637 Body Positioning
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
What are the key concepts of gravity?
Affects O2 transport
Essential to normal cardiovascular and pulmonary function
Physiological position - “upright and moving” with normal O2 transport
O2 transport can be improved, maintained, worsened by body position changes
Consider compression forces in upright and sidelying positions
Frequent body position changes and avoiding prolonged period in same position is optimal
Length of time a body position is maintained in response dependent and NOT time dependent
Patient preference, age, body mass, condition/pathology
In the upright position, where are ventilation & perfusion more distributed? What is increased more toward the lower zone? What is decreased more toward the lower zone?
Ventilation and perfusion are both more distributed toward the lower zone (base) due to gravity
Perfusion increases more dramatically than ventilation toward the base
V/Q is lower at the base than at the apex (means that blood flow is greater, can achieve more efficient gas exchange)
Where is V/Q highest in the upright position?
Mid-lung
What is the accepted standard of care for patient positioning? What does body positioning affect physiologically? What could be potential explanations for the positive effects?
Accepted standard of care = adjusting/turning client every 2 hours
Body position has “potent and direct” effects on steps of the O2 transport pathway (and movement of mucus)
Improved mucociliary transport OR positioning the better lung downward to improve gas exchange
What is the equation for functional residual capacity?
FRC = ERV + RV
What is the optimal bed position for patients with pulmonary conditions?
60 degrees or more in sitting or for exercise
~45 degrees is what COPD pts prefer
What is the significance of upright positioning on mucus?
Positioning impacts how mucus settles
Layers of mucus → consolidates → hard to mobilize b/c thickening
Upright is better for mobilizing mucus
FREQUENCY matters
How does the upright position impact kidney function?
Promotion of urinary drainage from the renal pelvi to the bladder when in the upright position, as a result of the reduced area for urinary stasis when in upright vs supine position
Optimal renal function is essential to preserving normal hemodynamic status
What are the approximations of upright position in supine?
Supine → recumbent → propped up (typical goal) → sitting/standing (ideal)
What specific structure does the supine position affect during respiration? Why? What lung capacities reduce in supine? Why?
Diaphragm
Due to increased pressure from abdominal viscera that keeps diaphragm from moving caudally
Increase in intrathoracic blood volume
TLC, VC, and FVC all reduce in supine
Less inspired air with greater diaphragmatic movement
What pts would benefit from sidelying the good lung down? When is the sidelying position often preferred to the supine position? What are the effects of prolonged sidelying? What does sidelying increase?
ABGs improve in pts with unilateral lung disease when positioned with good lung down
Sidelying >supine preferred by pts who are hospitalized
Decreased dynamic lung compliance in lateral and prone positions than supine in intubated pts
Prolonged sidelying can mobilize lung water in pts with pulmonary edema and pulmonary inflammation
Sidelying increases EDV pressure on dependent side
What kind of patients would benefit from GOOD LUNG DOWN?
Tumor, areas of atelectasis, cystic fibrosis
How does the prone position affect the heart? Blood vessels? Weight of heart and abdominal organs? Posterior lung surface area? Fluid concentration? Secretions? Overall benefits? Risks?
Increased volume to right side of heart
Constriction of blood vessels to lungs decreases
Weight of heart and abdominal organs is on chest instead of lungs
Greater posterior lung surface area
Fluid concentrated to anterior
Secretions can leave mouth and nose easier as head is down
Benefits: requires less support from ventilator, can improve heart function and better distribution of gas exchange in lungs
Risks: potential increased incidence of pressure injuries
What position is best to organize pleural fluid?
Upright position
What is the issue with acute cardiopulmonary conditions with meeting body demands? What are causes of poor return to PLOF? What does the ICU consist of? What are issues of psychological stress?
Pts oxygen transport pathway cannot meet needs of body
Causes of poor return to PLOF: acute inflammation, severity of illness, exposure to corticosteroids, neuromuscular blocks, sedation, bedrest, and marginal baseline function
ICU: continuous central line monitoring, vasoactive medication, sedation, circulatory assist devices, mechanical ventilation, and artificial airways
Psychological stress: fear, unknown length of stay, powerlessness, anxiety, isolation, spiritual distress
*What are the systemic effects of immobilization? (CV, resp, MSK, CNS, met)
(Table 19.1)
Cardiovascular system
Increased basal heart rate
Decreased maximal heart rate
Decreased maximal oxygen uptake
Orthostatic hypotension
increased venous thrombosis risk
Decreased total blood volume
Decreased hemoglobin concentration
Respiratory system
Decreased vital capacity
Decreased residual volume
Decreased PaO2
Impaired ability to clear secretions
Increased ventilation-perfusion mismatch
Musculoskeletal system
Decreased strength
Decreased girth
Decreased efficiency of contraction
Joint contractures
Decubitus ulcers
Central nervous system
Emotional and behavioral disturbances
Cognitive deficits
Altered sensation
Decreased balance
Metabolic system
Hypercalcemia
Osteoporosis
Patients in acute care setting with cardiopulmonary conditions may have what?
Poor cough mechanics
Difficulty performing airway clearance
Difficulty achieving enough inspiratory effort
Poor oxygenation status
Poor hemodynamic status
Decreased endurance, activity tolerance, and functional mobility (Table 19.2)
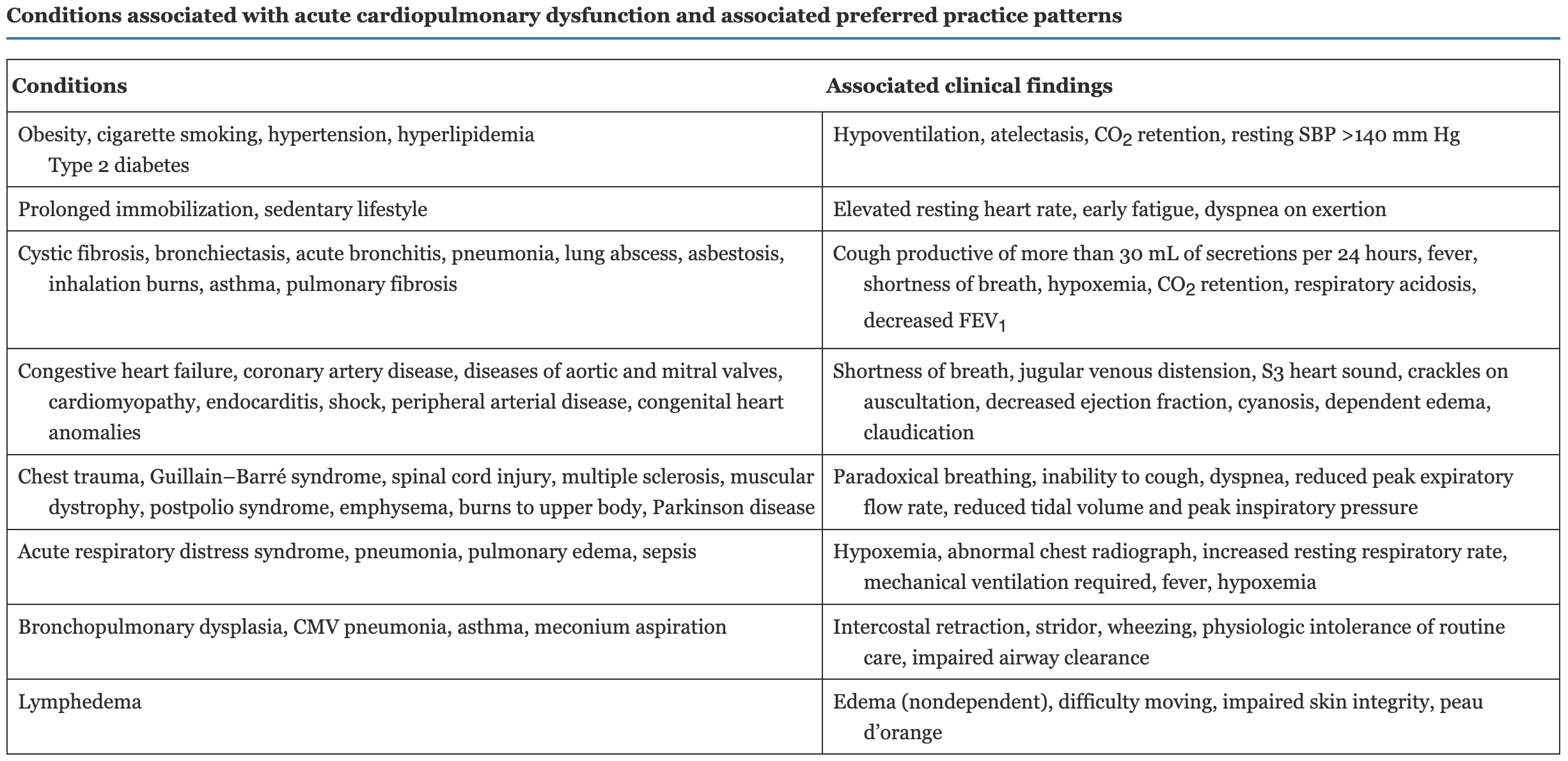
What are conditions associated with acute cardiopulmonary dysfunction and associated preferred practice patterns? Where will you commonly find an S3 heart sound? CO2 retention/respiratory acidosis?
(Table 19.2)
What are airway clearance techniques? Indications? Important factors in airway clearance plan? What precautions to follow?*
Manual or mechanical procedures to mobilize secretions from the airways
Postural drainage positions may be used to leverage gravity in the mobilization of secretions in addition to manual techniques such as percussion and vibration as well as cough and breathing techniques and airway suctioning
Indications: impaired mucociliary transport, excessive pulmonary secretions, ineffective or absent cough
Important factors in airway clearance plan: stability of medical status, pathophysiology and symptoms, pt’s adherence to techniques
Maintaining droplet, airborne, and contact safety precautions are imperative as pathology may be contagious
What are some 8 condition that require airway clearance?
Cystic fibrosis
Bronchiectasis
Atelectasis
Respiratory muscle weakness
Mechanical ventilation
Neonatal respiratory distress syndrome
Asthma
ALSO: CHF
True or false: the higher a score on the BORG rating of perceived exertion, the better it is
False, a score of 10 means “maximal, just like my hardest race” and a score of 0 means “rest”
True or false: there are usually multiple areas of consolidation, not just one
True
What do you prioritize with postural drainage? What equipment do you need to have ready? How long do you maintain each position and how many positions on average? What should the patient do? What are signs of intolerance?
Treat most affected lung segments first
Positions can be modified due to a precaution or relative contraindication
Equipment for positioning: adjustable bed, pillows, bolsters, blanket rolls, enough personnel
Have secretion materials ready BEFORE starting: tissues, secretion cup, airway suctioning equipment, and body substance barriers
Each position should be maintained for 5-10 minutes as long as the pt is stable; 2-3 positions on average
Pt should be encouraged to take deep breaths and cough (or be suctioned) between each position change
Can be used in coordination with other services, bathing, turning for skin protection, linen change
Signs of intolerance: anxiety, SOB, HTN, nausea, dizziness, bronchospasm
*What are precautions and relative contraindications for postural drainage?
Precautions
Pulmonary edema
Hemoptysis
Massive obesity
Large pleural effusion
Massive ascites
Relative contraindications
Increased intracranial pressure
Hemodynamically unstable
Recent esophageal anastomosis
Recent spinal fusion or injury
Recent head trauma
Diaphragmatic hernia
Recent eye surgery
What is percussion? Technique? Speed and duration? What to avoid?
Airway clearance technique used to mobilize secretions either manually or with a device
Should be specific to affected lung segment
Technique:
Cupped hands to trap air (can use percussor cups)
Alternating to produce hollow, thumping sound (should not sound like a slap)
Wrists and elbows stay relaxed as hands are clapped over thorax
Speed 100-480 bpm for 3-5 min
Avoid bony prominences, surgical incisions, medical appliances
What is vibration? Who would benefit from it? Technique? Speed and duration?
Palmar aspect of pt’s hand in full contact with chest wall
Hands may be overlapping
Pt is cued to take a deep breath
On exhale, PT applies pressure and gently oscillates until full exhale
Speed = 12-20 hz (12-20 cycles/sec)
5-8 breaths
*What are precautions and relative contraindications for percussion and vibration?
Precautions
Uncontrolled bronchospasm
Osteoporosis
Rib fractures
Metastatic cancer to ribs
Tumor obstruction of airway
Anxiety
Coagulopathy
Convulsive or seizure disorder
Recent pacemaker placement
Relative contraindications
Hemoptysis
Untreated tension pneumothorax
Platelet count below 20.000 per mm³
Unstable hemodynamic status
Open wounds, burns in the thoracic area
Pulmonary embolism
Subcutaneous emphysema
Recent skin grafts or flaps on thorax
Which is the less aggressive method: vibration or percussion?
Vibration