Lung disease and control
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
54 Terms
What are the 2 categories of lung disease and what do they both reduce?
obstructive and restrictive
ventilation
What is obstructive lung disease?
reduction in flow through airways
What is restrictive lung disease?
reduction in lung/chest expansion
Which type of lung disease is characterised by chest wall abnormalities and muscle contraction deficiencies?
restrictive
What could cause the loss of compliance typical of restrictive lung disease?
normal aging process with which vital capacity goes down
increase in collagen = build up of fibrous tissue
exposure to env. factors like asbestosis
What should FEV1 % be in healthy lungs?
over 80%
What could the narrowing of airways in obstructive lung disease be due to? In all cases, does resistance to airflow increase or decrease?
Excess secretions
Bronchoconstriction – Asthma
Inflammation
increase
Can spirometry show obstructive lung disease? How?
yes, shows a decrease in FEV1 (goes below 80%)
Are Vital Capacity and lung volume modified in obstructive lung disease? What is?
shouldn’t be
FEV 1 decreases
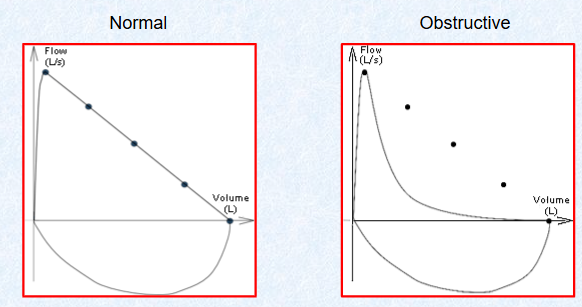
What is the key clinical feature of obstructive lung disease?
flow volume loop - linear in healthy, concave in obstructive lung disease
Name 4 examples of obstructive lung diseases
Chronic Bronchitis
Asthma - most common
Chronic obstructive pulmonary disease (COPD)
Emphysema
Describe the pathology of chronic bronchitis
persistent cough and excessive mucus secretion (3 consecutive months in the last 2 years)
Describe the pathology of asthma
inflammatory disease with hyperactive airways, inflammatory cells move into airways and release inflammatory mediators like histamine = bronchoconstriction
What are the 2 types of triggers for asthma?
Atopic (extrinsic) – allergies, contact with inhaled allergens.
Non-Atopic (intrinsic) – Respiratory infections, cold air, stress, exercise, inhaled irritants, drugs like ibuprofen.
Describe the pathology of COPD (chronic obstructive pulmonary disease)
structural changes - increase in resistance of small airways
Describe the pathology of emphysema
decline in the alveolar surface area available for gas exchange bc of loss of elastic recoil nature
What’s a short-acting treatment for asthma?
short-acting β2-adrenoceptor agonists – salbutamol = dilation of airways
What’s a long-acting treatment for asthma?
Inhaled steroids. Glucocorticoids such as beclometasone, act to reduce the inflammatory responses.
Long acting β-adrenoreceptor agonists
Muscarinic antagonists - reduce constriction
How do β2-adrenoceptor agonists like salbutamol increase airway diameters? How does this impact resistance to airflow?
act like adrenaline/noradrenaline and elevate cAMP
goes down, air flow goes up
Are Vital Capacity and lung volume modified in restrictive lung disease? What is?
vital capacity and FVC decrease but FEV1% (BC RATIO, both go down but not their relative amounts) stays the same or even goes up
In which type of lung disease does FEV1 % decrease while FVC is unchanged?
obstructive lung disease
In which type of lung disease does FVC decrease while FEV1 % is unchanged or increased?
restrictive lung disease
What does the flow-volume loop curve of restrictive lung disease look like?
shape is normal (linear) but reduction in the volumes of air moved + reduction in peak flow
How does asbestosis lead to loss of compliance?
fine asbestosis particles enter lungs and are recognised as foreign, mucus and tissue are synthesised to move them out but this fails = slow build-up of fibrous tissue = loss of compliance
If a patient comes into a clinic with a vital capacity reduced below that expected for height, age, sex etc, which kind of disease would be diagnosed?
restrictive or mix of obstructive and restrictive
If a patient comes in with a reduced FEV1 below 80%, which kind of lung disease would be diagnosed?
obstructive
Is breathing an involuntary, automatic process?
Automatic and involuntary most of the time but can be modified consciously
Give an example of when breathing can be consciously modified. Are these long term or temporary?
hyperventilation and breath holding
temporary and can be overridden
Where is the basic respiratory rhythm generated?
centres in the medulla
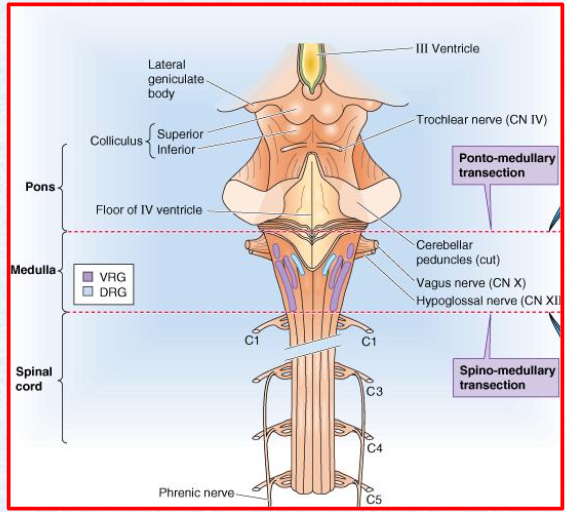
Using this diagram and ur knowledge, what would the effect of a lesion between the pons and the medulla have on breathing pattern?
normal breathing pattern maintained
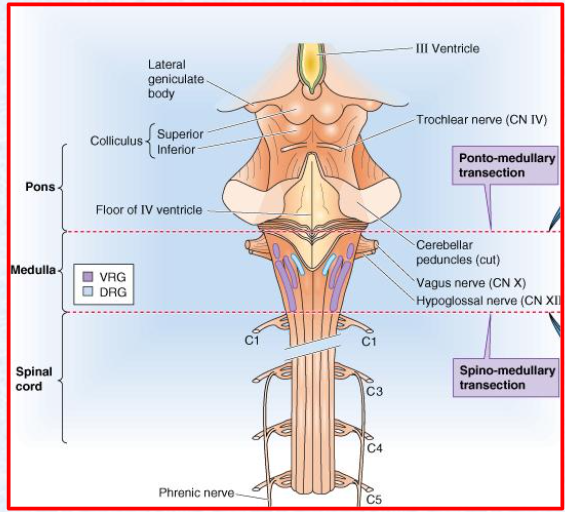
Using this diagram and ur knowledge, what would the effect of a lesion between the medulla and the spinal cord have on breathing pattern?
would stop bc breathing pattern comes from medulla
Through the firing of which nerves is the basic breathing pattern initiated in the medulla, therefore triggering quiet inspiration?
pre botzinger complex (preBötC
Which centre of the medulla controls quiet respiration? Through the activation of which muscles?
DRG - dorsal respiratory group
inspiratory muscles
Which centre of the medulla controls forced inspiration and expiration?
Ventral Respiratory Group (VRG)
Which centre of the medulla is inactive during quiet respiration?
Ventral Respiratory Group (VRG)
Where are signals from the medulla centres sent to control respiration?
down to the diaphragm for contraction

How can we see on this diagram that DRG activity (at the bottom) controls lung volume ie quiet respiration, at the top? How long do inspiration and expiration last during quiet respiration?
active inspiratory neurons increase rapidly through a rapid positive feedback loop (for about 2s) then they cease their activity = expiration ie release/elastic recoil of lungs (for 3s)
Which centre within the brain stem controls voluntary breathing?
pons
Which aspects of respiration does the pons regulate ? By sending stimuli to which centre in the brain?
rate and depth of breathing
medulla
What are the 2 centres of the pons centre?
pneumotaxic and apneustic centres
How does the pneumotaxic centre of the Pons affect inspiration? Does it have an inhibitory or stimulatory effect on the inspiratory centre?
increases the rate of ventilation by shortening inspirations
inhibitory
How does the apneustic centre of the Pons affect inspiration? Does it have an inhibitory or stimulatory effect on the inspiratory centre?
increases/prolongs the depth and reduces the rate by prolonging inspirations
stimulatory
What effect does the Hering-Breuer reflex have on inspiration? What does this prevent and through the activation of which receptors?
limits it to prevent over-inflation of the lungs
Stretch receptors in the lung send signals back to the medulla
Is the Hering-Breuer reflex an example of positive or negative feedback loops? Explain it briefly
negative
lungs inflate, stretch receptors detect this and send inhibitory signals to the medulla through the vagus nerve which stops lungs from inflating too much
What are 2 types of chemoreceptors in the lungs?
central and peripheral chemoreceptors
What conditions do central chemoreceptors monitor and where? Do they act indirectly or directly on ventilation?
ph and CO2 in cerebro-spinal fluid
indirectly
If CO2 goes up, how is pH affected? What response would this lead to? Which receptors would be responsible for this?
pH goes down (acidosis) + increase in ventilation to blow off CO2
central chemoreceptors
Where are peripheral chemorecptors located?
What conditions would stimulate a response from peripheral chemoreceptors? Which would is the primary driving force of a response and which is least likely to provoke one?
Increase in CO2 - primary driving force
Decrease in pH
Decrease in O2 - least likely, would have to be a dramatic drop
How does stimulation of peripheral chemoreceptors affect ventilation?
increases it
What is the effector of quiet respiration? What sub-centre and centre of the brain control it?
diaphragm
dorsal respiratory group, medulla
What are the effectors of forced respiration? What sub-centre and centre of the brain control it?
external and internal intercostals and abdominal muscles
ventral respiratory group, medulla
What are stimuli for the medulla?
CO2 and pH and sometimes O2
What are stimuli for the pons? Through the activation of which system in the brain is a signal sent to the pons?
emotions and voluntary control
limbic system