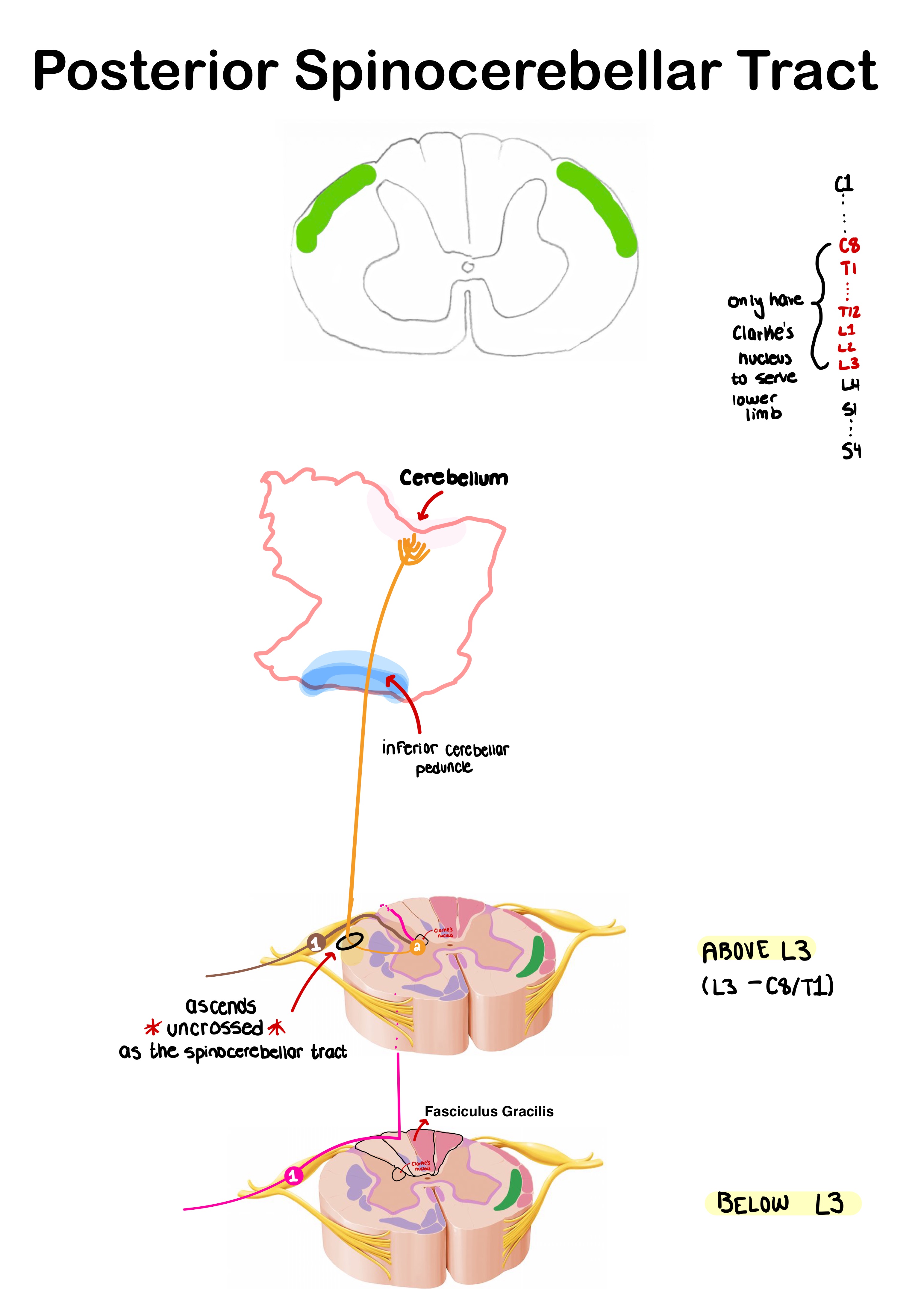
Posterior Spinocerebellar Tract
What information is carried in the Posterior Spinocerebellar Tract Pathway?
Unconscious proprioception from trunk and lower extremities

In which level is Posterior spinocerebellar tract fibers found?
at the level of Clarke’s nucleus and above; below this level, they travel within the fasciculus gracilis
Cuneocerebellar Tract
What information does the Cuneocerebellar Tract carry? Why is it separate from the spinocerebellar pathway?
→ Unconscious proprioception from upper extremities only
Note: separate from Cuneocerebellar Tract b/c Clarke’s nucleus doesn’t exist above T1
List the 3 minor sensory pathways,
Spino-tectal
Spino-reticular
Spino-olivary
How do the minor pathways differ from the major sensory pathways?
Start in the spinal cord “spino-”
End in the brainstem “tectum-” “reticular-” “olivary”
doesn’t not in cerebral cortex or cerebellum
unconcious pathways (b/c it’s not going to the cortex)
Minor Pathways
What info does the Spinotectal Tract carry?
Spinal cord to Tectum
→ afferent info for spinovisual reflexes (helps orient head and eyes towards stimulus)
Minor Pathways
What information does the Spinoreticular Tract carry?
Spinal cord to Reticular formation
awakened state/levels of consciousness
Minor Pathways
What information does the Spino-olivary Tract carry?
Spinal cord to Inferior olivary nuclei
→ Unconscious proprioception
Fill this table out.
Descending Pathway
What are the characteristics of Descending Pathways?
→ carry voluntary motor pathways
e.g., pyramidal pathways for body and head
-2 neuron pathway
How is motor control organized in the cerebral cortex, and is this organization maintained in the spinal cord?
Motor control in the cerebral cortex is somatotopically organized (motor homunculus):
Face = lateral, foot = medial
Hands and face occupy a disproportionately large area for fine motor control and speech
this cortical organization is NOT maintained at the spinal cord level
was maintainte for ascending pathways (sensory homunculus)
How do upper motor neurons (UMNs) and lower motor neurons (LMNs) work together to produce movement?
1) UMNs originate in the brain (cortex or brainstem)
2) They then decend in various motor pathways and synapse on LMNs
UMNs never synapse directly on muscle they instruct the LMN
3) LMN cell bodies are found in the ventral gray horn (spinal cord) or cranial nerve nuclei (brainstem)
4) LMNs are the final common pathway, where they exit via the ventral root and directly innervate skeletal muscle
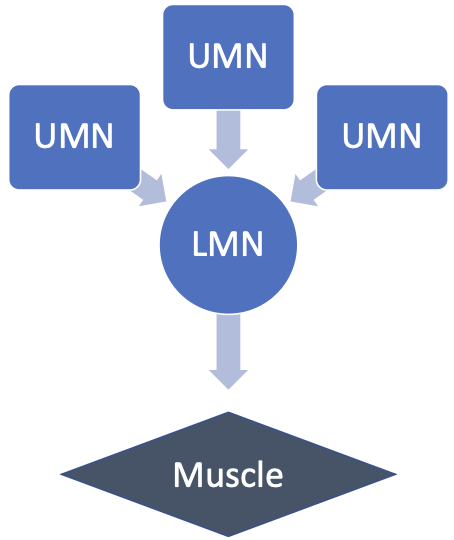
What happens when an UMN is damaged vs a LMN?
UMN is damaged → still some motor function via a different UMN pathway
LMN is damaged → no signals get through to muscle → no motor function
Lateral Corticospinal Tract - pyramidal pathway
What information does the Lateral Corticospinal Tract carry?
Voluntary, concious, skilled movements at distal flexors (hands/fingers)
Lateral Corticospinal Tract
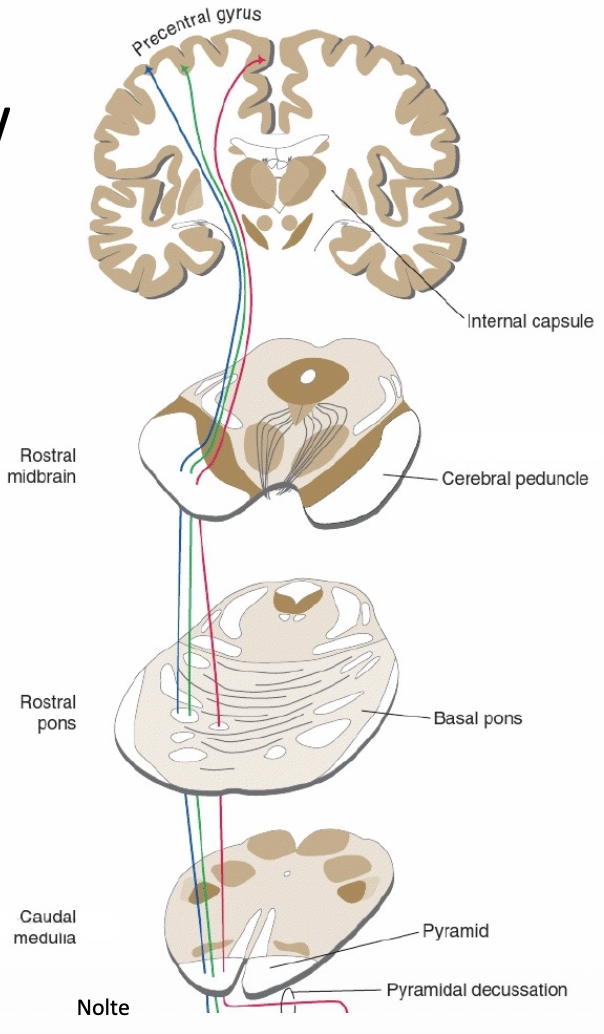
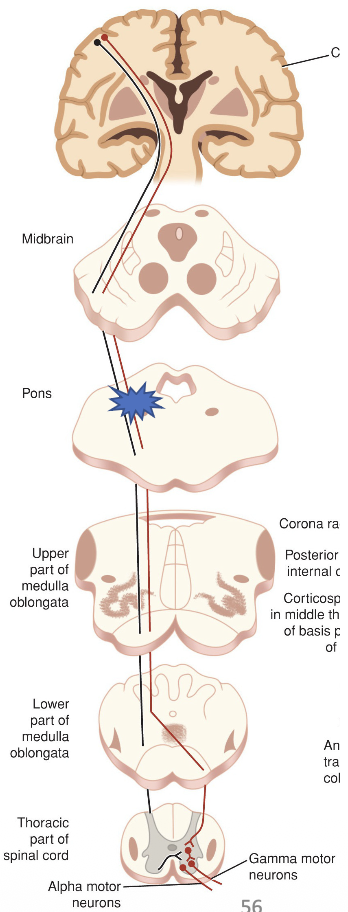
Outline the Lateral Corticospinal Tract pathway.
1st-order neuron (UMN)
Cell bodies: pyramidal cells in mainly in precentral gyrus (1er or 2er motor cortex in frontal lobe), some from postcentral gyrus
Axons converge in corona radiata → internal capsule (posterior limb)
Descend through brainstem in:
Midbrain: crus cerebri (cerebral peduncle)
Pons: base of the pons
Medulla: pyramids
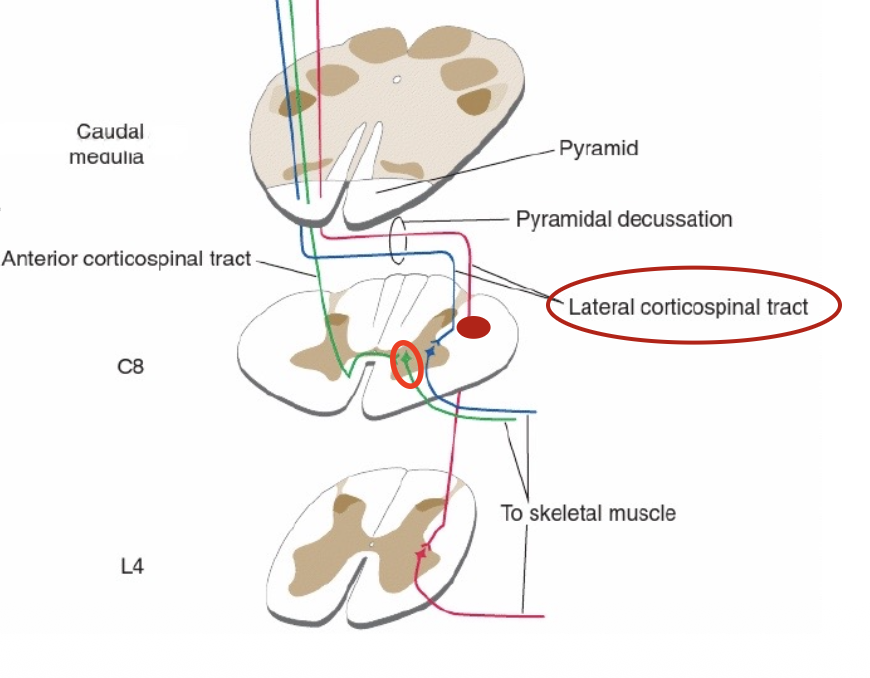
85-90% axons cross in the pyramidal decussation (lowest level of medulla)
Enter the spinal cord as lateral corticospinal tract in lateral white column
Exit lateral white column to synapse on LMN (α-motor neuron) in ventral horn
2nd-order neuron (LMN)
Cell bodies: ventral root
LMN exits the spinal cord in ventral horn to innervate a muscle
For the Corticospinal tract:
Which neuron is descending through the brainstem?
Which neuron is descending in the spinal cord?
And in what white column?
Brainstem: UMN (1st order neuron)
Spinal cord: UMN (1st order neuron)
Lateral white column as the lateral corticospinal tract
What happens to the 10-15% UMN fibers that don’t cross at the pyramidal decussation of the Corticospinal Tract? What do these specific fibers control?
→ Descend in anterior white column as “Anterior corticospinal tract”
Info: Fibers mostly control axial muscles in neck and shoulders (upper thoracic)
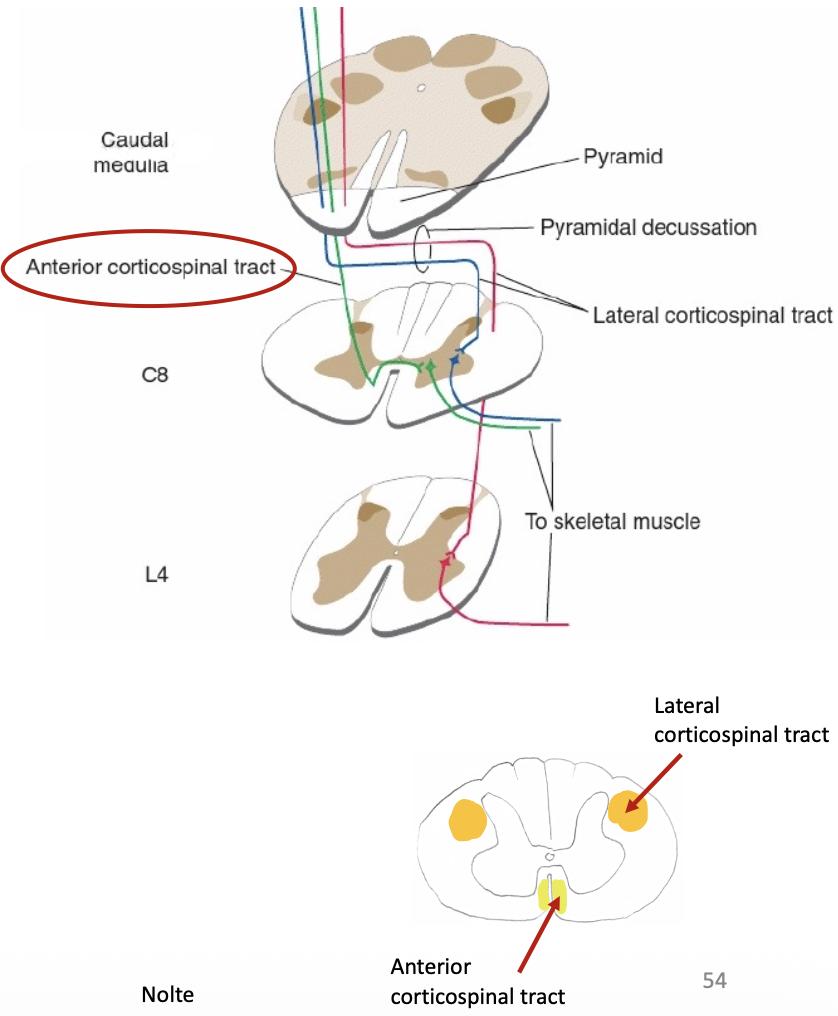
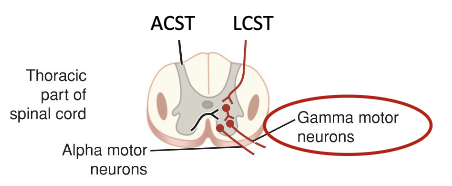
In addition to synapsing on α-motor LMN, what else can the Lateral corticospinal Tract & Anterior corticospinal tract (minor pathway) synapse on?
inhibitory gamma LMN → inhibit certain reflexes
Pyramidal Pathways
What occurs if there’s a lesion to the:
Posterior limb of the Internal capsule (brain)
Left corticospinal tract (pons)
Left lateral corticospinal tract (spinal cord)
Internal capsule (posterior limb) = impact sensory and motor on opposite side
Pon = lose voluntary motor function on opposite side (b/c ABOVE motor decussation)
Spinal cord = lose voluntary motor function on same side (b/c BELOW motor decussation)
Pyramidal Pathways
What does damage to UMN result in?
Spastic paralysis (paresis)
partial loss of voluntary motor control = ↑ muscle tone
Hyperreflexia (overactive involuntary reflexes)
Recall: Gamma LMNs inhibit reflex, so when there’s no innervation via UMN due to damage → lose of reflexes
Fine motor movements impaired
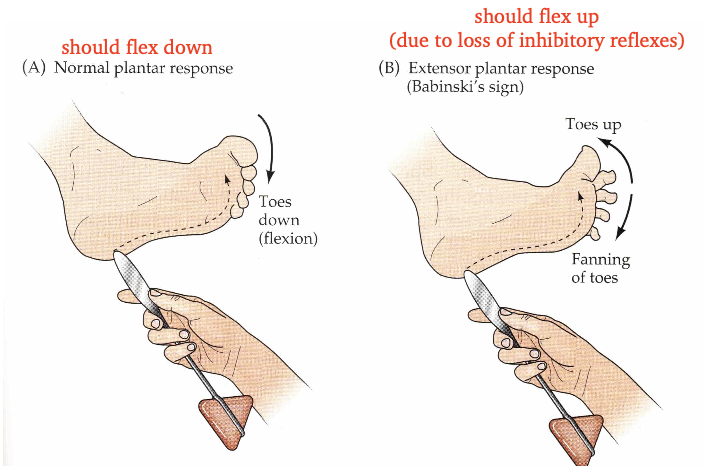
includes Babinski’s sign
Pyramidal Pathways
What does damage to LMN result in?
Flaccid paralysis
complete loss of function
decreased or absent reflexes
muscle atrophy
Pyramidal Pathways
What is Babinski’s sign?
→ indicates UMN damage to corticospinal tract
Anything that starts in cortex is _______. Anything that starts in the brainstem is _______.
Anything that starts in cortex is concious. Anything that starts in the brainstem is unconcious.
Extrapyramidal Pathways
List the Extrapyramidal pathways. What form of control do they have?
→ involuntary (unconscious) motor control on muscle indirectly via LMN (come from brainstem = involuntary)
Rubrospinal
Tectospinal
Vestibulospinal
Reticulospinal
What do the vestibular nuclei have inputs from?
inner ear and cerebellum
Where would you find UMN for the lateral corticospinal tract?
Where would you find cell bodies for LMN?
The axons travelling in area 1 are innervating what side of the body? If there was a lesion here, what effects would you expect to see?
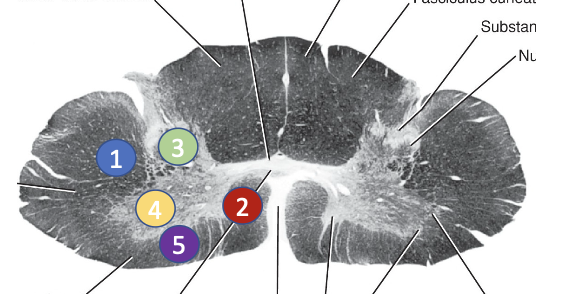
1) 1 (lateral corticospinal tract)
2) 4 (Ventral horn)
3) Right — spastic paresis of the right side of the body
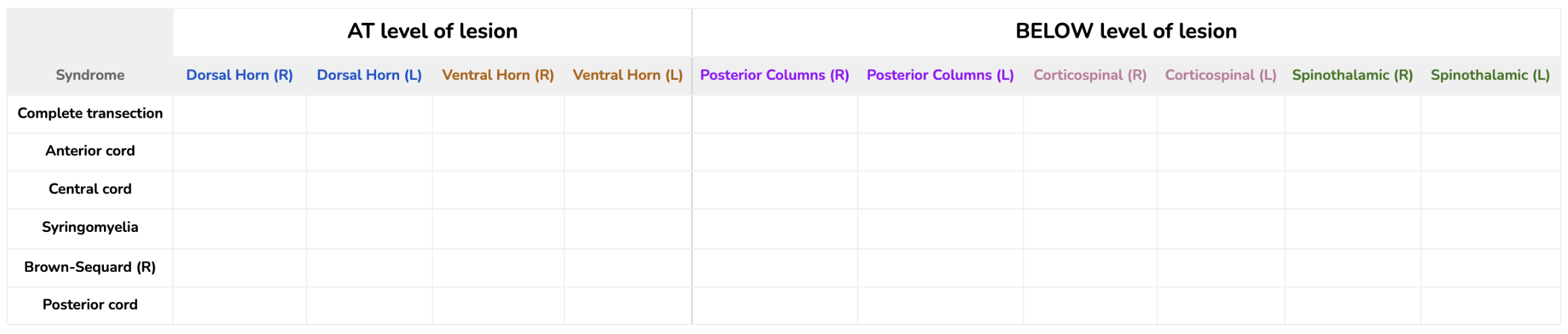
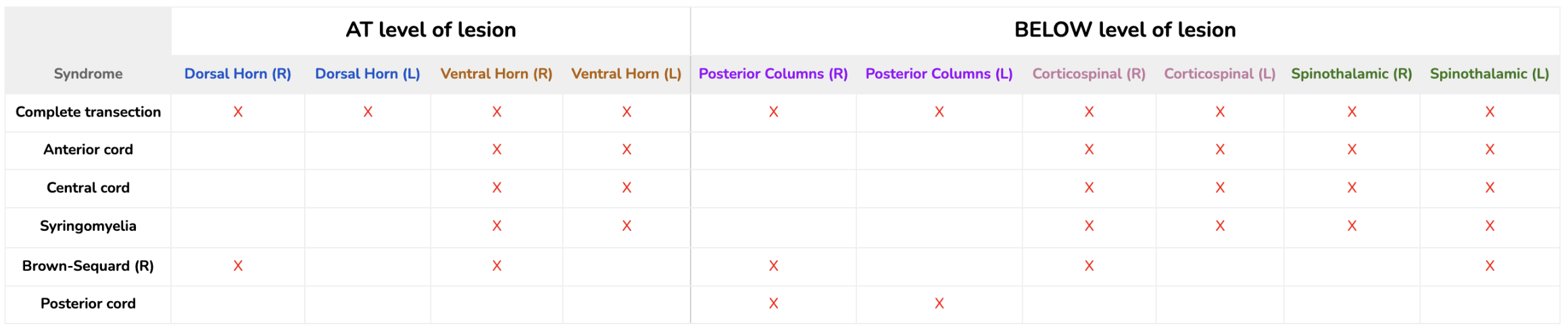
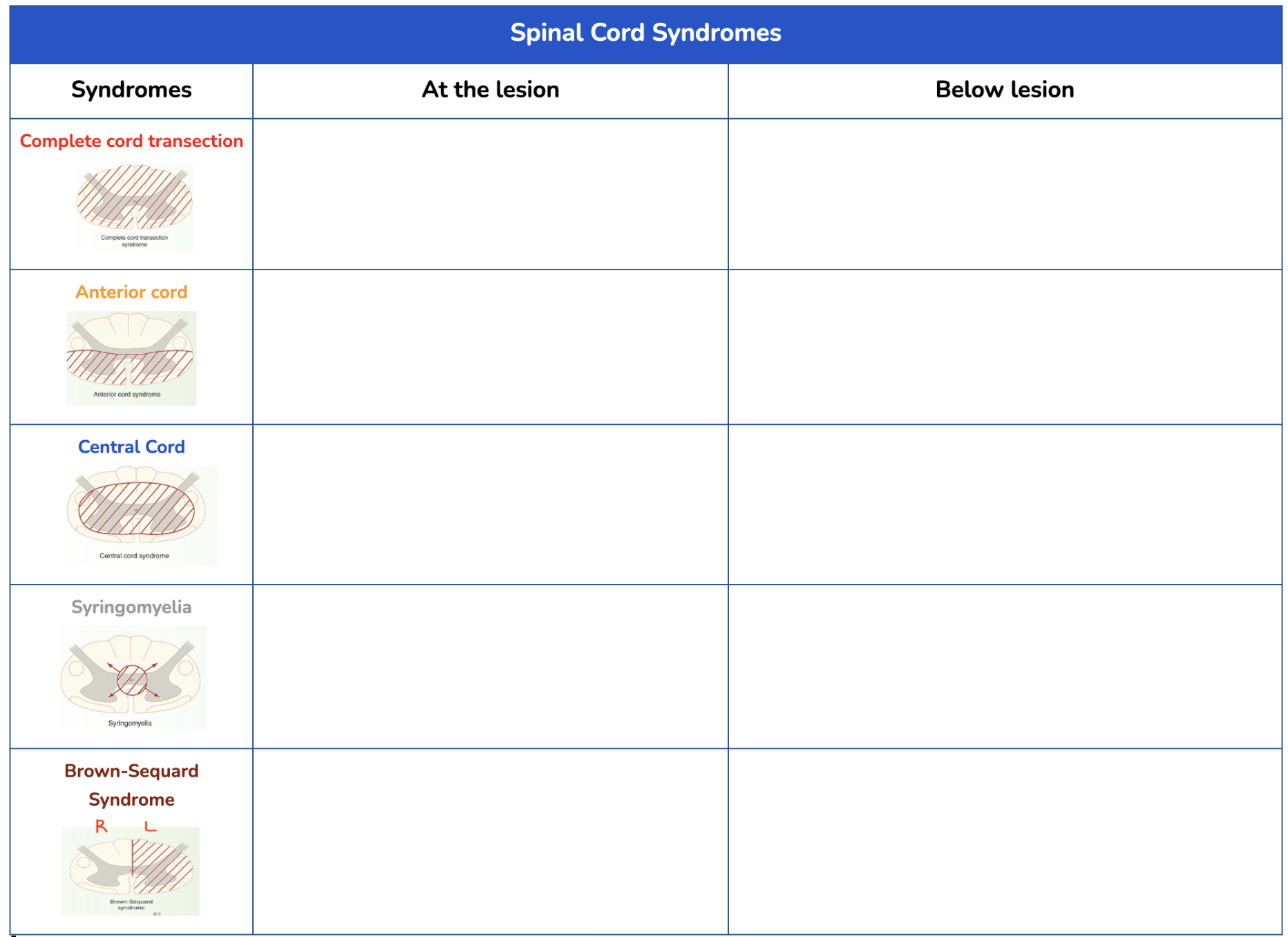
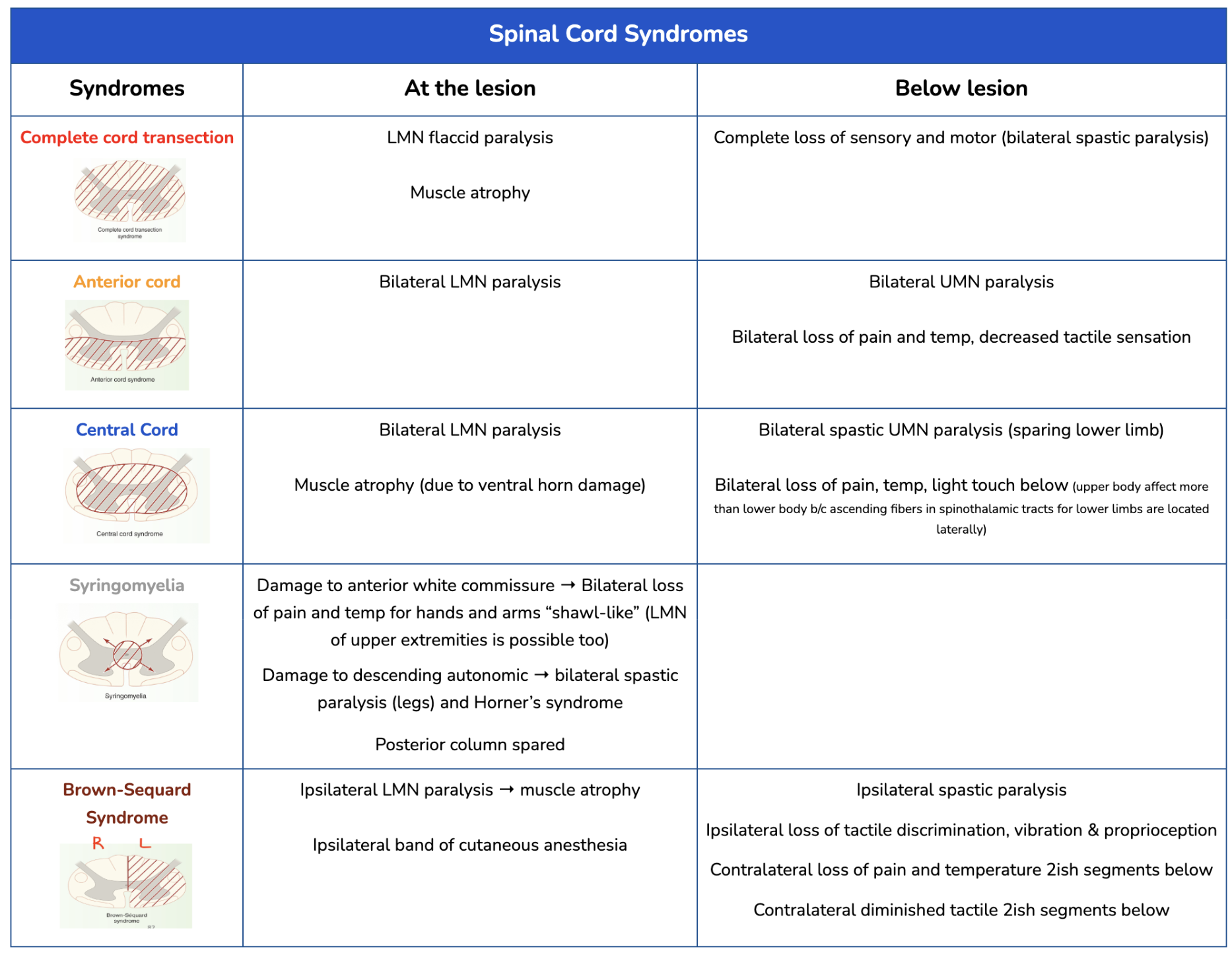
Spinal Cord Syndromes
Fill out the table on the Level of Lesion.
Spinal Cord Syndromes
Define Spinal Shock.
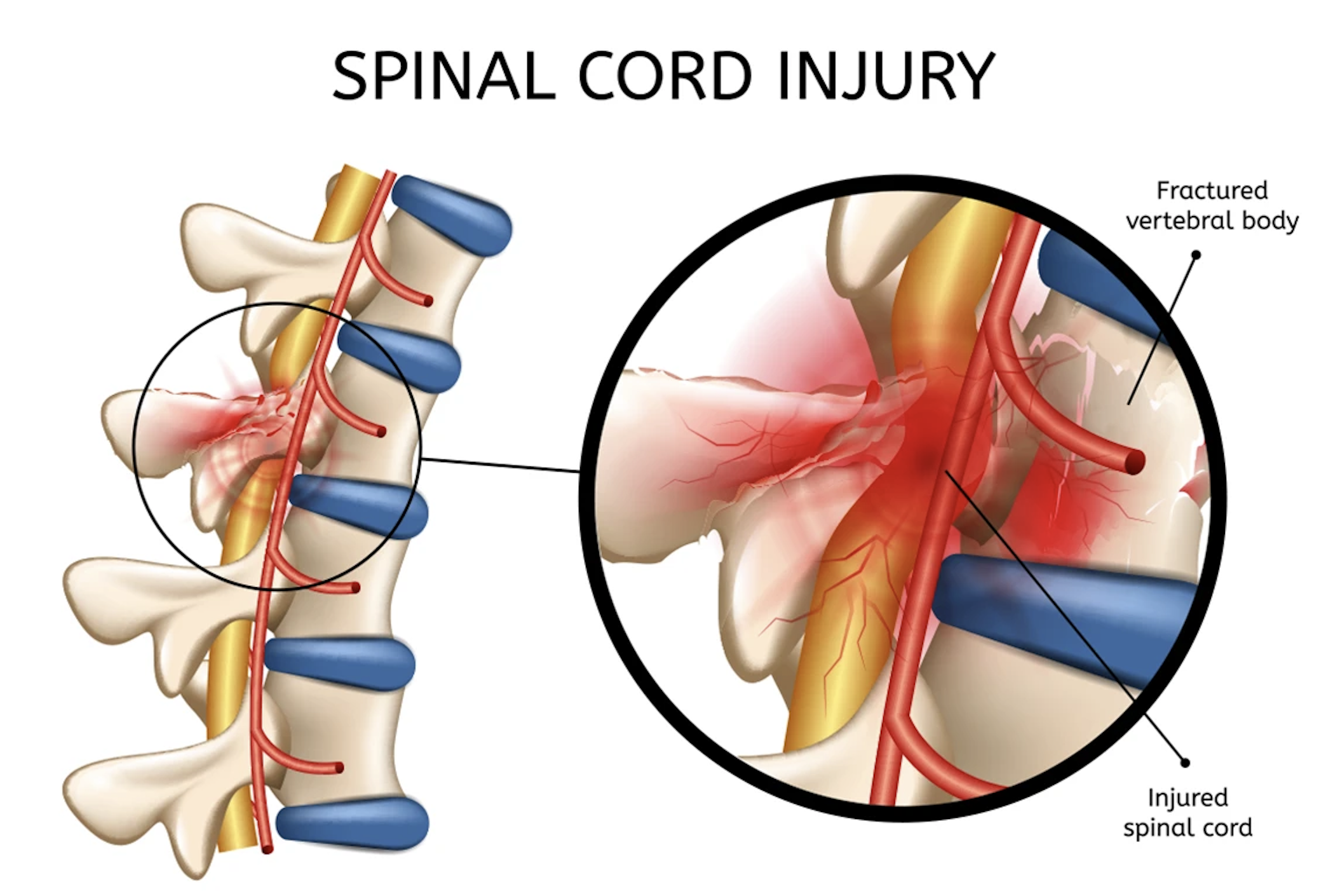
→ occurs right after severe injury to spinal cord (spinal cord is intact but it underwent trauma)
At the level = ❌ segmental spinal reflexes (due to spinal shock)
Below = ❌ sensory and motor function
→ as spinal shock wears off it develops into spasticity and hyper-reflexia
Spinal Cord Syndromes
Define Poliomyelitis.
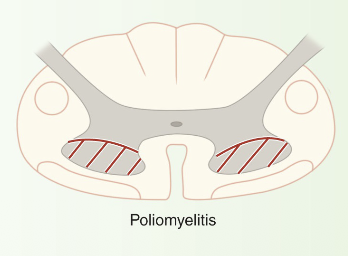
→ Viral infection that affect LMN in anterior/ventral grey columns
At the level: bilateral LMN paralysis (affects legs than arms)
Spinal Cord Syndromes
Define Multiple Sclerosis.
Demyelination of ascending & descending tracts
Spinal Cord Syndromes
Define Amyotrophic Lateral Sclerosis (ALS).
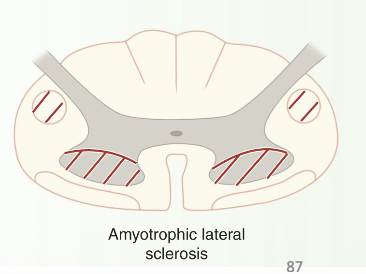
→ damage to corticospinal tracts and motor neurons in gray matter
At lesion: LMN signs
Below: UMN signs (ipsilateral → progress to bilateral)
Sensory is intact
Spinal Cord Syndromes
Define Posterior cord syndrome/Pernicious Anemia.
→ occurs due to B12 deficiency (can cause dementia and optic atrophy – if longstanding)
Damage to dorsal columns and peripheral nerves → Bilateral loss of conscious proprioception, 2 point tactile, pressure and vibration
Bilateral spastic paralysis occurs later with Pernicious Anemia
Pain and temp intact
Spinal Cord Syndromes
Define Neurosyphilis.
→ dorsal column syndrome
impaired two-point discrimination, vibratory sense, concious proprioception → difficulty walking
Note: motor pathways are intact