psyc335 midterm 2
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
history of ‘gambling addiction’ as a diagnosis
pathological gambling = first introduced in ICD-9 and DSM-3 → as an IMPULSE CONTROL disorder
DSM-5: renamed gambling disorder + moved to substance-related and addictive disorders category
‘problem gambling’ = used as a lower threshold (full criteria not met)
gambling disorder = new condition in DSM-5 and ICD-11
DSM-5 criteria of gambling disorder
4 or more of: symptoms and observable signs
a. pre-occupied with gambling
b. needs to gamble with increasing amounts [tolerance]
c. repeated attempts to reduce or quit gambling
d. restless or irritable when attempting to stop gambling [withdrawal]
e. gamble as means of escape or to alleviate mood
f. frequently returns to get even [loss chasing]
g. lies to conceal involvement
h. jeopardised/lost r/s or job due to gambling
i. forced to borrow money due to gambling debt
*exclusion criteria: not better explained by manic episode (bipolar disorder) → risk-taking and spending
loss chasing (desperate pursuit)
hallmark of point when casual gambling becomes problematic
‘a spiral of intensifying gambling until all financial options are exhausted’
can chase WITHIN and BETWEEN sessions (increase bet size/go back sooner)
withdrawal from gambling
physiological and psychological symptoms
approx 50% feelings of irritability and restlessness
2/3 gamblers reporting >1 SOMATIC symptom (nausea, shaking, sweating)
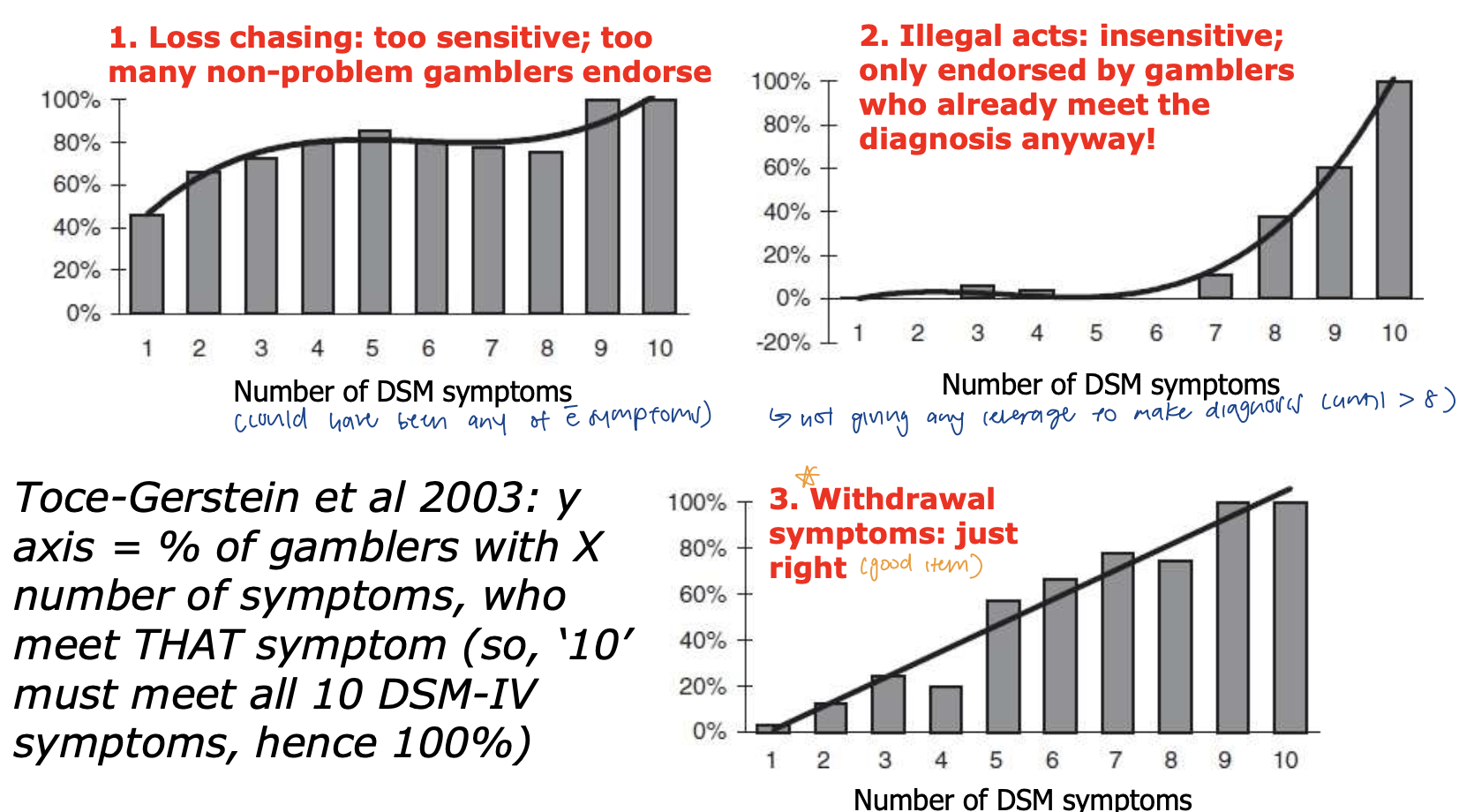
what is the inequality of items
loss chasing: too sensitive
too many gamblers say yes to it (even if they only have 1 symptom, 50% of the time its loss chasing)
illegal acts: insensitive
no leverage to make diagnosis until >8 symptoms
removed in DSM-5
withdrawal symptoms: just right
increases as gambling severity increases
5 pieces of evidence for re-classification into addictions category
symptom hallmarks (withdrawal, tolerance)
co-morbidities (other MH probs)
shared heritability/genetics (twin studies)
neuroimaging/neurocognitive similarities
effective treatments
DSM diagnosis of gambling problems
involves face to face INTERVIEW w clinician who is trained and qualified (expert judgement)
cannot be self-report questionnaire
2 short self-report tools for diagnosis
south oaks gambling screen (SOGS)
binary ratings, lifetime gambling
translated into many other languages → may be used in countries with little gambling research
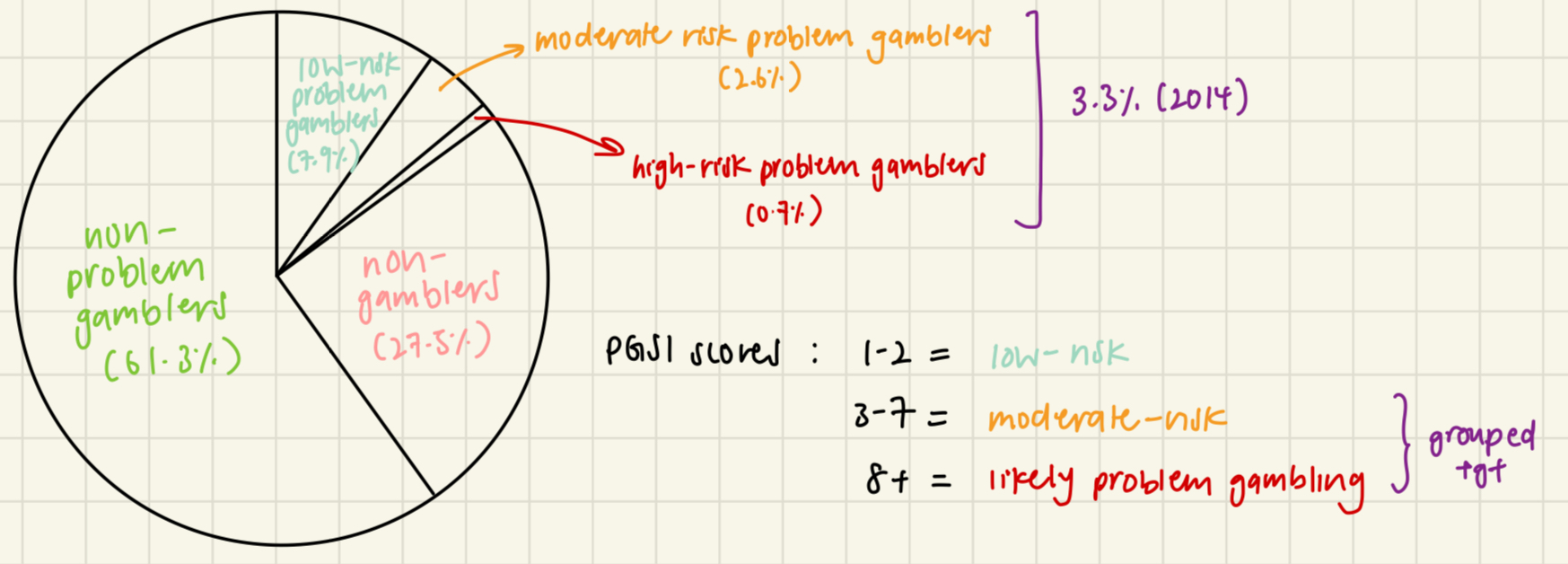
problem gambling severity index (PGSI)
gold standard; prevalence surveys
detects various LEVELS of PG
scores range from 0-27
NOT mapped directly to DSM criteria
poker players: length of time spend playing more harmful than financial losses
2014 BC prevalence survey (via PGSI)
telephone survey, n = 3058
“risk” implied likelihood of developing it in future VS actual meaning = currently have signs of gambling harm
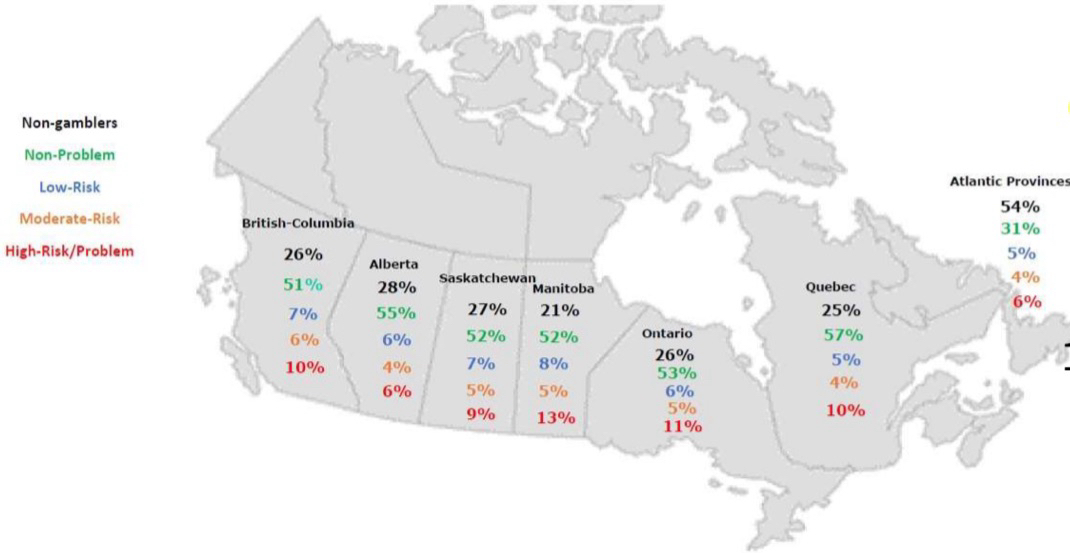
demographic predictors of gambling problems
robust factors → reliable across provinces
men
younger age (20s vs 50s/60s)
lower SES (hhld income)
racialized groups (indg ppl, asian communities, migrant communities)
other MH problems
*risk factors = statistical and NOT absolute
latest data (2024) MHRC online survey
n = 8211 adults
correlates to more ONLINE behaviour → not directly comparable
measure: PGSI
27% reported online gambling, 14% in last month
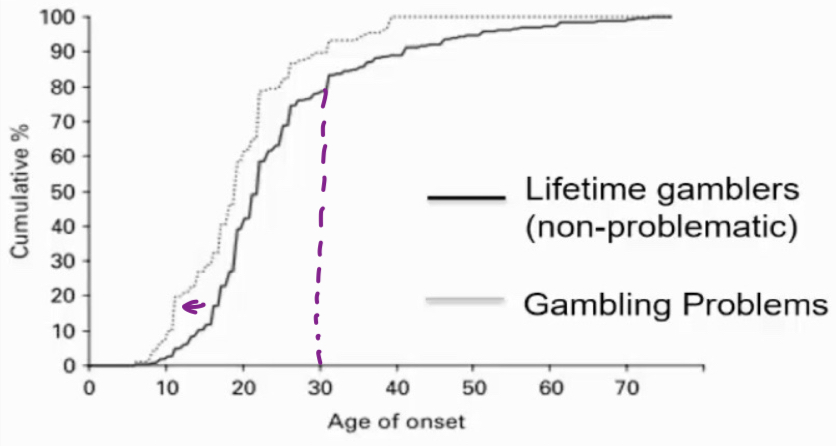
age of onset (“how old were you when you first gambled”)
78% lifetime gambling, 2.3% lifetime gambling problems (meeting more than 1 symptom on DSM)
earlier start to gambling = risk factor for future GP
start past 30 years = smaller likelihood of developing PG
gambling disorder as DEVELOPMENTAL
co-morbidities and temporal ordering
0.6% diagnosed w pathological gambling
¾ of them have co-existing drug problems
96% of them have any other DSM diagnosis
temporal ordering → which diagnosis came first
i. gambling first
financial strain, debt → anxiety, depression
ii. gambling second
to cope/escape negative emotions
evidence for this
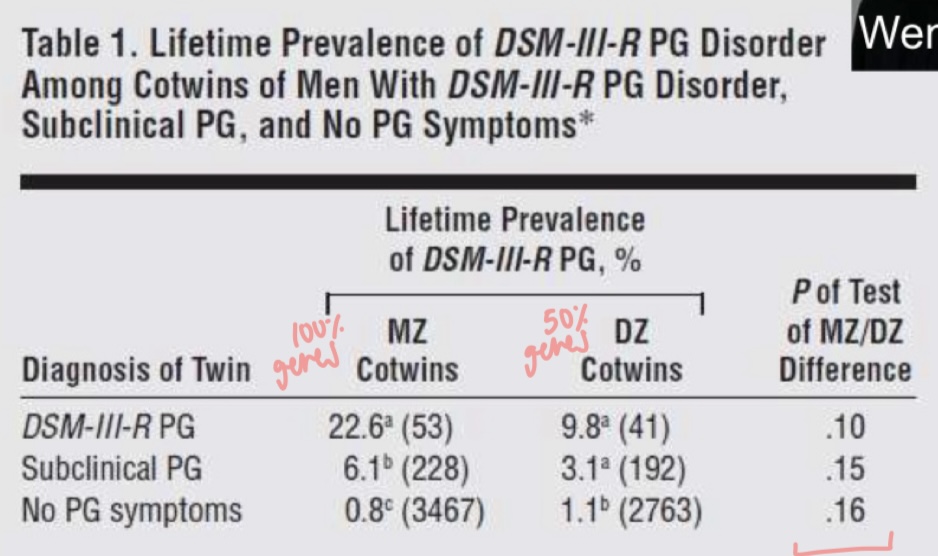
genes or environment (slutske et al study)
6744 twins from vietnam database (military sample of men)
environment same, no adoption involved
rate of lifetime PG diagnoses = 1.4%
any symptom = 6.2%
PG heritability = 40-50% (estimated from MZ-DZ disparity)
overlap in genetics of PG and alc dependence = 12-20% (addiction vulnerability)
environmental risk factors for gambling
exposure to parental gambling in childhood/adolescence
social learning theory/modeling
parental gambling PROBLEMS predicted child gambling problems (not parental gambling in general)
childhood adversity
adult sample: 61% reported childhood maltreatment
youth pathological gamblers: 20% reported physical abuse, 18% sexual abuse
*likely role of genes x environment interactions
5 main actors shaping gambling policy in BC
provincial gov
main proponent of expansion and main recipient of growing revenue
municipal gov
supportive of expansion as source of new rev BUT some opposed expansion due to neg effects
private gambling operators
lobbied for expansion
charities (e.g. bingo venues)
conflicted w provincial gov over dist of revenues
academic researchers
problematic types of legal gambling in canada
casino-based table and EGMs
non-casino EGMs and VLTs
single sporting event betting (legalized federally in 2021)
allocation of net gambling revenue
community chess model → gov = major provider + expanded availability of gambling
drives policy → more profitable than alc, tobacco and cannabis combined
revenue disproportionately taken from those who have problems with it → morally acceptable ?
reasons for needing a public health focused gambling policy
gov policies influence benefits and harms of gambling → availability/access, funding for prevention and treatment
harms and costs of PG mainly PRIVATE + hard to measure rel to benefits (revenue) → creates systemic bias toward expansion
4 main economic impacts of gambling
increased gov revenue
increased public services
increased regulatory costs (when expanding)
pos and neg impacts on non-gambling biz depending on whether complimentary/competitive w gambling
4 main social impacts of gambling
increased PG and associated harms (e.g. bankruptcy, suicide)
increased crime (except illegal gambling)
increased socio-economic inequality
more negative attitudes toward gambling
policy issues in canada
proportion of revenue from problem gamblers: approx 30% in canada
% rev dedicated to prevention, treatment and research
expansion of avail of casino games and EGMs (esp expansion in smaller centres)
rev from locals vs tourists
promotion and expansion of sports betting
treatment program limitations
hard to engage ppl who need the help
presence of stigma
expensive to promote and find those who need help
co-morbidities w other problems
*should aim to reduce stigma in order to help more ppl
gambling traditions in canada’s first nations
lahal ‘the bone game’
2 teams, played at social gatherings incl funerals + accompanied by gambling songs
element of perception → trick opponent to guess the wrong hand that the bone is in
nowadays: ‘pot’ won might b based on entry fee → traditionally valuable items put up by hosts (resources)
similar to lukuchuko
westernization of indigenous gambling
11% of sample participated in traditional first nation games in past year
only 25% considered them to be gambling
‘gambling’ term connected to western, commercial forms, disconnected from traditional games
non-commercial games w no house-edge VS modern commercial games (neg consequences arise from house edge)
gambling revenue from people with gambling problems
profits concentrated among pop of problem gamblers → contribute DISPROPORTIONATELY to gambling revenue
calc use prevalence estimates of PG rate
questionnaire estimates of typical monthly spending on gambling (inaccurate self-report)
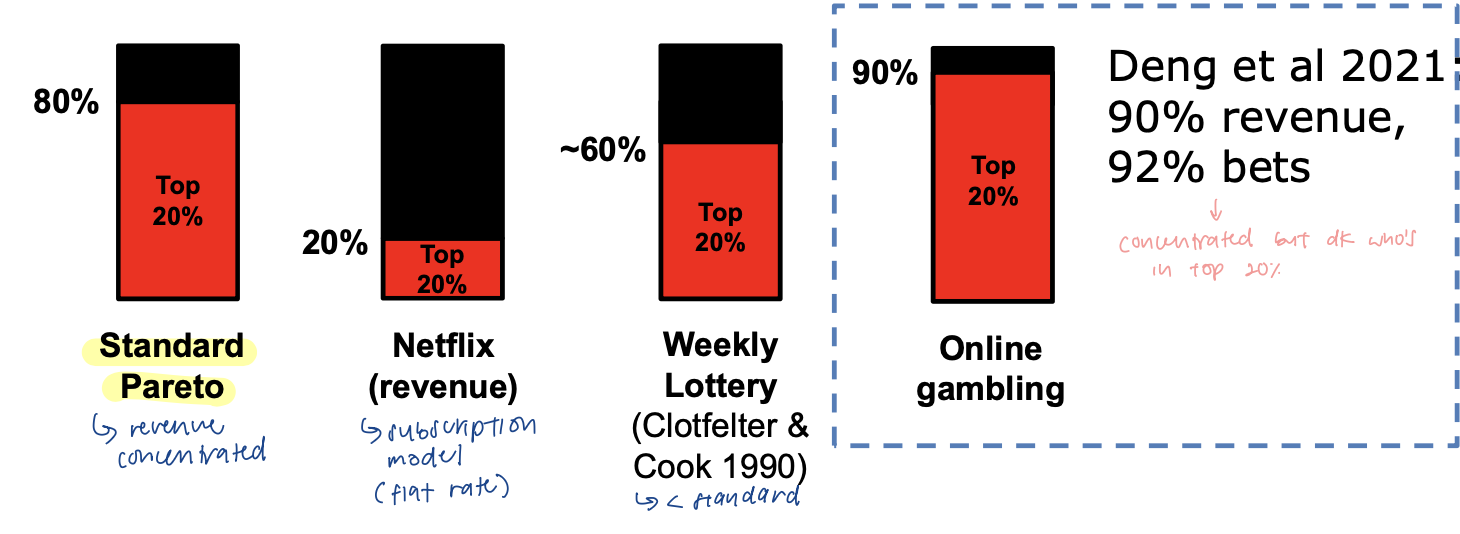
‘hyper pareto’: gambling conc in a small number of whales (very profitable customers)
standard pareto: rev conc in top 20% of users (80%)
netflix: subscription model (flat rate)
weekly lottery: top 20% = approx 60% of rev
online gambling: top 20% = 90% of revenue, 92% bets
exact record of what each gambler spent → hard to get diagnosis data on PG
indigenous gambling and PG in canada
data from 2018 canada community health survey
rel popularity of gambling (basic involevement) FAIRLY SIMILAR to non-indigenous canadians
some elevation for EGMs, bingo, instant lotteries
rate of PG MUCH HIGHER among indigenous canadians (2.0%) vs 0.5%
highest of any racial/ethnic grp in canada
BC youth data for gambling
BC adolescent health survey 2018
21% of BC youth aged 12-18 gambled for money in past year
youth employment 20+ hrs per week linked to gambling for money → access to disposable income
involvement in sports on weekly basis associated w sports betting
monthly gambling → sedentary lifestyle, less social connection, excessive tech use
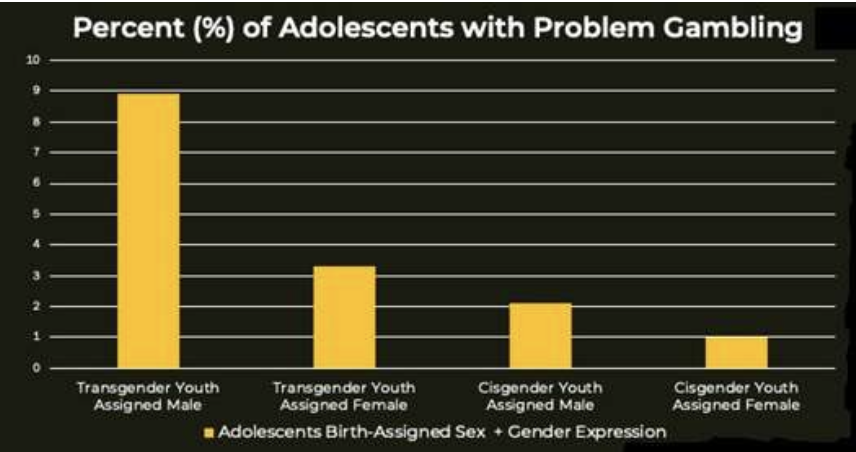
gambling problems in 3% of those who gambled → highest in NON-BINARY youth
gambling and gender identity
non-binary gender: 2.7%
youth identifying as non-binary showed HIGHER rates of PG 5.7% vs 1.8% → esp transgender youth assigned male at birth
interaction b/w biological sex and gender identity
intersectionality definition
overlap of social identities
ppl may identify w multiple under-represented and or marginalized grps at the same time
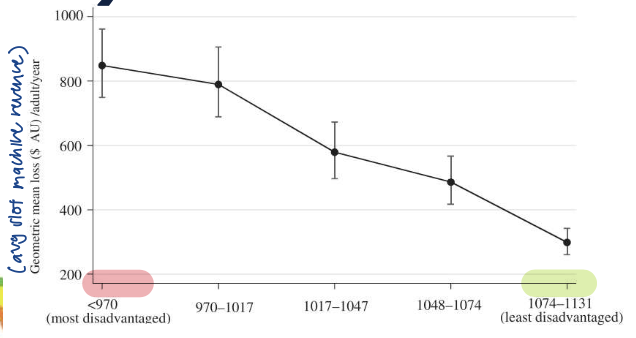
geospatial analysis of SES (aus study)
in lower SES neighbourhoods:
higher losses (higher slot machine revenue)
more slot machine venues
for lottery too
businesses want to open more gambling sites in less affluent areas → not randomly distributed
diversity in the gambling research field
‘gender gap’: can be measured in academic papers from inferring first names (gender neutral names excluded)
senior authors more likely to be men
researchers who were men published 16% more papers overall
stronger gender bias for gambling papers than non-gambling ones → reflects systemic biases against women in academic careers
key points of disproportionate gambling effects
on many racialized and minoritized groups
ppl who are socio-economically disadvantaged
high income grps spend MORE on gambling but lower income grps spend a GREATER PROPORTION of their income → experience more financial harm
ppl w gambling problems account for a disproportionate slice of revenue (~20-40%)
**high levels of gambling lead inevitably to financial strain and debt → can further amplify social inequalities (vicious cycle)
^for commercial games w built-in house-edge
3 distinct theoretical approaches to gambling and PG
psychodynamic account (freudian)
behavioural account (conditioning, learning)
cognitive account
theory 1: psychodynamic account
bergler: PG as MASOCHISM → unconscious desire to lose (to punish yourself)
driven by denial/rebellion against parental authority → rejecting values of family unit hence driven to humiliate themselves
limitation: UNFALSIFIABLE (cannot be tested)
recognizes that PG not necessarily abt WINNING money → but rather obsessed with losing
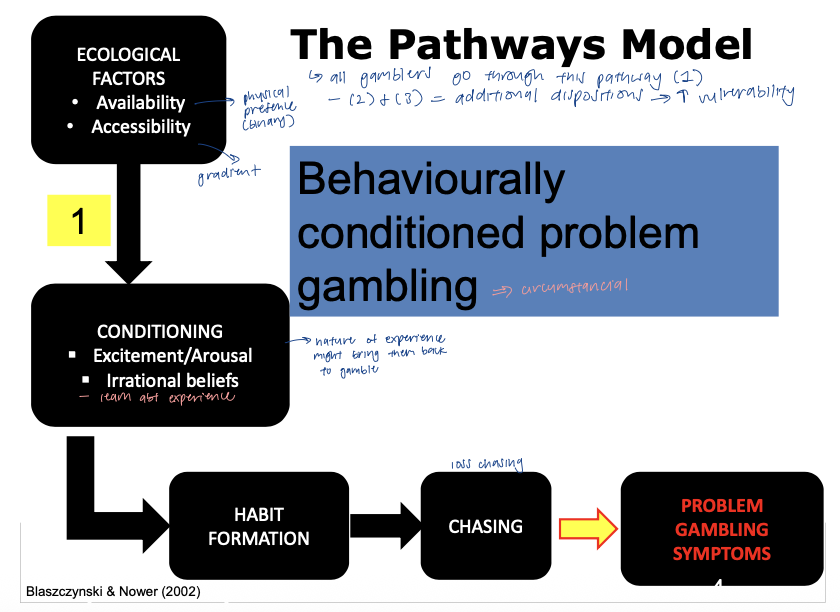
pathways model
proposes 3 subgroups of and routes into PG
specifies key roles for conditioning, arousal, cognitions, depression/anxiety, neurobiology and impulsivity
pathways model: pw 1 [behaviourally conditioned PG]
all gamblers go through this pathways (final common pw)
ecological factors (availability and accessibility) → conditioning (excitement/arousal from experience) → HABIT FORMATION → (loss) chasing → PG symptoms
may not have vulnerability factors but happened to be at the wrong place at the wrong time
can occur at any age
pathways model: pw 1 evidence
early ‘big wins’ in first experiences w gambling → predictor of PG in future
retrospective interviews (turner 2006)
social gambler (casual w no symptoms: $139 first win (0%)
subclinical (@ risk): $499 first win (12%)
pathological: $620 (26%)
powerful one trial conditioning event + skews expected value calculations
e.g. getting a job at a betting shop w no prior inclination to gambling → want to practice tips picked up (wrong place at the wrong time)
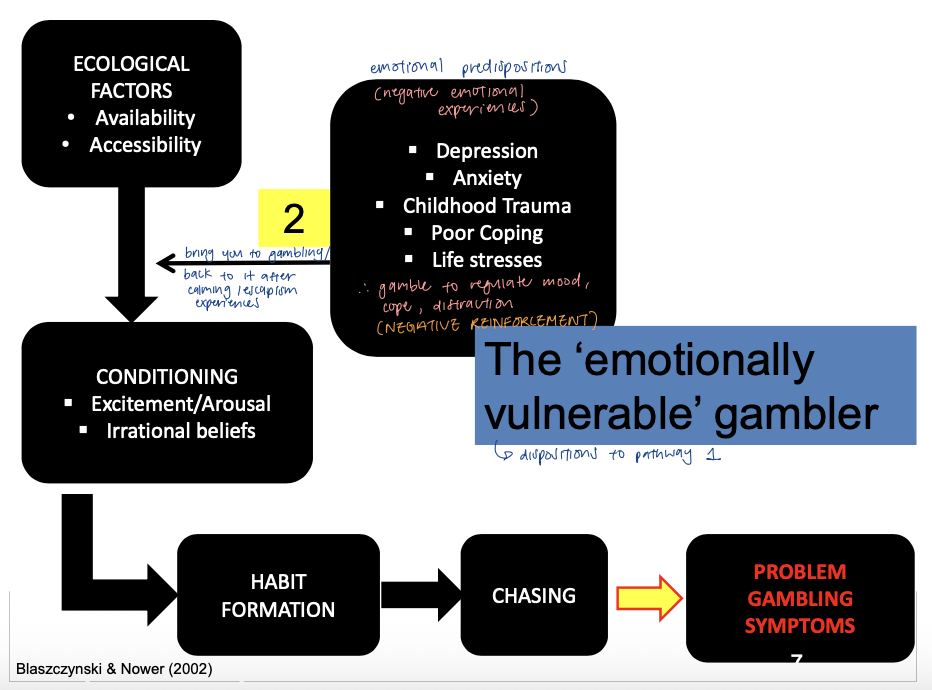
pathways model: pw 2 [the ‘emotionally vulnerable’ gambler]
piggyback onto first pathway (dispositions present)
posits an emotional disturbance that predisposes gambling engagement and persistence
emotional predispositions (depression, anxiety, childhood trauma, poor coping, life stresses) - negative reinforcement → gamble for first time OR bring you back to gambling → conditioning → habit formation → chasing → PG symptoms
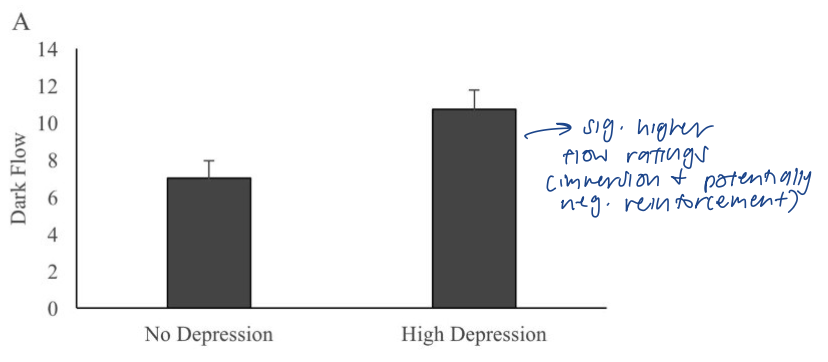
pathways model: pw 2 evidence
depression and ‘dark flow’
study on casino visitors: depressed group had sig HIGHER flow ratings → immersion and potentially negative reinforcement
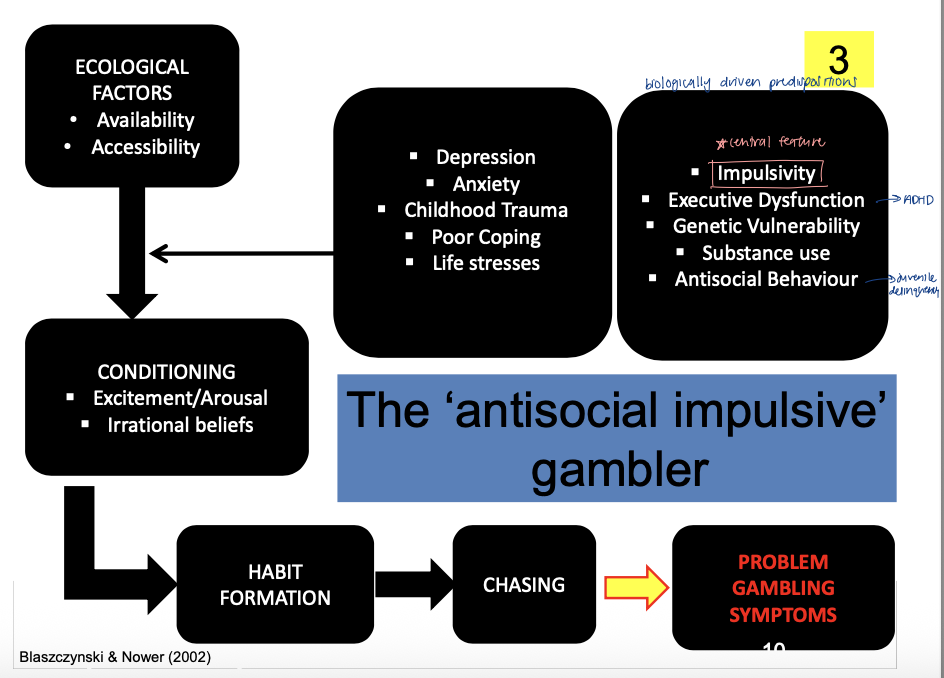
pathways model: pw 3 [the ‘antisocial impulsive’ gambler]
biologically driven predispositions
gambling commences at early age, rapidly escalates in intensity
IMPULSIVITY (+ executive dysfunction, genetic vulnerability, substance use, antisocial behaviour) → gamble for first time OR bring you back to gambling → conditioning → habit formation → chasing → PG symptoms
pathways model: pw 3 evidence
impulsivity as the ‘addictive personality’
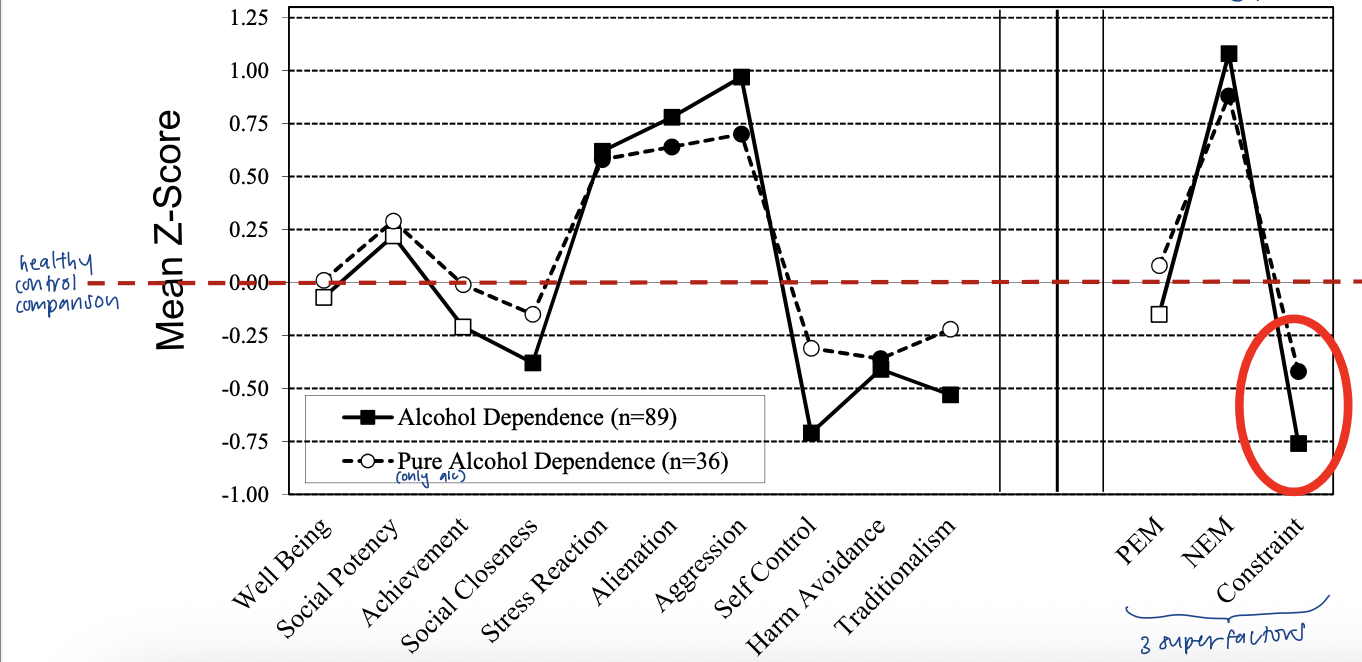
prospective design (long-drawn; across time) using Dunedin birth cohort
multidimensional personality questionnaire (MPQ) at 18yrs old
3 superfactors: negative emotionality (neuroticism), positive emotionality (extraversion), constraint (opp of impulsivity)
drug use and gambling assessment at 21yrs old
alc dependence (10%), cannabis dependence (9%), nicotine dependence (18%), gambling problems (6%)
pathways model: pw 3 evidence (personality profile)
personality/risk profile for: (similar pattern across)
alcohol problems
cannabis dependence
problem gambling
*low constraint (high impulsivity), high neg emotionality (proneness to stress), positive emotionality (no predictive value)
testing the pathways model
TYPE THEORY: puts ppl into 3 diff categories (often turns out to be dimensions/traits instead)
reasons for long length of model
measurement is tricky due to many components + hard to test
complex statistics for testing types, require large samples
3 cluster solution
pw 1 (44%), pw 2 (40%), pw 3 (16%)
pw 3 CLEARLY DISTINCT from pw 2 → distinct vulnerabilities (independent)
gambling in parkinson’s disease
L-dopa (standard pharmaco treatment) turns into DA/precursor for DA
DA agonist meds can trigger EXCESSIVE gambling
most linked to 2 drugs: pramipexole and ropinirole → bind to DA D3 receptors
constellation w other impulse control/reward problems (sex-related)
men: hyper-sexuality
women: compulsive shopping buying
drug stimulating DA → drives gambling problems
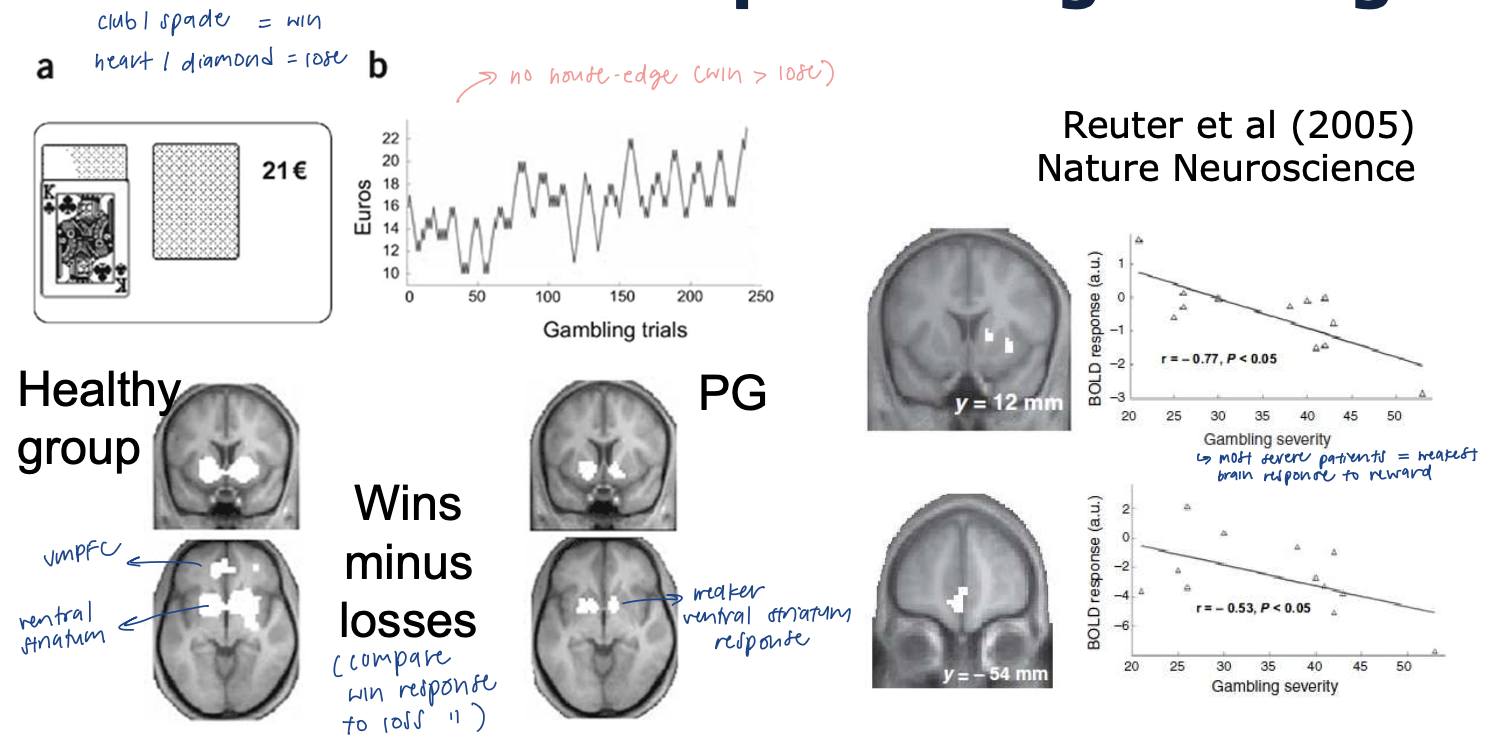
fMRI of reward in PG (case control design - 1 illness grp, 1 no illness)
task w no house-edge (win > lose)
reduced striatum and vmPFC reward activity in PG → corr w gambling severity
HC: strong response to reward
PG: most severe patients = weakest brain response to reward
supports reward deficiency hypothesis (underactive system)
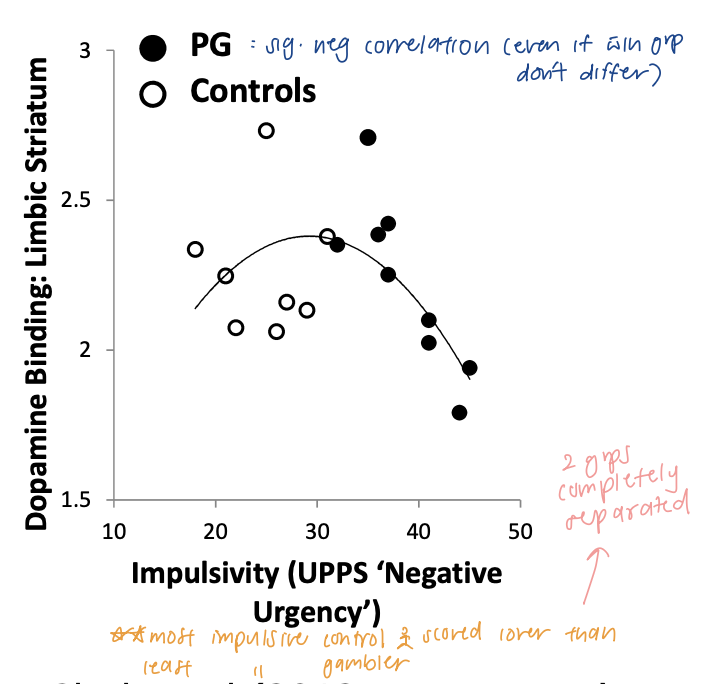
DA PET binding in gambling disorder
hypothesis: reduced DA binding in grp w gambling disorder (not seen)
NO grp diffs in extracted DA D2 in striatum but related to trait impulsivity
most impulsive control person scored lower than the least impulsive gambler → 2 groups completely separated
PG: sig neg correlation
** DA very sensitive to age
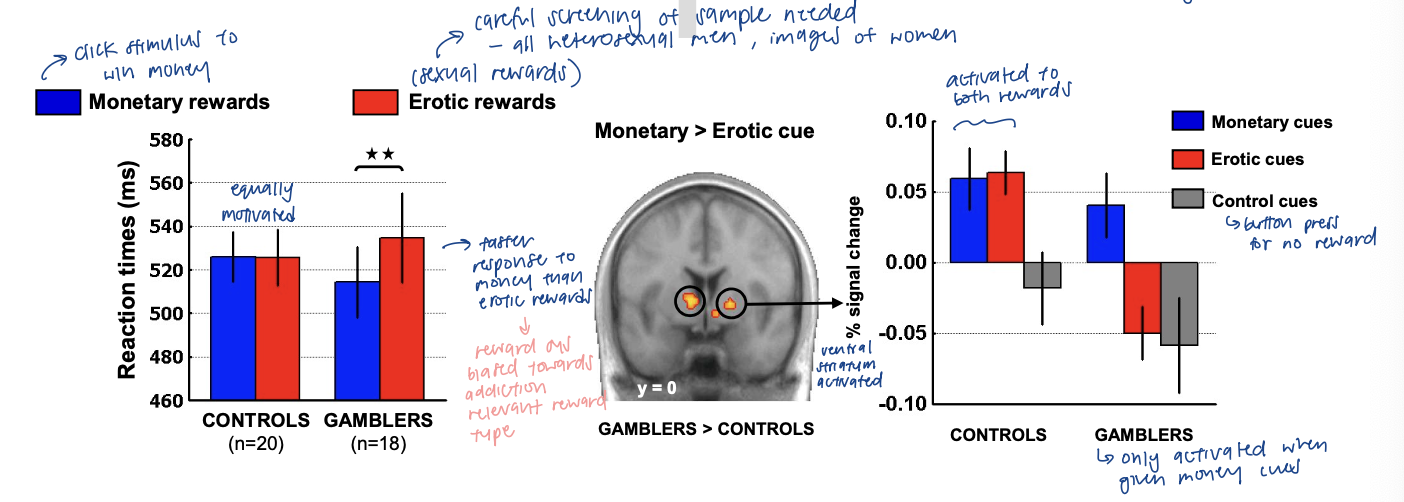
fMRI to natural rewards
**winning money = addiction relevant reward
task: response time to earn monetary reward or sexual reward
men w gambling disorder: IMBALANCED response to gambling-related ($) vs natural (sexual) rewards
gamblers: faster response to money than erotic rewards → reward sys BIASED toward addiction relevant rewards
control: no diff
SAME pattern in ventral striatum response
controls: activated to both rewards
gamblers: only activated when given money cues
reward repertoire shrinks to only target of addiction vs HC w many diff things we get reward from
both reward deficiency and incentive salience happening ??
BC resources for gambling problems
telephone helpline (gambling support) → not needed to be gambler themselves
voluntary self-exclusion program → gamblers block themselves from casino and online gambling access
no contact incl lack of treatment options
who’s responsible if somehow allowed back in (legal issues)
‘responsible gambling’ tools like limit-setting options → e.g. limit to gamble in a month
psychological treatment → free counselling programs
financial support (debt management loans), family therapy
no residential facilities for gambling in BC → expensive
2 forms of psychological treatments
cognitive-behavioural therapy (CBT) → most dominant
C: testing and restructuring false beliefs (distortions)
write what person is thinking → challenge that belief
B: exposure (imagined at first) and desensitization
conditioning: take client to casino foyer → flooding for phobias
feed into each other → cannot be independently used
motivational interviewing (MI) / enhancement
enhancing motivation to CHANGE, exploring AMBIVALENCE (pros and cons of gambling)
assessing ‘change talk’: are the pros really beneficial → move them along change continuum
any treatment most effective when client is motivated to change their behaviour → MI used in combination w other therapies
many drop out prematurely
*many open questions on effectiveness
indiv vs group setting
in-person vs online delivery
(complete) abstinence vs controlled gambling
anonymous programs vs not complete removal of gambling/returning to previous state
pharmacotherapy for gambling disorder (medications)
placebo vs drug trials
measure symptom severity
classes of drugs: opioid, serotonin, dopamine
opioid medications have the best results → block opioid receptors (drug 2x better than placebo)
serotonin (SSRIs, anti-depressant meds) → not effective 68% drugs, 66% placebo
dopamine (treat schizophrenia) → placebo more effective than drug
from placebo-controlled trials: most promising meds = opioid antagonists → REDUCE URGE (to gamble) + CRAVINGS
reasons for variability b/w placebos
diff duration of treatments
background of study (education, no response, MI)
biggest issue w treatment
even though treatment = FOC and good quality …
few people w addictions actually seek help
awareness of programs + how to access
stigma surrounding admitting harm and consequences
bijker et al (2022) systematic review and meta-analysis of prevalence of help seeking for gambling
moderate-risk gamblers: 3.7%
problem gambling (highest classification on PGSI): 20.6%
1 in 25 moderate-risk gamblers and 1 in 5 ppl w PG have sought help for gambling related problems
theory 2: behavioural account (learning)
gambling and pavlovian conditioning
cues associated w gambling should become CS → visual stimulus of casino lobby (smells, colours, sounds)
reward salience
DA involved in this learning
theory 2: behavioural account - gambling cues and craving in the brain
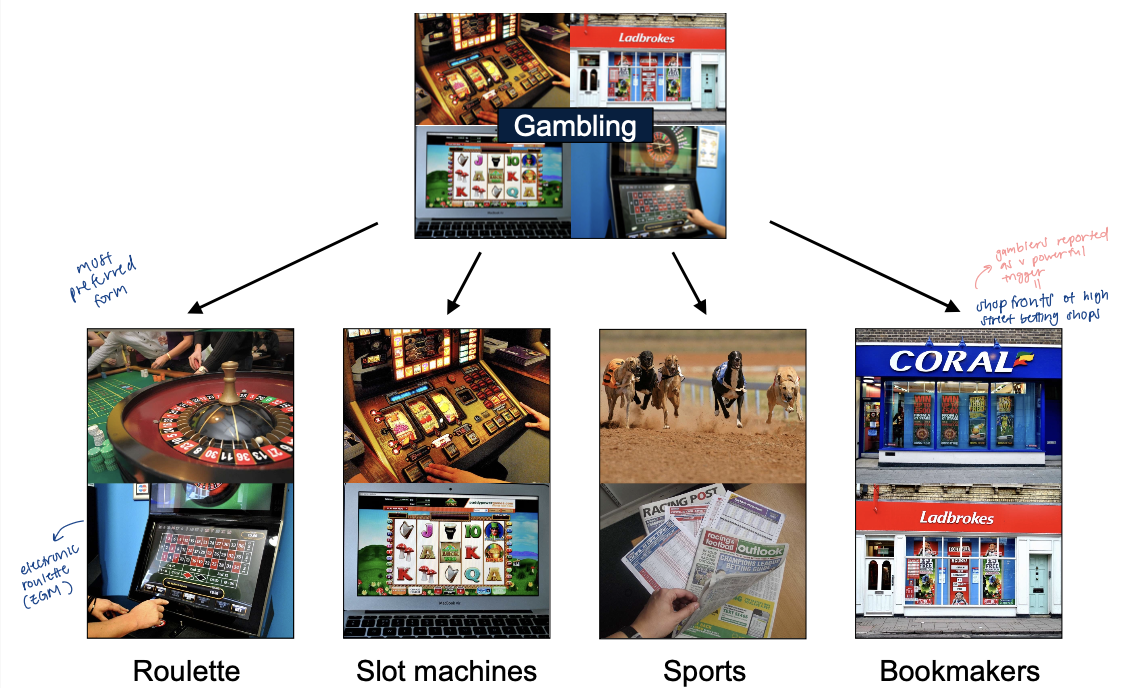
UK: clinic patients majority men vs much less skewed in vancouver
gambling culture differences and gender norms
only men recruited bc thought not enough women to do stats by gender
gambling cues TAILORED to preferred games of each participant
vs smoking (generic cues)
shop fronts of high street betting shops → powerful trigger for gamblers
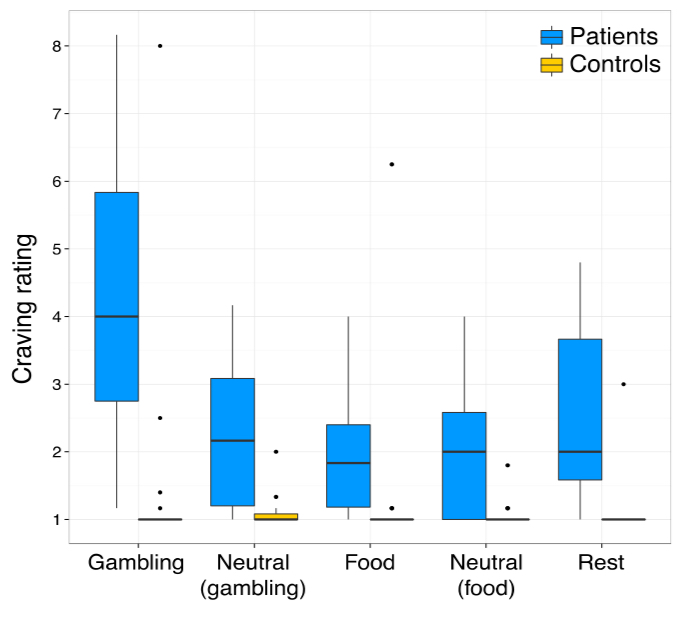
used highly appetizing food images to test whether other reward processing altered
took CRAVINGS rating after each block of images (during brain scan)
analyzed brain connectivity changes (striatum as ‘seed’ region) + simple contrast analysis
results of gambling cues and cravings study
2 sets of neutral images used → some visually matched to gambling images (same colours and visual complexity), others matched to food images
HC: at lowest levels
gambling disorder: increased craving ratings overall → ESP after blocks of gambling images (cue reactivity)
fMRI analysis - gambling cues
all subjects: gambling cues - neutral cues → brain activity: frontal lobe, striatum, visual cortex
interaction test: brain areas more responsive to gambling cues (vs neutral cues) in GD MORE than in HC → insula, medial PFC
correlation w craving (gamblers): areas where brain activity to gambling contrast correlate w craving intensity → INSULA (bilaterally - both hemispheres)
more activity = more craving in gamblers (pos correlation)
neuropsychology on INSULA and craving
study on stroke patients who used to be smokers (medical records)
if stroke affected INSULA → more likely to spontaneously quit
no cravings/urge to smoke
forgot they used to smoke (not amnesia)
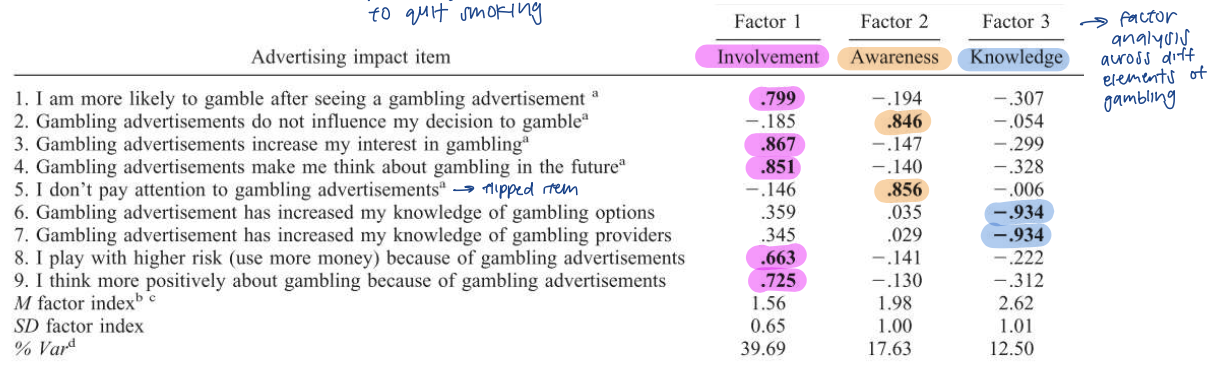
gambling advertisement (classical conditioning)
packed w learned cues tho now banned and heavily regulated
3 factors: involvement, awareness, knowledge
factor analysis across diff elements of gambling
results:
involvement: grp w PG show STRONGER impact of ads
involvement and knowledge: younger age and men had higher scores
theory 2: behavioural theory (operant conditioning) and role of arousal
gambling = operant response that SOMETIMES results in a win → potential for POSITIVE REINFORCEMENT
skinner’s schedules of reinforcement
fixed interval: 1 reward avail every 10s → e.g. salaries at end of month
variable interval: unpredictable interval → e.g. songs on radio
fixed ratio: 1 prize every 10 presses
variable ratio: unpredictable reward (unsure which bet is going to win) → e.g. slot machine/gambling
VR schedules characteristics
ratio schedules yield HIGHER RATES of response than IS → can ‘slack off’ after reward received
VR schedules: HIGHLY RESISTANT TO EXTINCTION → persistent
uncertainty = key to effect
not easy to establish for animals → trng required to get animal to that point (built up)
early ‘big wins’ may be a key conditioning event
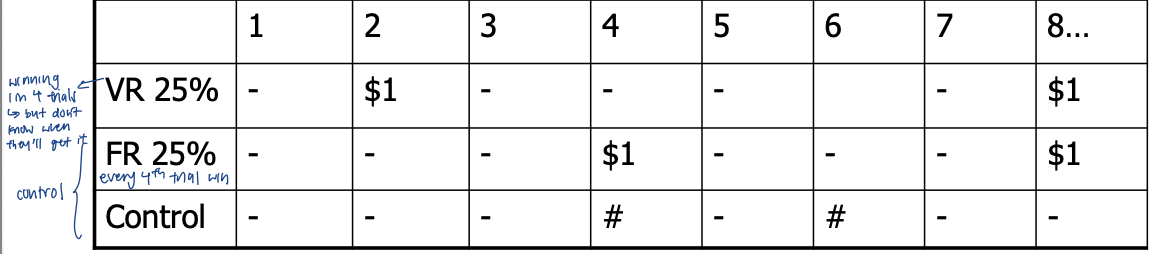
DA release (raclopride PET) to unpredictable rewards
long boring task (task releasing natural DA → competes w radio tracer at receptors; reduce PET signal via competition)
VR minus control: increase DA in L striatum
FR minus control: no sig DA release
*only PET scan during task
effects of uncertainty on DA cell signals
DA cell activity during appetitive pavlovian conditioning (purple squiggle and fruit juice)
5 stimuli w diff probabilities of reward
not always tied to juice BUT cue learning still exists (CS response) → DA cell activated during the “pause” (unsure if getting reward)
at peak uncertainty (0.5) → CS + anticipatory activity in pause b/w CS and juice
surplus DA activity (double hit)
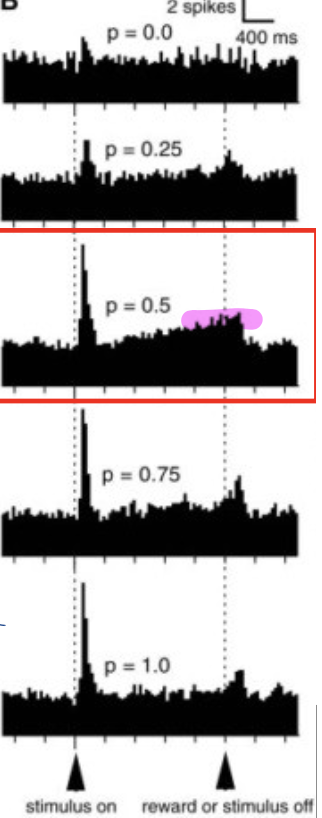
gambling and hyper-learning (double hit)
evidence for pavlovian cue learning in gambling
uncertain rewards: both cue learning AND anticipation (additional activity during delay period) → potential DA double hit created
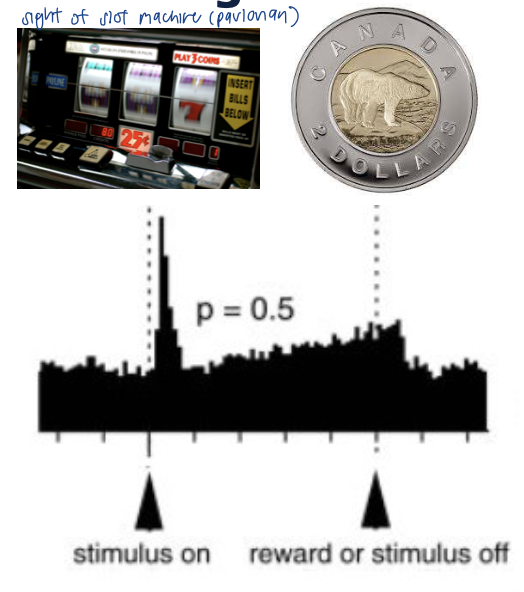
“its all about the pause” - how gamblers describe playing slot machines
neg reinforcement: gamble to alleviate neg emotions, relieve stress/low mood/boredom
pos reinforcement: winning, cheering
physiological arousal during gambling play
excitement = commodity that gambler is prepared to pay for (source of UTILITY)
psychophysiology of blackjack (measure HR change)
measure HR change from baseline
substantial HR INCREASE → biggest change = 55bpm (intense cardio level)
mostly in casino setting → need for ECOLOGICAL VALIDITY
when replicated in lab → not as intense changes in HR
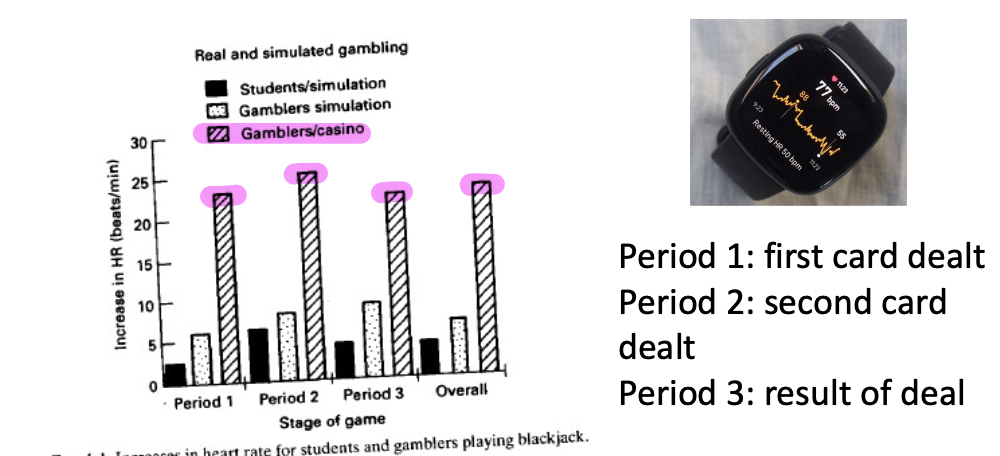
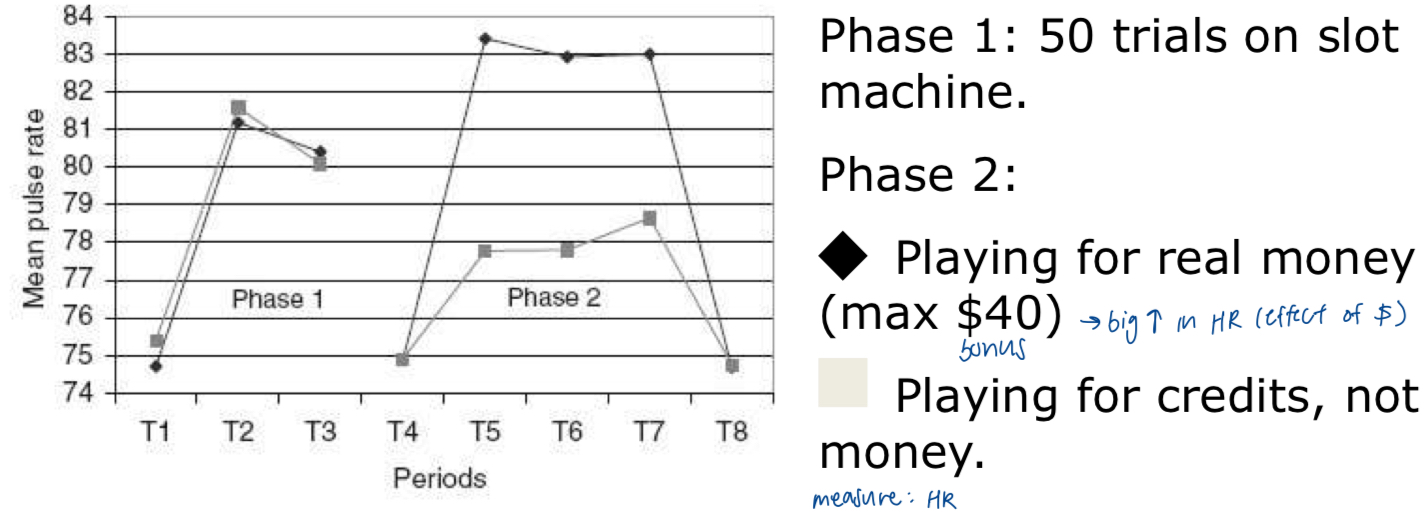
monetary bet/prize as prerequisite for physiological arousal
playing for real money → big INCREASE in HR compared to just playing for credits
processing of physiological arousal
physiological changes (SIGNAL) → detection of that change (INTEROCEPTION) - insula → COGNITIVE APPRAISAL (do you like that feeling)
lots of studies on PG measured SIGNAL but inconsistent findings
cognitive appraisal theory of emotion
capilano bridge study
misattribution of cognitive responses as other feelings (e.g. romantic attraction)
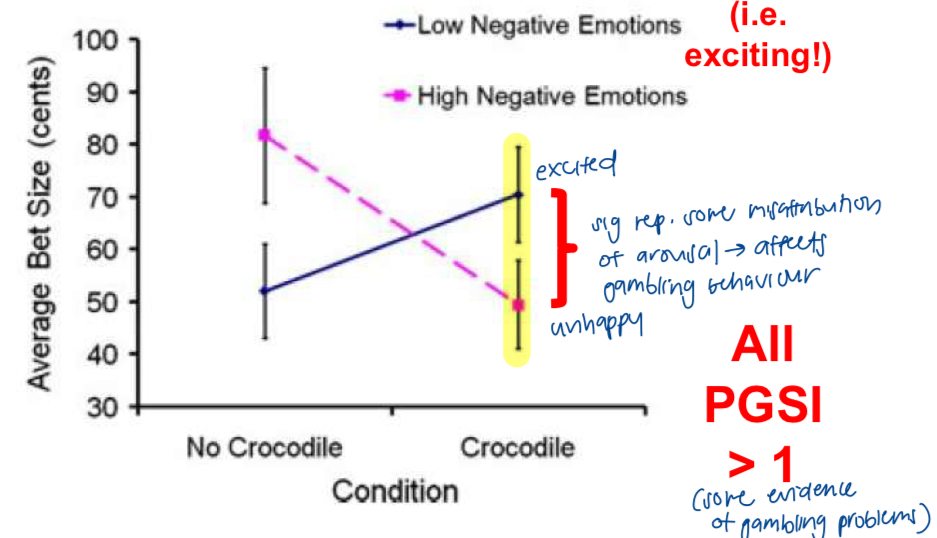
capilano bridge of gambling
slot machine gamblers (PGSI >1) visiting australian crocodile sanctuary
aim: cognitive appraisal → not physiological arousal directly
play at entry foyer OR after holding baby croc for awhile
measure: emotion rating scale
crocodile grp: significant difference reps some MISATTRIBUTION of arousal → affects gambling behaviour
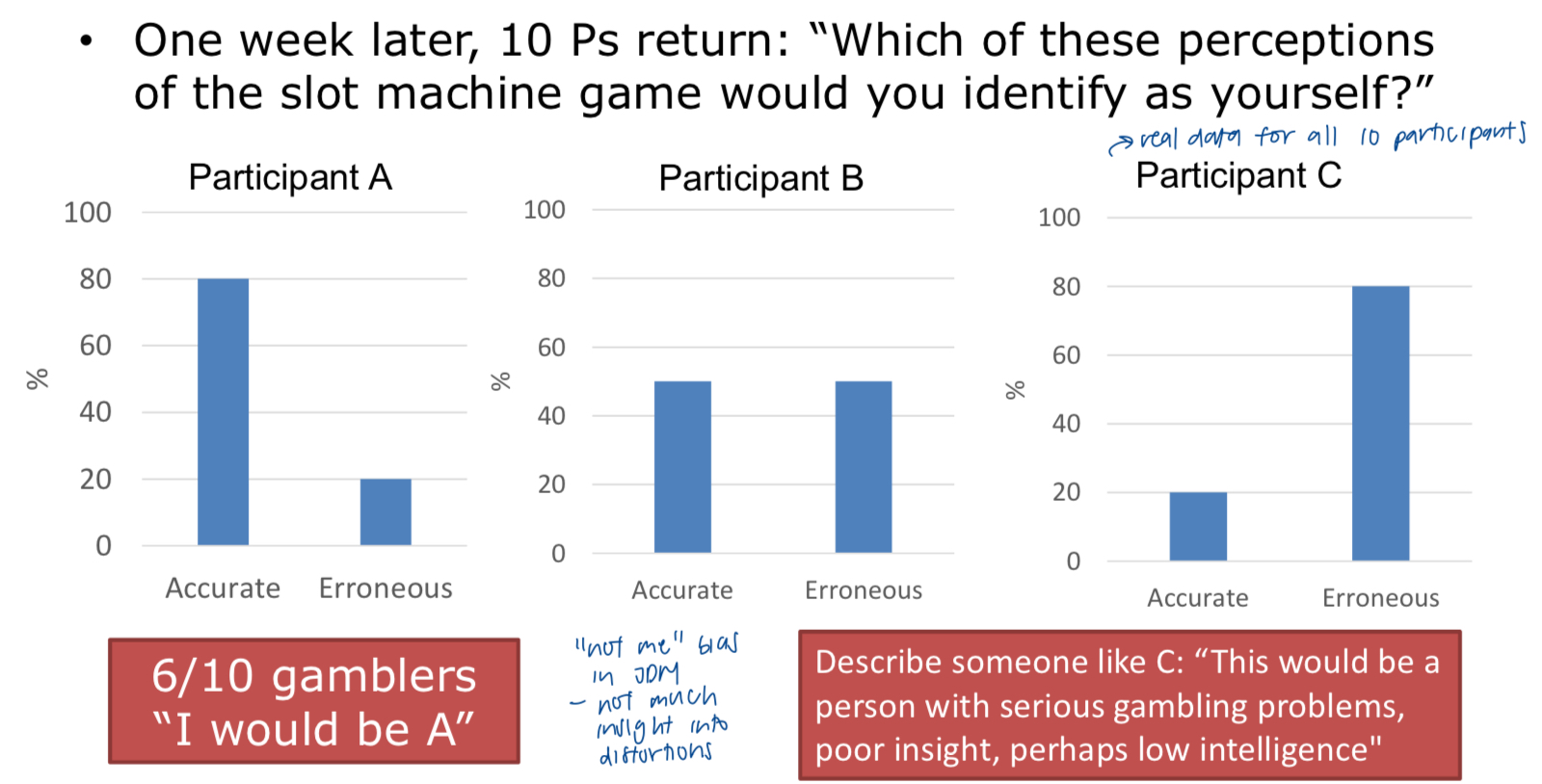
‘think aloud’ technique
gambler plays in natural environment for 5min + VOCALIZES all thoughts
thoughts coded as mathematically accurate of faulty
anthropomorphizing machine → giving consciousness to machine
gamblers fallacy; hindsight bias (knew that was gg to happen)
results
70-90% of gamblers’ thoughts are erroneous → tied to actual play and preferred game
erroneous thoughts elevated in ppl w disordered gambling
CEILING EFFECT: harder to detect any effect in PG
those w greatest HR increases made most erroneous thoughts
when identifying results → perceived self as more accurate even tho irl more erroneous
“not me” bias → lack insight into distortions
*levels of gambling cognitions elevated in problem gambling
‘think aloud’ critique
requirement to verbalize = UNNATURAL
demand characteristics: responding in ways they think the researchers want
relatively few ways to express accurate thoughts abt the game
bias in procedure
healthy ppl express SO MANY irrational beliefs during gambling
ceiling effect: hard to show PG do it even more
cognitions as a way of rationalizing unconscious operant responding?
lack of empirical evidence establishing CAUSAL significance
gambling related cognitions scale (self-report questionnaire) [GRCS]
5 subscales
[cognitive distortions] → PG score higher than avg on these items
illusion of control (IC)
specific RITUALS and BEHAVIOURS that may increase chances of winning (praying, superstitions, lucky charms)
predictive control (PC)
losses when gambling bound to be followed by series of wins (patterns, predictions)
interpretive bias (IB)
relating winnings to skill and ability makes person continue gambling
[beliefs about the self]
gambling expectancies (GE)
gambling makes things seem better
inability to stop gambling (IS)
not strong enough to stop gambling
*levels of gambling cognitions elevated in problem gambling
dice-throwing behaviour (henslin)
qualitative study of st louis taxi drivers → played craps during breaks
dice game: throw particular dice + bet on totals thrown
believed that a hard throw produces a large number, soft one produces a low number
other techniques involve evidencing concentration and effort (e.g. blowing on dice)
ellen langer’s illusion of control
IC + IB (illusion of control + interpretive bias)
“an expectancy of a personal success probability inappropriately higher than the objective probability”
skill vs chance
skill: you believe you can do smthg to change chance
chance: ppl behave as if they were in a situation requiring skill
hypothesis: if skilful features are inserted into chance situations, ppl shd feel inappropriately confident → cause the illusion of control
4 features
choice
motor involvement (smthg dextrous)
familiarity
competition
illusory control: feature 1 - irrelevant choice
lottery based on football cards (cost $1)
either chose their card or given a card (yoked to previous participant)
asked how much they would sell their ticket for
choosers: $8.67, non-chooser: $1.96 (p<.005)
endowment effect: choice = ownership → cog mechanism
illusory control: feature 2 - motor involvement
field study in vegas casino + using own money
craps: players place higher bets and bet more riskily (on single numbers) on their OWN throw
roulette: higher bets when player vs croupier (casino staff) throws ball onto wheel
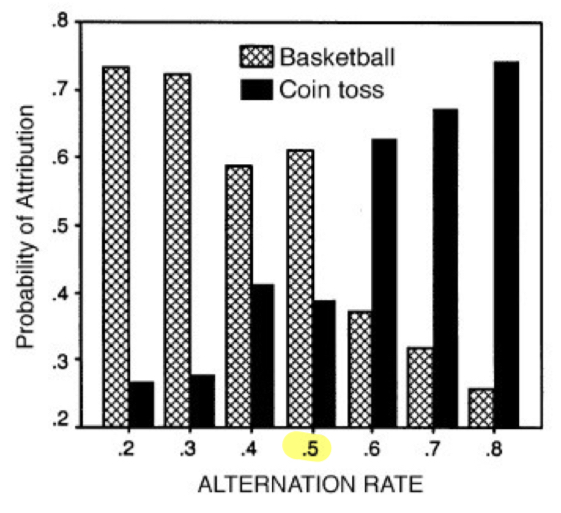
attribution of random sequence
to basketball or coin toss
0.58 = switchier than chance
0.2 = bball
0.8 = coin flip
sequential effects: template for randomness not very accurate (too switchy)
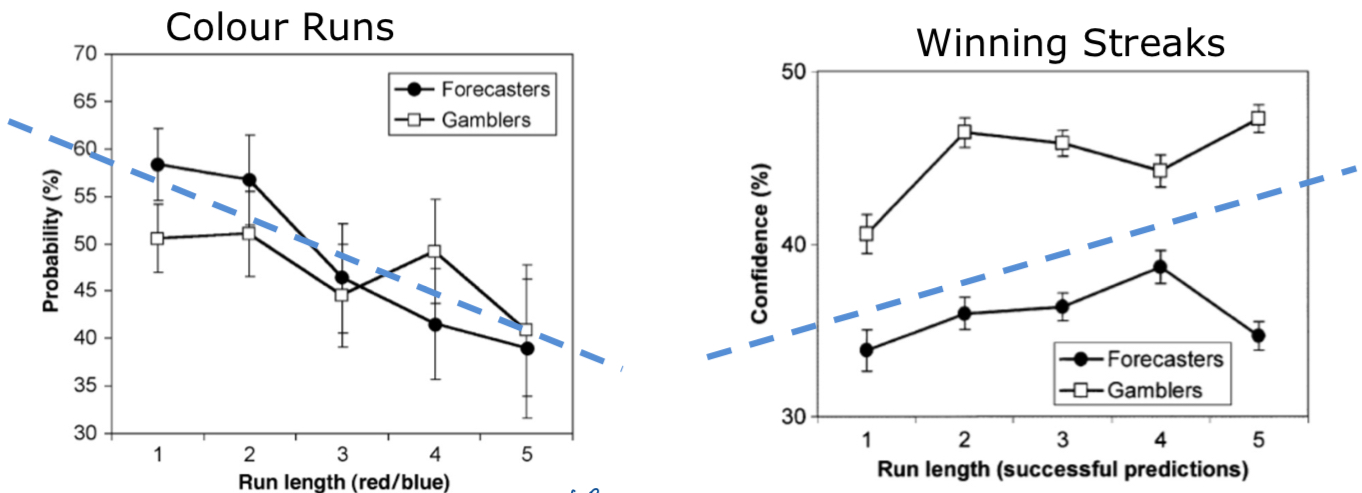
roulette predictions and confidence ratings
colour runs
the gambler’s fallacy: likelihood of choosing either colour DECREASES as a function of run length of that colour
negative recency
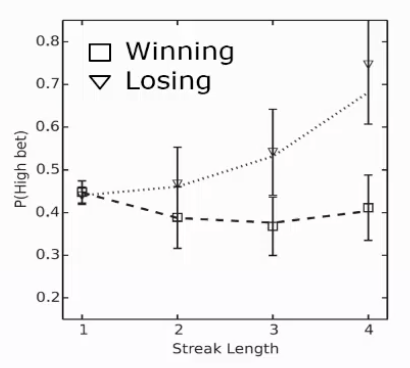
winning streaks
the ‘hot hand’: confidence in one’s predictions INCREASES as a function of past success (in the zone) → more confident in next prediction
the ‘cold hand’ effect: after a streak of LOSSES → less confident in their next colour prediction
**more than 1 sequential bias shown even within same task
the hot hand ‘fallacy’/bias/effect
gilovich et al: bball player scores 3 consecutive shots → likelihood of scoring next shot
players, fans, coaches: yes
NBA shooting records and field study: no
opponents attacking strat
increased anxiety
“the outcomes of previous shots influenced PREDICTIONS but not performance”
‘fallacy’ → categorical mistake (no control here)
human action vs machine
human: expect streaks to continue
vs
coin flip/roulette wheel: assume randomness (revert back)
losing streaks can also cause LOSS CHASING
3 experiments
gamblers fallacy = very ROBUST in all 3
experiment 3: place a bet
how much you bet not sensitive to winning BUT jumps up in long losing streaks → loss chasing
not visible in confidence
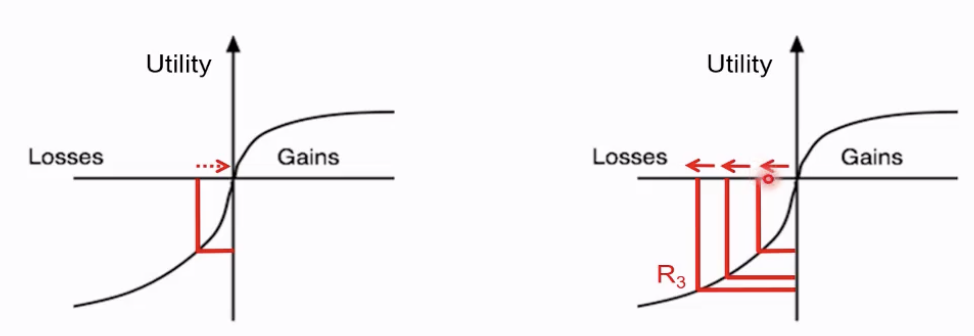
reference points and ‘wiping the slate’ (prospect theory - value function) - practice drawing
person ‘re-references’ after each outcome
choices NOT influenced by past gains or losses → NO loss chasing
go back to origin after each decision
person does NOT re-reference b/w each decision
after 3 successive losses, curve flattens which may make person INSENSITIVE to further losses → YES loss chasing
make decision from R3 → not worried about losses that much (not loss averse)
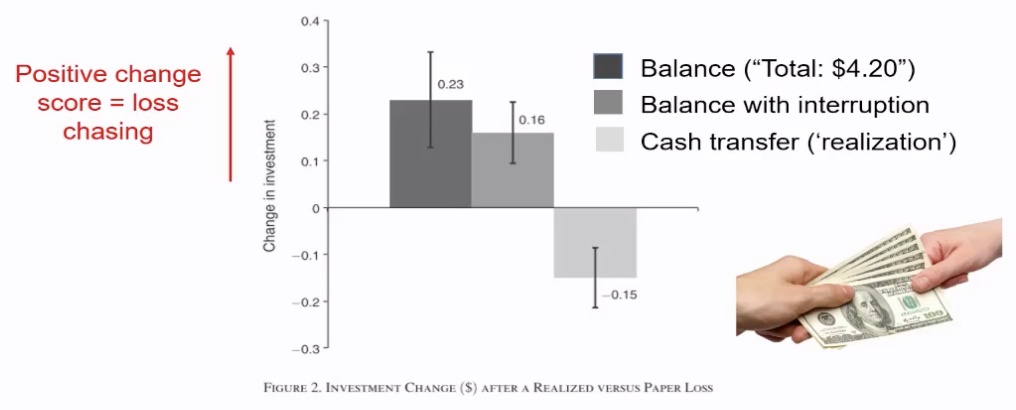
reference points and physical exchange of money
physical exchange of money b/w gambles forces gamblers to ‘re'-reference’ and abolish loss-chasing
control: balance with interruption → same pattern as balance/original
when money becomes abstract (cannot see it physically) → weight attached to losing it not the same
cash transfer (‘realization’) → not just the time delay
positive change score = loss chasing
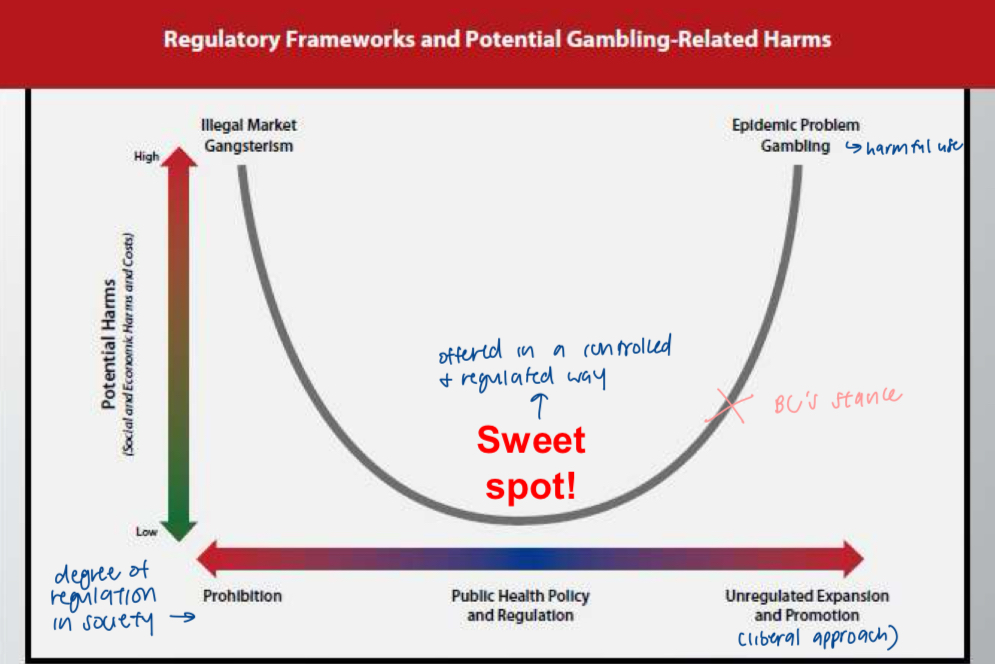
gambling regulation and gambling harms (Marks curve) - practice drawing
horizontal axis: degree of regulation in society (prohibition - unregulated expansion and promotion)
vertical axis: potential harms
sweet spot = offered in a controlled and regulated way
BC’s stance: more towards right side
rat gambling task (rGT) - rat ver of IGT
4 nose-poke holes to choose from:
reward: number of food pellets + probability
loss: time-out → cannot win any food
deck 2 = best deck
deck 4 = worst (big costs even tho large reward)
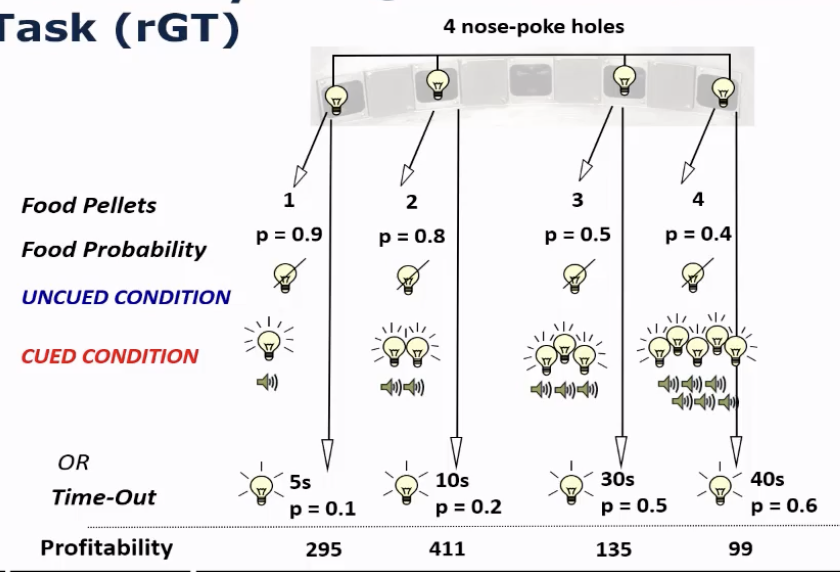
rat gambling task (rGT) - addition of bells and whistles
uncued condition: no lights
cued condition: amount of lights and jingles depends on the deck
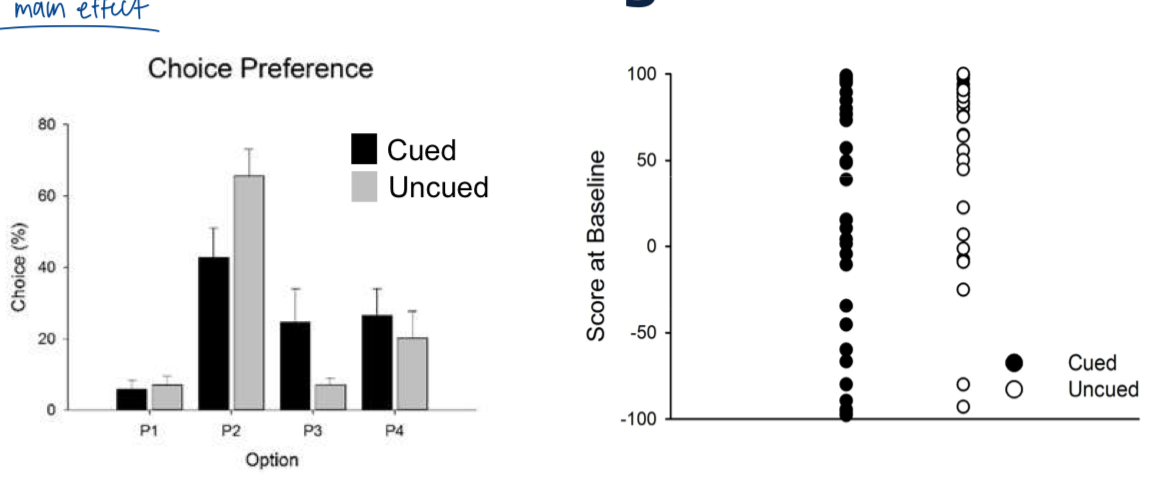
results:
adding audiovisual feedback REDUCED preference for the best ‘deck’ → more attracted to risky decks
large individual differences → personality dimensions
later experiments: preference for P2 vs P3 shifted by dopamine D3 drugs (complicated)
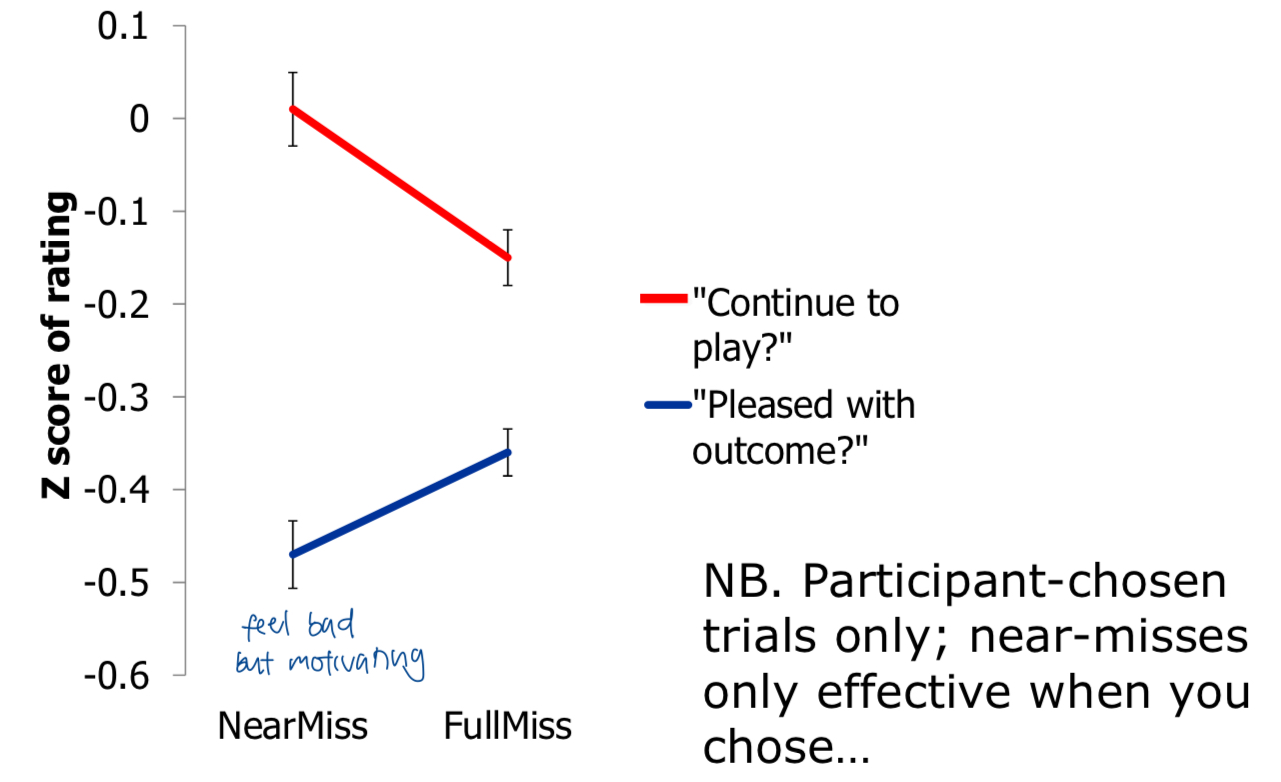
slot machine simulations (stripped down version w 2 reels)
outcomes:
win
near-miss
full-miss
*two misses categorically the same as any loss (no win)
rating: how much do you want to continue gambling
near misses are aversive (feel bad) but enhance motivation to play
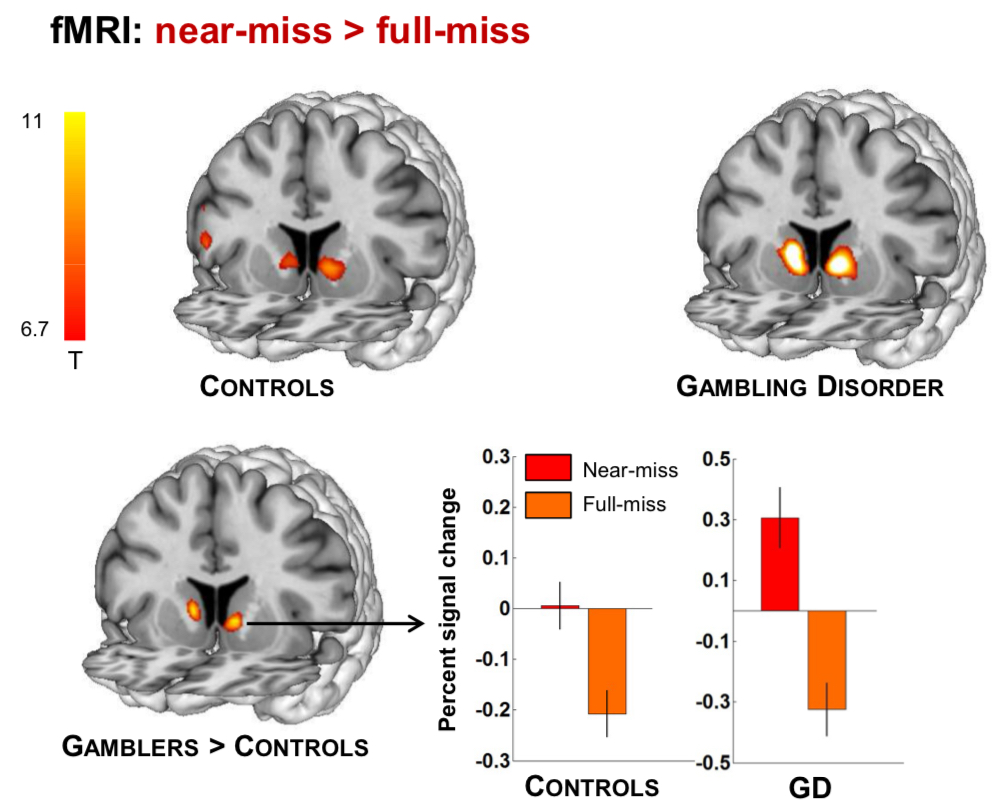
fMRI for slot machine simulations
near miss compared to full miss: increase brain activity in ventral striatum
near miss brain activity: increased reactivity in men with gambling disorder compared to control
treatment for pathways model
pw 1: reduce gambling advertisements
pw 2: antidepressants, CBT for depression
pw 3: intensive and structured programs to prevent them from dropping out