Looks like no one added any tags here yet for you.
•Functions of the Kidney
▫Urine formation
▫Excretion of waste products
▫Regulation of electrolytes
▫Regulation of acid-base balance
▫Control of water balance & blood pressure
▫Regulation of red blood cell production
▫Synthesis of vitamin D to active form
▫Regulates calcium & phosphorus balance
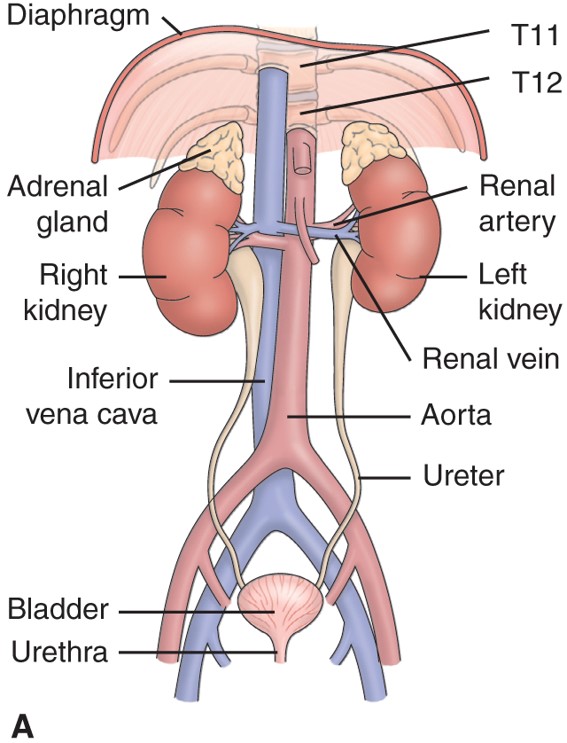
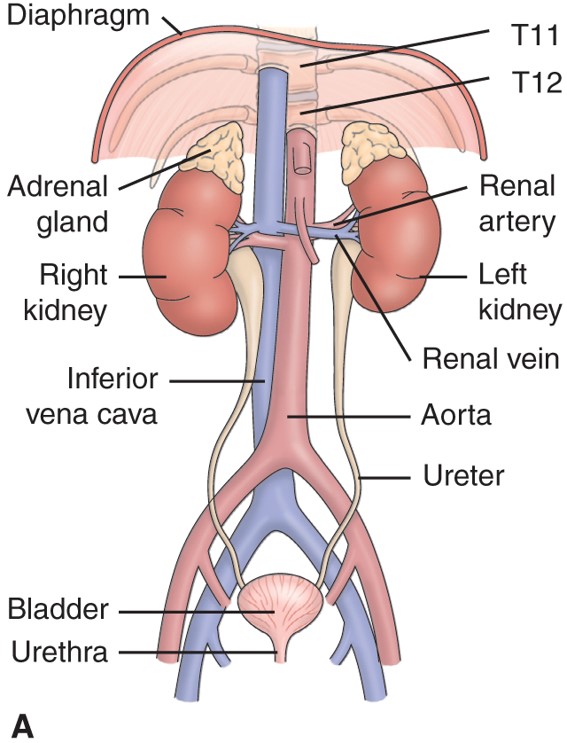
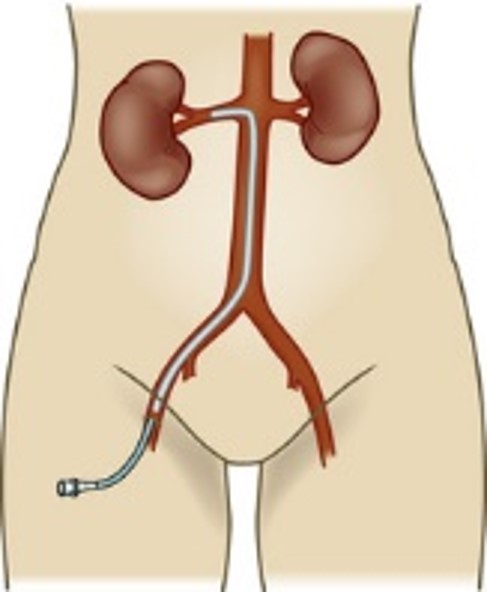
Anatomy Structures:
▫Kidneys
▫Ureters
▫Bladder
▫Urethra
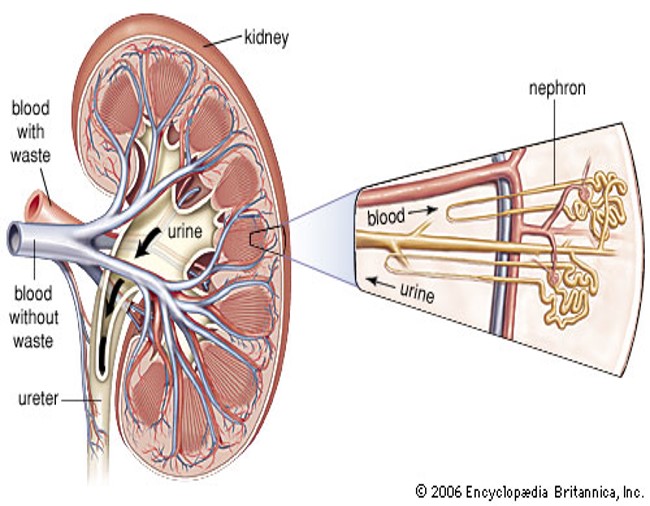
Internal Structure of the Kidney
Age Related Changes
•Ages 30-90
•7th decade of life
•Atherosclerosis
•Decreased blood flow
•Altered hormone levels
•Loss of elasticity –Females
•Prostate enlargement – Males
Health History & Assessment
•Pain
•Past history of UTI
•Fever, chills
•Changes in urinary pattern
•Dysuria
•Nocturia
•Hematuria
•Anuria
•Nutritional lifestyle patterns
•Weight gain or loss
•Medications
•Smoking
•Vital signs
•Intake and output
•Weight; BMI
•Inspect
•Palpate
•Percussion
•Auscultation
•NORMAL:
•No CVA tenderness
•Non-palpable kidney, bladder
•No palpable masses
Diagnostic Assessment
•Color: amber yellow
•Odor: aromatic
•Protein: random, 0-trace
•Glucose: none
•Ketones: none
•Bilirubin: none
•Specific gravity: 1.003-1.030
•Osmolality: 300-1300
•pH: 4.0-8.0, avg 6.0
•RBCs: 0-4
•WBCs: 0-5
•Casts: none to occasional
•Culture: no organisms
Lab Tests and Imaging Studies
•Review the description, purpose and nursing responsibilities
•Urinalysis
•Creatinine clearance: no calculation; no values; just purpose and nursing responsibilities
•Composite urine collection
•Urine clean catch
•Concentration test (aka: specific gravity)
•Residual urine
•Protein dipstick
•Quantative protein
•BUN, Creatinine, K+, Sodium, Calcium, Phos, Sodium Bicarb
•Renal biopsy
•Cystoscopy
•MRI
•Renal Ultrasound
•CT
•KUB
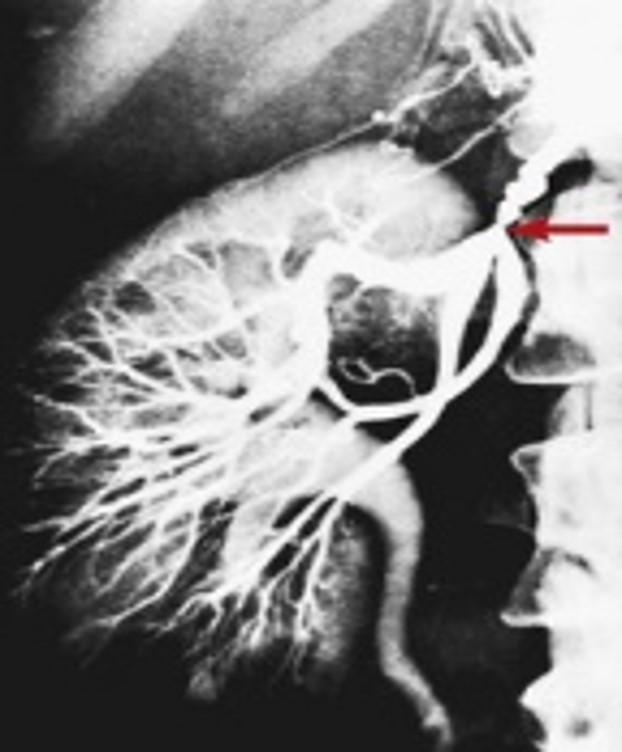
•Renal Arteriogram
Nursing Care of the Patient Undergoing Diagnostic Testing of the Renal-Urologic System—Assessment
•Patient knowledge
•Psychosocial and emotional factors; fear, anxiety
•Urologic function, include voiding habits/pattern
•Fluid intake
•Hygiene
•Presence of pain or discomfort
•Allergies
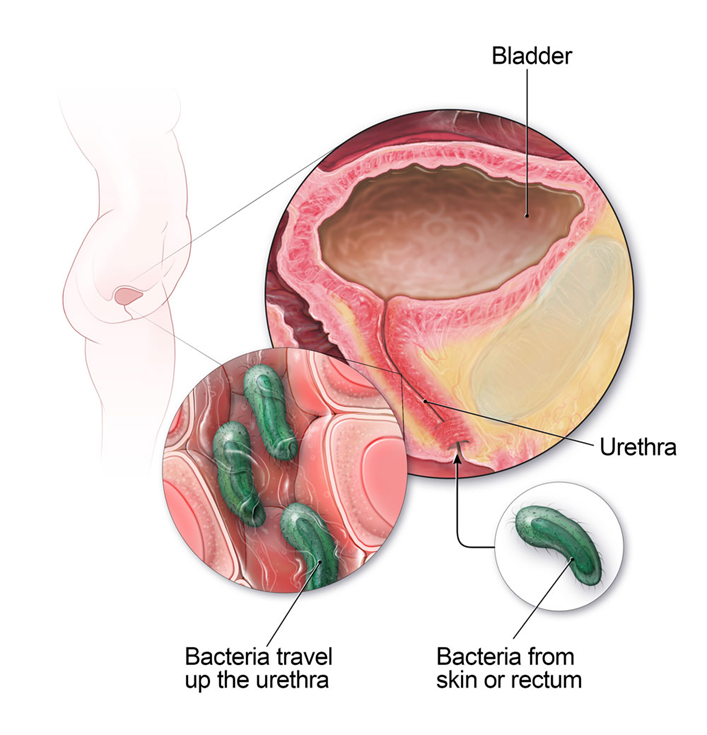
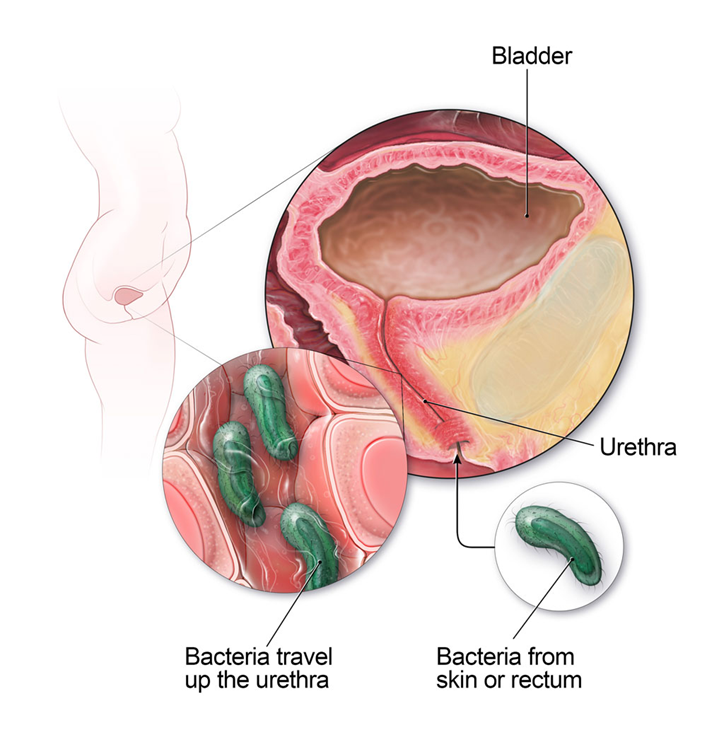
Urinary Tract Infection
•Bladder & its contents are typically free of bacteria
•Females >Males
•Invasion of bacteria
•E. Coli
•Etiology
•At Risk Patients
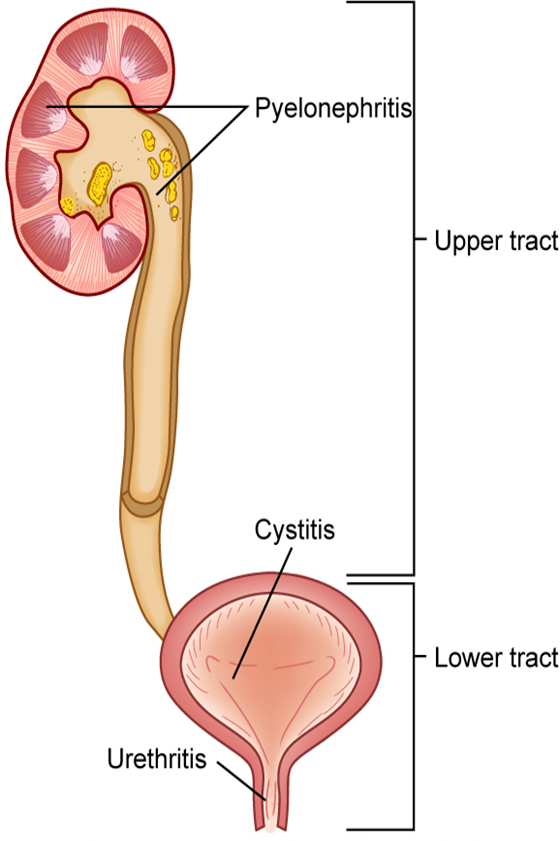
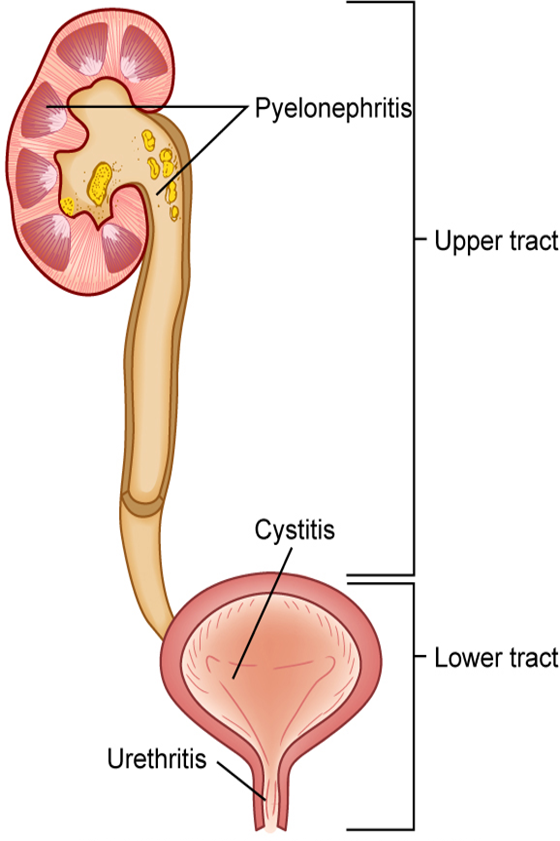
Urinary Tract Infection
•Upper versus Lower
•Urosepsis
•Uncomplicated versus Complicated
•CAUTI
UTI: Diagnostics
•Diagnostics
Dipstick Urinalysis
+Nitrites
+WBCs
+Leukocyte Esterase
Urine Cultures / CT and US of abdomen and Pelvis
UTI Medical Therapy
•Uncomplicated UTI
•Phenazopyridine àPain
•Antibiotics
trimethoprim/sulfamethoxazole (Bactrim)
trimethoprim alone (in patients with sulfa allergy)
nitrofurantoin (Macrodantin, Macrobid)
fosfomycin (Monurol)
•Recurrent UTI
•Phenzopyridine à Pain
•Antibiotics:
trimethoprim/sulfamethoxazole, nitrofurantoin
Sensitivity-guided antibiotic therapy
Prophylactic antibiotic regimen
Consider post-coital antibiotic prophylaxis
UTI Nursing Interventions
•Recognize AT RISK individuals
•Empty bladder and stool
Routine void Q3-4 hrs (minimum)
•Wipe front to back
•Increase PO water intake
•Cranberry
•Remove catheters early; avoid unnecessary catherization
•Avoid contaminating urine samples
•Perineal care
•Void after intercourse
UTI Nursing Interventions (pt. 2)
•Frequent rounds; offer bedpan or frequent toileting
•Early removal of indwelling catheters
•Handwashing
•Placement of “foley” is STERILE
•Avoid bladder irritants
•Localized heat
•Medication education
•Complete medical therapy
•When to call the healthcare provider
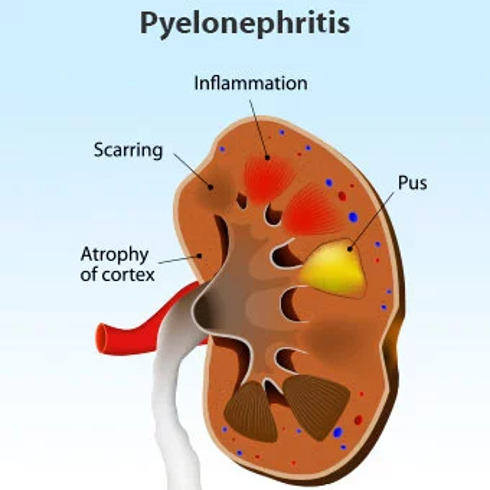
Pyelonephritis
•Inflammation of the renal parenchyma and collecting system
•Etiology
Bacterial infection
Urosepsis
Pre-existing factors
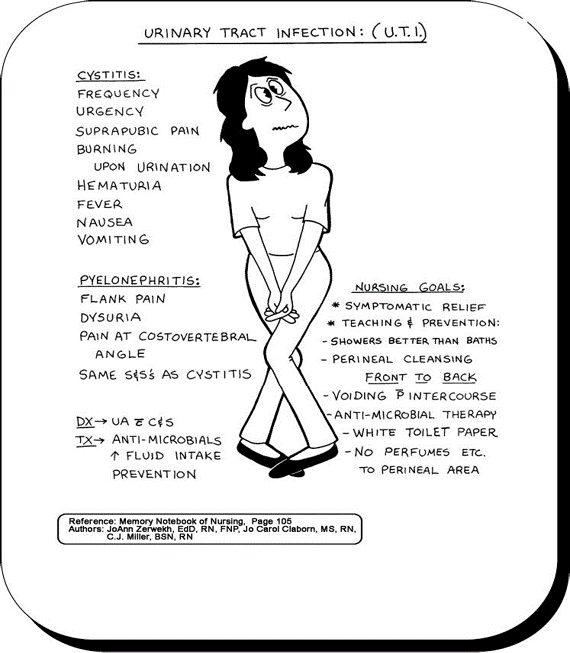
Pyelonephritis – Clinical Manifestations
•Symptoms (6)
Mild fatigue
Chills
Fever
Vomiting
Malaise
Flank pain
•Diagnostics (2)
Urinalysis
Ultrasound / CT
Pyelonephritis (Acute & Chronic)
ACUTE (7)
•H&P
•U/A + C/S
•Imaging studies
•Labs
•Assessment
•Mild Symptoms: Drug Therapy
•Severe Symptoms: Drug Therapy
CHRONIC (5)
•Kidneys become small, atrophic, shrunken and lose function
•Etiology: recurrent infections
•Imaging and Biopsy to confirm diagnosis
•One vs Both kidneys
•Progression to ESRD
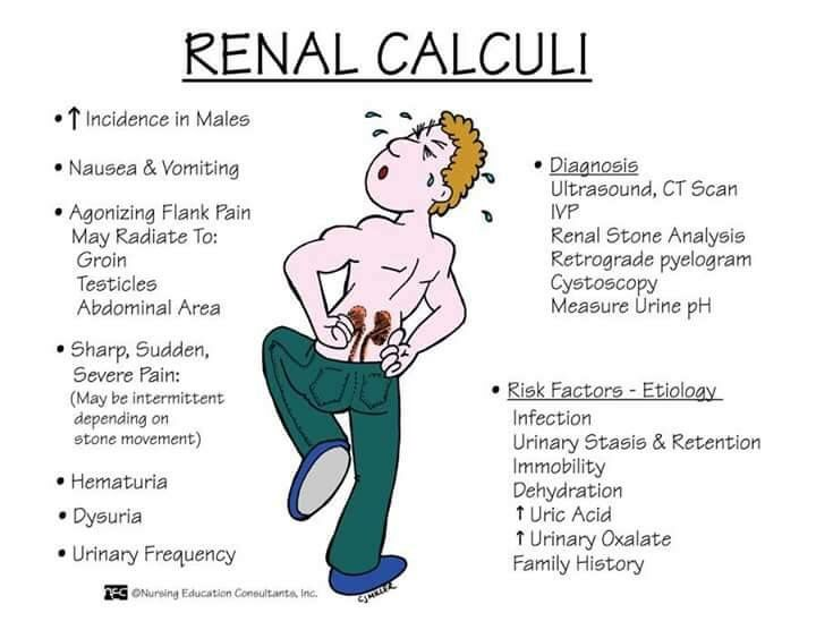
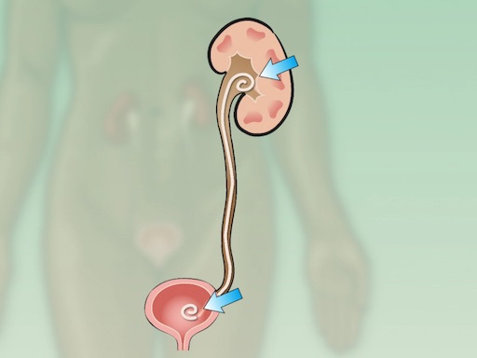
Urinary Tract Calculi
•Nephrolithiasis (kidney stone disease)
•Males
•20-55 yrs of age
•Reoccur in 50%
•Summer → Dehydration theory
•Gender Differences
Urinary Tract Calculi: Risk Factors
•Metabolic → Abnormalities that result in increased urine levels of calcium, oxalate uric acid, or citric acid
•Climate → Warm climates that cause increased fluid loss, low urine volume, and increased solute concentration in urine
•Diet
Large intake of dietary proteins that increases uric acid excretion
Excessive amounts of tea or fruit juices that elevate urinary oxalate level
Large intake of calcium and oxalate
Low fluid intake that increases urinary concentration
•Genetic Factors → Family history of stone formation, cystinuria, gout, or renal acidosis
•Lifestyle
Sedentary occupation, immobility
Urinary Tract Calculi: Types of Stones
•Review Characteristics, Predisposing Factors and Treatment
Calcium phosphate
Calcium oxalate
Uric acid
Cystine
Struvite (magnesium ammonium phosphate)
Urinary Tract Calculi: Diagnostics & Interprofessional care
Diagnostics
•Non-contrast CT
•U/A
•KUB
•(IVP) Intravenous Pyelogram
•Stone Retrival
▫Patient may pass
•Check urine pH
Interprofessional care
1) Manage the Attack
2) Etiology
H&P
OTC and Prescribed Meds
Labs, Diagnostics
Lifestyle
Diet
Tamsulosin or Terazosin
Acetohydroxamic Acid
Antibiotics
Invasive Treatment
Cystoscopy
Percutaneous Removal
Lithotripsy
Surgery
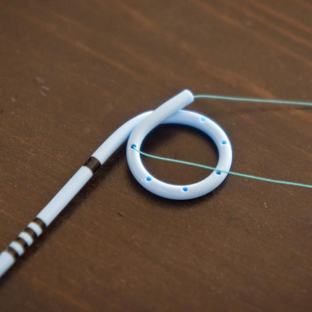
Ureteral Stent
Nursing Interventions for Kidney Stones
•Pain relief
•Monitoring for complications
•Promote fluid intake: 2-3L intake and 2L output
•Encourage ambulation
•Strain all urine
•Urine Cx every 1-2 months
•Medical therapy
•Diet Therapy
•Vital Signs (temperature)
•Patient education
▫Report decreased urine output
▫Report sudden increase in pain
▫If stent, hematuria expected, monitor for fever
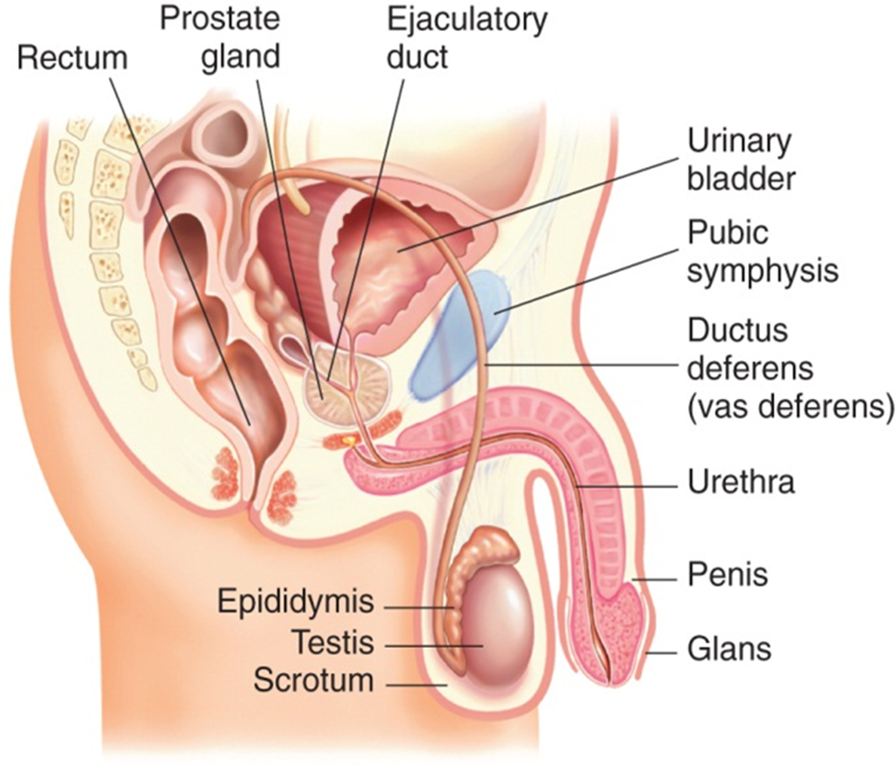
Benign Prostatic Hyperplasia (BPH) / RF
•Benign enlargement of the prostate gland
•Common in adult males
•50% of men will develop BPH
•Cause is unknown
•Enlargement of gland can lead to urethra obstruction
•Risk factors: aging, obesity, lack of physical activity, alcohol consumption, erectile dysfunction, smoking, and diabetes.
BPH (Diagnostics/ Goals/ Tx)
•Diagnostics: H&P, prostate can be palpated by digital rectal exam, urinalysis with culture, Prostate-specific antigen (PSA) to rule out prostate cancer.
•Goals: Restore bladder drainage, relieve patient’s symptoms, prevent/treat complications of BPH
•Treatment: Conservatively, Medications, Surgery
Drug Therapy
•5α-Reductase inhibitors
• α-Adrenergic receptor blockers
• Erectogenic drugs
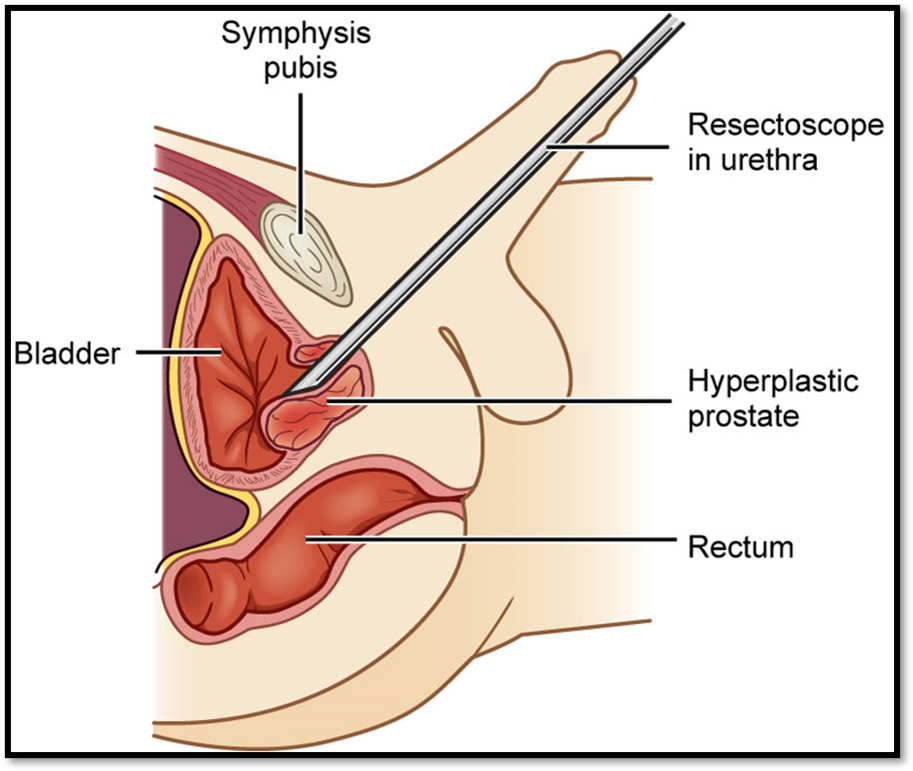
Nursing Implementation
•Preoperative care for TURP
Administer antibiotics
Treat UTIs
▫Restore urinary drainage
Coudé – curved-tip catheter
Filiform – rigid catheter
Aseptic technique very important in preventing infection
▫rovide patient opportunity to express concerns over alterations in sexual function
▫Inform patient of possible complications of procedures
Decreased or absent ejaculate volume
Retrograde ejaculation
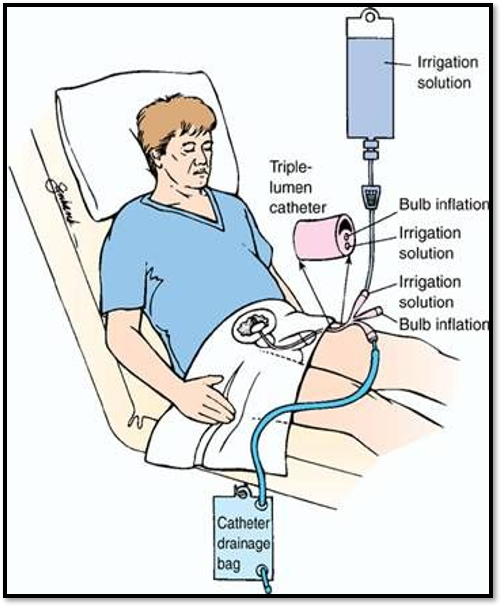
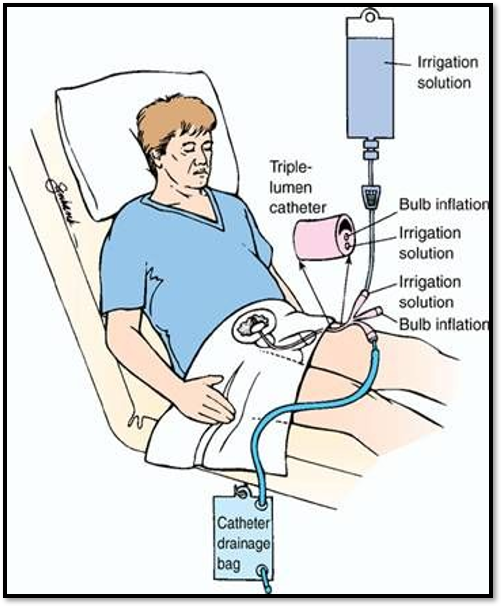
Nursing Implementation
•Maintain Patency with flushing and irrigation
•Continuous versus intermittent irrigation
•Sterile solutions
•Clears out clots and debris
•Used to instill medications into bladder
•Maintain closed system
Nursing Implementation Post-op
•Postoperative care for TURP
Postoperative bladder irrigation
Stool softeners and high fiber diet to prevent straining
Treat bladder spasms
Catheter care
Teach Kegel exercises
Observe for signs of infection
Manually on an intermittent basis
Continuous bladder irrigation (CBI)
Remove blood clots
Ensure drainage of urine
Use aseptic technique
•Assess for complications
Hemorrhage
Bladder spasms
Urinary incontinence
Infection
Nursing Implementation: Ambulatory and Home Care
•After prostate surgery
Return to urinary continence
Refer to continence clinic if not normal within 12 months
Use of penile clamp, condom catheter, incontinence pads or briefs to manage dribbling and continue socialization activities
Health Promotion
•Early detection and treatment
•55-69 greatest benefit from PSA
•Initial Q2 years
•Avoid irritants
•Cold Meds
•Patient Education