Knee Kinesiology
1/95
Earn XP
Description and Tags
DPT 5025
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
96 Terms
A hinge joint primarily allows what type of movement?
Flexion and extension; however, you also have internal/external rotation and ABD/ADD (slight) at the knee joint.
Knee: Bones
Femur, tibia, and patella (proximal tib-fib joint does not contribute significant movement to the knee joint).
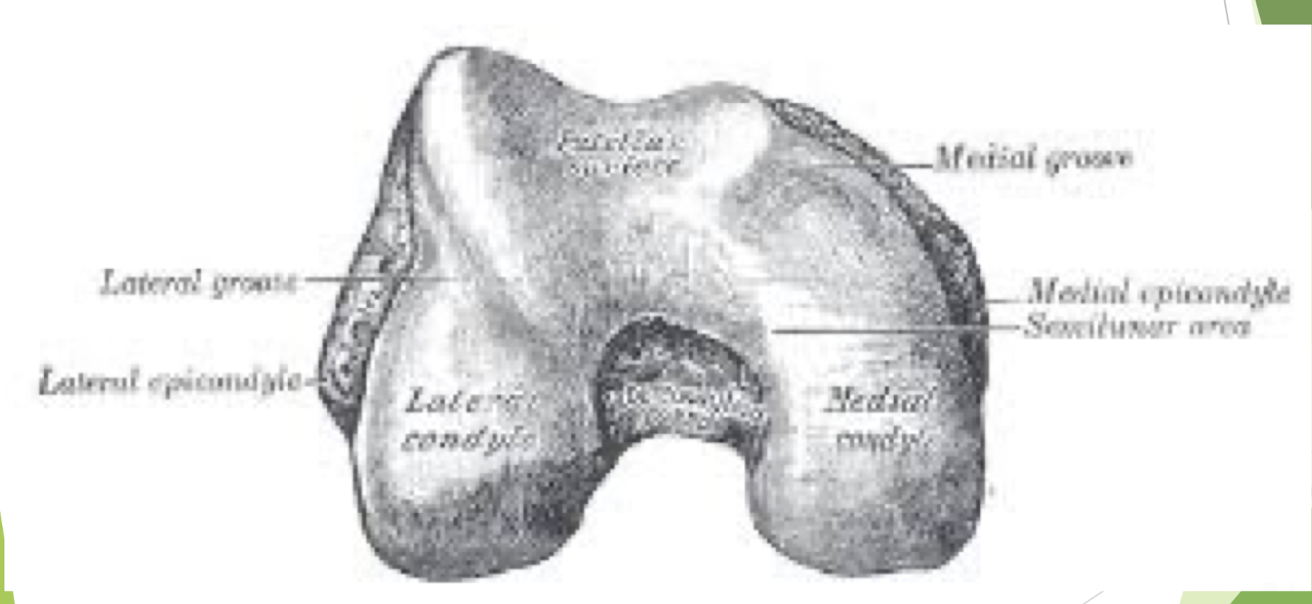
The Femur is divided into what?
Medial and lateral femoral condyles, which are convex.
The Tibia is divided into what?
Medial and lateral tibial plateaus, which are concave.
Patella
The largest sesamoid bone in the body that rides in the trochlear or intercondylar groove between the medial and lateral femoral condyles.
Patella and Trochlear Groove
Lateral femoral condyle has greater anterior projection to assist in preventing lateral patellar dislocation.
Patellar dislocation is more likely with a shallow groove.
Patella Main Function
The patella increases the lever arm length for the quadriceps muscle to extend the knee. In effect, the patella lifts the quad tendon further away from the knee joint axis, thus increasing the lever arm length measured from the joint center.
Patella– Effect on Lever Arm of Quadriceps
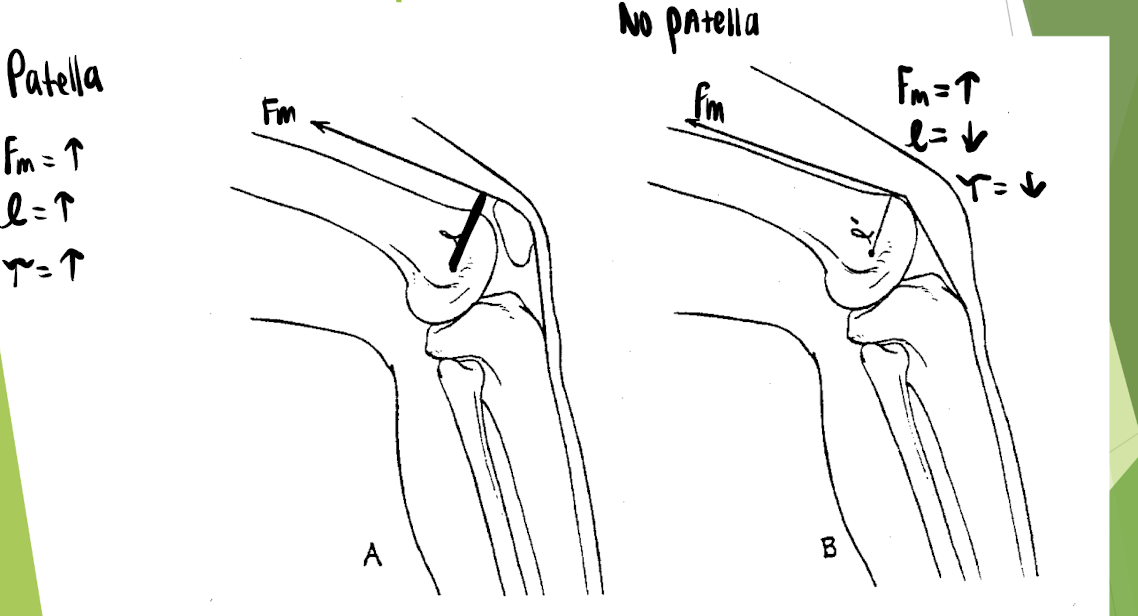
Without the patella, to get the same torque, what must you do?
Greatly increase the force production from the quadriceps due to the loss in lever arm length.
True or False: The patella greatly adds to the quadriceps mechanical advantage.
TRUE
Patellar Motion
No true convex/concave rule because there is no joint capsule.
Patellar Motion: Knee Extension
The patella moves superiorly along the trochlear groove. At full, there is less stability of the patella.
Patellar Motion: Knee Flexion
The patella moves distally along the trochlear groove. More stability!
Total Glide of Patella
5-7cm (check patellar mobility in both positions)
Femur
Largest and longest bone in the body.
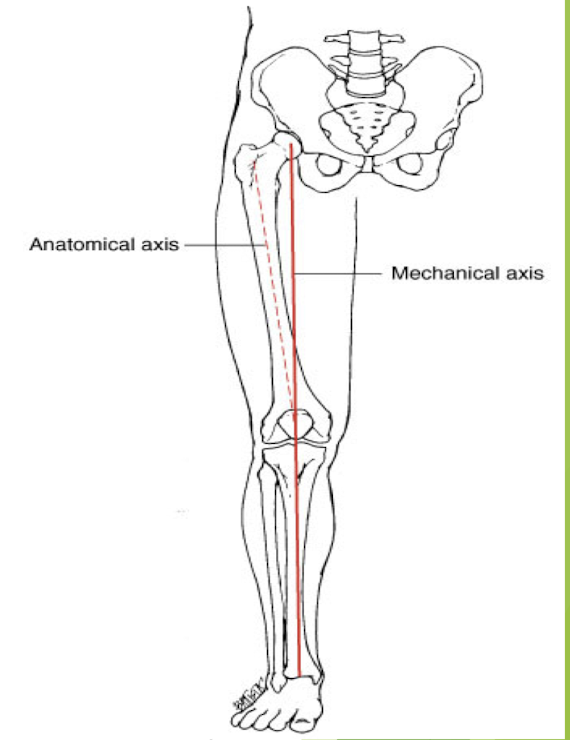
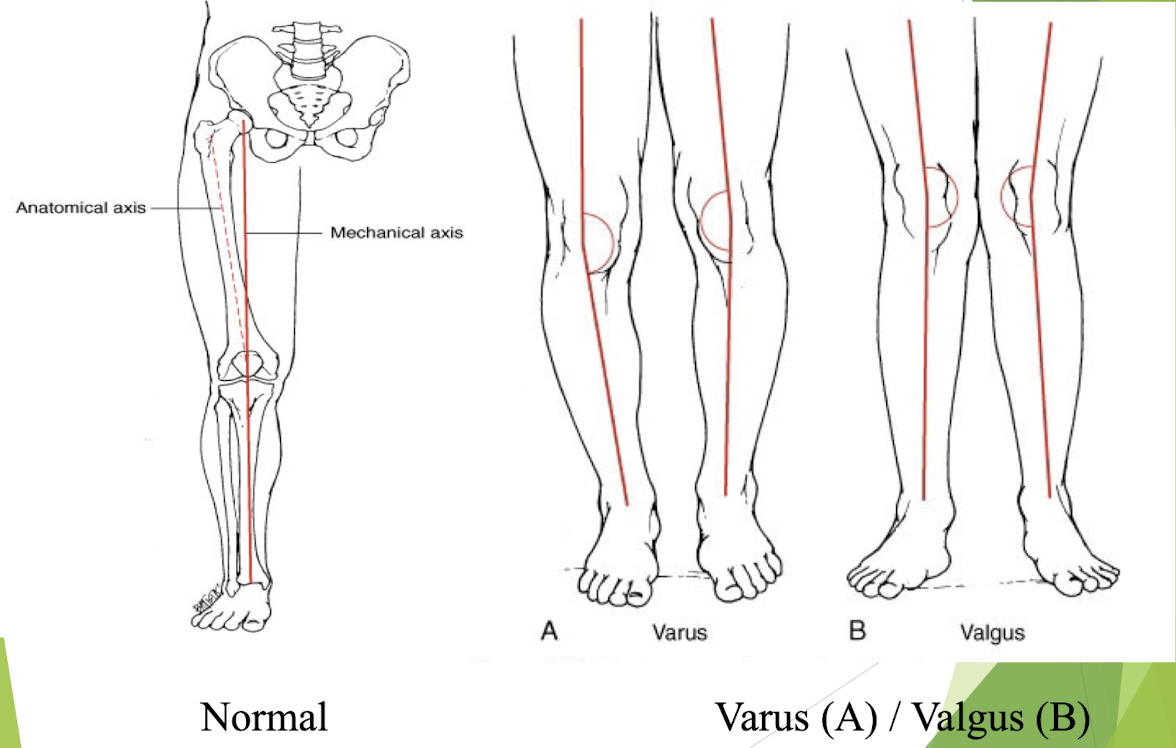
Physiological Valgus
When the medial and lateral femoral condyles sit in the same transverse plane, the shaft of the femur runs approximately 10 degrees lateral to a vertical line (this is normal).
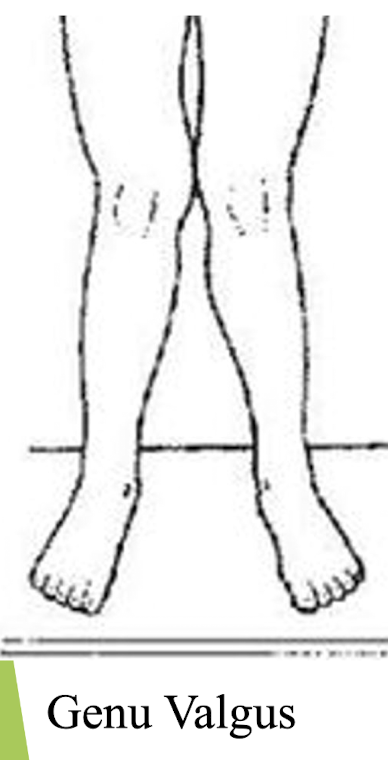
Genu Valgus
Knock-kneed
Femoral shaft > 10º from vertical.
Increased weight bearing on the lateral femoral condyle and lateral tibial plateau– sites for DJD.
Genu Varus
Bow-legged
Femoral shaft < 10º from vertical.
Increased weight bearing on the medial femoral condyle and medial tibial plateau– sites for DJD.
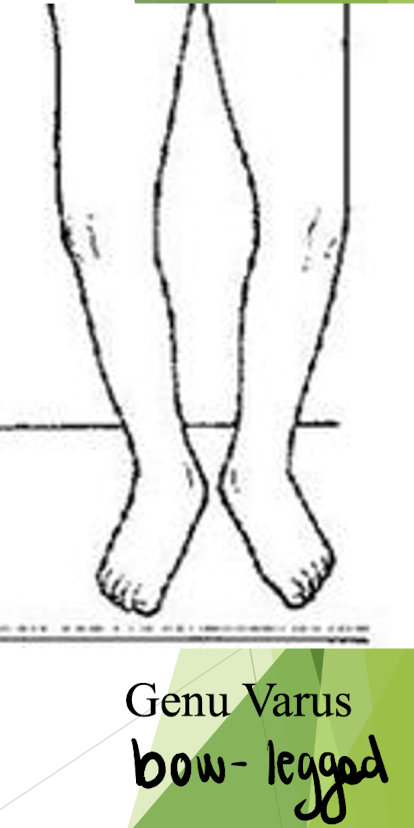
Alignment of Knees: Normal and Abnormal
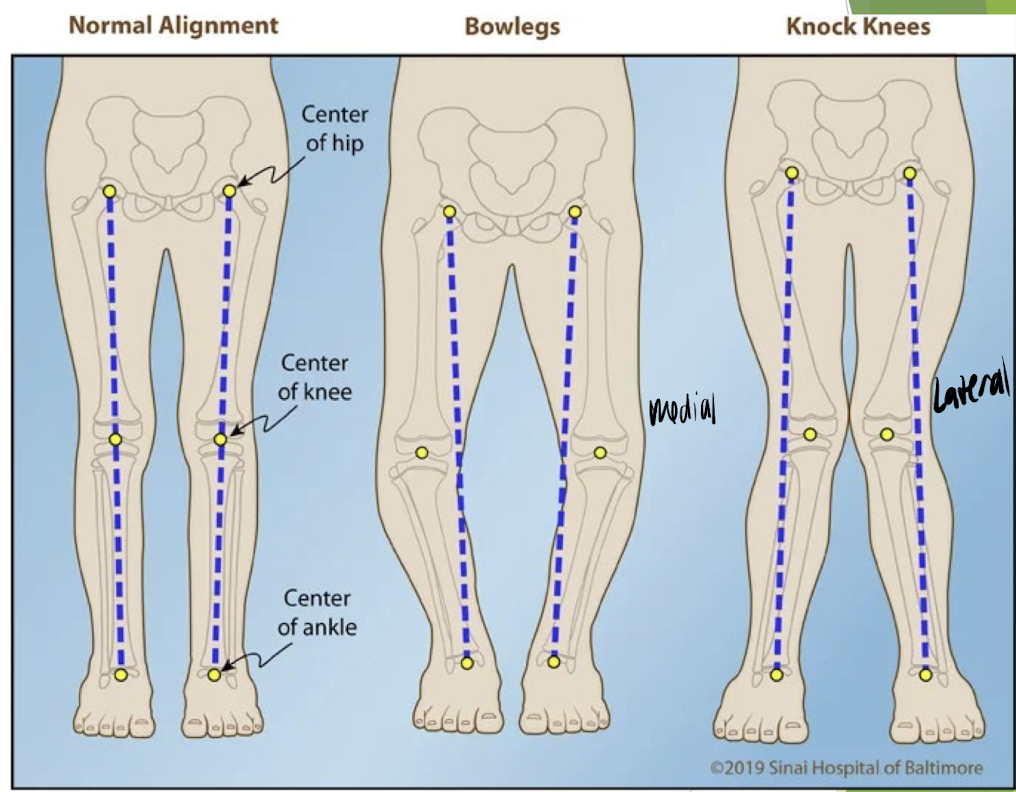
Genu Varus and Valgus Pictures
Tibia
The tibial plateaus are slightly concave and both the medial and lateral meniscus sit atop the plateaus.
The intercondylar eminence serves as the origin for the anterior and posterior cruciate ligaments.
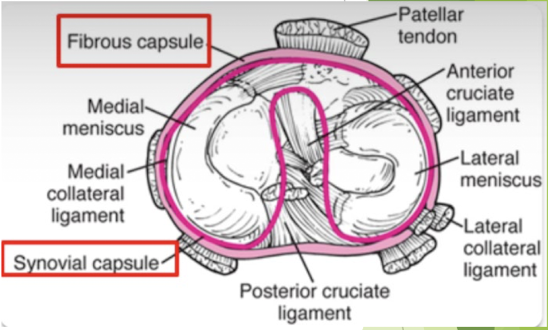
Knee Joint Capsule
Fibrous capsule attaches to the margins of the femoral and tibial condyles.
Synovial layer of capsule folds into the intercondylar notch; thus ACL and PCL are intracapsular but extrasynovial.
Knee Retinaculi
Fibrous bands that attach joint capsule to patella
Lateral retinaculum: blends with tendons of vastus lateralis; reinforced by slip from ITB
Medial retinaculum: blends with VMO
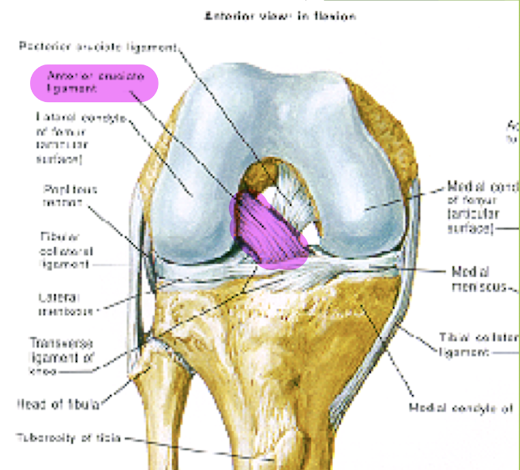
Anterior Cruciate Ligament (ACL)
Origin on anterior intercondylar eminence of the tibia to insert into medial side of lateral femoral condyle.
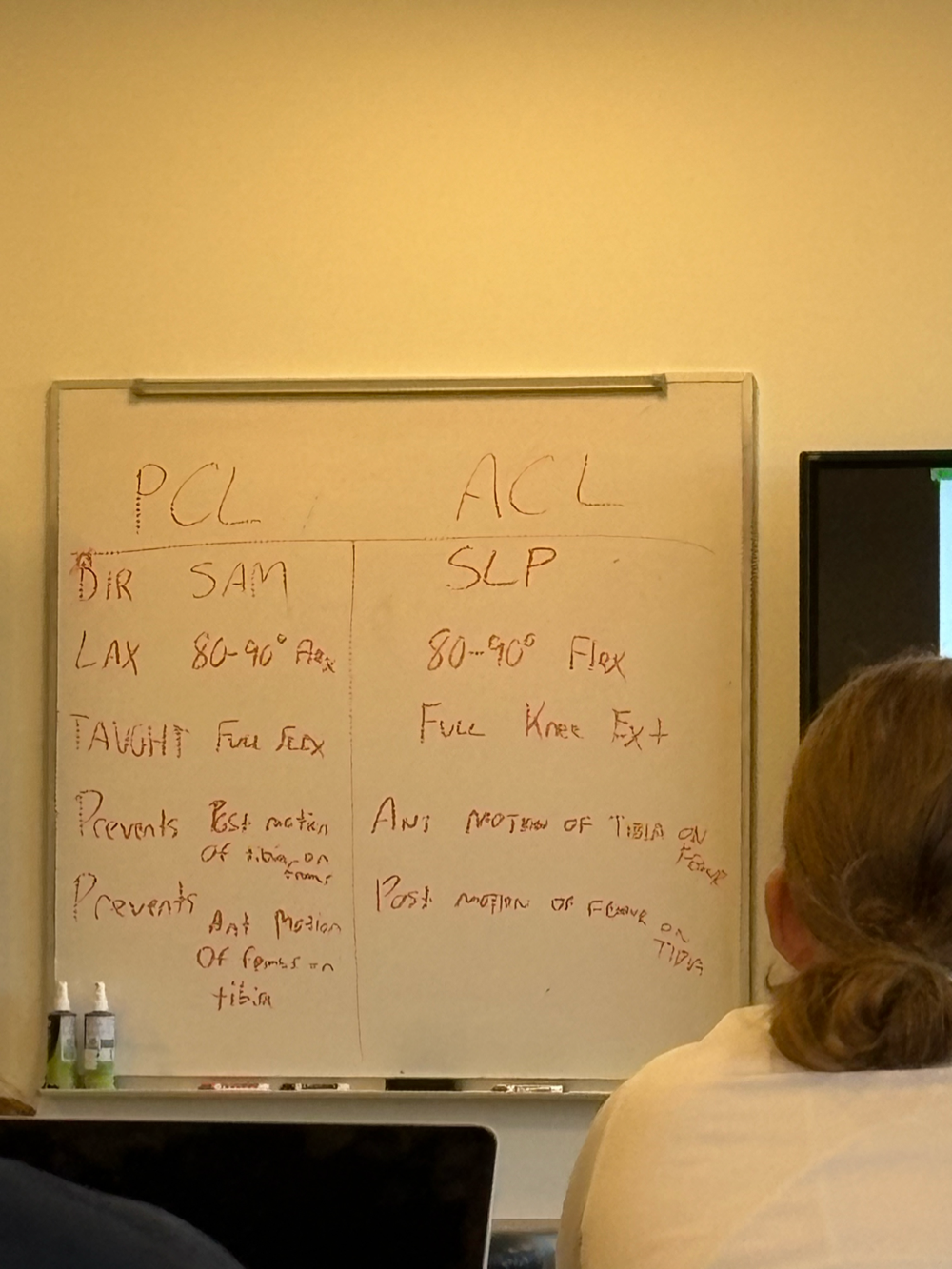
Runs superior-lateral-posterior direction (SLP)
Lies in the space between the fibrous and synovial layers of the capsule. Thus it is intracapsular, but extrasynovial.
The ACL has two main bundles: anteromedial and posterolateral
Facts about ACL
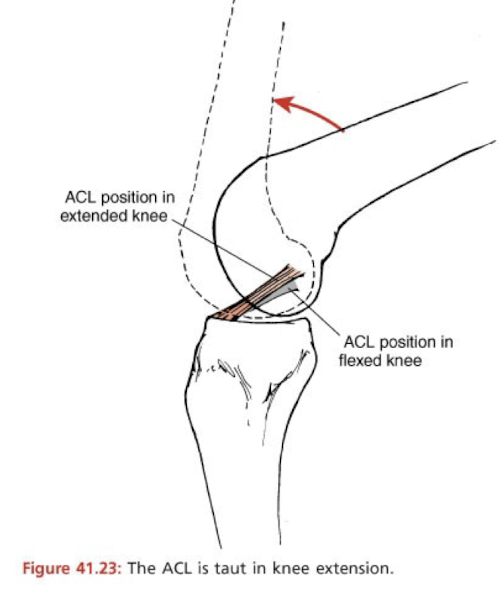
A portion of the ACL is ALWAYS taut throughout the entire knee ROM.
However, the ACL is most-lax in 80-90º of knee flexion.
The ACL is most taut in full knee extension.
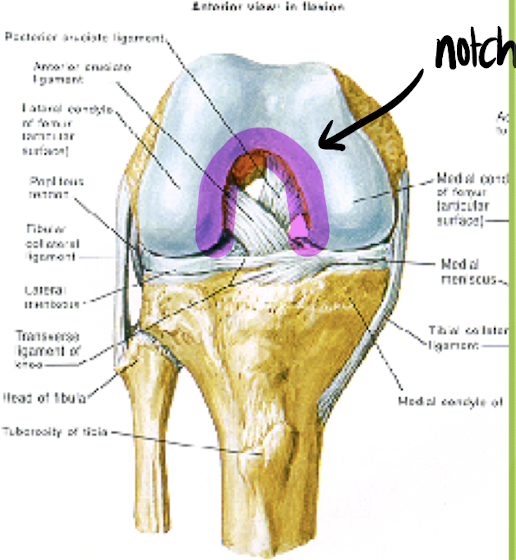
ACL and Intercondylar Notch
ACL comes into close proximity to the intercondylar notch in full knee extension.
A narrow or inverted V-shaped intercondylar notch has been associated with increased risk of ACL tear.
Surgeon will perform notchplasty to increase the size of the notch for the new ACL graft.
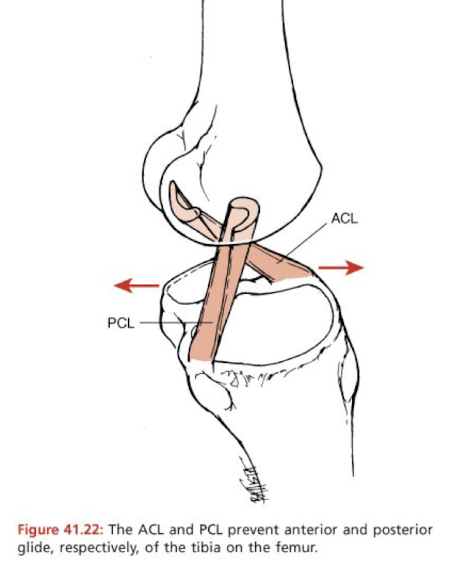
ACL Limits Excessive:
Hyperextension of the knee where femur moves posteriorly (limits shear forces)
Anterior translation of the tibia on the femur (limits shear forces)
Excessive rotation (IR) of the tibia, in either direction.
ACL: Non-contact injury (60-70% ACL tears)
Femur rotates on a planted foot (plant and cut maneuver)
Deceleration (often a precursor to a plant and cut maneuver, so the two mechanisms place stress on ACL)
Forceful hyperextension of the knee (such as common down from a jump and landing on one leg with that knee in extension- femur glides posterior on stable tibia)
ACL: Contact Injury (30-40% ACL tears)
Forceful blow to the lateral knee with the foot planted.
“Terrible Triad”= MCL, ACL, Medial Meniscus
The ACL provides up to ____ of the knee’s resistance to shear forces.
80%
Issues with ACL-deficient Knee
Increased shear forces lead to increased risk of secondary meniscal injuries.
Increased shear forces lead to increased risk of knee osteoarthritis (OA) long-term.
Posterior Cruciate Ligament (PCL)
Sits behind the ACL and its origin is on posterior portion of the intercondylar eminence. Runs Superior-Anterior-Medial (SAM) direction to attach to the lateral aspect of the medial femoral condyle.
What position does the PCL maintain throughout knee ROM?
Somewhat Taut
PCL– Most Lax Position
80-90º of knee flexion
PCL– Most Taut Position
As the knee approaches full flexion
What does the PCL do?
Prevent posterior motion of the tibia on the femur OR anterior motion of the femur on the tibia. Test- Posterior Drawer Test.
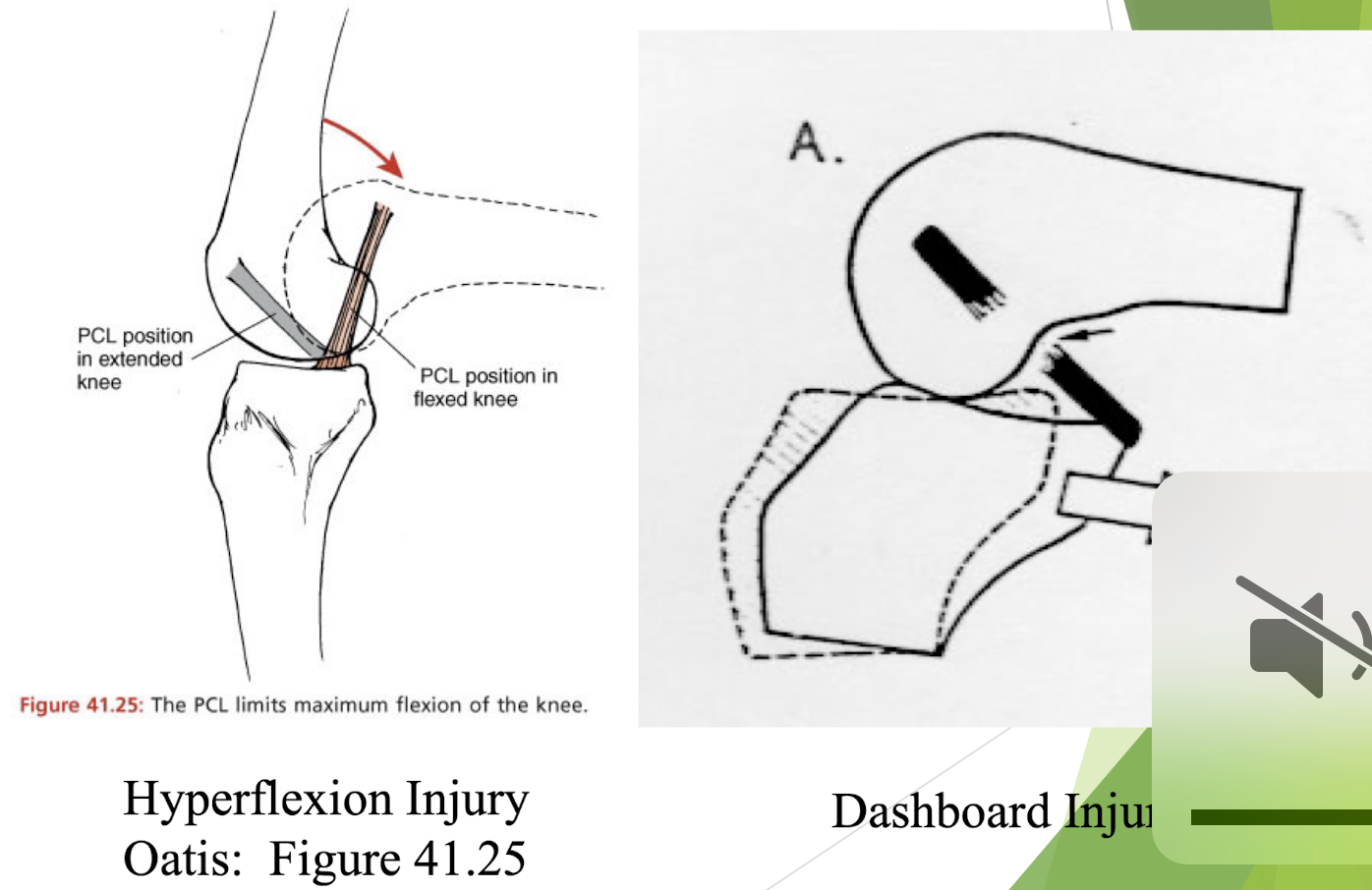
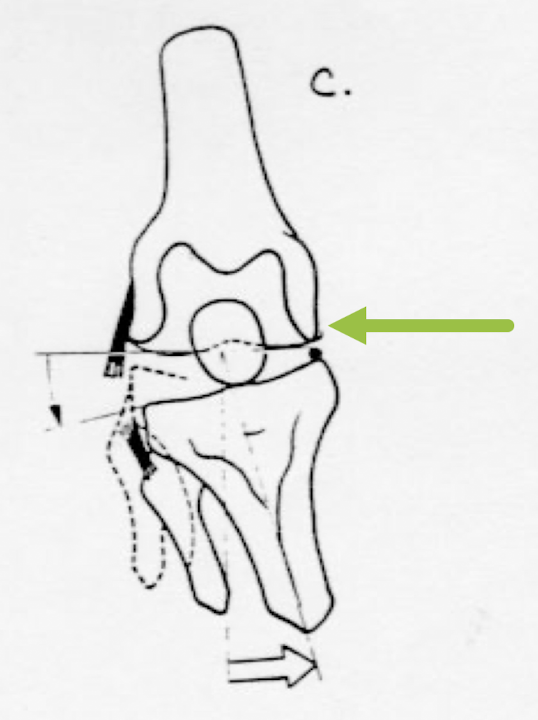
True or False: PCL injuries are much less common than ACL injuries.
TRUE– hyperflexion injury or tibia impact on dashboard.
Chart from Class of PCL and ACL
PCL Injuries Pictures
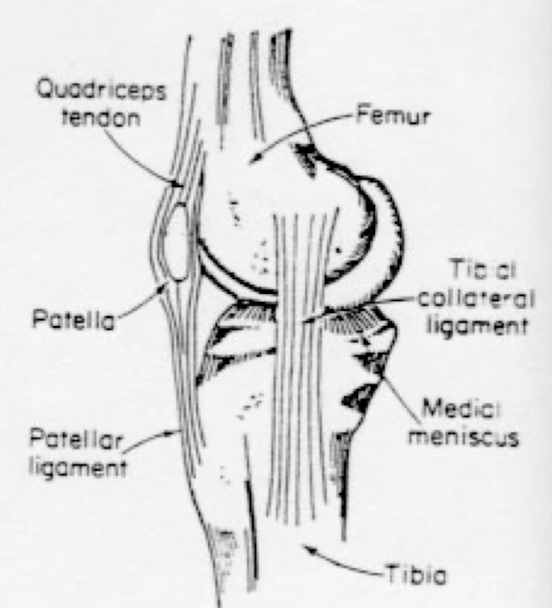
Medial (Tibial) Collateral Ligament
Flat, broad band that runs from medial femoral condyle to medial tibia. Anterior band: taut in flexion. Posterior band: taut in extension.
What is the primary role of the MCL?
Prevents excessive knee valgus, injured with contact blow to lateral knee, gaps medial knee.
What is the secondary role of the MCL?
Reinforces cruciates to prevent excessive tibial glide.
Terrible Triad
The MCL attaches to the medial joint capsule and thus to the medial meniscus. The ACL, medial collateral ligament, and the medial meniscus could potentially be injured together.
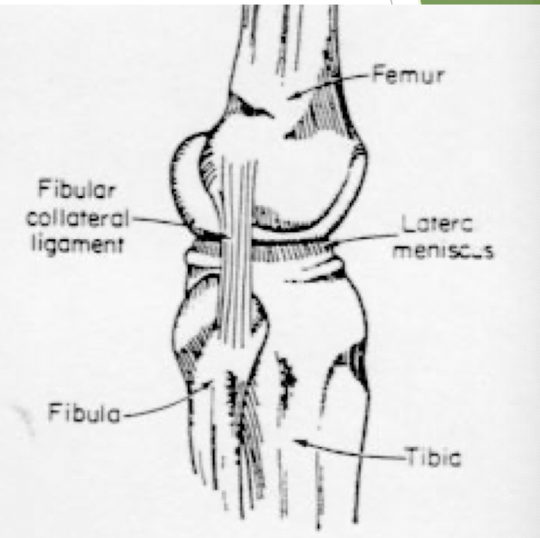
Lateral (Fibular) Collateral Ligament (LCL)
Cord-like and runs from the lateral femoral condyle to the fibular head. It does not attach to the joint capsule or the lateral meniscus.
What does the LCL prevent?
Excess varus stress to the knee. Contact injury from medial side of the knee– gaps lateral knee.
The collateral ligaments are taut in what position?
Full knee extension and lax in 90º flexion.
If the collaterals are taut, what does this limit?
Any tibial IR/ER in full knee extension.
Where are collaterals lax?
90º flexion which allows tibial IR/ER in knee flexion.
Blood Supply to Knee Ligaments
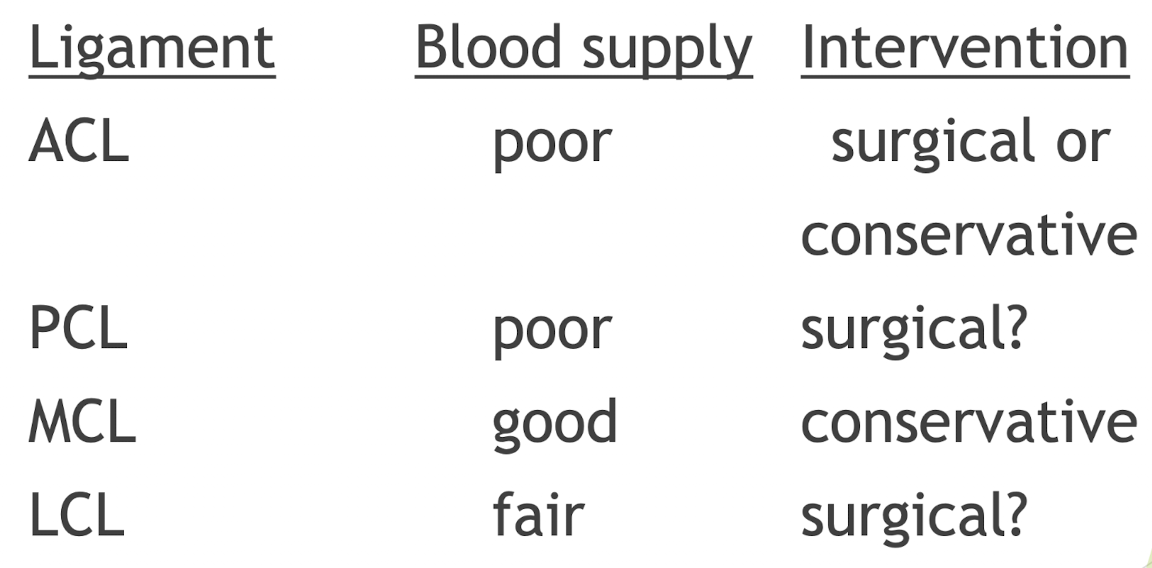
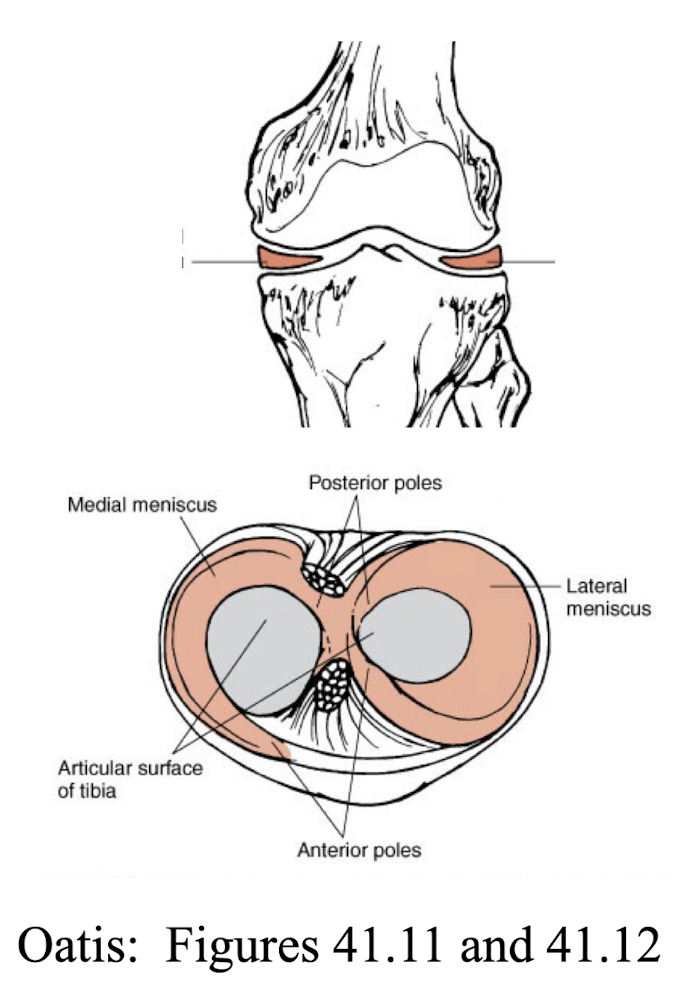
Menisci
Wedge-shaped sections of fibrocartilage that attach to the tibial plateaus via the coronary ligaments. Cover >50% of tibial plateau.
What are the function of the Menisci?
Act as shock absorbers.
Deepen the concavity of the tibia plateaus (add stability)
Increase the congruency of the joint surfaces (more effective weight distribution)
Where are the Menisci firmly attached to?
The tibial plateau but with enough slack so they can move with the femur.
Menisci Blood Supply
Only the outer 1/3rd has a definite blood supply (thus some healing potential). Remainder is avascular and not likely to heal.
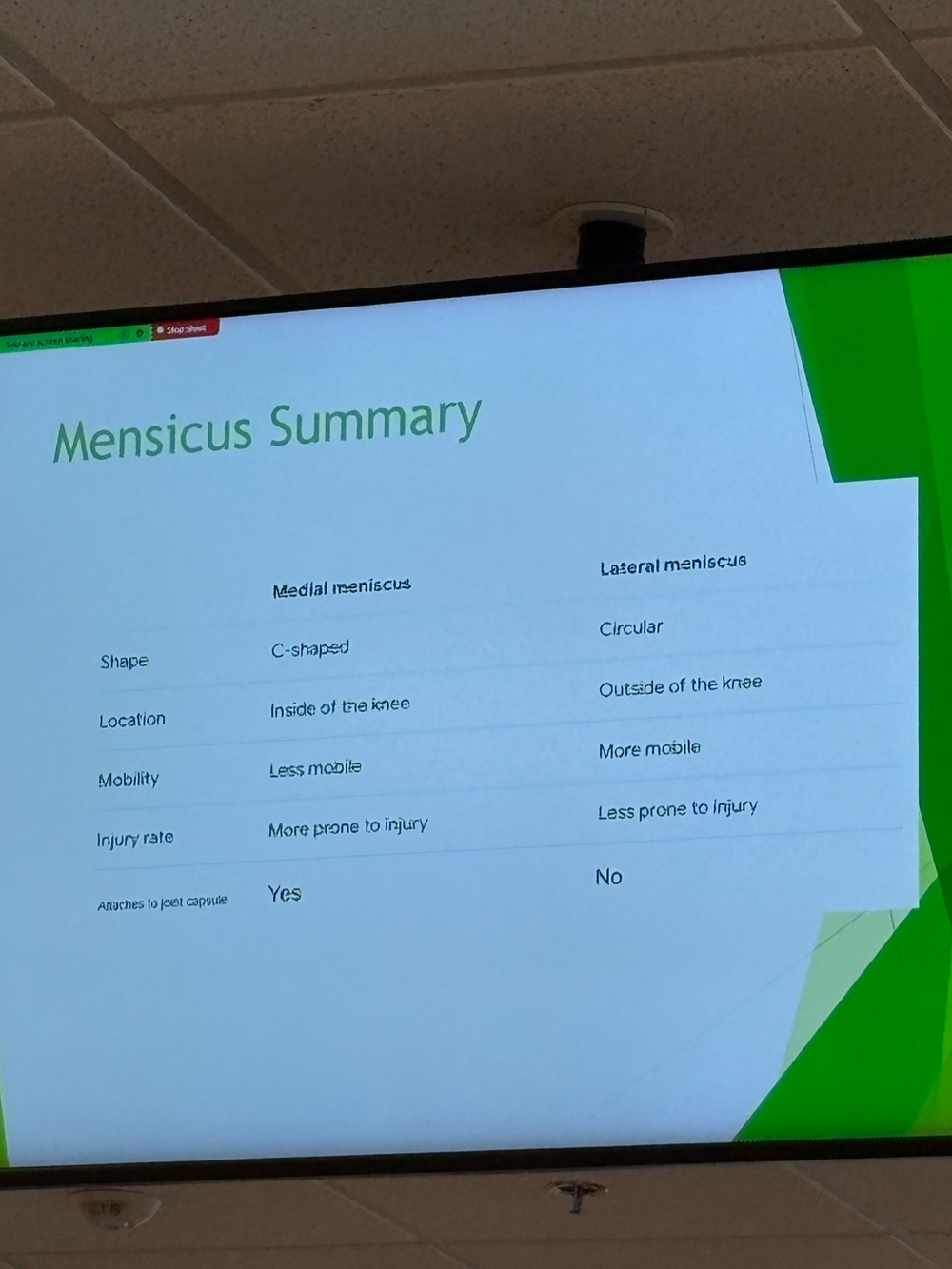
Medial Meniscus
Larger than the lateral meniscus and more oval-shaped. W
Where is the Medial Meniscus attached to?
Firm attachment to the tibia due to the coronary ligaments, also attachments to the joint capsule and the MCL.
Why does the medial meniscus have a fairly high injury rate?
Due to its multiple firm attachments.
Lateral Meniscus
Round shape and has no attachment to the joint capsule or LCL.
Where does the Lateral Meniscus attach?
Attaches fairly loosely to the tibial plateaus by the coronary ligaments.
Why does the Lateral Meniscus have lower incidence of injury?
The lateral meniscus has greater mobility and fewer attachments than the medial meniscus.
Menisci and Coronary Ligaments
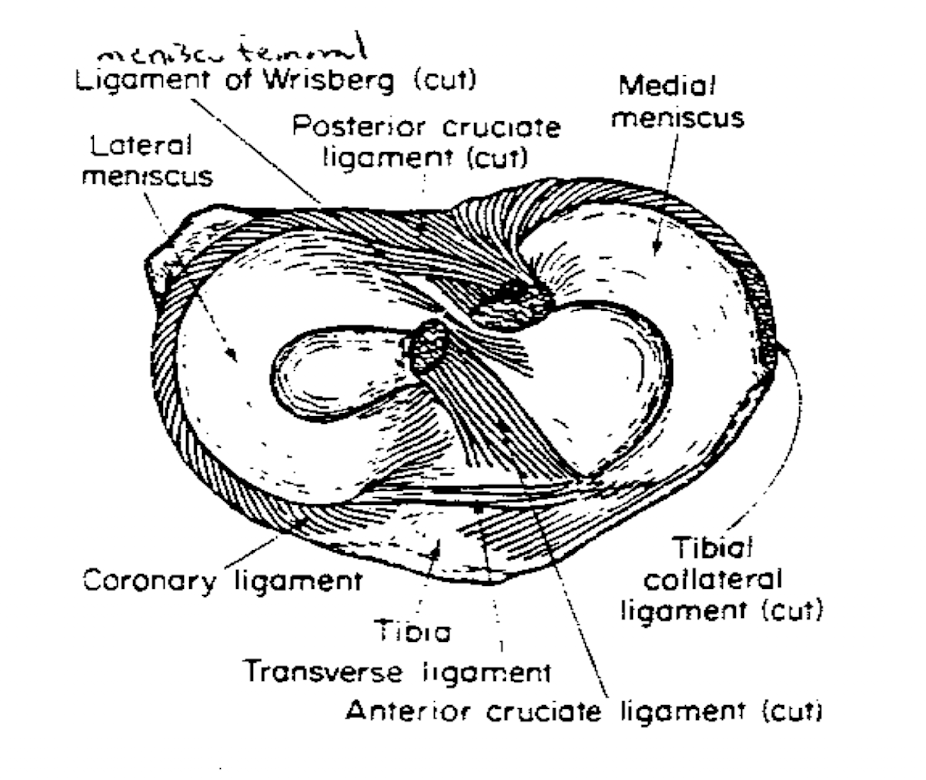
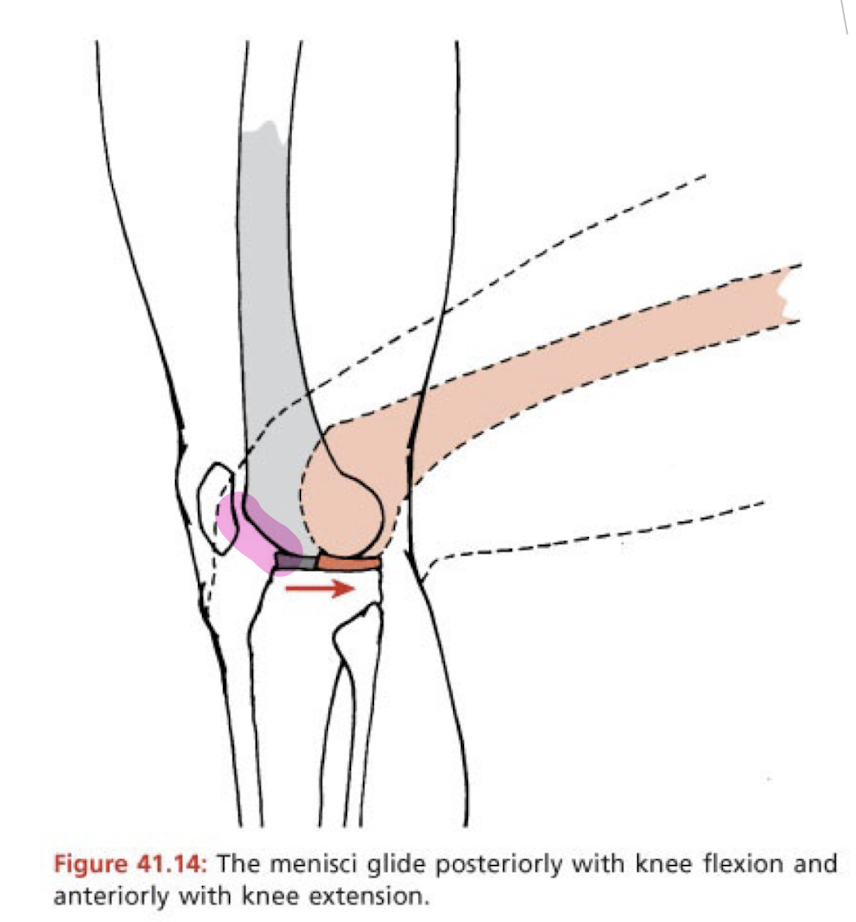
Meniscal Movement- Anteriorly
The menisci attach to the meniscopatellar ligament. During knee extension, both menisci are pulled anteriorly.
Meniscal Movement– Posteriorly
Both menisci attach to the semimembranosus, while the lateral meniscus attaches to the popliteus muscle. During knee flexion, both menisci move and are pulled posteriorly.
Meniscus Summary
Meniscal Movement Picture
Reasons for Frequent Meniscal Injuries
Large weight bearing joint; loads reach several times body weight– compressive forces.
Gliding movements of femur on tibia– shear forces.
Attachments to tibia make them more prone to injury, especially with rotary forces.
Torn meniscal tissue can fragment and dislodge, settling between bony surfaces– locking, clicking sensations.
What does knee stability depend on?
Primarily Ligamentous Structures
Secondary Knee Stability
Muscles (quad/hams), Menisci, Joint Capsule, Bony Congruency
Osteokinematic knee motions of flexion and extension are accompanied by what?
Gliding and rolling of the joint surfaces.
Open Chain Arthokinematics
Tibia moving on a stationary femur: Concave on Convex
Gliding and rolling of the tibia always occur in same directions.
Flexion: Posterior roll, posterior glide
Extension: Anterior roll, anterior glide
Open Chain Knee Flexion
Bone: Posterior
Roll: Posterior
Slide: Posterior
Open Chain Knee Extension
Bone: Anterior
Roll: Anterior
Slide: Anterior
Closed Chain Knee Flexion
Bone: Posterior
Roll: Posterior
Slide: Anterior
Closed Chain Knee Extension
Bone: Anterior
Roll: Anterior
Slide: Posterior
Closed-Chain
Gliding and rolling of the femur always occur in opposite directions to keep the femoral condyles centered on top of the tibial plateaus.
Gliding helps keep femur centered on top of the tibia. Flexion: Femur rolls posterior, glides anterior. Extension: Femur rolls anterior, glides posterior.
If only rolling occured, the condyles would fall anteriorly off the tibia during closed chain knee extension or fall off posteriorly during closed chain knee flexion.
Screw-Home Mechanism
In the last 20 degrees of knee extension, the tibia externally rotates (or the femur internally rotates) to “lock” the knee to add stability in full knee extension.
In closed chain movement, which ligament becomes taut to prevent excessive posterior movement of the femoral condyles?
ACL
Which femoral condyle is longer in A-P Direction?
Medial femoral condyle
Screw-Home Mechanism
Closed chain EXT: femoral condyles glide posteriorly.
The ACL tightens to limit this posterior glide.
ACL attaches to lateral femoral condyle; as the ACL tightens, it stops the lateral femoral condyle from gliding posteriorly.
However, the medial femoral condyle continues to glide posteriorly as it has a longer A-P length.
Thus, the femur internally rotates on the tibia.
How many degrees of total rotation occurs during the screw-home mechanism? (ACL deficient knee issue)
10º
Unscrew Mechanism
To flex the knee, the popliteus muscle helps unlock the joint by externally rotating the femur or internally rotating the tibia.
Normal Knee ROM
0º-135º (AAOS)
Walking Knee ROM
Stance phase 20º, swing phase 0º-68º
Up and Down Stairs Knee ROM
90º-110º
Rising from a Chair Knee ROM
90º
Tying Shoes Knee ROM
105º
Getting out of a Tub Knee ROM
130º
Knee Flexion Normal End Feel
Soft-Tissue Approximation
Knee Extension, Internal Rotation, and External Rotation Normal End Feel
Tissue Stretch
Normal End Feels
Tissue stretch, soft-tissue approximation, bone-to-bone
Abnormal End Feels
Bone-to-bone
Soft Capsular
Hard Capsular
Empty (due to pain)
Muscle spasm
Springy block (meniscus tear)
Knee Close Packed
Full knee extension and tibial external rotation/femoral internal rotation (via screw-home mechanism)
Knee Open-Packed Exception to the Rule
Capsular: 25º knee flexion (capsule most lax in this position– effusion)
Ligamentous: 80º-90º knee flexion (knee ligaments most lax)
Knee Extensors Prime Movers
Quadriceps Femoris Group
Knee Extensors Secondary Movers
TFL
What are the two common reasons for not being able to fully flex the knee?
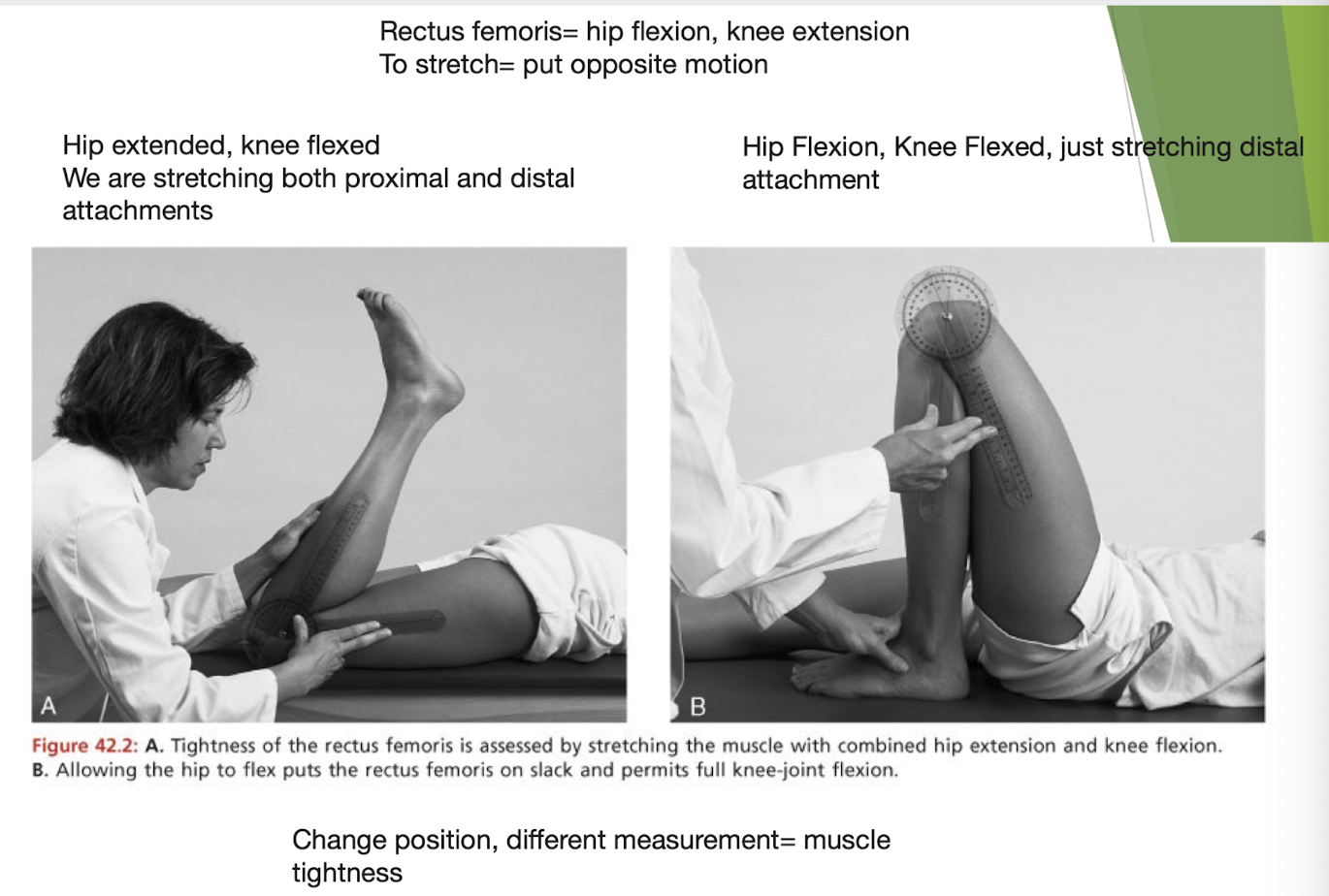
Rectus Femoris tightness or joint tightness
Where does the patella have the greatest effective lever arm length?
At 60º of knee flexion– quads are the strongest (greatest torque) at 60º.