Looks like no one added any tags here yet for you.
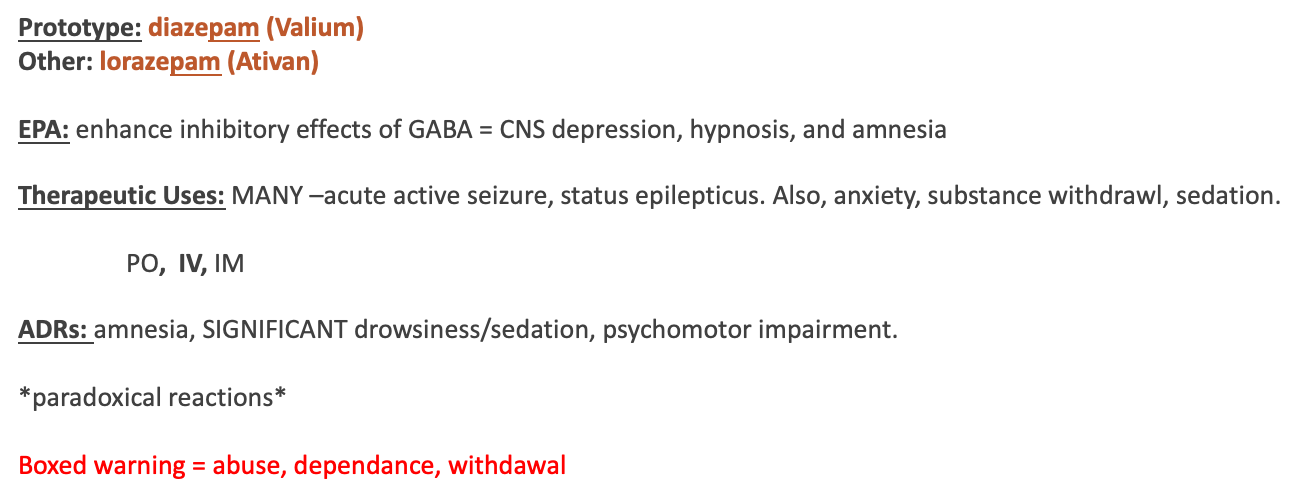
Benzodiazepines
Prototypes: diazepam (Valium) and alprazolam (Xanax)
EPA: Enhance inhibitory effects of gamma- aminobutyric acid (GABA)
Admin: Alprazolam Oral only; Diazepam PO/IV: Admin IV slowly/Monitor IV site
Therapeutic use: Generalized anxiety disorder (GAD) & panic disorder; emergency management seizure disorders
ADRs: CNS/Resp depression, Hypotension, Tolerance and physical dependence (especially with alprazolam)
*Overdose/toxicity: possibly life-threatening sedation, hypotension, respiratory depression, cardiac arrest
Contraindications/Interactions: Pregnancy – teratogenic • Glaucoma • Respiratory and/or CNS depression • Concurrent use of CNS depressants
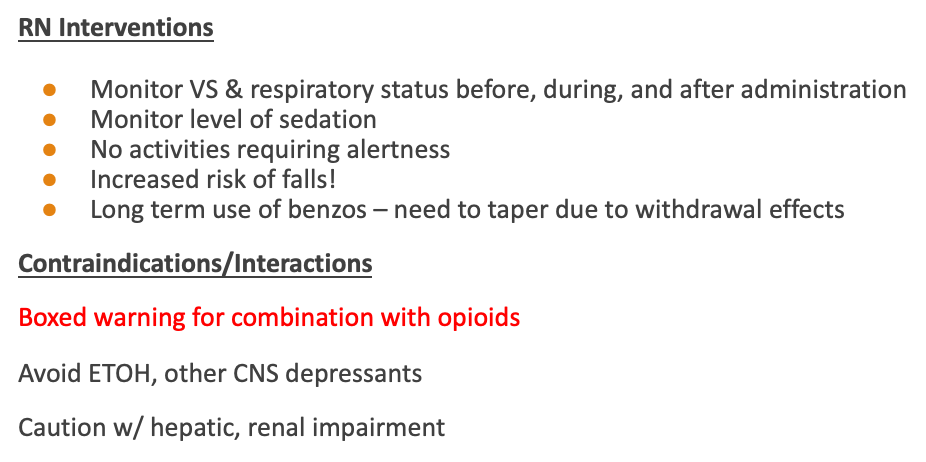
RN intervention/client education: Monitor for withdrawal symptoms: insomnia, anxiety, tremors, diaphoresis, hypertension, seizures • Monitor for phlebitis • Assess/Monitor Falls • Regular Vital Signs • Do not stop abruptly • Assess CNS and Resp depression
Antidote: Flumazenil (Anexate, Romazicon)
Non-benzo/misc. anxiolytic
Prototype: buspirone (BuSpar)
EPA: Binds to serotonin & dopamine receptors; agonistic action on dopamine*
Admin: PO; give 2-4 weeks before tapering Benzodiazepines. Can take 2-4 weeks to take effect
Therapeutic use: Short term treatment of Generalized anxiety disorder (GAD)
ADRs: Paradoxical effects: insomnia, anxiety, restlessness. GENERALLY well tolerated
Contraindications/interactions: MAO inhibitors → (HTN) • Grapefruit juice, Ketoconazole, erythromycin → inc. blood levels • Avoid CNS depressants
RN intervention/client education: Monitor for paradoxical effects • Avoid contraindicated meds/grapefruit juice
TCA
prototype: amitriptyline (Elavil)
EPA: Block norepinephrine reuptake pump & serotonin reuptake pump in synaptic space → boosts availability of serotonin, norepinephrine, acetylcholine, dopamine
Admin: PO at bedtime due to sedative effects. Takes several weeks to take effect
Therapeutic use: Treatment of major depression. 2nd line drug
ADRs: MANY. Anticholinergic effects (dry mouth, dizziness, urinary retention), sedation, inc risk for suicide (child/adolescent)
**abrupt discontinuation can cause withdrawal (anxiety, headache, muscle pain, nausea)
**high risk for overdose (life threatening dysrhythmias, confusion, seizure)
contraindications/interactions: Avoid use of MAOIs Avoid Anticholinergics (Why?) Avoid CNS depressants Cardiac dysrhythmias Seizure d/o Recent myocardial infarction (MI)
RN intervention/client education: Give @ bedtime Monitor orthostatic vital signs. Monitor for increases in depression and suicidal ideation. Taper the drug over 2 weeks to prevent or minimize withdrawal.
SSRI
prototype: fluoxetine (Prozac)
EPA: Block reuptake of serotonin → strengthened transmission of serotonin at serotonergic synapses
Admin: PO in morning due to CNS excitation. Takes 4-6 weeks to take effect
Therapeutic use: Many indications! Depression, anxiety, OCD, bulimia nervosa, premenstrual dysphoric disorder
ADRs: Insomnia, Sexual dysfunction, Weight gain, Serotonin syndrome **Increase risk for suicidal ideation (especially children, young adults) Serotonin syndrome; hyperpyrexia, agitation → coma, muscle rigidity, seizure
contraindications/interactions: MAOIs St. John’s wort Ibuprofen
RN intervention/client education: Monitor for insomnia, anxiety Monitor for dec. libido and/or impotence Monitor weight gain Monitor for inc. depression or suicidal ideation Monitor for s/sx serotonin syndrome Do not stop abruptly
SNRI
prototype: vanlafaxine (Effexor XR)
EPA: Block neuronal reuptake of serotonin AND norepinephrine → increased amt of serotonin/norepinephrine available
Admin: PO. Start with low dose and gradually titrate up.
Therapeutic use: Major depression, social anxiety disorder, generalized anxiety disorder (GAD)
ADRs: Very similar to SSRI. Sexual dysfunction less common than w/SSRI and can cause hypertension
Contraindications/interactions: MAOIs First Generation Antipsychotics/Typicals Ibuprofen
RN intervention/client education: Take in the morning w/food Monitor for insomnia Monitor for dec. libido and/or impotence Monitor weight gain Monitor for inc. depression or suicidal ideation Monitor for s/sx serotonin syndrome Do not stop abruptly Monitor BP periodically
MOAI (monamine oxidase inhibitors)
prototype: phenelzine (Nardil)
EPA: Blocks monoamine oxidase-A and Monoamine Oxidase – B
Admin: PO. Start with low dose possible
Therapeutic use: Depression that hasn’t responded to other medications, Depression in Bipolar
ADRs: CNS stimulation, Constipation, weight gain, sexual dysfunction, orthostatic hypotension
**Hypertensive crisis when eating foods containing tyramine (aged cheeses,/meat, yeast, chocolate, alcohol)
Contraindications/interactions: Cardiac disease Clients > 60 SSRIs Glaucoma
RN intervention/client education: Monitor Vital signs and BP Provide client a list of foods to avoid Instruct client to report severe anxiety, insomnia and agitation to provider
Atypical Antidepressant
prototype: BUPROPION (Wellbutrin)
EPA: Inhibits dopamine reuptake thereby inc dopamine availability
Admin: PO
Therapeutic use: Depression, Seasonal affective d/o; adjunctive to smoking cessation
ADRs: weight loss, appetite suppression, inc risk for seizure. CNS stimulation: insomnia, agitation, tremor.
**Inc risk for psychosis/hallucination
contraindications/interactions: History of an eating disorder Seizure disorder MAOI Head trauma or tumor in the CNS (why?) Interacts with many medications
RN intervention/client education: Weekly weights Assess for ADRs Assess for inc. depression symptoms or suicidal ideation
Mood Stabilizer
Prototype: lithium carbonate (Lithobid)
EPA: Not well understood. Changes to transport of sodium ions in nerve cells and alters metabolism of catecholamines (fight or flight) in response to stress. This is thought to dec. mania assoc w/bipolar.
Administration: PO; give w/milk or food to reduce GI upset
Therapeutic Use: Controls acute mania and acute manic episodes assoc. w/bipolar disorder. Used prophylactically to prevent recurrence of mania or depression
ADRs: Therapeutic levels: GI distress, confusion, muscle weakness, memory impairment. Polyuria, dec. secretion of thyroid hormone àgoiter or hypothyroidism. Fine hand tremors.
Toxicity due to narrow therapeutic range (muscle weakness, fine tremor progressing to coarse tremor, ataxia, confusion, seizures, coma, and death)
Contraindications/Interactions:
•Pregnancy/Lactation
•Moderate-Severe cardiac disorders
•Dehydration
•Hyponatremia
•MANY DRUG INTERACTIONS
•AVOID NSAIDS
RN Intervention/Client Education
NARROW therapeutic range
Monitor Lithium levels. Desired serum plasma levels = 0.6-0.8 mEq/L
Regular Bloodwork:
Electrolytes (sodium) and CBC
thyroid function - hypothyroidism
renal function
Monitor for signs/symptoms of toxicity and other ADRs
Drink 2-3L of fluid per day
Avoid caffeine and stressors
Consume foods with sodium
FIRST GENERATION ANTIPSYCHOTICS (FGA)/TRADITIONAL
Prototype: chlorpromazine
Other Drugs: haloperidol (Haldol)
EPA: Block several receptors: norepinephrine, acetylcholine, dopamine, histamine.
Administration: PO, IV, IM, Rectal
Therapeutic Use: Suppresses symptoms of schizophrenia. Acute manic phase of bipolar disorder
ADRs:
Extrapyramidal symptoms (EPS): Abnormal muscle contraction/posturing and Acute dystonia
Neuroleptic malignant syndrome: Fever, stiffness of muscles, altered mental status, change in BP resp. failure
Akathisia (inability to sit still)
Anticholinergic Symptoms (dry mouth, dizziness, urinary retention, etc)
Parkinsonism
Orthostatic hypotension
Cardiac arrhythmias à prolonged QT interval
Liver failure
Contraindications/Interactions
alcohol/other CNS depressants
Caution with meds that activate dopamine receptors (levodopa)
SSRIs àincrease levels of serotonin à serotonin syndrome
Hyponatremia
Antihypertensives
Pregnancy/Lactation
Parkinsons disease, bone marrow depression
RN Intervention/Client Education
•Monitor for ADRs
•wear gloves when handling
•Have client report:
•muscle rigidity, tremors, and sluggish movements, drooling, and shuffling gait
•severe spasms of the neck and body
•involuntary movements of tongue, face, limbs, trunk
•palpitations, fainting spells, other cardiac symptoms
•avoid sun exposure, use sunscreen, wear protective clothing, wear sunglasses
•sudden fever immediately to provider
SECOND GENERATION ANTIPSYCHOTICS (SGA)/ATYPICALS
Prototype: risperidone (Risperdal)
Other Drugs: olanzapine (Zyprexa), quetiapine (Seroquel), apriprazole(Abilify), clozapine (Clozaril)
EPA: Block receptors for dopamine and serotonin. Dopamine blockade is less than conventional antipsychotics thus fewer EPS occur
Administration: PO – instructions vary by drug
Therapeutic Use: Treat symptoms of Schizophrenia and Bipolar disorder
ADRs: sedation, hypotension (blockade of alpha-adrenergic receptors); Metabolic syndrome: wtgain, diabetes, dyslipidemia; Arrhythmias; Agranulocytosis (Clozapine); Extrapyramidal symptoms when given high doses
Contraindications/Interactions
•Prolonged QT (EKG)
•Severe CNS depression
•Psychosis related to dementia in older adults
•Pregnancy/Lactation
•Drugs to treat parkinsons disease
•MANY drug interactions
RN Intervention/Client Education
Very similar to FGAs/Typicals
Weekly blood tests (CBC)
Periodic blood glucose monitoring
Report lethargy/flu like symptoms
Notify provider if you become pregnant
Notify provider if you have increased HR
WARNING:
administration of clozapine and other second-generation antipsychotics to elderly patients with dementia can increase risk of death. The FDA has not approved the drug for use in dementia-related psychosis.
Centrally Acting Muscle Relaxants
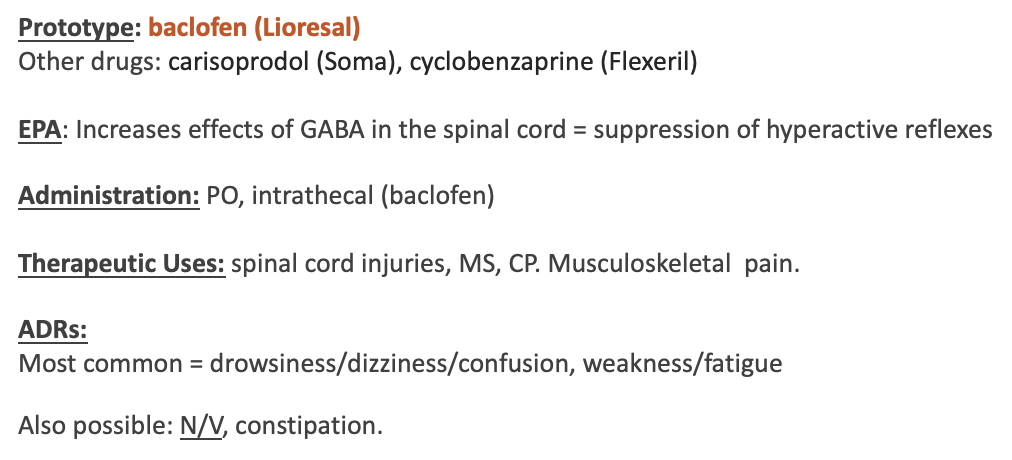
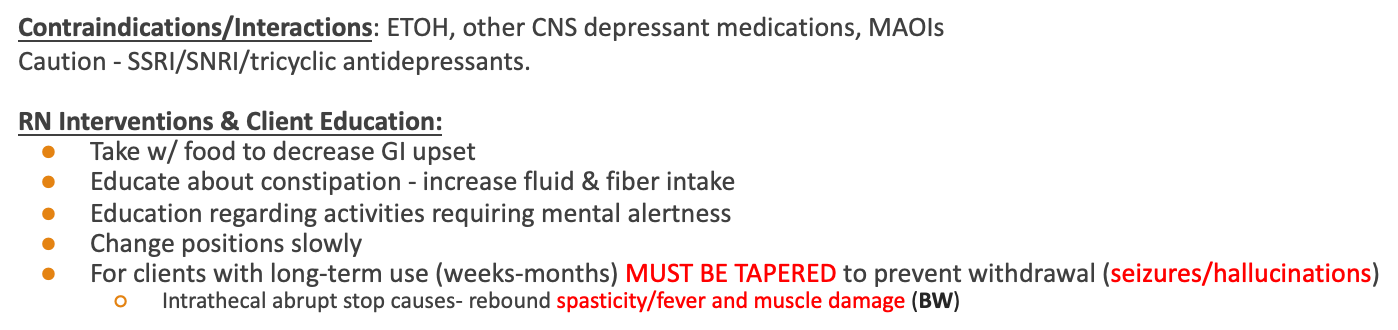

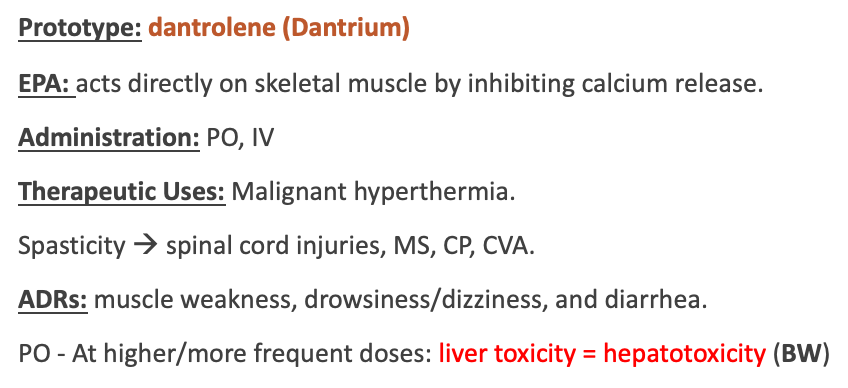


(p)
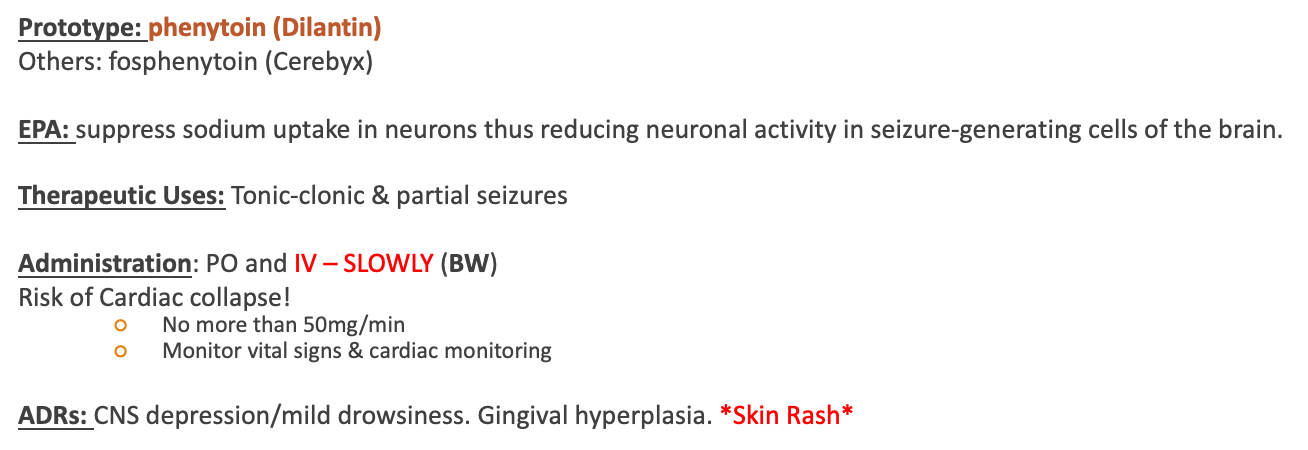
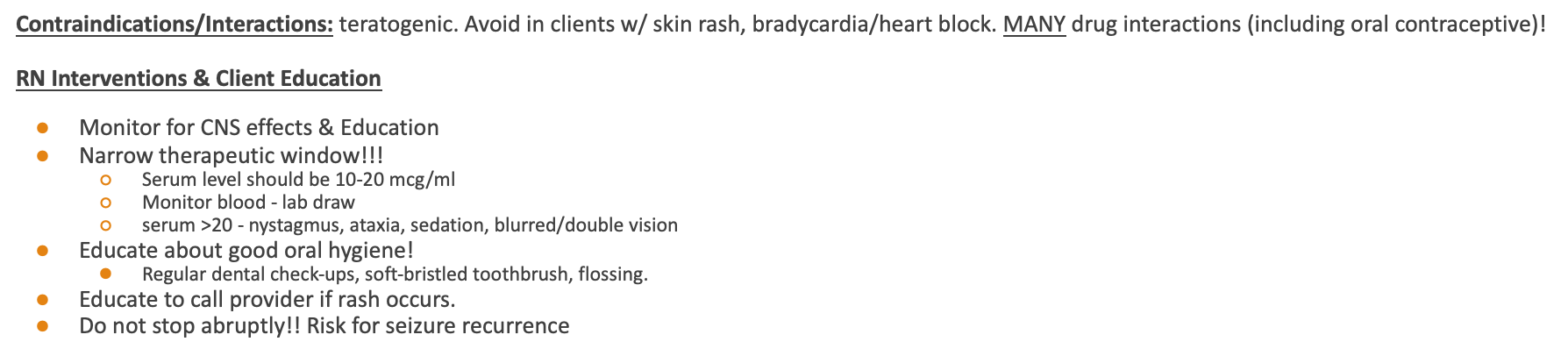
Traditional AEDs (2)
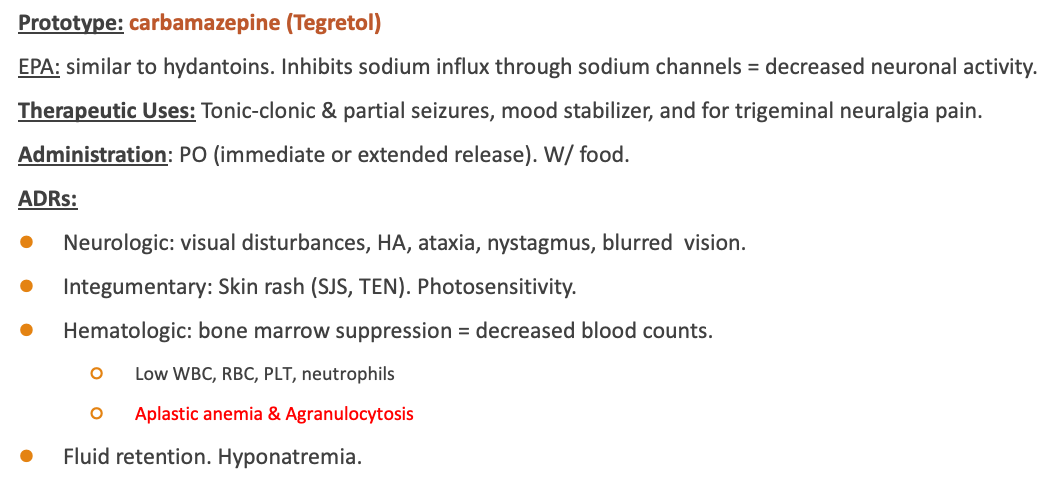
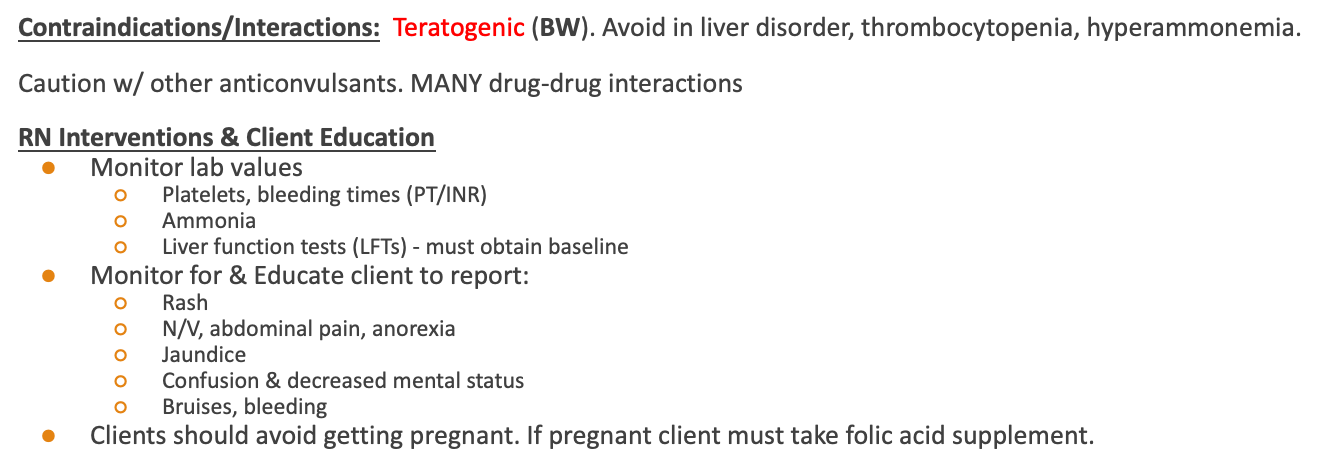
Traditional AED (3)

Newer AEDs 2