Cariology Exam One [Diets and Caries Marshall]
1/125
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
126 Terms
What is the difference between sugar and sugars
Sugar refers to sucrose
Sugars refers to monosaccharides and disaccarides
What is the difference between nutritive and non-nutritive
Nutritive = Ones you get calories from
Non-Nutritive = Ones you don't get calories from
Define Refine
to bring to a pure state; free of impurities
EX/
Field corn
- Cornmeal
-- Cornstarch
--- Corn syrup
---- HFCS
In each processing step of refining
We remove fiber and nutrients and we concentrate the simple sugars
With respect to caries: Each step of refining
Decrease the workload for the bacteria. Increasing the bioavailability of the sugar or starch
Make easier for them to ferment the carbohydrates
Modified starches
modified for a specific function/ quality for food products - very intentional by food industry
Used as
- Thickeners
- Stabilizers
- Binders
- Emulsifiers
Modified starches: How did we modify
- Oxidized, hydrolyzed by acid, gelatinized
- Chemical structure changed
- Effectively reduced the number of steps before the "starch" is cariogenic
Observational studies
The investigator watches whats going on. There is no intervention
In observational studies the focus is mainly on sugar (Ie. change in sugar intake). But it may not just be the sugar because
other things may be going on in the patients environment
DMFT
Decayed missing filled teeth
DMFS
Decayed missing filled surfaces
STUDY: Sugar intake vs caries prevalence
Design:
- Comparison of sugar availability and the DMFT scores of 12 year old children by country
- Left hand side we see sugar supply
- Right hand side DMFT
We see:
- As you increase sugar you see an increase in the DMFT scores
Supports the hypothesis one may see more caries

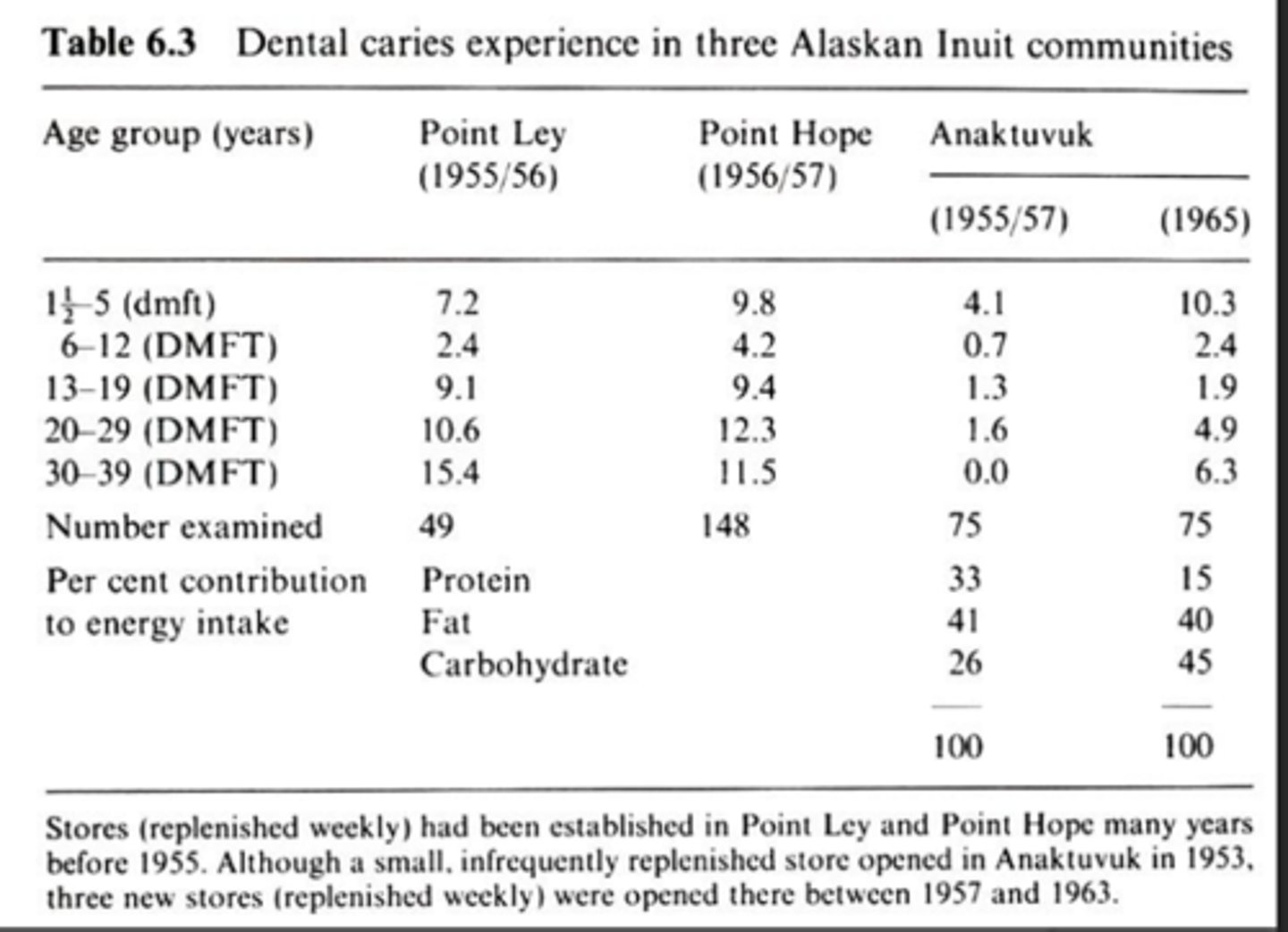
STUDY: Caries prevalence before and after sugar introduction
Design:
3 Inuit communities
- 2 (Point Ley and Point Hope) had sugar and white flour prior to 1950
- Anaktuvuk- Sugar and white flour were introduced in 1953
Two things to look at here
- Anaktuvuk that recently got the sugar introduced had lower caries (DMFT) for all ages in 1955/57 then the other two areas
- With time and that sugar exposure their caries increase to a comparable amount to the other sites
Takeaway:
1. Individuals moving to the states from developing countries and adapting our diets are at a higher risk of caries then they were at their home country
2. Developing countries where we export our highly processes foods we are exporting caries and obesity
STUDY: Caries prevalence before and after sugar introduction
Design:
Tristan Da Cunha
- Island store began carrying sugar and refined flour in 1940
- Mean daily sugar/flour consumption increased from 4.2 g/day (1938) to 350 g/day (1966)
All groups you can see an increase in DMFT with time and exposure
Concern with diets where we introduce sugar is we get entire cultural changes. Hard to tease out sugar from overall diet processing as well as lifestyle factors

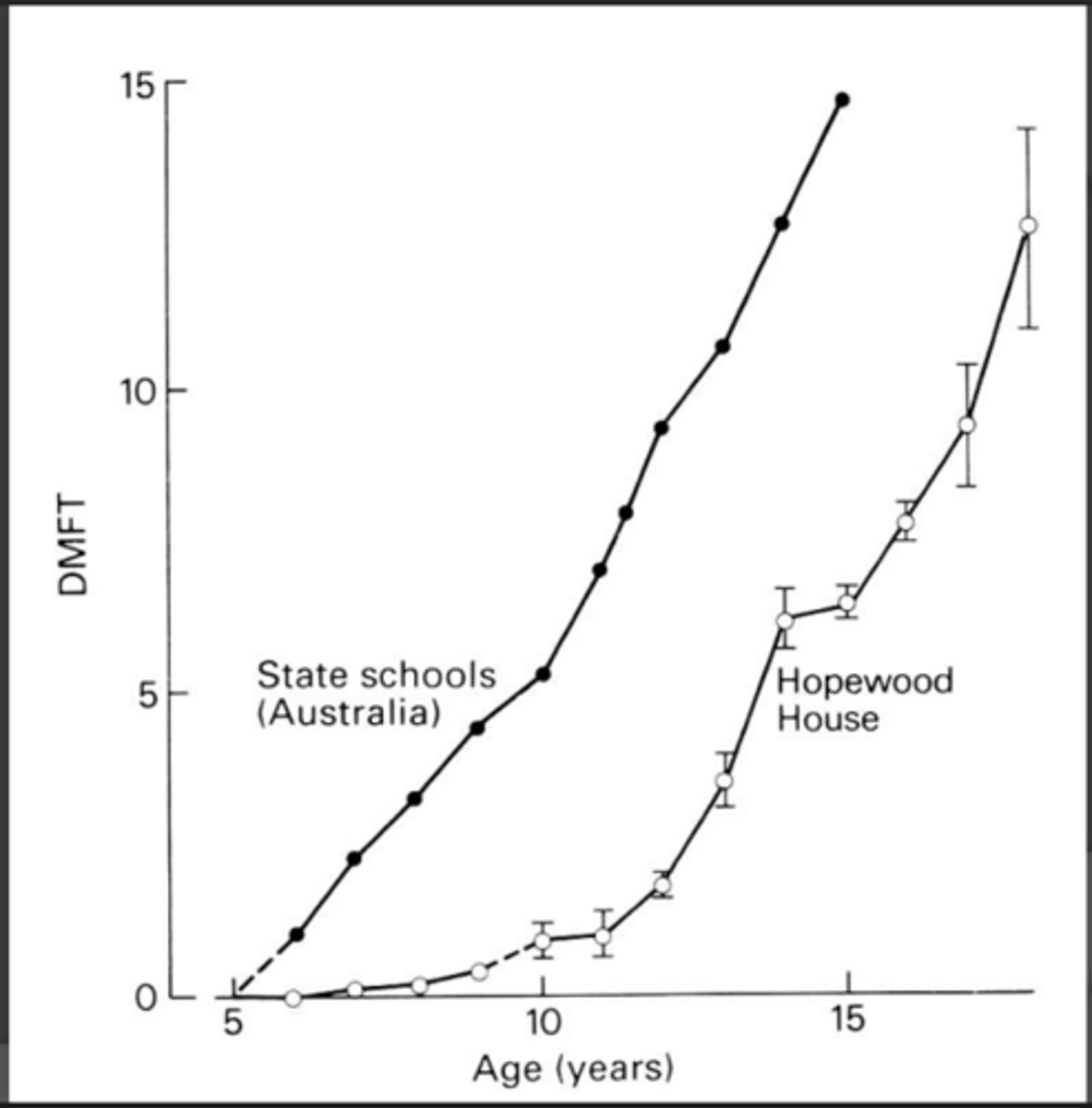
STUDY: Caries prevalence on diets low in sugar: population living within "westernized cultures"
Hopewood house, South Wales, Australia
Design:
- Birth-12 years: lactovegetarian diet emphasizing whole grains, raw vegetables and minimal sugar or white flour
- 12 years: "westernized" diet of local community
*definitely important for exam*
While they were at Hopewood house with very little sugar or flour (0-10) the Hopewood house had significantly less DMFT (lack of exposure was protective)
at age 12 they moved and adapted the diet of their peers: Their caries rate paralleled their peers.
Takeaway:
- The limited exposure to sugar and refined flour was protective while it wasn't there but it did not offer lifelong protection of caries
STUDY: Caries prevalence on diets low in sugar: populations living within "westernized" cultures
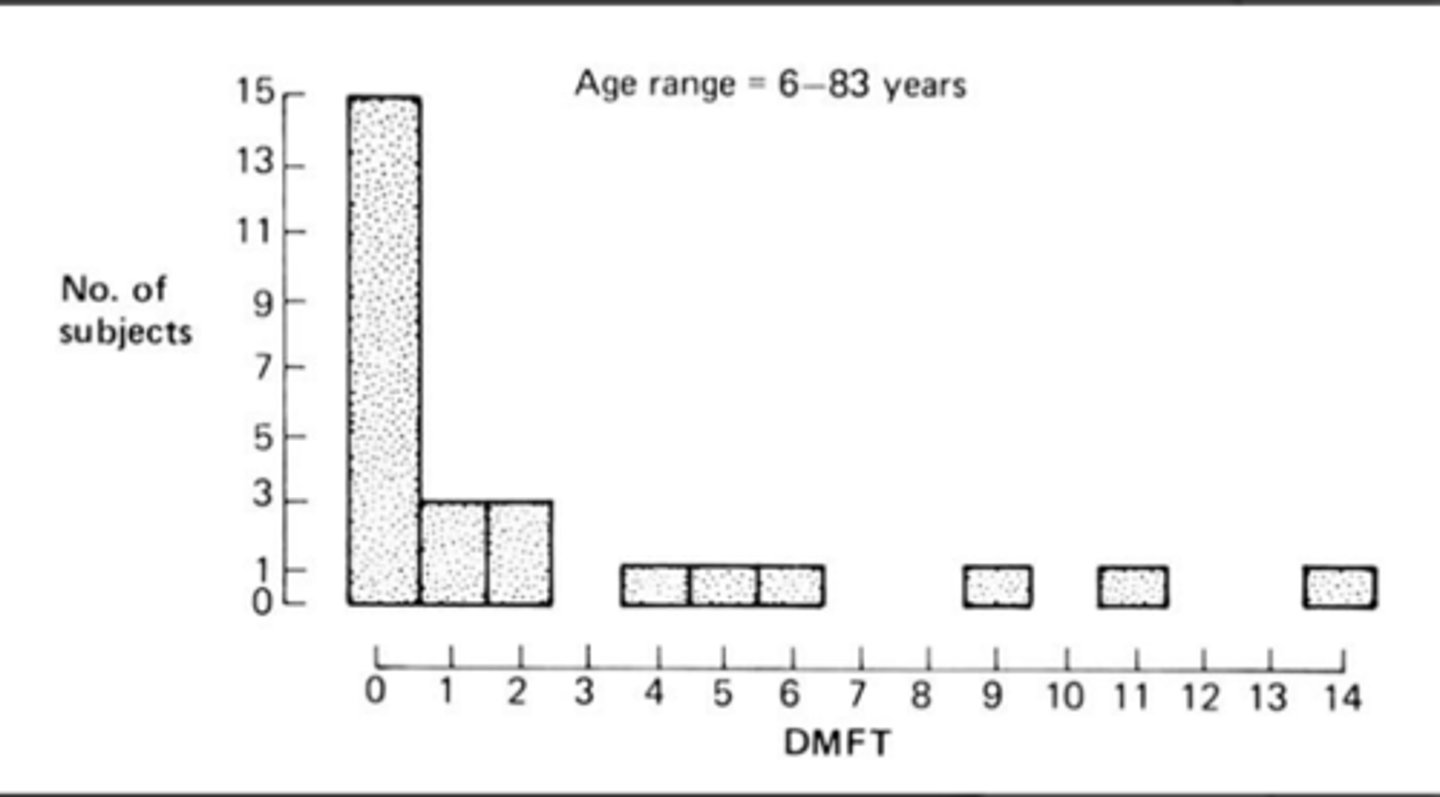
Hereditary fructose intolerance
- Inborn error of metabolism- can't split fructose
Image shows individuals who have the disorder and their DMFT scores
- Kids typically avoid sugar and results in less DMFT.
- Some of the results are from individuals who were forced to eat sugar as kids
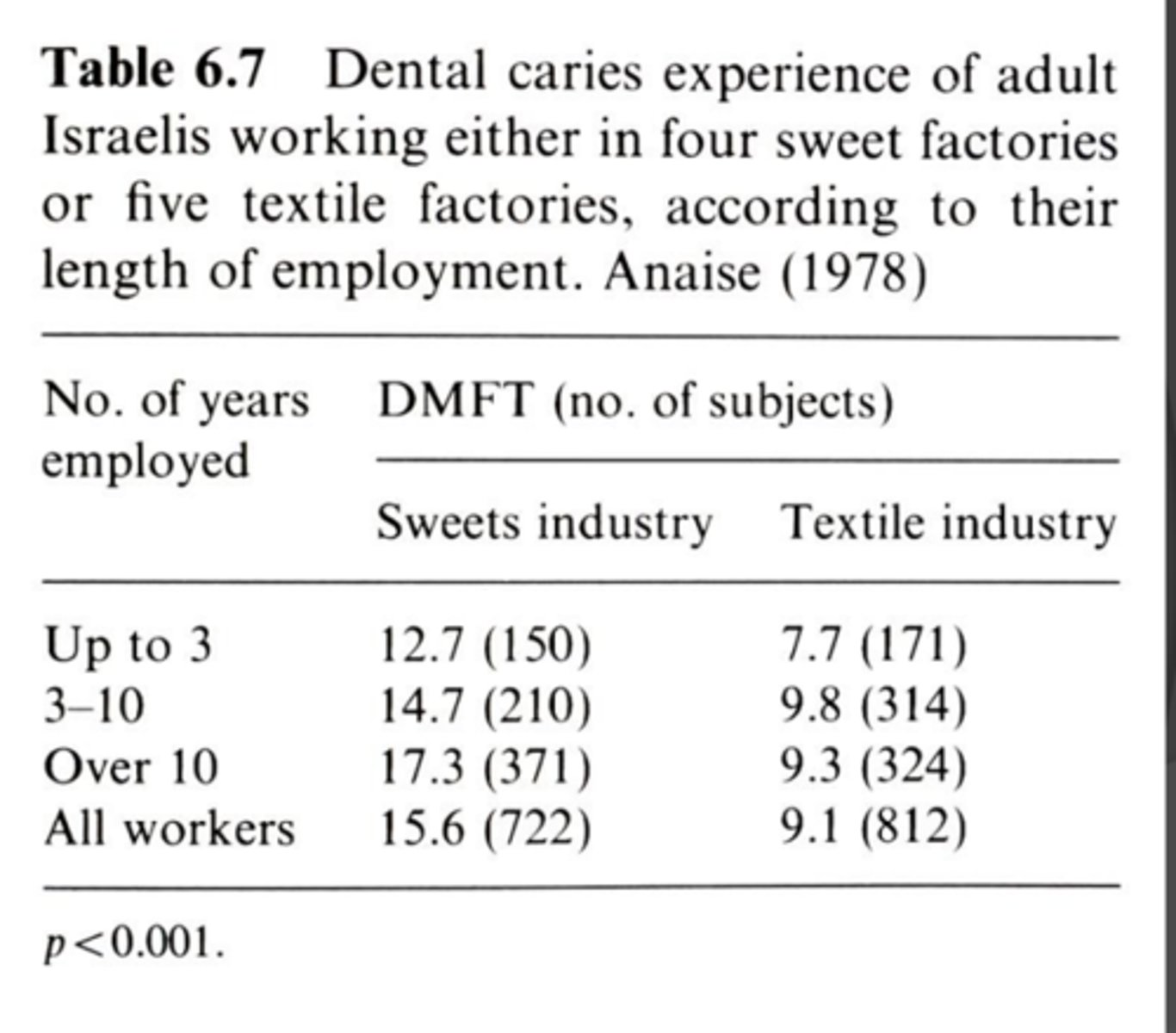
Caries prevalence on diets high in sugar
- Employees of the confection industry
Sweets industry vs Textile industry
Sweets industry: In time there is an increase in caries prevalence
Textiles industry: No real increase in caries over time and also is less then those in the sweets industry
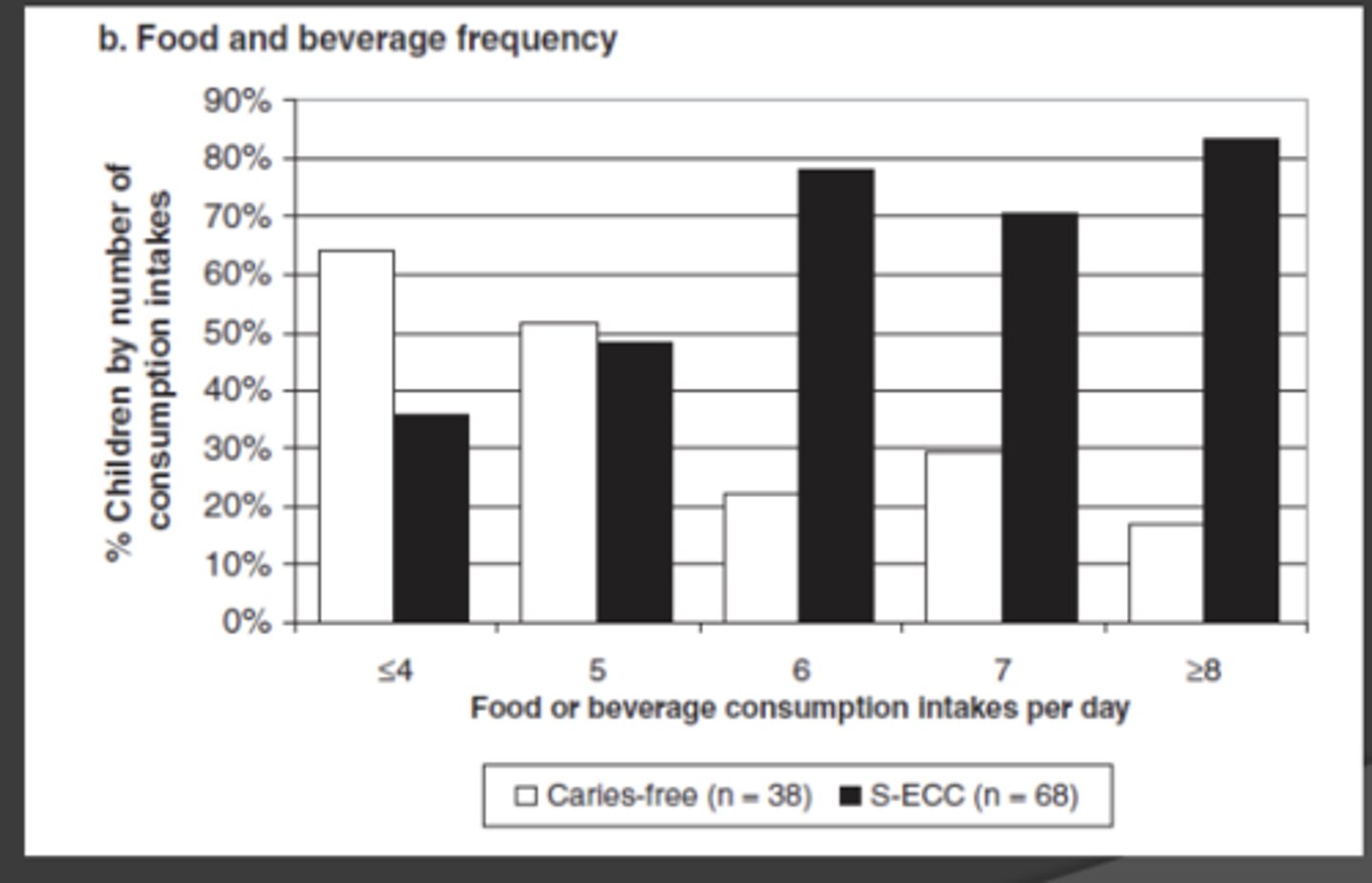
Frequency of any food or beverage intake on caries outcome
- Contemporary society
- Hour intervals
STUDY: Cross sectional
Young kids who were either caries free or had severe early childhood caries requiring surgical treatment
Takeaway:
With increasing number of exposures we see an increasing number of children with early childhood caries and a decreasing in those without early childhood caries
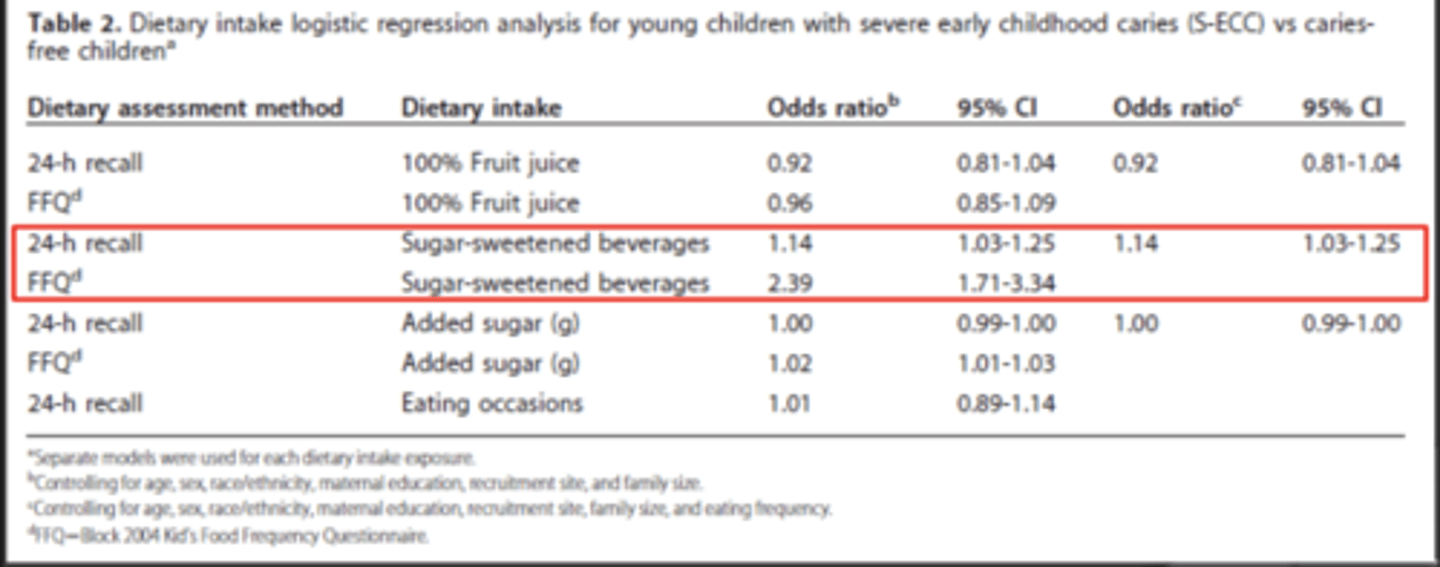
Cross Sectional study:
Sugar Sweetened Beverages and Early Childhood caries
Subjects:
2-6 year old, healthy children
- caries free
- SECC: 3+ smooth surface lesions with 1+ pulpal involvement
Exposure:
Tools: 24 hour recall and Block FFQ
- 100% fruit juice
- SSB
- Eating occasions
Outcome
- Caries
Takeaway:
Regardless of how they looked at it the factor that increased caries risk was the sugar sweetened beverages (SSB)
Did not see a major impact from the fruit juice or the eating events
STUDY: Dr. Levy's IFS data (longitudinal/cohort)
Strength: Having exposure data before outcome
Caries at 17 years: lifelong impact of beverages - fluoride- toothbrushing
Objective:
Investigate associations between childhood and adolescent beverage intakes and age 17 caries experience, while adjusting for fluoride and toothbrushing
Exposure:
- Beverage intakes
- Toothbrushing events
- Fluoride
Outcome:
- Caries experience adjusted for surfaces
-- DFSAR
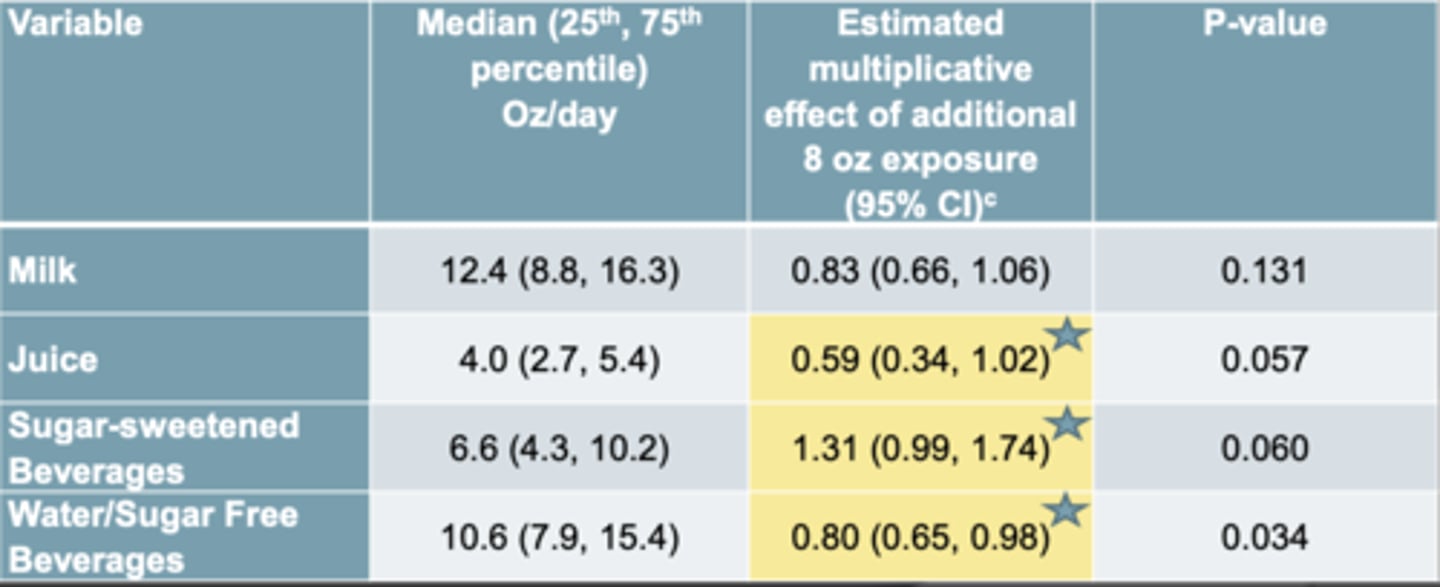
Data before adjustments
Takeaway:
The juice and the water seemed to protect against the caries where the SSB increased the risk of caries
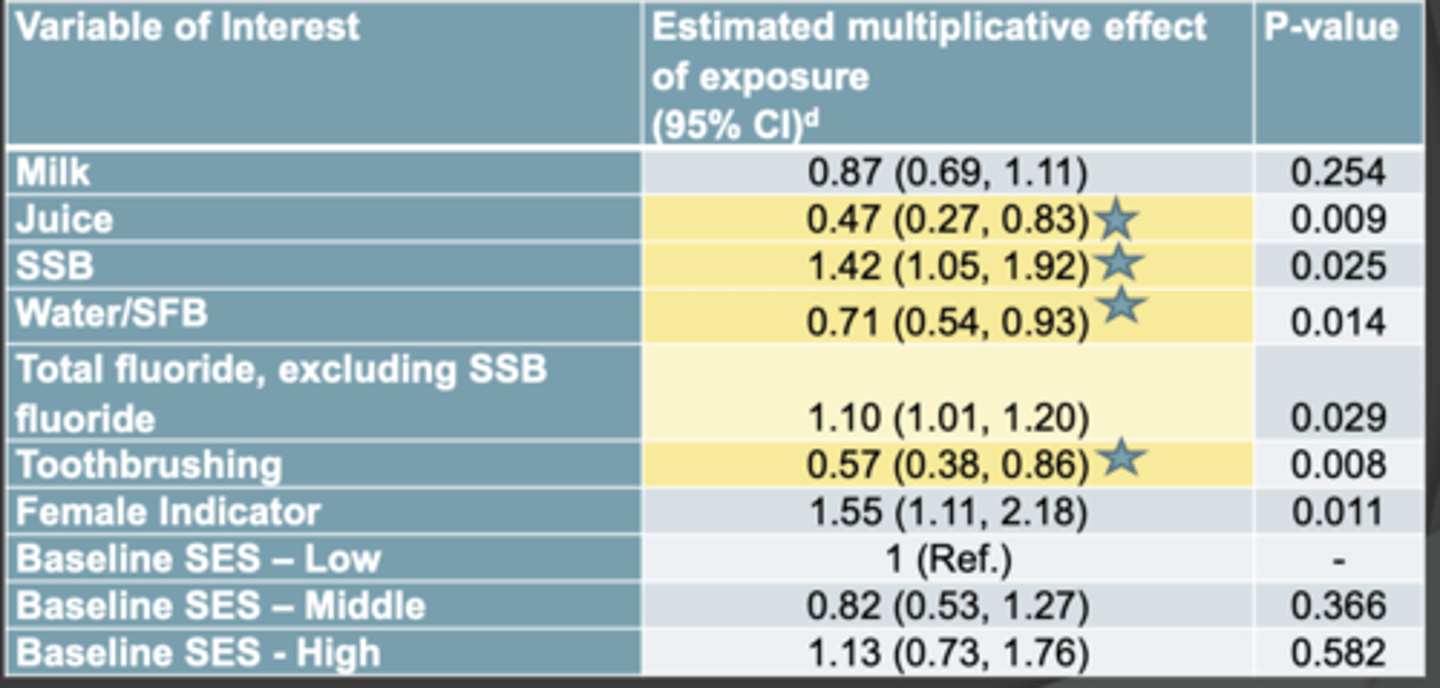
Levy's study: After adjusting for all the other stuff
Adjusted for:
- Beverage intake
- Total fluoride excluding ssb
- Toothbrushing
- Sex and SES
Takeaway:
- The SSB increases caries
Why was juice protective
- Nobody knows
OBSERVATIONAL STUDY SUMMARY: Sugar consumption is
positively associated with caries incidence
OBSERVATIONAL STUDY SUMMARY: Diets high in _________ offer current, but not future, protection against caries
unrefined carbohydrates
OBSERVATIONAL STUDY SUMMARY: Consumption _______ is positively associated with caries risk
frequency
OBSERVATIONAL STUDY SUMMARY: Added sugar sweetened beverages are _______ associated with caries risk
positively
Clinical studies
- Clinical= humans were involved
- Clinical studies are a type of experimental study.
- Experimental implies that the investigator is in charge- there's an intervention or a challenge of some sort
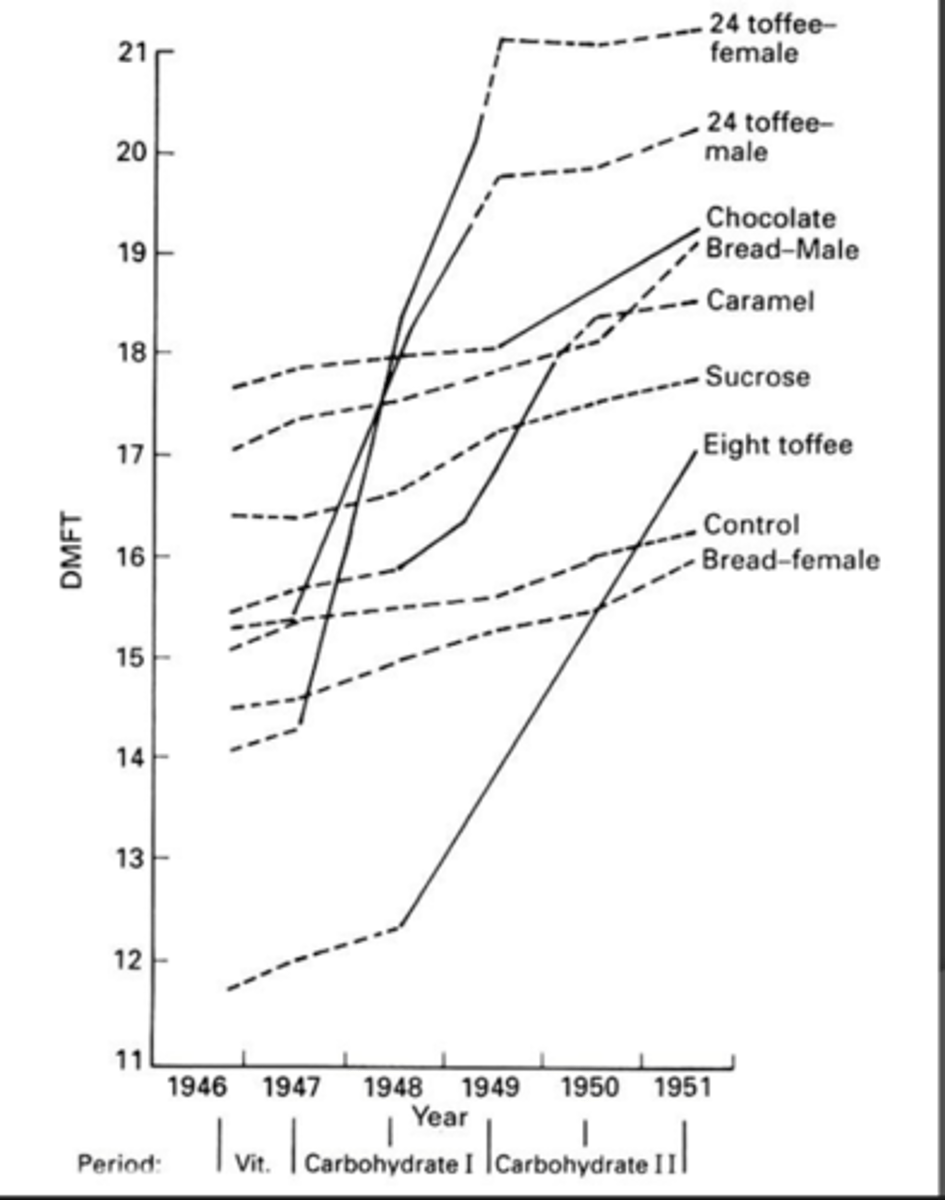
STUDY
Vipeholm, Sweden
Objective:
Determine how caries incidence is influenced by
- Mealtime exposure to non-retentive sugars
- Mealtime exposure to retentive sugars
- Between meal exposures to retentive sugars
Design:
- 960
- Mental hospital with 12 wards (4 wings and 3 floors); diets assigned by ward (no sharing)
*Definitely on exam*
Total DMFT scores including existing lesions
Straight lines: at and between meal exposures
Dotted line: meal exposures
Takeaway:
- When you have the at and between the slope is much higher than when just exposures during meals. This suggests that:
1. Between and at meals increase risk
2) At meals only not so much
Vipeholm but only looking at new lesions
Again
Just at meals not as much of an increase as between and at meals

Big summary of Vipeholm study
1. Sugar at meals- minimal impact on lesions
2. Sugar at and between meals- major impact on caries
3. (not shown) but not everyone gets caries and a few get caries with minimal carbohydrate exposures
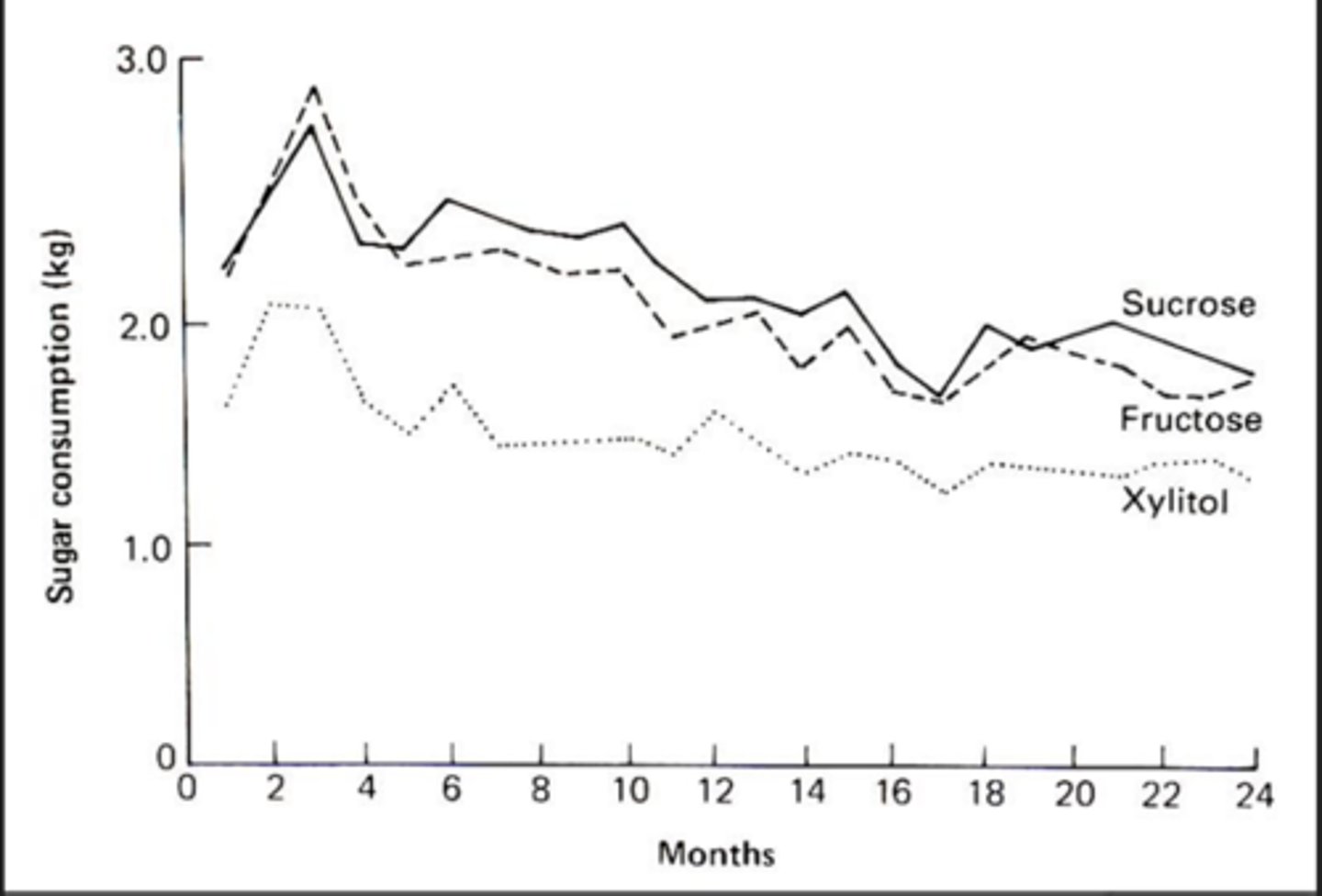
STUDY
Turku, Finland
Objective
To determine the effect of total substitution of fructose or xylitol for sucrose on dental caries
Design:
- Volunteer, adult subjects
- Secondary gum trial
Image depicts sugar intake according to diet over a two year period
at the beginning every ate a lot
Takeaway:
Sucrose/fructose higher than xylitol because xylitol tastes not as good and Gi tolerance is not as good
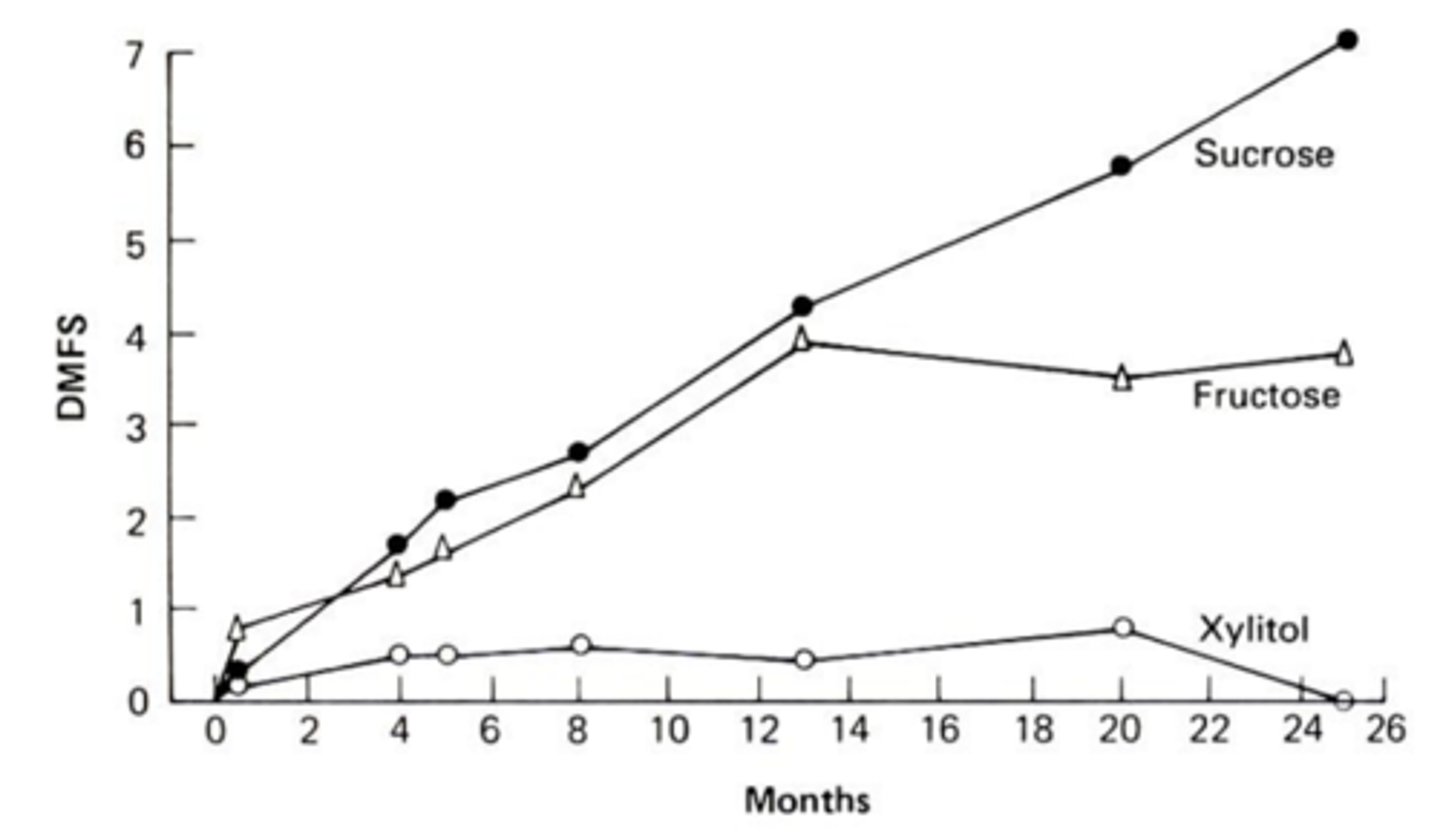
Takeaway
Turku Finland DMFT
Those who received the sucrose and fructose diets had much higher DMFS scores than those on xylitol
Technically there is no difference between sucrose and fructose
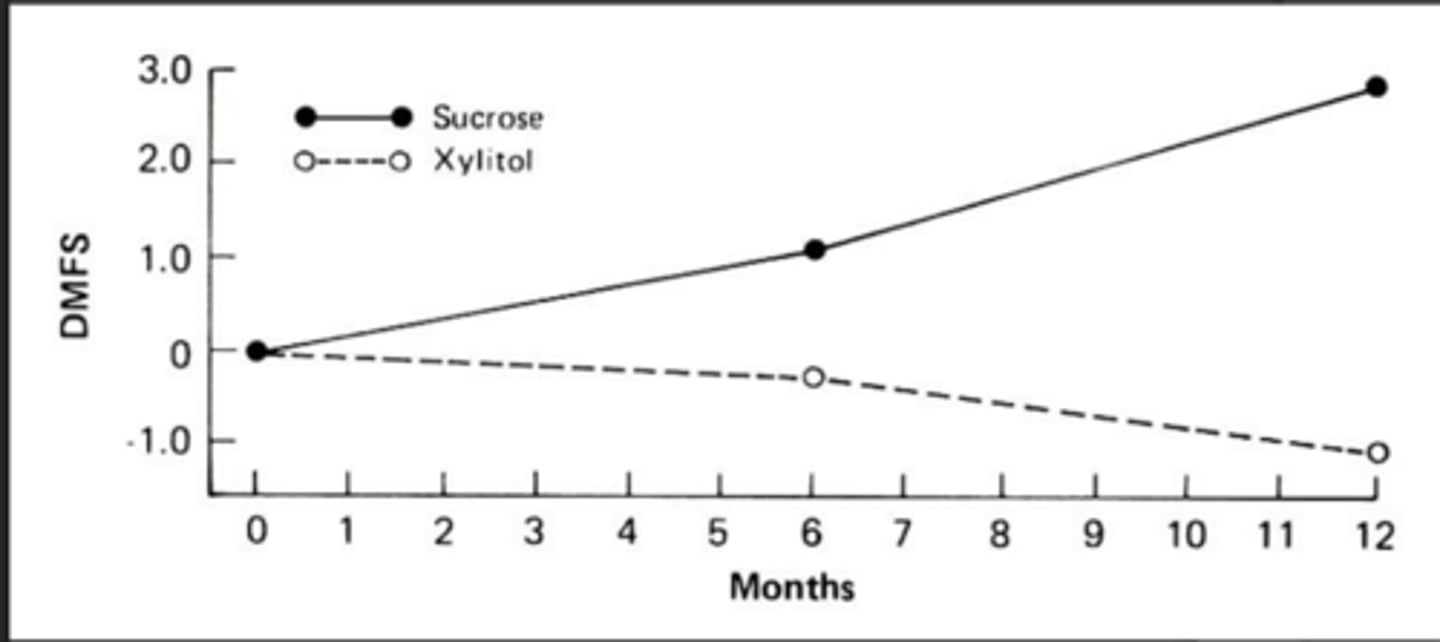
Turku gum trial
- Because Xylitol had less caries wanted to see if it was protective
Design:
- Chewing four sticks of gum per day
- Either sucrose or xylitol gum
Sucrose: Definitely see increase in caries
Xylitol: See a slight decrease in caries (is it due to remin??? we don't know yet)
CLINICAL STUDIES SUMMARY: Sugar consumption with meals is associated with
a slight increase in caries
CLINICAL STUDIES SUMMARY: sugar consumption with and between meals is associated with a
substantial increase in caries
CLINICAL STUDIES SUMMARY: Individual variability in caries susceptibility
exists
CLINICAL STUDIES SUMMARY: Increased caries incidence disappears with
sugar removal
CLINICAL STUDIES SUMMARY: caries do occur
without sugar
CLINICAL STUDIES SUMMARY: substitution of sucrose by sugar alcohols is associated with
reduced caries incidence
CLINICAL STUDIES SUMMARY: Substitution of sucrose by other sugars
does not reduce caries
Animal studies
Also an experimental study but uses animals instead of humans
Advantages:
- More invasive
- Shorter lifespans
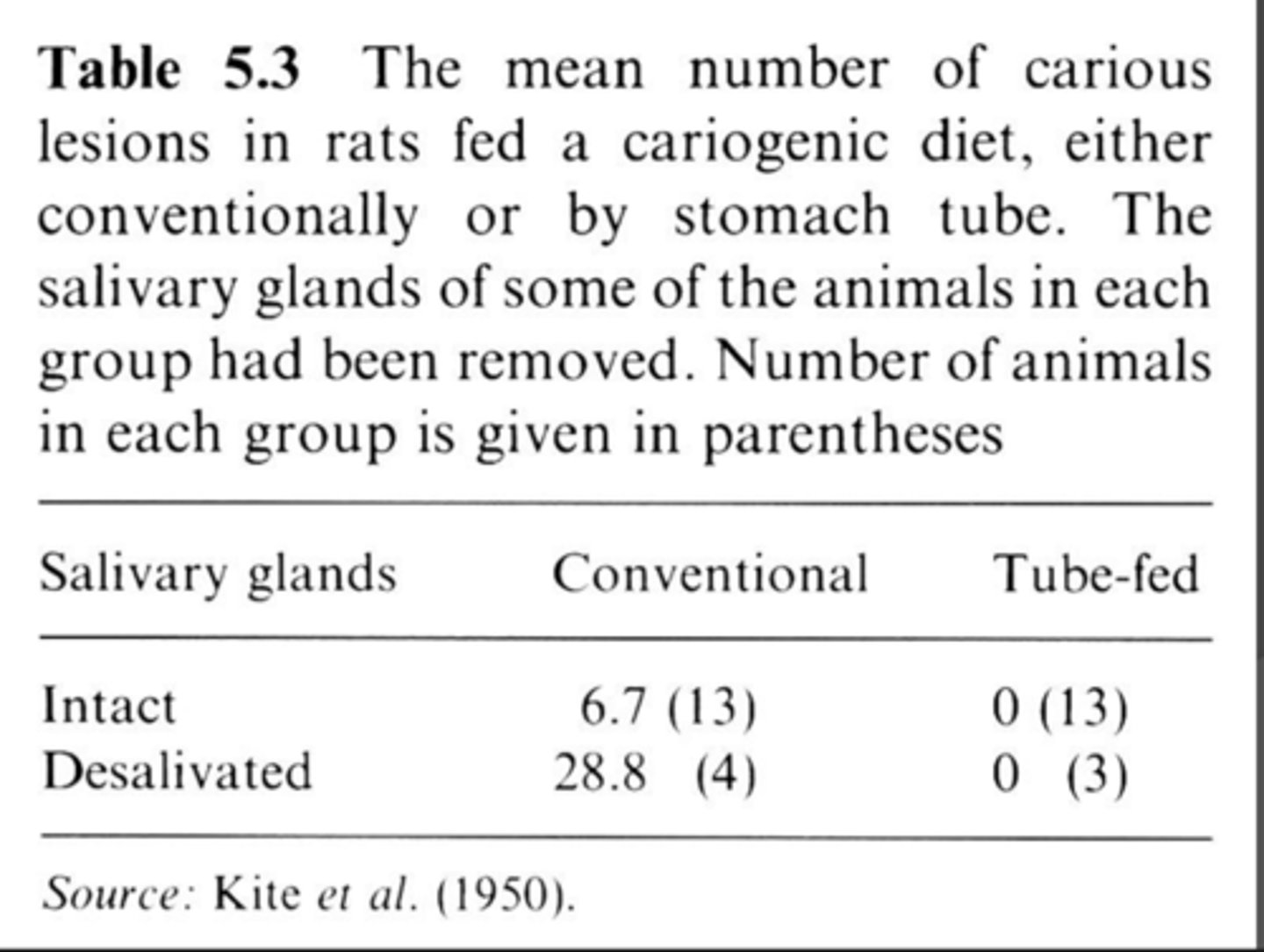
STUDY:
Research questions:
1) Is exposure of the teeth/plaque to the substrate required for caries formation
- Local vs systemic
2) Does the presence or absence of saliva impact the process
Design:
- Cariogenic diet by mouth or GI tube
- Removed salivary glands
Points to note:
- Tube feeding = 0 caries (localized effect not systemic)
- Decreased saliva = increase severity of caries (saliva is protective)
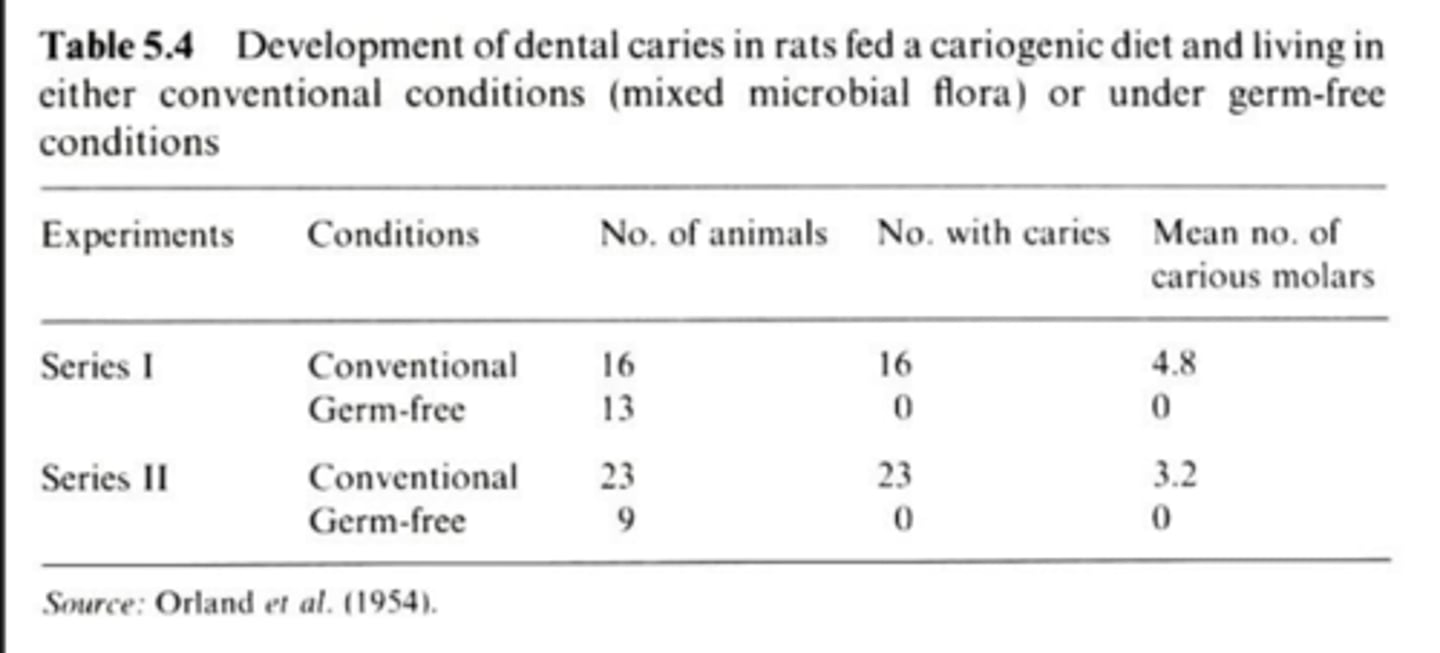
STUDY
Research question:
- Can you produce caries in a germ-free environment
Design
- Cariogenic diet with no bacteria in the system
- Normal rats
- Germ free rats
- Compare the rats
Take home:
- No bacteria = no caries
- Have to have cariogenic bacteria for caries
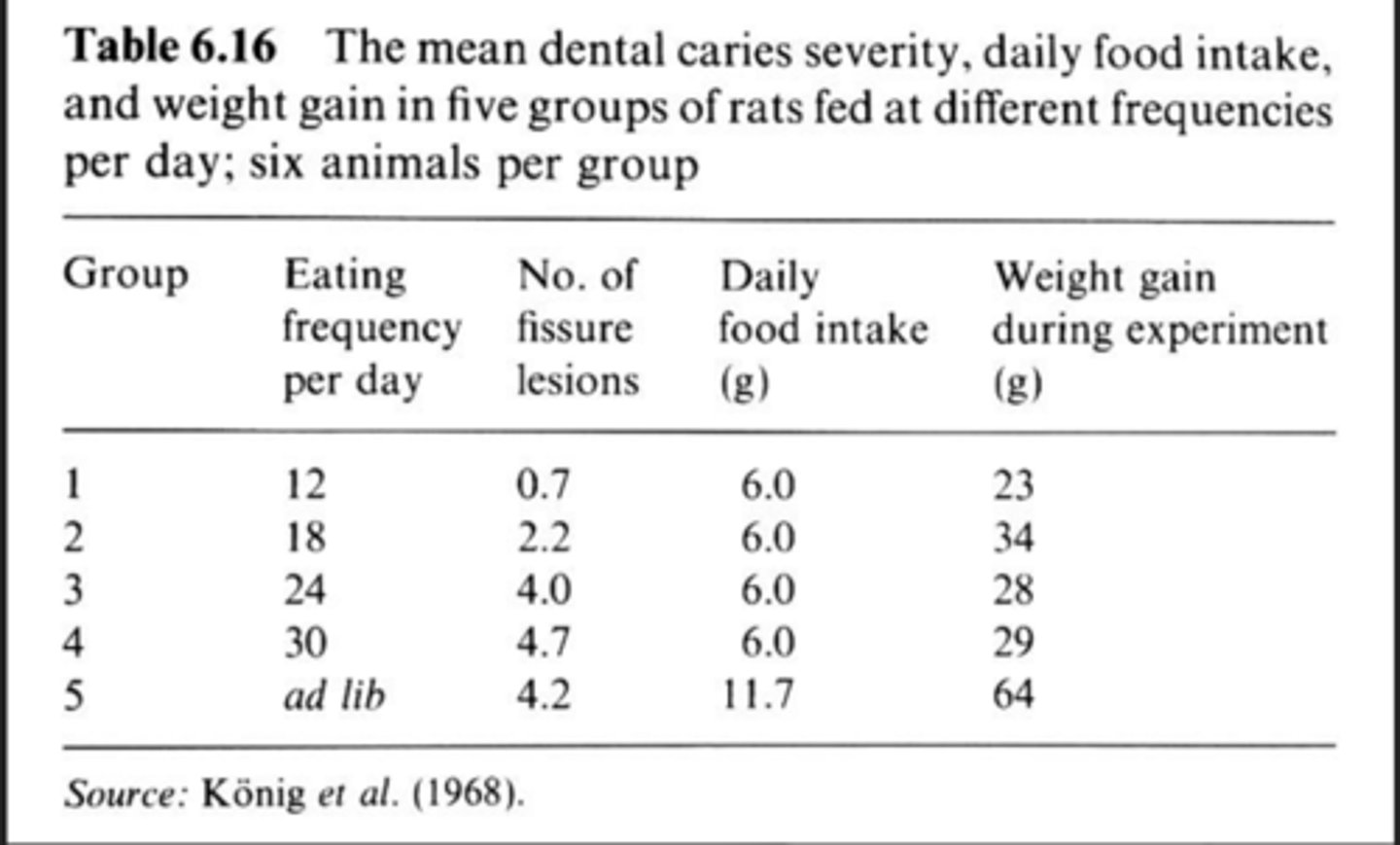
STUDY
Research question:
- How does the frequency (number of exposures) of feeding and the volume of intake affect caries development?
Design:
- Fed rats ad lib or at set volumes at specific time of the day
- Restrict the intake the rats they will eat it all at once
- If you feed plenty theyll nibble throughout the day
Takeaway:
- Same amount consumed but increasing frequency of exposure = increased caries
- Saturated effect at 24 exposures
STUDY
Research question:
- Is the concentration of sugar associated with caries formation
Design:
- Provided diets with different sugar concentrations in the presence of bacteria
Circle = smooth surface caries
Squares = pit and fissure
^^^ not important^^^
Takeaway:
- Increase the concentration of sugar = increase in caries for both types of lesions.

ANIMAL STUDIES SUMMARY: Effects of dietary sugar are
local, not systemic
ANIMAL STUDIES SUMMARY: Feeding frequency is _______ associated with caries incidence
positively
ANIMAL STUDIES SUMMARY: Sugar concentration is __________ associated with caries incidence
positively
ANIMAL STUDIES SUMMARY: All sugars are
highly cariogenic
Enamel slab experiments (also called in situ)
- Not quite clinical studies and allow more flexibility from an ethical perspective
- Individuals wear appliances containing enamel from extracted teeth in their mouths (or other test material)
- The enamel is then exposed to experimental conditions
PROS and CONS of Enamel slab experiments
Pro:
- mimics life
- intra oral environment
- ethics
- Not damaging real teeth
Cons:
- Not quite in vivo
ENAMEL SLAB EXPERIEMENTS SUMMARY: Fermentable sugars cause:
Non-fermentable sugars
Fermentable sugars cause demineralization
Non-fermentable sugars aid remineralization
ENAMEL SLAB EXPERIEMENTS SUMMARY: Sugar concentrations and exposure frequency increase
demineralization
Plaque pH Studies
Experimental clinical study
Micro electrodes are placed in the mouth at the tooth surface and pH changes are measured in response to a challenge (food, meal, nutrients)
Stephan Curve
*Important for exam*
Plot of the pH of plaque vs time
1. Fall of pH representing speed of sugar metabolism (acid production)
2. Rise in pH represents removal of acids
- Salivary clearance
- Saliva buffering
- Acid leaching from plaque
3. pH then returns to normal
4. 5.5 (dotted line) is the critical pH where demineralization begins
- there is individual variance as to exact pH where things change

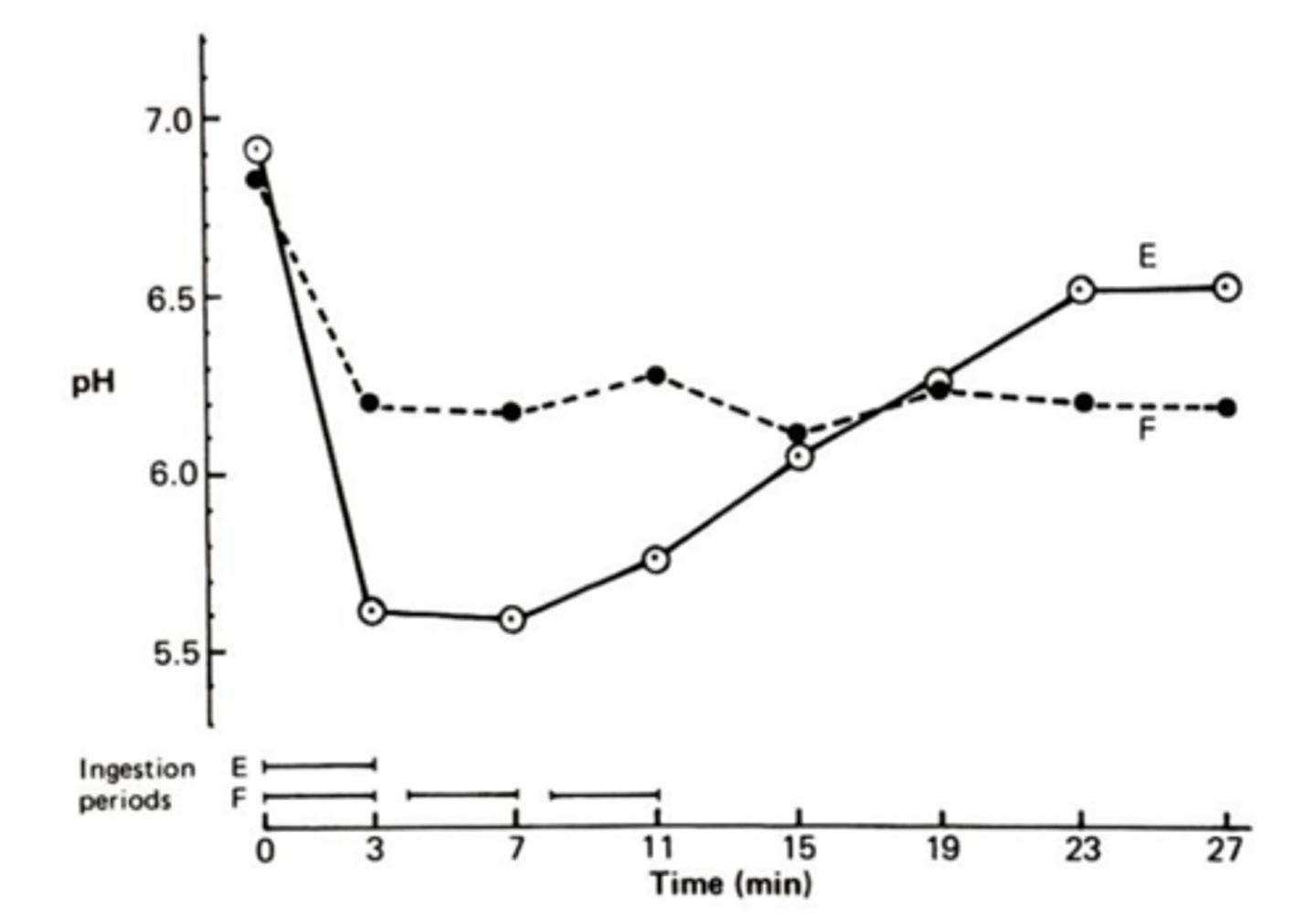
How food impacts pH:
E = sugared coffee alone
F = Sugared coffee and 2 nonacidogenic foods (eggs and non crisp bread)
Takaway:
- The drop was blunted when nonacidogenic food was consumed with the acidic coffee
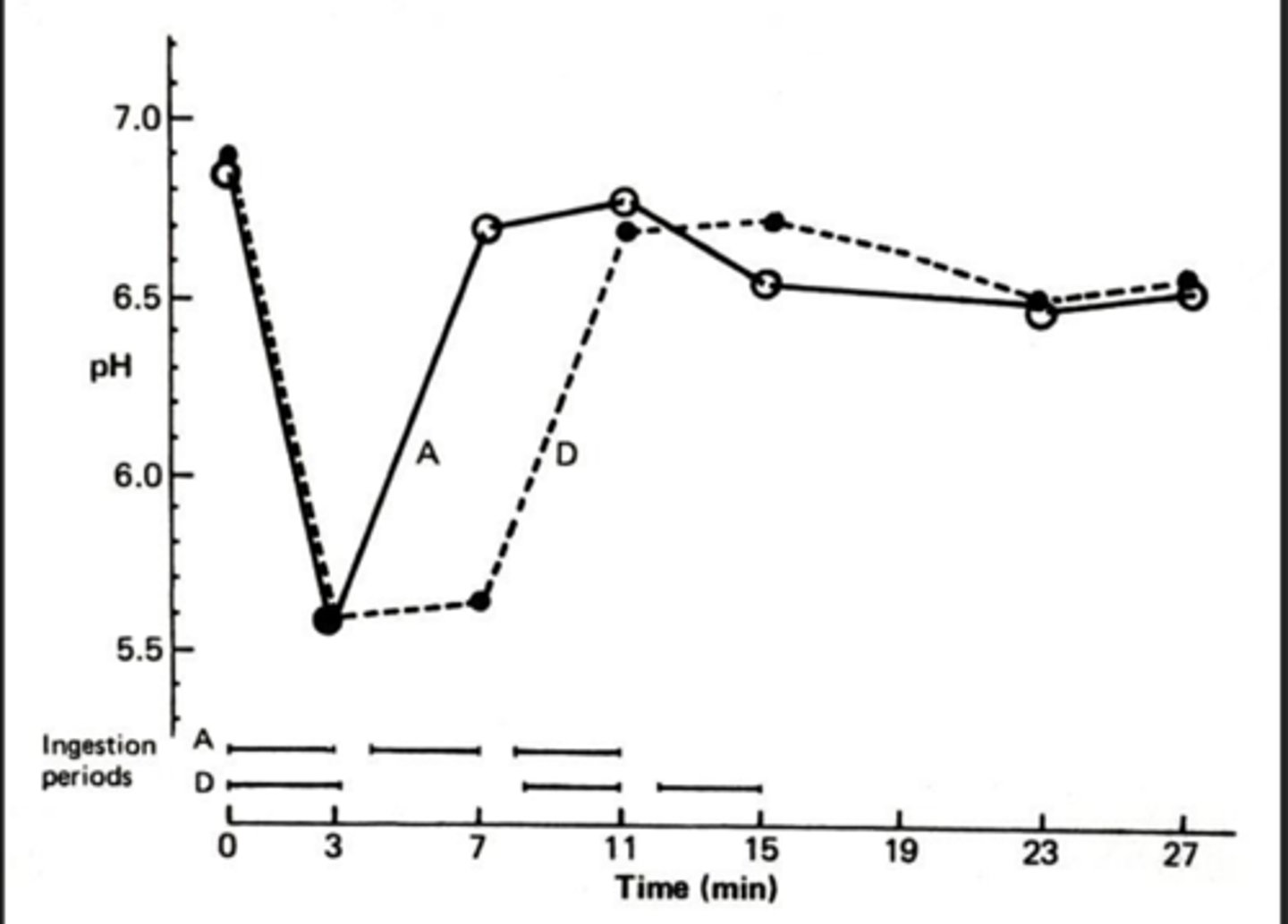
How food impacts pH-
A = Sugared Coffee immediately followed by egg and toast
D= Sugared coffee with egg and toast after 5 minute wait
Takeaway:
- Delay in solid food delays pH rise
- How one eats impacts acid production and length of time below the curve
PLAQUE pH STUDIES SUMMARY: The acidogenicity, not _____, of various foods, drinks and meal patterns has been determined
cariogenicity
PLAQUE pH STUDIES SUMMARY The critical pH is
5.0-5.5
Incubation studies
- In vitro
- Experimental
- Assess the ability of microorganisms to ferment food (produce acid)
- Test food incubated with plaque/saliva in test tube
- Results consistent with other science
INCUBATION STUDIES SUMMARY: All fermentable sugars can be fermented by
plaque microorganisms
FOOD AND CARIES
FOOD AND CARIES
Fat, protein, non-nutritive sweeteners are not
substrates for bacteria -- will not result in acid production and thus no caries risk
STUDY
Palmer: Diet and ECC
Subjects:
2-6 year old, healthy children, Boston Area
- Caries free
- Severe early childhood caries
Exposure:
24 hour recall: meal patterns, food intake
Outcome:
Caries
Design:
Foods grouped by composition:
- protective (nuts cheese xylitol)
- non-cariogenic (protein and fats)
- Low cariogenicity (starches, fruits, vegies, milk)
- Liquids (sugared beverages)
- Solid/ retentive (bread, chips, cereal, cookies)
Estimated cariogenicity scores/foods and beverages
Takaway:
1. Kids with ECC had more
- Sugared liquids
- Solid/retentive foods - highly processed
2. Total number foods higher in kids with ECC
3. More frequent exposure
Sugared beverages and your processed snacks increase your risk for caries

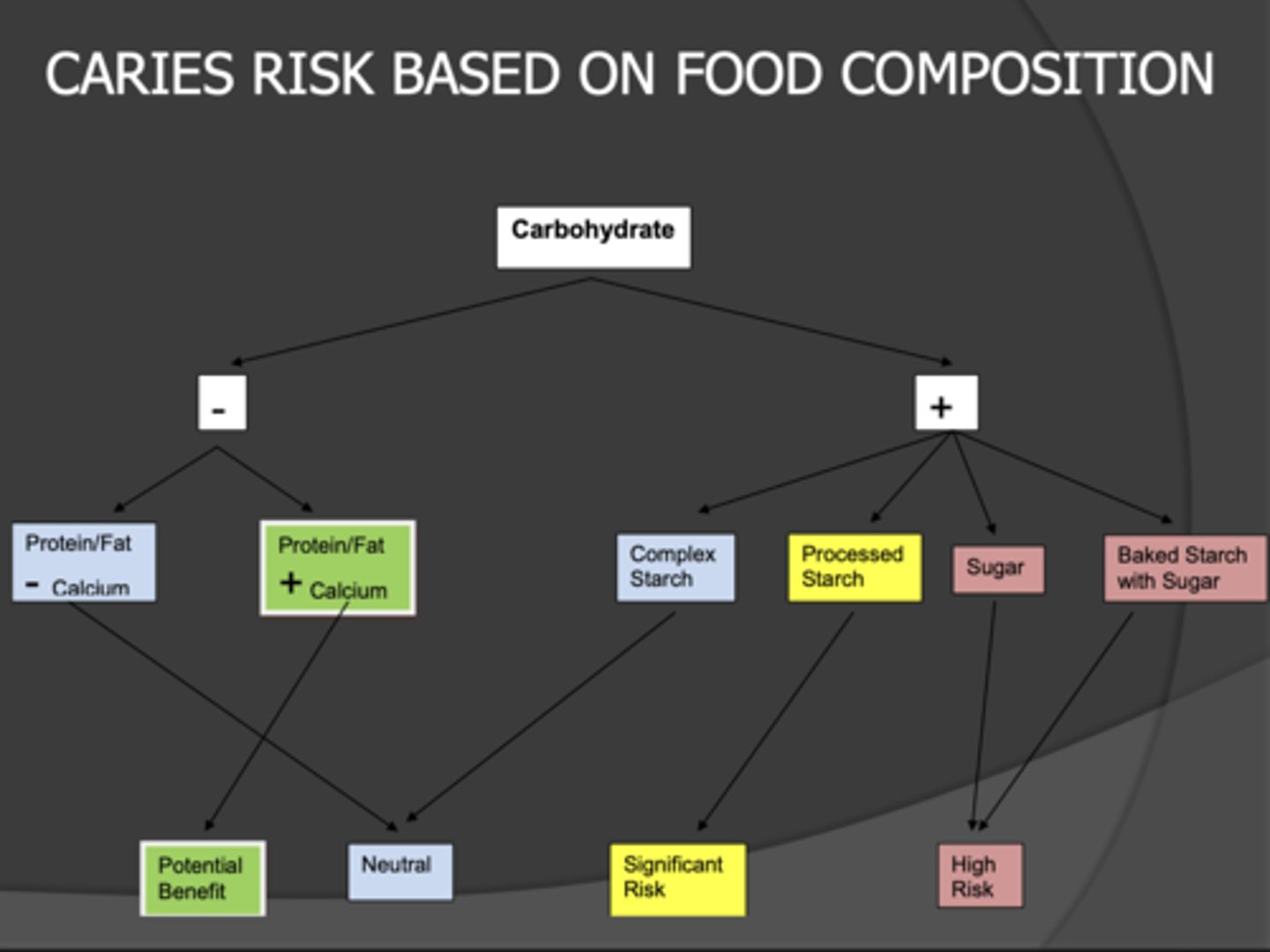
CARIES RISK BASED ON FOOD COMPOSITION SUMMARY
If a food has Carbohydrates:
But also has Protein/ fat:
- Worst case is it will be neutral
- If calcium = protective
But also has Starch:
- Complex = Neutral
- Processed = significant risk
But also has sugar:
- High risk
Risk is associated with susceptibility but note eating habits (frequency) increase risk
Food sugars
- Mono/Disaccharides
Fructose
Glucose
Sucrose
Lactose
Maltose
Starches
-Polysaccharides
Raw, Cooked (fine)
vs
Baked with sugars (bad)
Processed starches
- Not quite sugars (oligosaccharides):
Dextrins
HFCS
Maltodextrin
Modified starches
Natural/ Food sugars
Honey
Raw sugar
In respect to natural sugars bacteria
could not care where the sugar came from
STUDY: Starch intake and caries
Design:
- Longitudinal (11 year follow-up)
- Had a huge distribution of starch intake per day so were able to look at a big difference
Subjects:
- Finish adults (30-88)
Exposure:
- Starch
- Starch-rich foods (potatoes, tubers, pasta, etc)
Outcome:
- DMFT score
Takeaway:
Weather they looked at the starch (g/day) or the percent energy they found that:
Starch is not associated with dental caries (this is your unprocessed starch products)

Caries risk by food group

Basically the more bioavailable the CHO
the more cariogenic
4 factors that impact the bioavailability
+- CHO
+- protein/fat
Level of processing
Sugar concentration
Risk ratio when having a higher intake of ultra processed foods
71% increase risk of caries
Clearance time impacts
Oral motor skills
- Individual coordination
Food's physical properties
- Retentive/sticky
- Liquid
- Readily dissolved
Resting salivary rate
Induced salivary rate
Self Cleansing foods
Foods that clean the teeth (apples/celery/carrots)
- Plaque accumulation: fibrous foods do help prevent accumulation. Tend to see increase in plaque on soft/liquid diets
- Salivary flow: decrease plaque accumulation
- Mastication demands: decrease plaque accumulation
Do self cleansing foods remove plaque
No sir: you have to brush your silly little teeth to remove plaque
Buffering agents
Saliva (need adequate nutrients to produce healthy saliva)
- anything chewy will stimulate saliva
Peanuts and cheese: High fat and cheese has Calcium
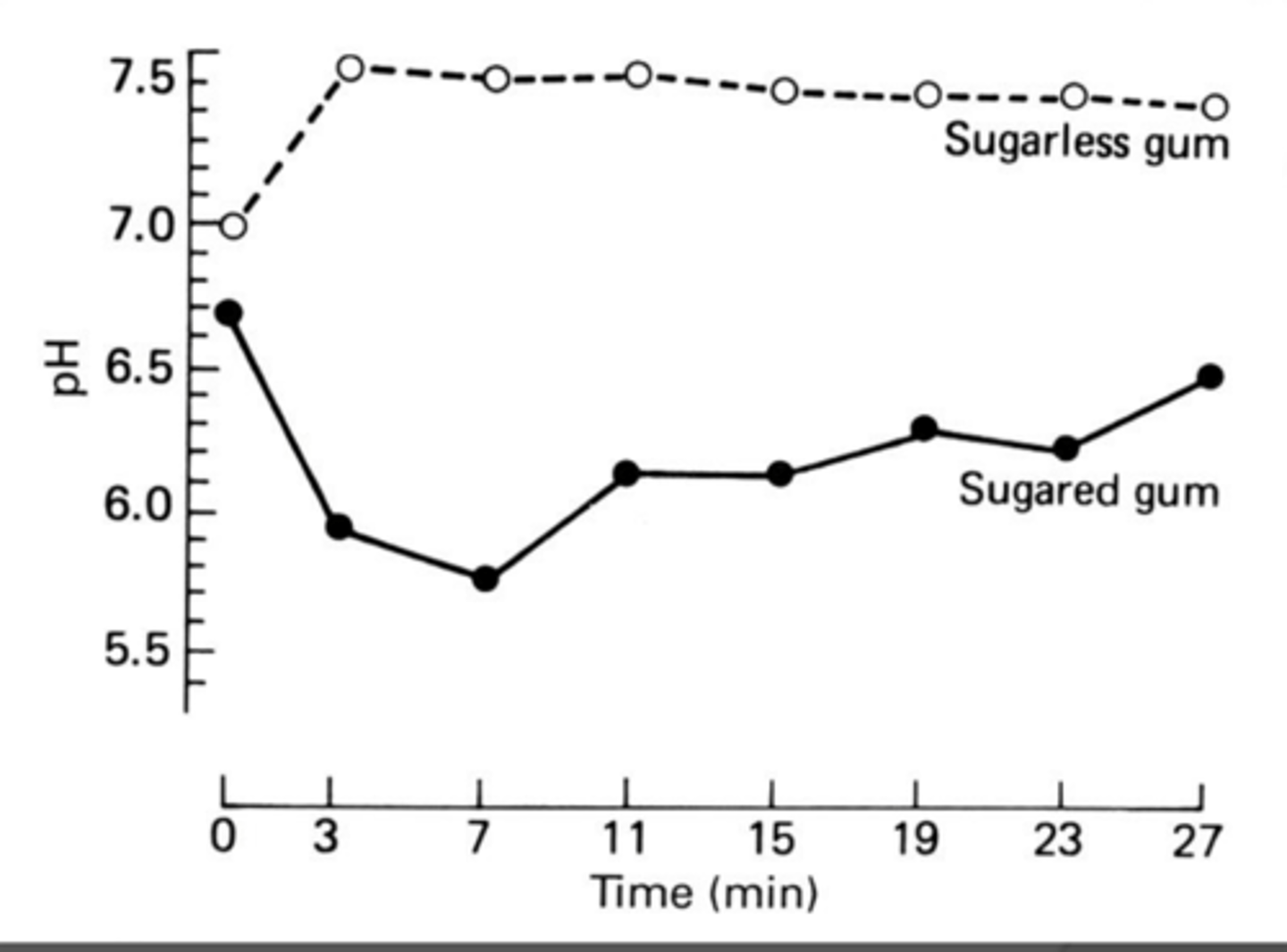
Sugarless gum vs Sugared gum
- Increase pH with sugarless gum
- Fairly blunted fall with sugared gum
Takeaway:
- the chewing isn't really helping if you are constantly reapplying the sugar gum
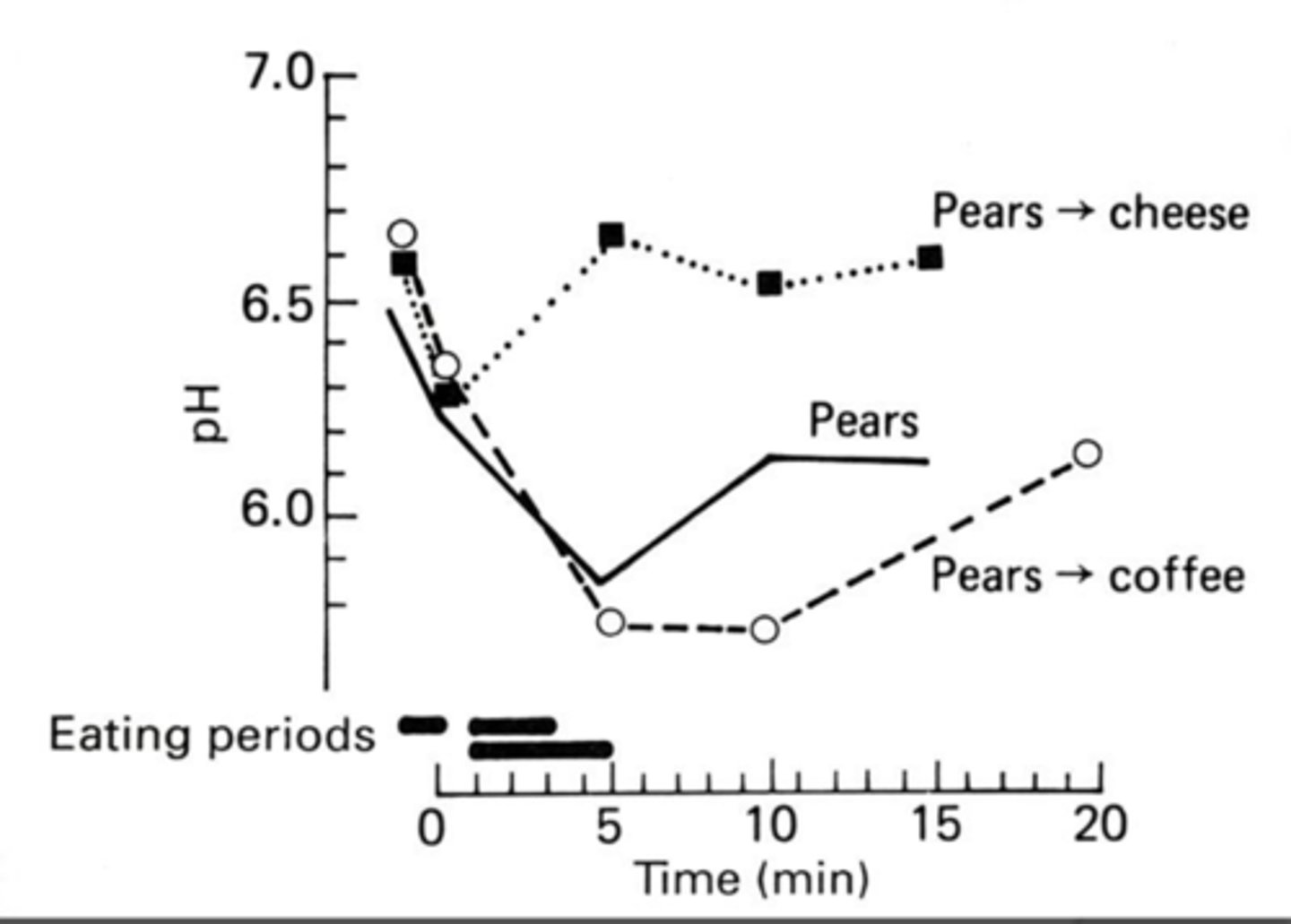
Sequence of Foods
How we eat are food is important
Pears= control
- eat pears pH falls then returns to normal
If we follow a pear with sugared coffee the pH stays down longer before returning to normal
If we follow a pear with the cheese it won't fall as far because the cheese is protective
Takeaway:
- Combination of foods modify the cariogenicity of the pear
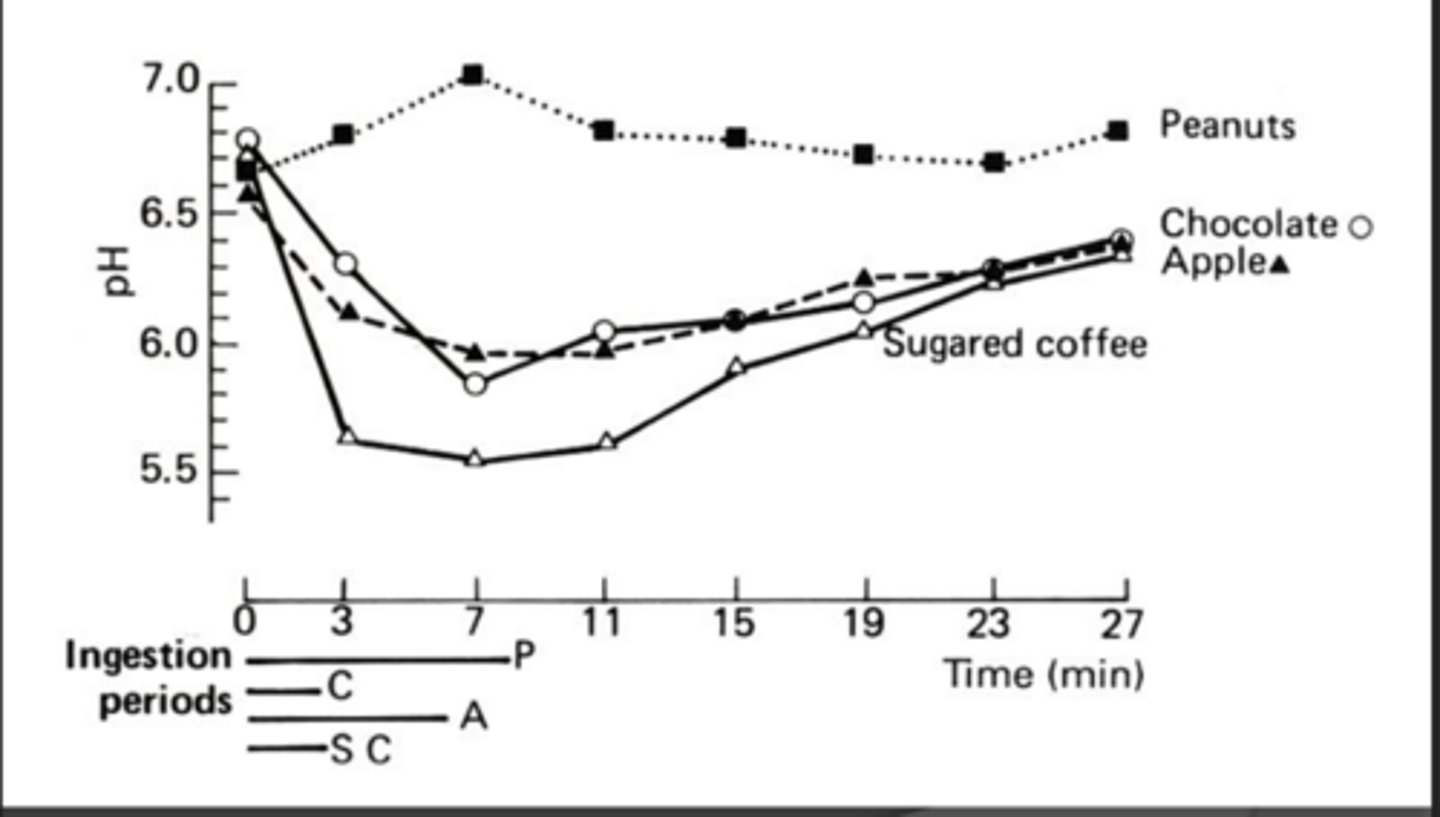
Composition of foods
Peanuts - no substrate
Chocolate- substrate and fat
Apple- substrate + chewing/friction
Coffee- only substrate
Mixed diets are thought to be protective against caries
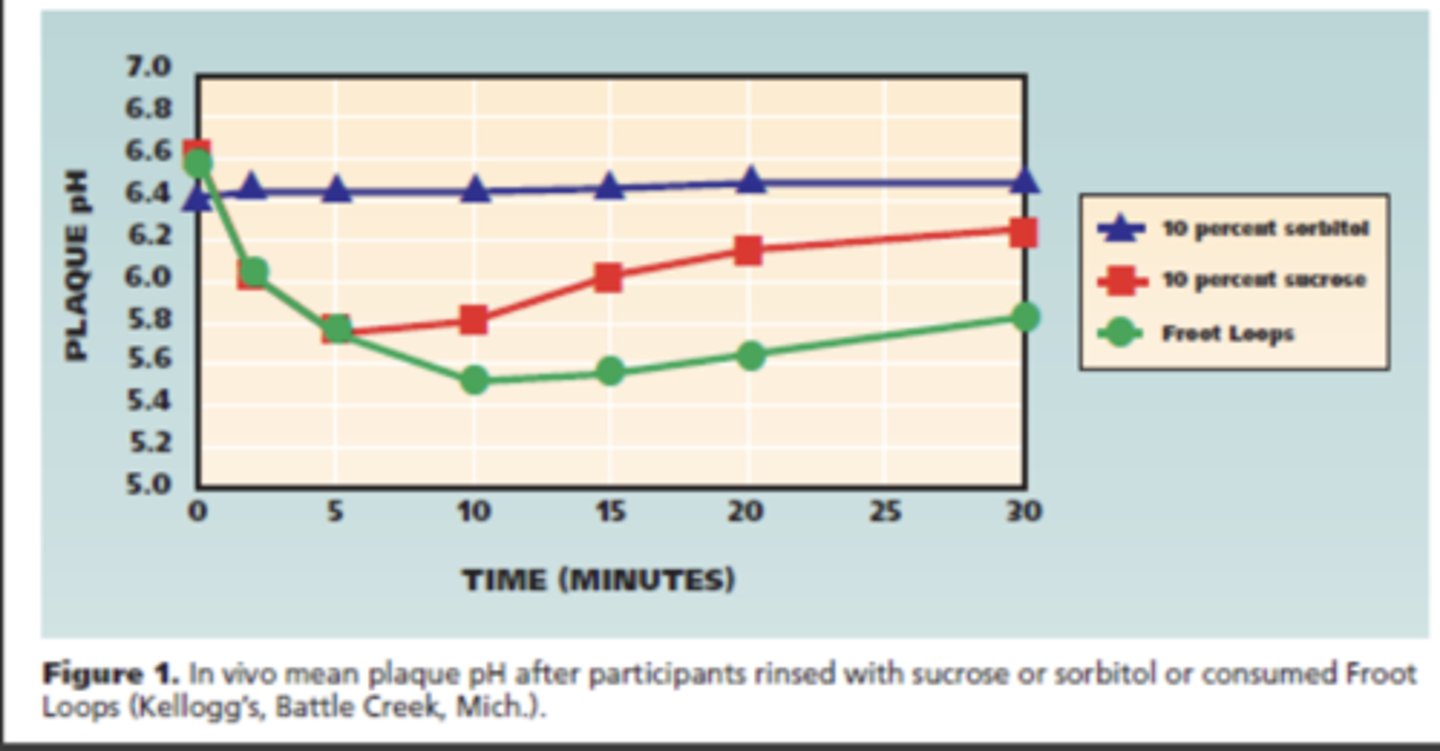
STUDY: Sugared snacks followed by beverages
Objective:
Identify if plaque acidogenicity differed in response to different beverages after a sugary snack
Methods:
Clinical trial with 20 healthy adults
Design: Intervention #1
-- Fruit loops
-- 10% sucrose rinse
-- 10% sorbitol rinse
Outcome
- Plaque pH
Results:
Sorbitol: No impact on plaque pH
Sucrose: Fell but since it was just sucrose it was cleared relatively quickly
Fruit loops: with the starch still hanging out on the teeth and stayed longer
Design: Intervention #2
- Fruit loops
-- Whole milk
-- 100% apple juice
-- Tap water
Outcome
- Plaque pH
Results:
Water: pH increased a little after milk
Milk: pH increased faster (returned to normal quicker when you have the fat and calcium in milk)
Apple juice: pH stayed lower for longer (due to additional substrate)

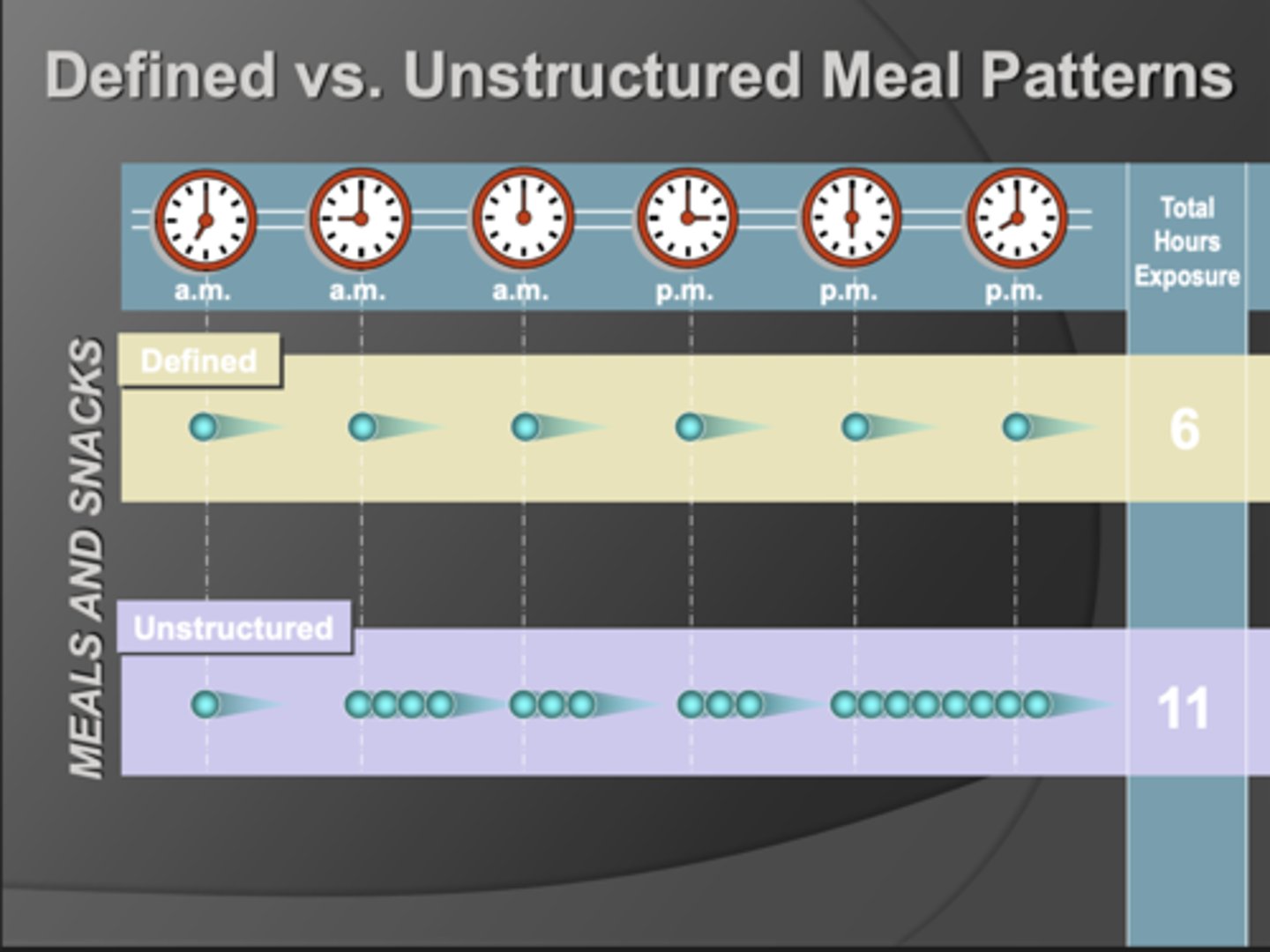
Meal Patterns
The length and frequency of eating behavior results in more time in the demin vs the remin
Takeaway:
- Grazing/ snacking is bad and can increase caries
Non-nutritive sweeteners
No nutrients from them
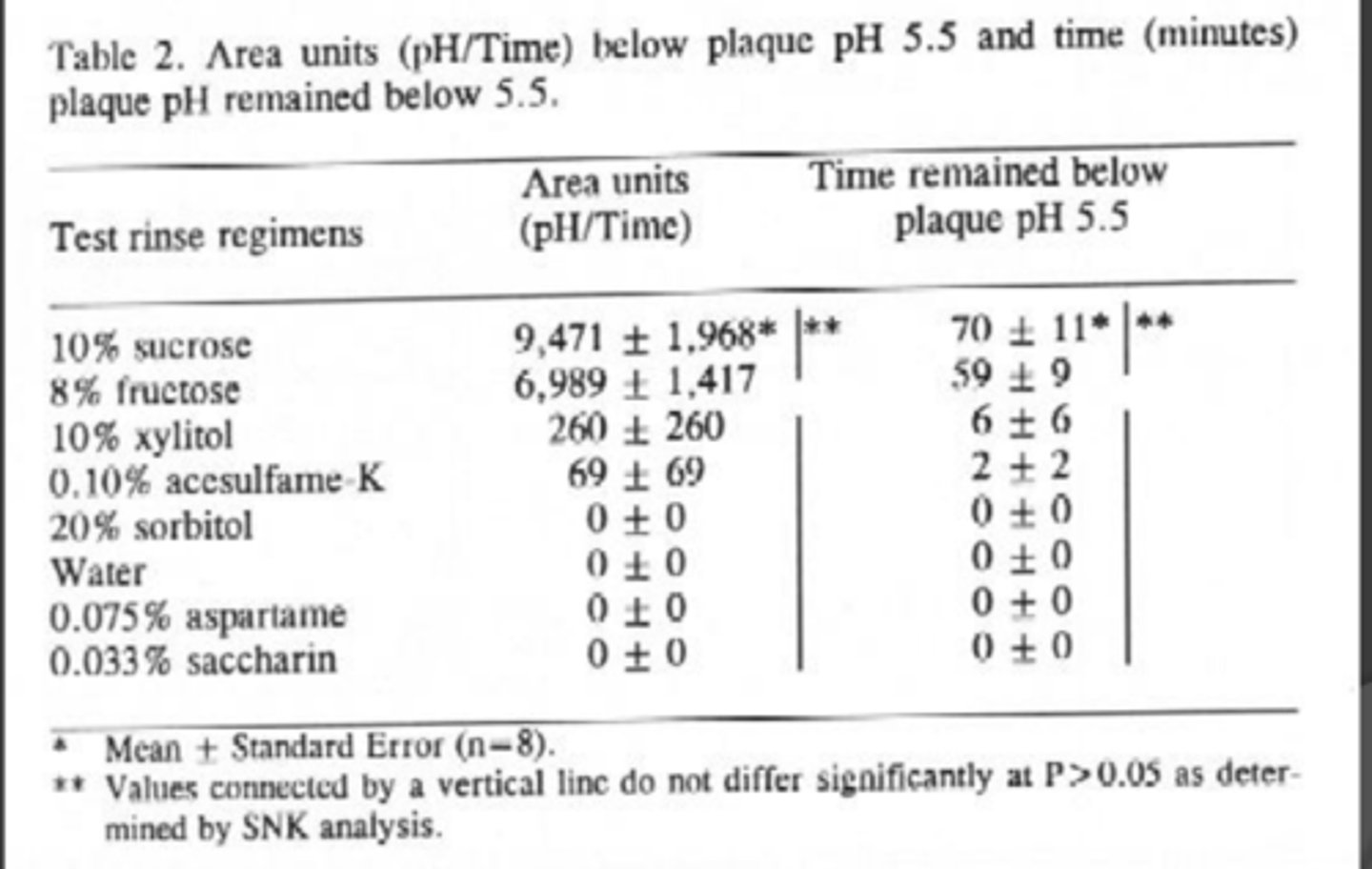
STUDY: Sweeteners and acidogenicity
Objective:
In adults, compare change in interdental plaque pH after rinsing with:
Sugars
- sucrose
--fructose
Polyols
- Sorbitol
- Xylitol
High intensity sweeteners
- Aspartame
- Saccharin
- Acesulfame K
Takeaway:
Sugars spent a lot of time under the pH curve and increased demineralization
Sugar alcohols and sweeteners virtually no time in demineralization
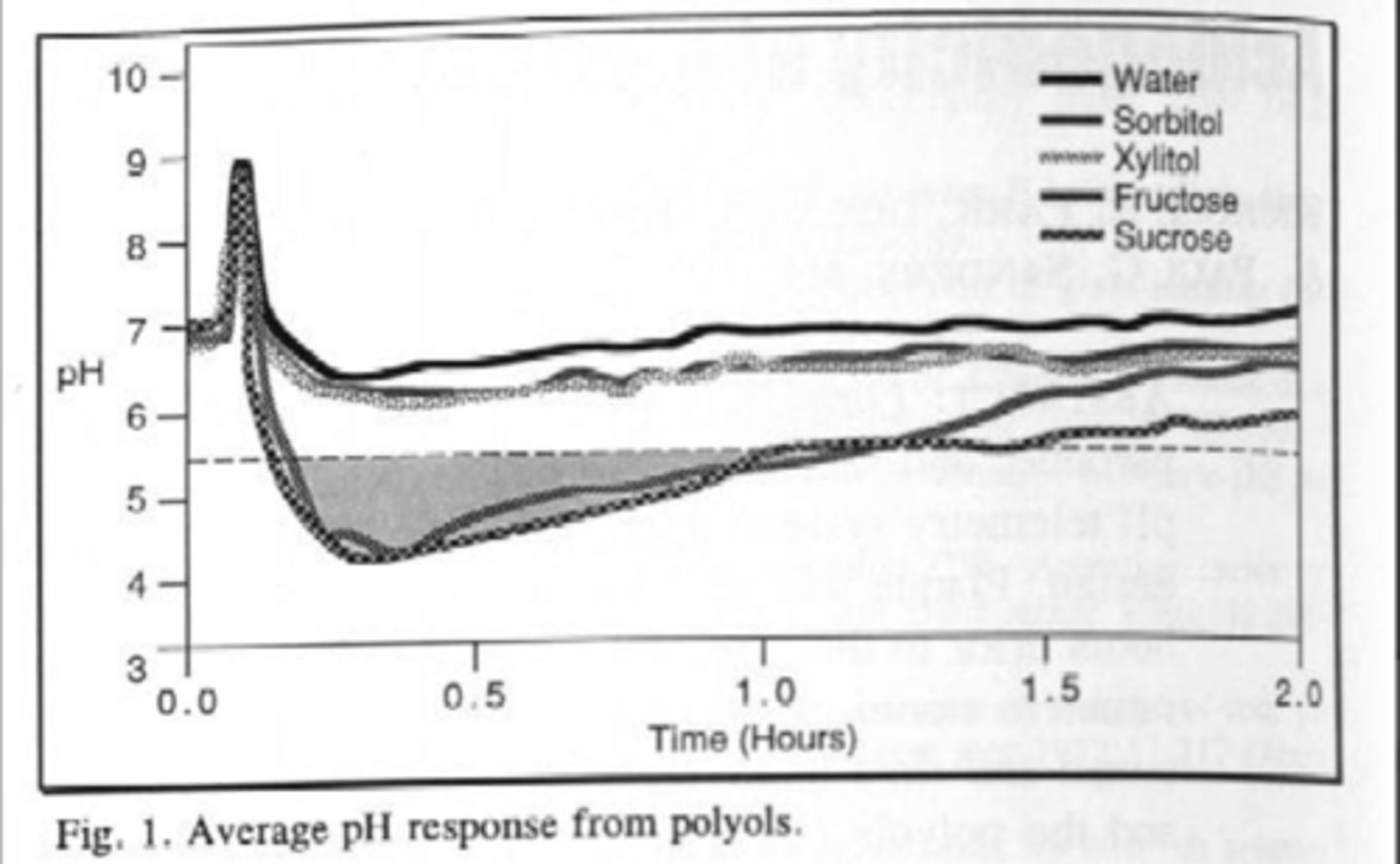
pH response from Sugar Alcohols (polyols)
Xylitol and Sorbitol pH didn't fall so they are not cariogenic
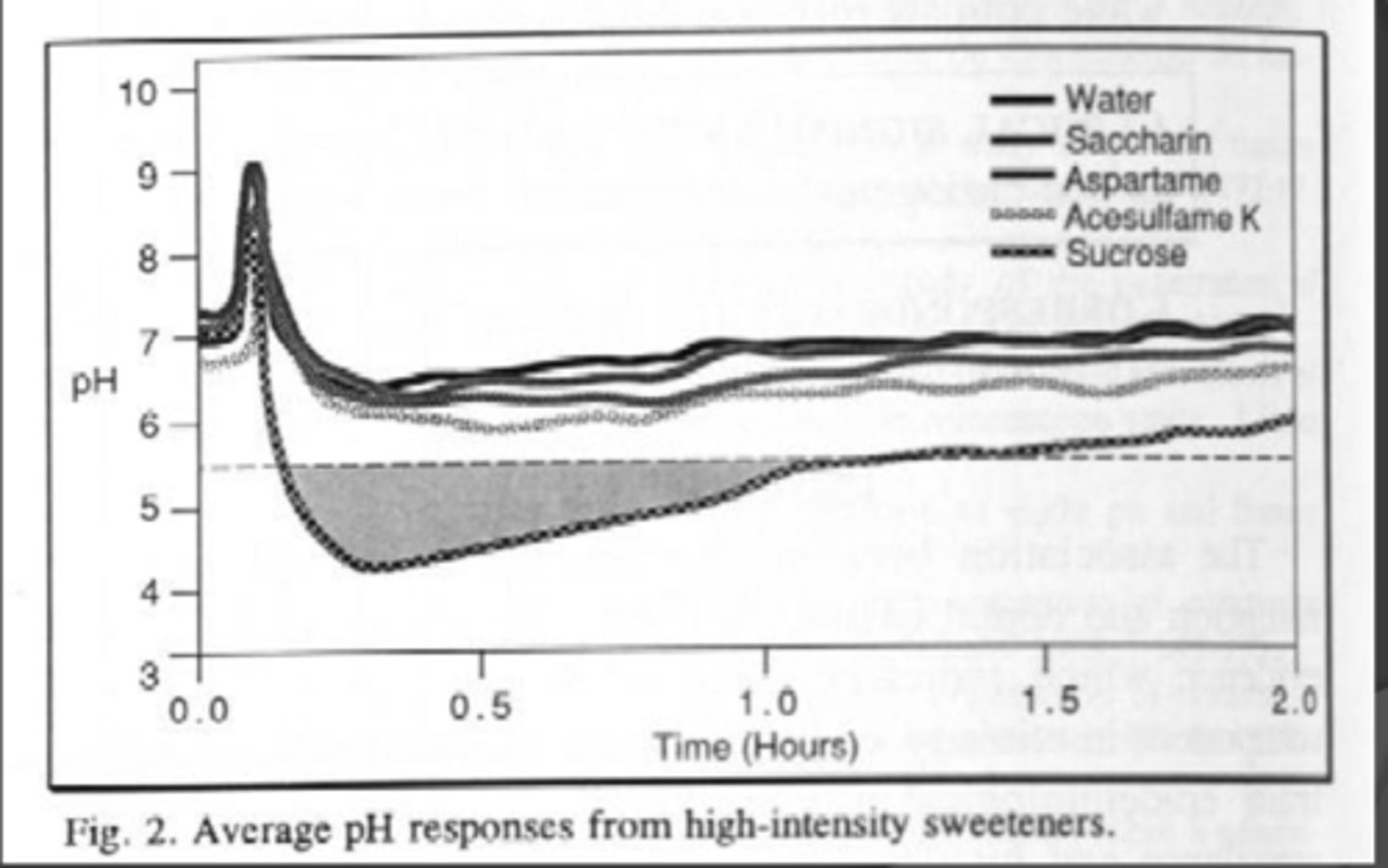
pH response from high-intensity Sweeteners
Aspartame, Acesulfame K, and saccharin also had no cariogenicity
SUMMARY: Sugar alcohols are not
Acidogenic or Cariogenic
SUMMARY: High-intensity sweeteners are not
Acidogenic or Cariogenic (these are not carbohydrates and thus can't be fermented)
Monk Fruit and Stevia
Monk fruit sweetener
- 0 kcal
- Mogrosides provide sweetness
Stevia
- 0 kcal
- Steviol glycosides
No carbohydrates no kcal = no caries
Both products have Gras approval
Erythritol
- Sugar alcohol
-- 0.2 kcal/g
- Naturally in some fruits, fermented foods
- GI friendly compared to other sugar alcohols
- Bulking agent with stevia, other intense sweeteners
Oral health:
- Not cariogenic
- reduced plaque
Intrinsic sugars
Reside inside cellular structure
- Sugars within fruits, vegetables grains
Extrinsic sugars
Reside outside of cellular structure
- Added sugars
- Processed fruits, Vegetables (juice)
- Milk is outside of cellular structure but though "healthy"
Non-Milk Extrinsic sugars
Term used in Great Britain and the rest of Europe to categorize sugars as healthy
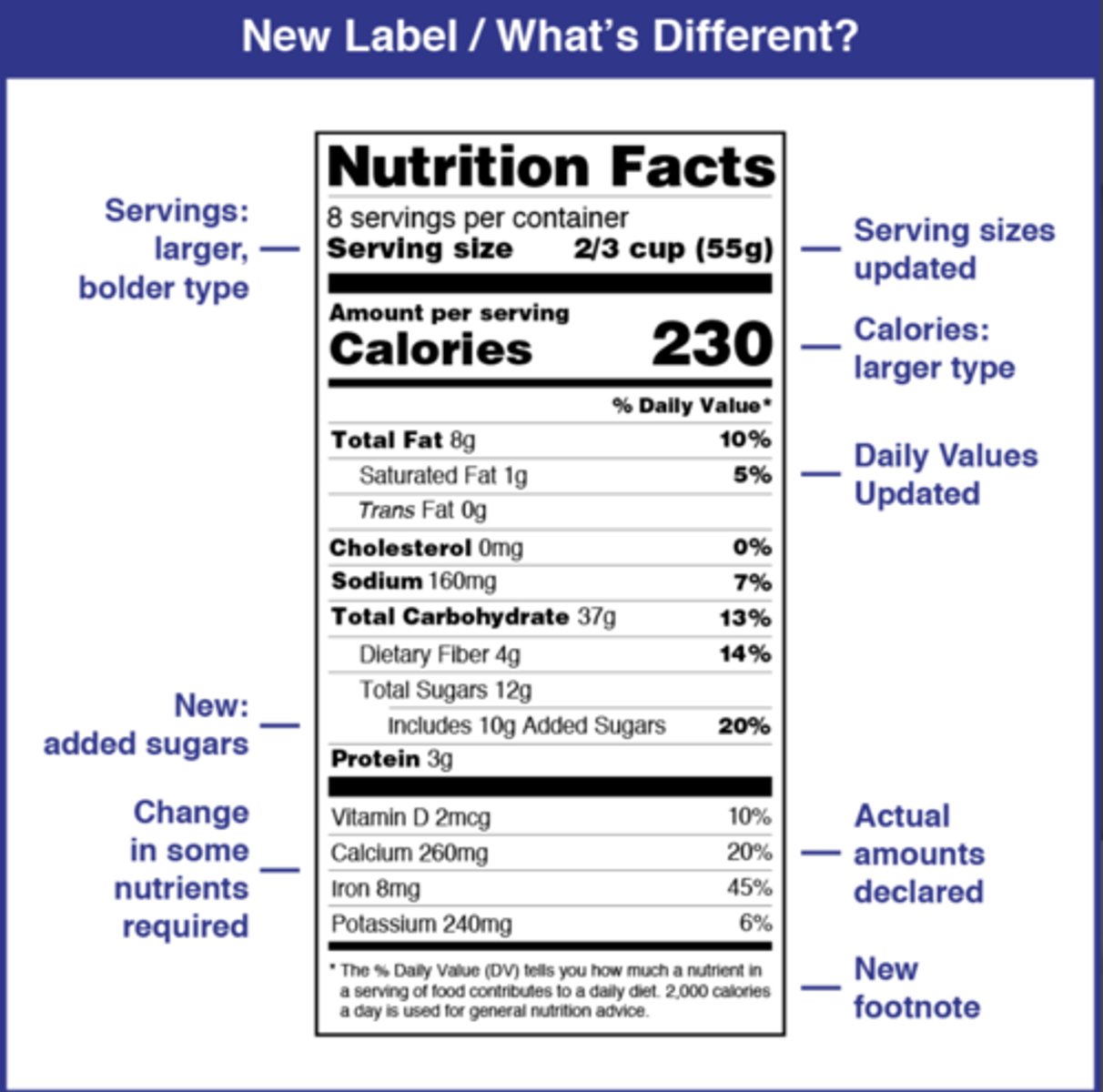
Nutrition labels ingredients are listed
Descending order by weight
Nutrient label evaluations of foods: Cariogenicity, systemic health
ingredients
Relative fat contents
Relative carbohydrate content
Relative sugar content
relative starch
Clearance
Nature of consumption
Food label
Total carbohydrates minus total sugars and dietary fibers = Starch
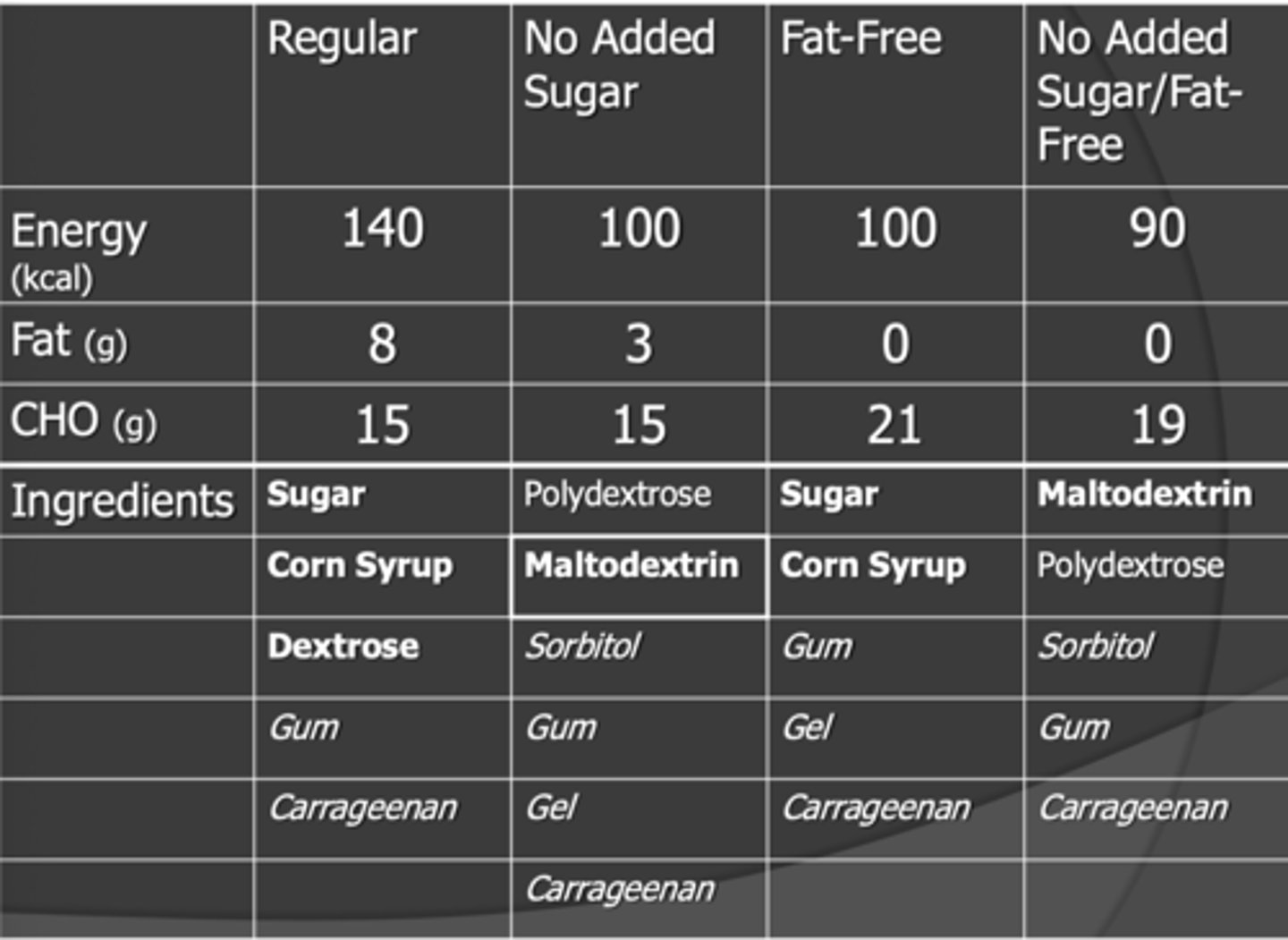
Ice Cream and cariogenicity
Ingredients in bold can be used by bacteria and cause caries
Takeaway:
- we are removing our sugars and replacing them with maltodextrin and polydextrose
Maltodextrin: is one of those highly processed starches with small chains in it. Its not really a sugar but in refining it we decreased the bacterial workload and thus she a cariogenic baddie
If we can digest it and get calories from it we can get cavities
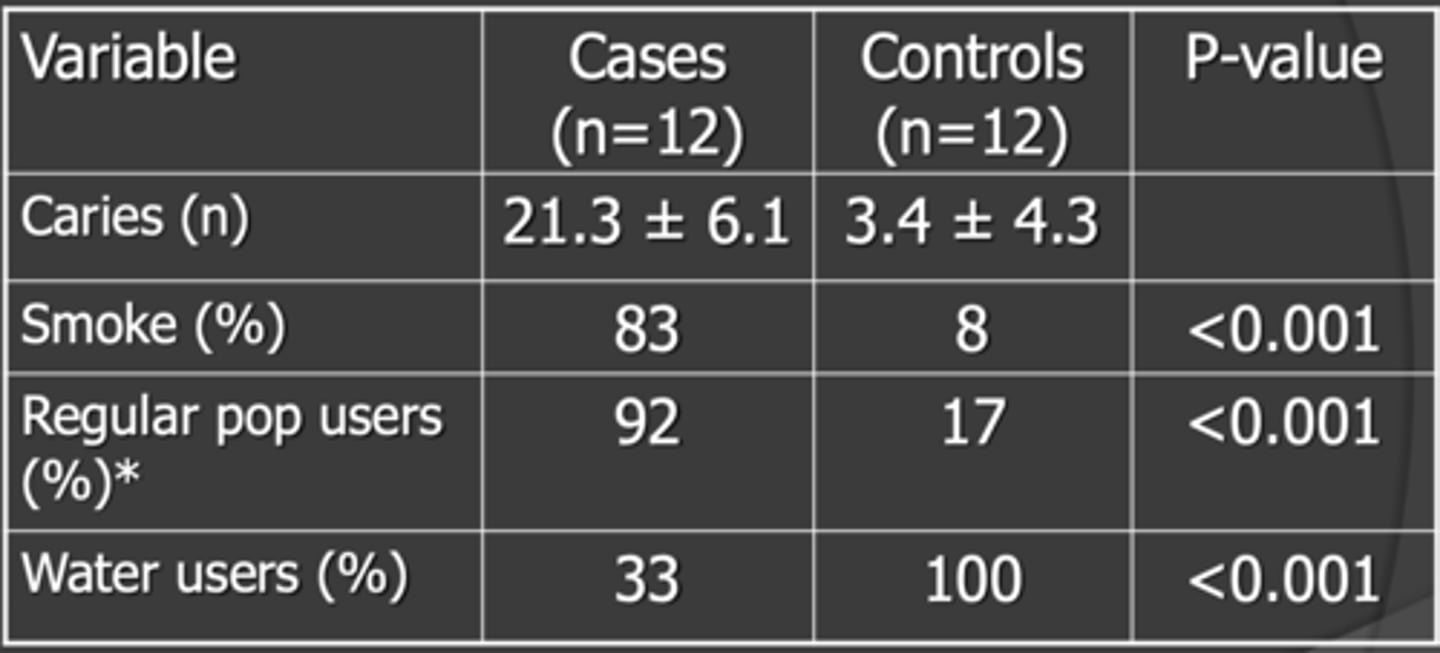
Does soda-pop cause cavities
Takeaway:
Higher pop consumption among those with rampant caries