Cardiopulmonary Final Study Guide
1/146
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
147 Terms
Understand basic anatomy of the cardiovascular system
Major tissue structures of the heart include? (4)
What are the layers of the heart? What does each layer do?
________ fluid acts as a ________ for the two layers.
major tissue structures of the heart include muscle, connective tissue, blood vessels, and nerves
endocardium: lines the inner surface of the heart/valves and is in contact with the blood
myocardium: thick muscular tissues, which provide pumping forces
epicardium: lines the outer surface of the heart and protects against infection and trauma
pericardium: a double walled sac, which surrounds and cushions the heart
pericardial fluid: acts as a lubricant for the two layers
Review normal cardiac function.
Which side receives oxygen rich vs oxygen poor blood?
right side of the heart receives oxygen poor blood
left side of the heart receives oxygen rich blood
How does sexual activity impact cardiac function? Think in terms of METs.
How many METs does sex cause? The doctor has to approve what level of exercise for sex to be cleared?
sex is between 3-5 METS. If the doctor tells them to do mod exercise, sex is okay
Have an understanding of ECG. What is normal? Abnormal?
-messed up electrolytes affects this!
-bradycardia: HR < 60 bpm (slow)
-tachycardia: HR > 100 bpm (fast)
-arrhythmias: irregular heart rhythms (atrial fibrillation)- ie. sinus arrhythmia
o using the term dysrhythmias now
Be able to identify ECG strips and make clinical decisions based upon that information.
See Cardiopulmonary ECG knowt: https://knowt.com/flashcards/e08674c6-1351-49dc-9852-4db06af2a556
Demonstrate basic knowledge and recognition of heart sounds as related to a particular diagnosis.
S1 - Sound and location
S2 - Sound and location
S3 - Sound location and cause?
S4 - sound location and cause?
Murmurs - What is it and what are the three types? Murmur in the arteries is called?
Pericardial friction rub - What is it?
S1 (first heart sound): "lub"
location: heard best at the apex of the heart
S2 (second heart sound): "dub"
location: heard best at the base of the heart
normal = "lub-dub, lub-dub, lub-dub"
S3 (third heart sound): "lub, dub, dub" after S1-S2 heart sounds
location: heard best at the apex, in the left lateral decubitus position
cause: rapid filling of the ventricles (aka ventricular gallop)
indicates heart failure
S4 (fourth heart sound): "la, lub, dub" before S1-S2 heart sounds
location: heard best at the apex, in the left lateral decubitus position
cause: atrial contraction against a stiffened ventricle (aka atrial gallop)
extra sound at the beginning "la, lub, dub"= S4, S1, S2; normal for Olympic level athletes (abnormal sign of hypertensives disease, coronary artery bypass, pulmonary disease)
murmur: swoosh or blow sound (like wind); loud and hard sound caused from turbulent blood flow through narrowed (stenosis) or leaky valves (regurgitation). Murmur in the arteries is called a bruit. There are three types:
stenosis: valve doesn't open properly
regurgitation: valve doesn't close properly
prolapse: leaflets get flappy/don't come together
pericardial friction rub: hear S1/S2 in the background; pericardium houses the heart, 2 layers filled with lubricant.
What is a murmur in the arteries called?
bruit
Understand signs and symptoms of the cardiac pathologies outlined in your handouts, along with the appropriate medical/surgical and physical therapy interventions, including exercise prescription.
Pharmacological management of coronary arteries disease: What is the goal?
Beta blockers
Calcium channel blockers
Nitrates
ACE inhibitors
Stroke volume: What is it? What are the three factors that influence it?
pharmacological management of coronary artery disease: goal to reestablish the balance of myocardial supply & demand
beta blockers: decrease beta sympathetic activity on the heart resulting in a decrease in HR and contractility and therefore energy demand
calcium channel blockers: reduce BP and therefore decrease the work of the heart; this type of medication also prevents coronary smooth muscle spasm and may increase myocardial blood supply
nitrates: potent vasodilators that decrease preload and afterload and therefore myocardial work as well as dilating coronary arteries
ACE inhibitors (angiotensin converting enzyme): reduces afterload, allowing the heart to pump more blood with each beat, improving cardiac output and reducing strain on the heart; frequently used to counteract the adverse effects of ventricular remodeling that occurs after MI
stroke volume: amount of blood ejected from the heart with each beat. influenced by 3 factors:
preload (ventricular stretch)
contractility (ability to squeeze)
afterload (resistance to ejection)
Be familiar with the Karvonen Formula.
What are the intensity levels and their target %HRR?
THRR= [(HRmax-HRrest) x intensity] + HRrest
1. 220- age = estimated max HR
2. Estimated max HR – resting HR = HR reserve (HRR)
3. HHR x percentage (e.g., 70% ) = percent of HRR
4. Percent of HRR + resting HR = target HR
![<p>THRR= [(HRmax-HRrest) x intensity] + HRrest</p><p>1. 220- age = estimated max HR </p><p>2. Estimated max HR – resting HR = HR reserve (HRR) </p><p>3. HHR x percentage (e.g., 70% ) = percent of HRR </p><p>4. Percent of HRR + resting HR = target HR</p><p></p><p></p>](https://knowt-user-attachments.s3.amazonaws.com/2af51e54-47cf-4492-898c-0e70fa8229dd.jpg)
Be aware of the particular safety precautions, including vital signs, associated with the cardiac pathologies.
-prolong the warmup and cooldown
-start the pt where they are
-monitor vital signs
-ask how the pt is feeling
What is the ischemic threshold?
ischemic threshold: the point at which myocardial oxygen demand exceeds oxygen supply, leading to ischemia. Above the RPP (rate pressure product)
patient becomes symptomatic: chest pain, ECG changes
cardiac rehab: stay below ischemic threshold (RPP)
How does the rate pressure product relate to ischemic threshold?
What is the equation?
What does it indicate?
Higher RPP means?
For cardiac rehab, this mean you must?
RPP= HR x SBP
indicates: myocardial oxygen demand (MVO2) aka the Double Product
Higher RPP = Higher oxygen demand: as HR or SBP increase, the heart requires more oxygen
For cardiac rehab, stay below ischemic threshold ( aka below RPP)
How is a heart attack diagnosed in the emergency department?
What are the most common methods?
What are the three ways?
For one of the ways, what is CK-MB and what does it indicate?
A rising of elevated troponin levels after 3 - 4 hours confirms what, even if ECG is normal?
What is troponin?
What is key for calcium regulation of the heart and skeletal contractions?
most common methods to determine MI: ECG and blood work + complaints
clinical assessment: the ED physician evaluates symptoms such as chest pain, SOB, nausea, dizziness, and radiating pain to the arm, neck, or jaw
electrocardiogram (ECG/EKG): a 12-lead ECG is performed immediately to detect changes in electrical activity, such as ST-segment elevation
blood tests (troponin and creatine phosphokinase [CK])- MB levels)**
the presence of elevated levels of CK-MB indicates MI
CK-MB is an enzyme released with intracellular myocardial damage
a rising of elevated troponin level after 3-4 hrs confirms MI, even if the ECG is normal
troponin is a protein found in heart muscle cells; when the heart muscle is damaged (aka heart attack), troponin is released into the bloodstream
Proteins stored in myofibrils that are key for calcium regulate heart and skeletal contractions
What precautions must be taken with a patient who has atrial fibrillation?
First, what are the concerns? What should you do? When should you stop treatment?
What type of exercise intensity is good for this patient population? Avoid?
Watch out for? S/S?
Be aware of the patients _______, especially if using _________
concerns: irregular heart rhythm, reduced cardiac efficiency, and risk of blood clots or stroke
monitor vital signs closely
check HR, BP, and O2sat before, during, and after treatment; utilize RPE scale
stop treatment if HR spikes, severe fatigue, dizziness or lightheadedness and chest pain is present
utilize low to moderate intensity exercises
avoid sudden burst of exertion (light aerobic activity)
avoid Valsalva maneuver
watch out for poor cardiac output; s/s:
SOB
cyanosis
confusion
extreme fatigue
chest discomfort
be aware of the patients medications especially if using anticoagulants (blood thinners)
ex. meds (Warfarin, Apixaban, and Rivaroxaban)
increased bleeding risk, may cause bruising and bleeding
*medical clearance may be required
What is a safe exercise prescription for a patient who has compensated CHF?
First, what is CHF?
For exercise prescription., who should be consulted as needed?
Safe and regular exercise will?
Low level exercise is okay if the pt is?
Progress as the pt is able to?
What two types of training should be done?
What other vital sign should be monitored during the session?
Supplemental oxygen?
What should you do every visit and every single day at home?
Why?
CHF: systemic disease caused by ineffective contractility contributes to myocardial hypertrophy (R ventricle failed, JVD and bilateral LE edema present)
exercise prescription (consult with MD PRN)
safe and regular exercise: improve functional status and decrease symptoms
low-level exercise is okay if the pt is hemodynamically stable
progress as the pt is able to tolerate more activity (MODERATE)
resistance training and inspiratory muscle training
monitor oxygen saturation via pulse oximetry
need for supplemental oxygen? maybe only during exercise
weight them at every visit and at home every single day
pick up that subtle FLUID weight gain and tell MD to prevent complications
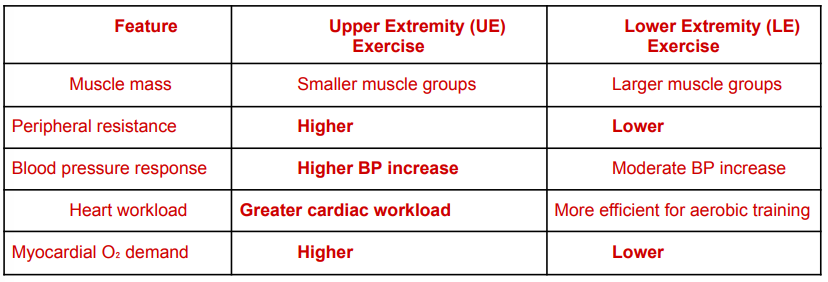
With myocardial oxygen demand, how does UE exercise contrast with LE exercise?
What about in terms of muscle mass, peripheral resistance, BP response, heart workload and myocardial oxygen demand?
What are the three main reasons why UE exercise increases myocardial oxygen demand?
in pts with cardiac conditions (including a-fib or coronary artery disease), UE exercise increases myocardial oxygen demand more than LE exercise at the same workload; more static/isometric components in arm activities raises BP significantly
key differences:
muscle mass
UE exercise: smaller muscle groups (less efficient O2 extraction)
LE exercise: larger muscle groups
peripheral resistance
UE exercise: higher (heart must pump harder)
LE exercise: lower
blood pressure response
UE exercise: higher BP increase
LE exercise: moderate BP increase
heart workload
UE exercise: greater cardiac workload
LE exercise: more efficient for aerobic training
myocardial oxygen demand
UE exercise: higher
LE exercise: lower
Why UE Exercise Increases Myocardial Oxygen Demand:
Smaller muscles → less efficient oxygen extraction
Higher peripheral vascular resistance → the heart must pump harder.
More static/isometric components in arm activities → raises blood pressure significantly.
What activities would be included in Outpatient Cardiac Rehab? Exercise prescription?
Exercise
Education
Monitoring
Exercise prescription FITTE
Goals
Activities
exercise
aerobic training
resistance training
flexibility
education
risk factor modification
lifestyle changes
monitoring
HR, BP, ECG, RPE
exercise prescription (FITTE)
frequency: 3-5 days/wk
intensity: 40-80% HRR or RPE 11-14
duration: 20-60 minutes
goals
improve cardiovascular endurance
restore functional capacity
reduce risk factors
activities
treadmill walking
stationary cycling
elliptical
light resistance training
flexibility exercises
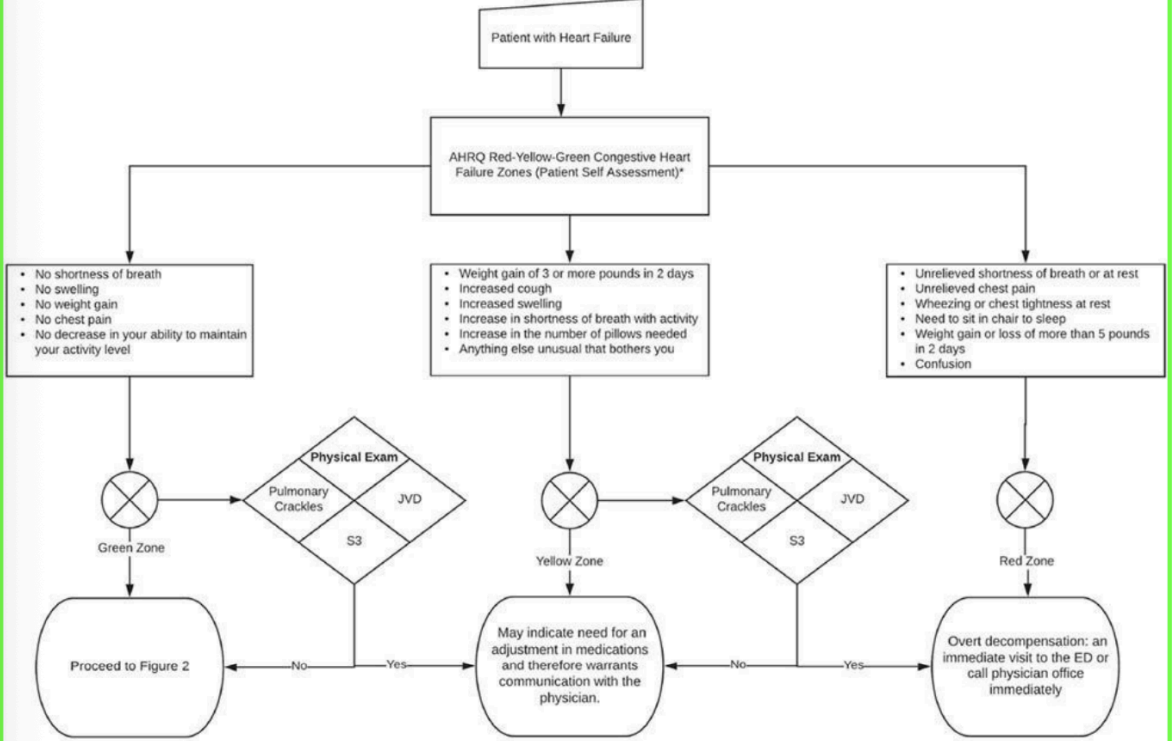
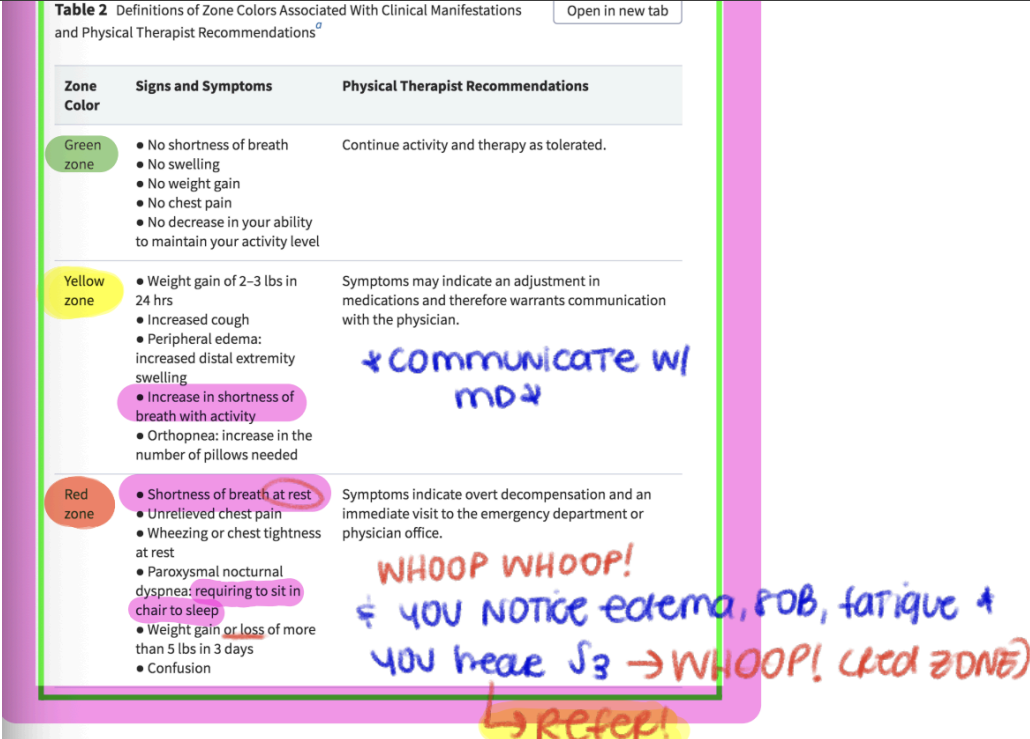
Be familiar with the Heart Failure Clinical Practice Guidelines published in 2020.
• Table 2 Zone Colors (Green, Yellow, Red)
• Figure 1 Algorithm
How does the RESPeRATE biofeedback machine help in the treatment of hypertension?
What is it?
Decreases what three things? Prolongs? Stimulates what nerve, this elicits what?
Measures what? What feedback can it give?
Strapped around where on the body?
How long does it stay on?
FDA approved biofeedback device for HTN
decreases RR, HR, BP, and prolongs exhalation, stimulates the vagus nerve, elicits parasympathetic response
measures your respiration and gives you feedback on when to slow your respiration down
auditory feedback (tones): "breathe in, breathe out"
strapped around your waist
will stay on for entire 15 minute session
What is the Zona Plus?
By what mechanism does this device work to lower blood pressure? How does it give feedback?
FDA approved biofeedback device for HTN. It is a handheld, isometric exercise device designed to help lower BP through controlled grip exercises
It was believed that isometrics are bad for HTN, but it's not true! The issue is when the pt is holding their breath (have them talk, count reps, valsalva, etc.)
Squeeze as hard as you can w/o hurting yourself until the device tells you to stop; once you start treatment, it will let you know when you are squeezing too hard or too soft
Visual and auditory feedback: "hold, squeeze more, etc."/beeps
How might the symptoms of a myocardial infarction differ between men and women?
common symptoms in women: may or may not have chest pain and are more likely to report...
usual fatigue (often days before MI)
SOB (even w/o chest pain)
N/V, or indigestion-like symptoms
back, jaw, or neck pain
dizziness or lightheadedness
cold sweats
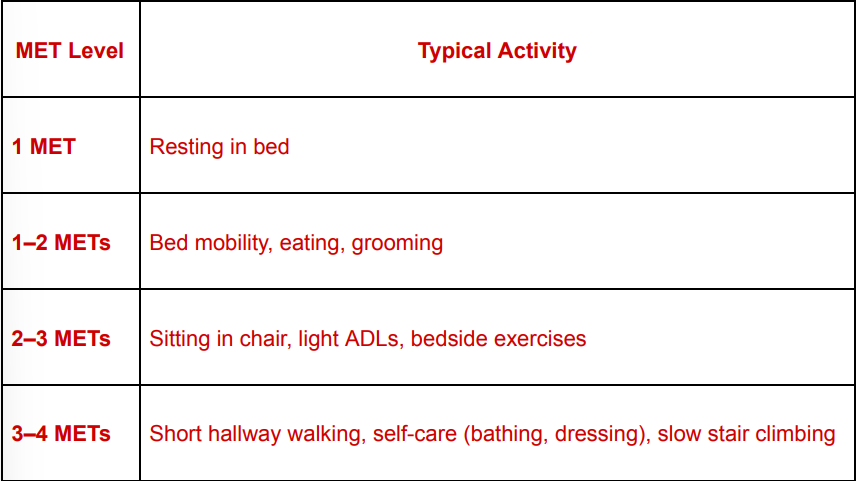
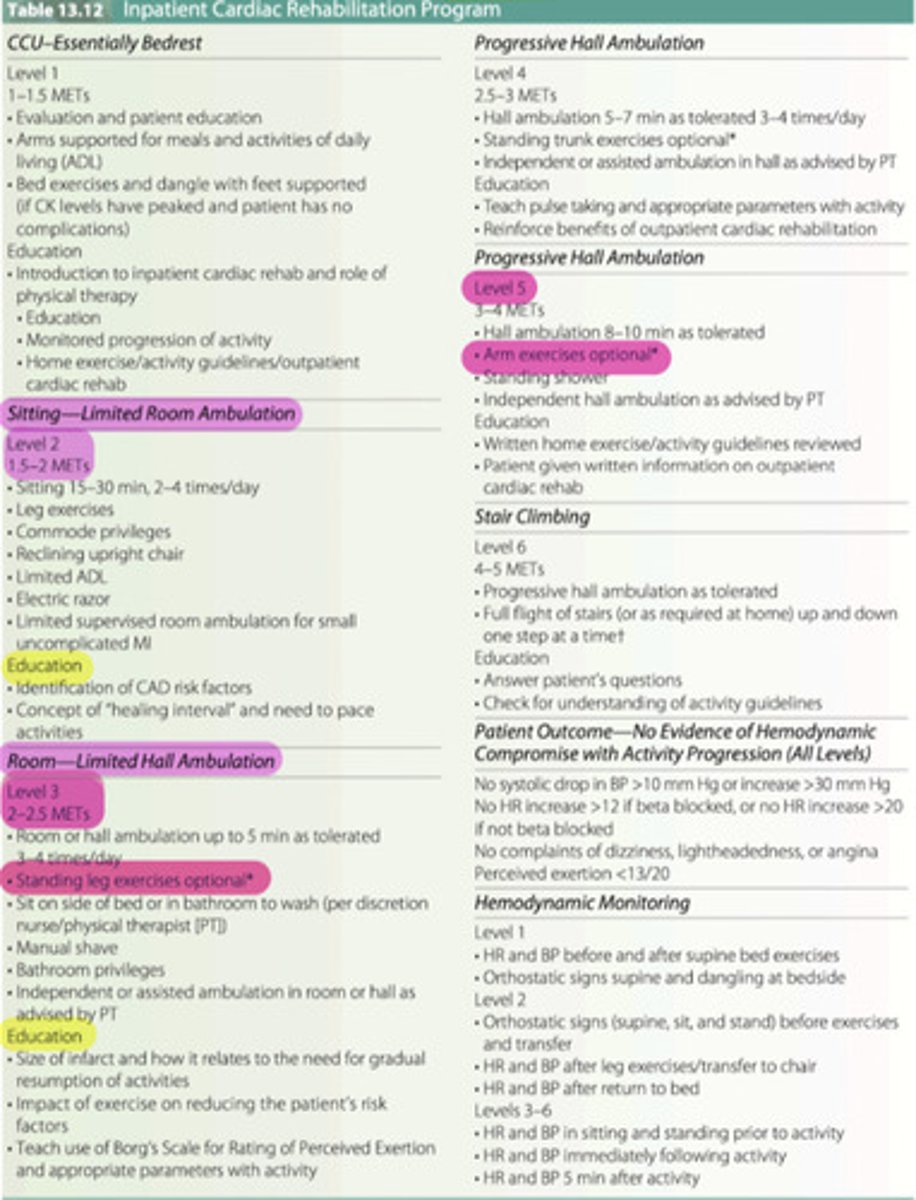
Describe MET levels and associated activity in Inpatient Cardiac Rehabilitation Phase I.
In phase 1, why are activities progressed according to METs?
What are the activities for each met level (1, 1-2, 2-3, 3-4)
Therapists usually keep METs, HR, and RPE less than or equal to?
Stop exercise if?
in Phase I inpatient cardiac rehabilitation, activities are progressed according to METs to ensure the heart is not overloaded after events such as myocardial infarction, cardiac sx, or coronary artery disease
1 MET
resting in bed
1-2 METs
bed mobility, eating, grooming
early mobility activities: PROM or AROM
2-3 METs
sitting in chair, light ADLs/self-care, bedside exercises
intermediate activity: standing exercises
3-4 METS
short hallway walking, self-care (bathing, dressing), slow stair climbing
higher end of inpatient activity: bathroom activities
therapists usually keep activity:
≤4 METs
HR increase ≤ 20 bpm above resting
RPE ≤11-13
stop exercise if symptoms occur such as chest pain, dizziness, or severe SOB!
What cardiovascular complications are associated with women taking birth control pills?
thrombosis (blood clots)
What role does estrogen play in cardioprotection for women?
Protects the heart by? (5)
After menopause, what can be seen?
protects the heart by:
improving blood flow (vasodilation, lower BP) through nitric oxide (NO)
enhancing cholesterol level (increasing HDL, lowers LDL)
reducing inflammation and oxidative stress
prevent excessive clotting by balancing clotting factors
improving insulin sensitivity, lowering risk of diabetes
after menopause:
estrogen drops, leading to higher BP
worse cholesterol
increased inflammation
diabetes risk
raising heart disease risk
What "white coat syndrome” and how would you assist a patient with it?
White coat syndrome: pt's BP rises in a clinical setting due to anxiety but is normal outside the office
monitor BP, deep breathing exercises, relaxed environment (quiet, comfortable setting with feet flat on the floor and back supported)
How does the vagus nerve relate to cardiac function?
How does it decrease HR?
What is the other thing it decreases? What does it mean?
through parasympathetic control (regulating)
decreases HR: the vagus nerve releases acetylcholine, which slows the firing of the SA node (the heart's natural pacemaker) and reduces HR
decreases contractility: it slightly reduces the force of contraction in the heart muscle (myocardium)
A patient is at Level 3 in her inpatient cardiac rehabilitation program. What activities are indicated at this point?
Level 3 indicates ______ activity with increasing _______.
Typical level 3 activities? (5)
Exercise parameters? (Intensity, RPE, HR, duration)
PT monitoring? (4)
Stop exercise if? (4)
in most hospital cardiac rehab protocols, Level 3 indicates moderate activity with increasing independence
typical Level 3 activities
ambulation in hallway 150-300 ft (45-90 m)
slow stair climbing (usually 1 flight)
self-care activities (ADLs) independently
light UE activities
seated or standing exercises
exercise parameters
intensity: 2-2.5 METs
RPE: 11-13 (light to somewhat hard)
HR increase: ≤20-30 bpm above resting
duration: 5-10 minutes of continuous walking
PT monitoring
HR
BP
O2 saturation
symptoms: angina, dizziness, dyspnea
STOP EXERCISE IF:
angina
SBP drop >10 mmHg
HR abnormal response
severe dyspnea
What precautions must be taken with a patient who has an automatic implantable cardiac defibrillator or pacemaker?
Know what threshold? This means keep HR at what range and why?
Can aerobic activity be performed?
Can TENS unit be used?
Contact sports participation?
Early post implant precautions (4)? Duration of precautions? Purpose of precautions?
Exercise considerations? (3)
What to do if ICD shock happens?
know the discharge threshold: keep HR 20-30bpm BELOW the activation threshold to avoid inappropriate shocks
you CAN do aerobic exercise with this pt
NO TENS unit
NO contact sports
important especially during early rehab after implantation
early post-implant precautions (first 4-6 weeks)
no shoulder flexion or abduction >90° on the side of implantation
no lifting >5-10 lbs
avoid pushing/pulling with affected arm
avoid sudden arm movements
purpose: prevent lead displacement
exercise considerations
avoid exercise near device shock threshold
monitor HR carefully
avoid strong electromagnetic interference (rare in PT clinics)
if ICD shock occurs
stop activity
monitor vitals
notify physician if multiple shocks occur
What does rate modulation indicate with a pacemaker?
Traditional pacemakers deliver a _____ heat rate when they detect bradycardia; Rate modulation sensory detect what things to increase or decrease the HR accordingly? This helps?
What does rate modulation mean? Why use it?
Sensors may detect what 4 things?
Clinical PT implication:
HR response may not be?
What other things should be used to monitor intensity?
adjust HR based on the pt's activity level or physiological needs
traditional pacemakers deliver a fixed heart rate when they detect bradycardia; rate modulation sensory detect body movement, breathing, or other physiological changes and increase or decrease HR accordingly
this helps pts maintain appropriate cardiac output during activities like walking, climbing stairs, or exercising
rate modulation means the pacemaker automatically increases HR in response to activity or metabolic demand bc some pts cannot increase HR normally (chronotropic incompetence)
sensors may detect: motion, respiration, body temperature, QT interval changes
clinical PT implication
HR response may not be perfectly proportional to exercise intensity
use RPE and symptoms in addition to HR to monitor intensity
What cardiopulmonary complications are associated with cocaine? Morphine?
Cocaine is a strong ________ ________. What are the cardiac complications associated with cocaine use? Pulmonary complications? In PT, pts may present with?
Morphine is a _______ _______ _______ _______. What are the cardiovascular effects associated with morphine use? Pulmonary effects? PT implication?
cocaine: strong sympathomimetic stimulant.
cardiac complications:
myocardial infarction
arrhythmias
coronary vasospasm
HTN
sudden cardiac death
cardiomyopathy
pulmonary complications:
pulmonary edema
respiratory failure
in PT:
pts may present with chest pain despite normal coronary arteries due to vasospasm
morphine: a central nervous system depressant
cardiovascular effects:
hypotension
bradycardia
peripheral vasodilation
pulmonary effects:
respiratory depression
reduced respiratory drive
PT implication:
monitor respiratory rate and oxygenation closely
How does autonomic neuropathy impact the heart rate response during exercise?
Often seen in which population?
Normal exercise response VS autonomic neuropathy response?
PT implication?
often seen in diabetes
normal exercise response
sympathetic activation-> HR increases appropriately
with autonomic neuropathy
blunted or absent HR response
reduced HR variability
possible orthostatic hypotension
PT implications
use alternative intensity measures (As HR alone becomes unreliable)
RPE (preferred)
workload
BP monitoring
symptoms
What precautions must be taken with a patient who had a heart transplant?
Heart transplant issues? (5)
Exercise prescription?
Rules when it comes to assistive devices? How would they get out of bed?
Heart transplant patients have cardiac denervation. What are the physiological effects (3)? Exercise monitoring?
Additional PT precautions (because of immunosuppression (3) and other things to monitor (3)
heart transplant issues:
denervated heart issues
vagus nerve and sympathetic fibers are severed during the transplant
changes in BP
increased risk for orthostatic hypotension due to delayed vascular tone adjustment
sternal precautions/immunocompromised
heart transplant recipients require lifelong immunosuppressive therapy to prevent organ rejection
fatigue is a sign of rejection or ischemia
if fatigue worsens or is accompanied by other symptoms, stop exercise and seek medical evaluation; educate pts!
deconditioned
prolonged pre-transplant inactivity from heart failure, post-surgical recovery limitations, effects of immunosuppressive medications (muscle atrophy, bone loss)
exercise prescription= focus on RPE, duration, and gradual increases
no crutches
no WB w/walker
move in tube- how they'd get out of bed
cardiac denervation physiological effects:
resting HR high (~100-110 bpm)
slow HR increase during exercise
HR recovery slow after exercise
due to no autonomic nerve connection
exercise monitoring
RPE (11-14)
workload
BP
symptoms
HR not reliable early in exercise
PT precautions
because of immunosuppression:
infection risk
monitor wounds carefully
avoid sick contacts
monitor for:
rejection signs
HTN
OP from medications
How might an exercise prescription be modified for a patient with congenital heart defects?
Frequent?
Monitor for what three things?
Sessions should initially be _____, especially for what type of patients?
Avoid what 4 things?
When should RPE be used?
Needs what before starting a program?
frequent rest breaks
monitor for dizziness, fatigue, SOB
supervised sessions initially, especially post-surgical pts
avoid Valsalva maneuver and isometric holds (can increase BP and strain the heart), and avoid heavy lifting and contact sports-> risk of aneurysm
use RPE instead of HR if medications affect HR response (beta-blockers)
individualized clearance from a cardiologist before starting a program
What is the exercise prescription when treating elevated cholesterol levels?
Aerobic exercise, resistance training, HIIT, and lifestyle integration?
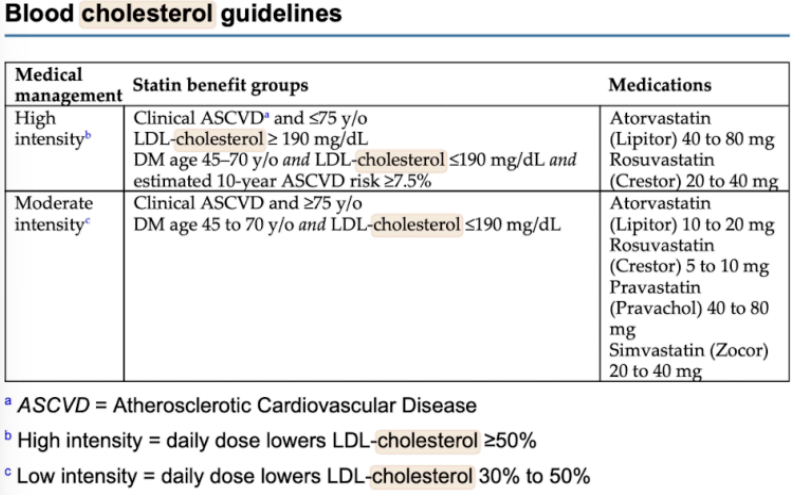
Blood cholesterol guidelines?
Aerobic exercise, resistance training, HIIT, and lifestyle integration:
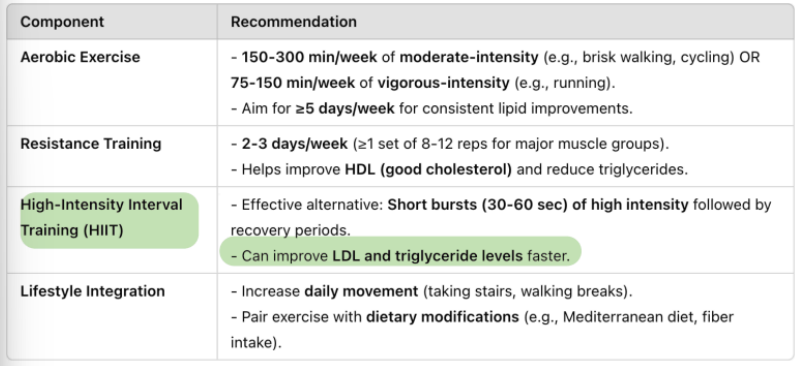
HIIT can improve LDL and triglyceride levels faster
Blood cholesterol guidelines:
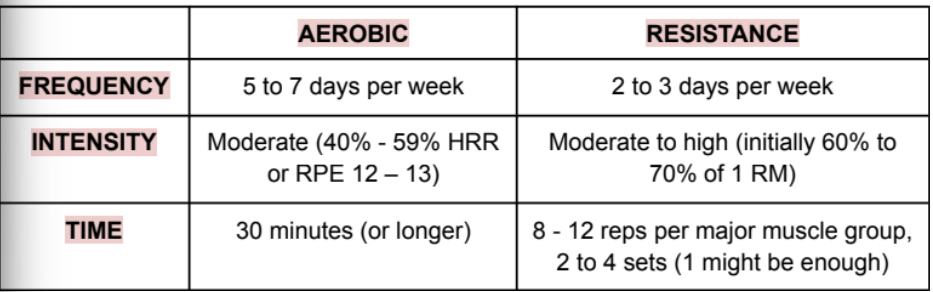
What is the exercise prescription and lifestyle modification needed when treating hypertension? (For aerobic and for resistance)
Frequency
Intensity
Time
What is the multimodal approach?
Lifestyle modifications? (Promote what diet? Foods rich in? Limit? Get good what?)
Monitor what?
Be aware of what influence? Why?
frequency
aerobic: 5-7 days/wk
resistance: 2-3 days/wk
intensity
aerobic: moderate (40-59% HRR or RPE 12-13)
resistance: moderate to high (initially 60% to 70% of 1 RM)
time
aerobic: 30 minutes or longer
resistance: 8-12 reps per major muscle group, 2-4 sets (1 might be enough)
multimodal approach: aerobic activities, resistance training, flexibility exercises (consider other neuromotor activities, like yoga and tai chi)
lifestyle modifications: promote the DASH diet (acts as diuretic), potassium rich foods, limit sodium and stress, good sleep.
monitor vital signs
be aware of medication influence; if their lifestyle modifications are working, the medications might continue to lower their BP and cause hypotension
What are sternal precautions and how do they affect functional mobility? (Keep your Move in the Tube)
Do NOT do what 4 things?
Explain the tube concept. This allows for what while still protecting what area of the body?
do NOT lift, push, or pull more than 10lbs
do NOT push to get out of bed or a chair
do NOT raise your arms over your head
do NOT use AD (walker cane>>> not in tube)
the "tube" concept
arms stay close to the torso
movements are symmetrical
avoid wide or forceful arm movements
this allows more functional movement while still protecting the sternum
When would you stop exercise during a physical therapy session?
Cardiovascular symptoms?
Vital sign changes?
BP?
O2sat?
Other red flags?
exercise should be stopped immediately if the pt develops signs of cardiovascular or pulmonary instability
cardiovascular symptoms:
chest pain or angina
excessive SOB
dizziness or lightheadedness
palpitations or arrhythmias
cyanosis
severe fatigue
vital sign changes:
HR: excessive rise or drop
new arrhythmia
BP
drop in systolic BP > 10 mmHg with increasing workload
SBP > 250 mmHg
DBP > 115 mmHg
O2sat
SpO2 < 85-90%
other red flags
nausea
diaphoresis (cold sweating)
confusion
loss of coordination
A patient has a history of stable angina for which he takes nitroglycerin sublingual tablets as needed. He is exercising on the stationary bicycle. He begins to complain of chest pain. How do you respond?
If a patient with Stable Angina develops chest pain while exercising, you should treat it as exercise-induced angina:
1) stop activity
2) sit or lie them down and assess symptoms and vitals (HR, BP, O2, ask abt pain characteristics like location intensity radiation)
3) should have nitro on their body/always with them! ASK!
4) they put a pill under their tongue, NOT YOU, every 5 minutes (max 3 times). After every pill wait 5 minutes and reassess, if pain is still there give another pill and wait again. After three pills:
if it gets better, dismiss PT for the day
if pain is still there or gets worse, CALL 911 (Suspect MI)
Be able to identify signs and symptoms associated with excessive effort or exercise intolerance.
wheezing, cyanosis (bluish skin/lips)
chest pain, palpitations, dizziness
pale, cool, or clammy skin (heat exhaustion)
flushed, hot, dry skin (heat stroke)
severe muscle cramps, joint pain, excessive soreness
A patient has a diagnosis of atrial fibrillation for which he takes medication. During aerobic exercise you detect a significant increase in cardiac arrhythmia. How would you respond?
if a pt with a-fib develops a significant increase in arrhythmia during aerobic exercise, the PT should prioritize pt safety and cardiovascular monitoring
1) stop the activity immediately
-discontinue aerobic activity
-have the pt sit or lie down in a safe position
o this reduces myocardial workload and helps stabilize heart rhythm
2) assess the pt
-check and document:
o HR and rhythm
o BP
o oxygen saturation
o RR
o pt symptoms (ie. palpitations, chest pain, SOB, dizziness or lightheadedness)
3) monitor until rhythm stabilizes
-continue monitoring vitals while the pt rests
-if the arrhythmia returns to baseline and the pt is asymptomatic, continue to observe but do not resume exercise during that session without medical clearance
4) activate medical assistance if symptoms occur
-seek medical evaluation if the pt develops:
o chest pain
o syncope or near syncope
o severe SOB
o hypotension
o persistent or worsening arrhythmia
-notify the physician or activate emergency response if the pt becomes unstable
future exercise considerations
-for pts with a-fib:
o use lower exercise intensity
o monitor heart rhythm and symptoms closely
o use RPE (11-13) rather than HR alone
o gradually progress activity
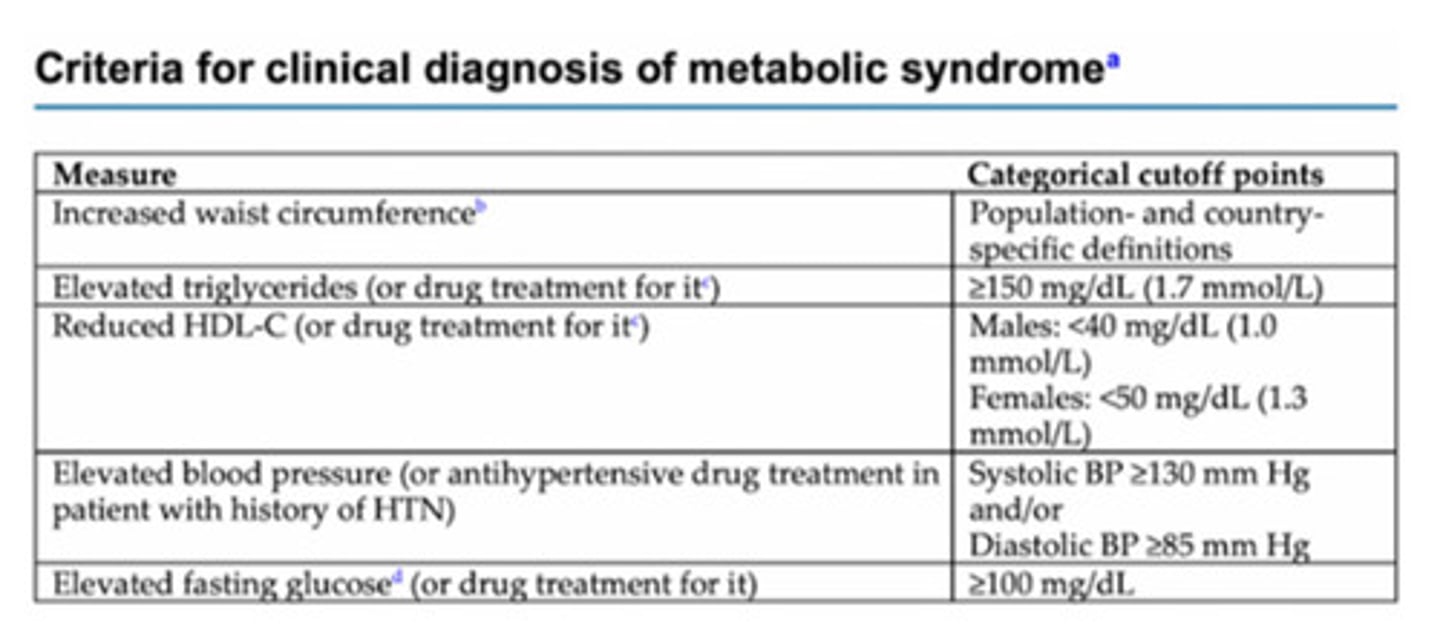
What is Metabolic Syndrome? How would it be treated?
cluster of conditions that increase the risk of heart disease, stroke, and type II diabetes (central obesity, high BP, high triglycerides, low HDL-cholesterol, insulin resistance)
treatment for Metabolic Syndrome
1) lifestyle changes (diet, no smoking, exercise)
2) aerobic exercise
3) medications (statins, metformin, aspirin)
Describe an exercise program for a patient with Diabetes. What precautions need to be taken?
-aerobic frequency: 3-7 days/wk (no more than two consecutive days without activity)
-intensity: mod to vigorous
-time: 150 minutes/wk
-type: aerobic (large muscle groups, rhythmic, continuous fashion
o include mod to vigorous resistance training to improve strength, flexibility, and balance activities
How does the aquatics environment impact a patient's cardiovascular status?
-ensure BP remains stable and pts do not experience orthostatic hypotension or cardiovascular collapse
-you don't want to take out a limp pt out of the pool
-hydrostatic pressure: promotes venous return and stabilizes BP (can limit the expansion of the lungs)
o individuals with heart failure or cardiovascular instability**: increasing venous return could overwhelm the heart--> cardiac overload and symptoms of HF, such as SOB, edema***, or rise in BP
o breathing against hydrostatic pressure: this can strengthen the muscles involved in breathing (like the diaphragm and intercoastal muscles) and improve overall respiratory efficiency, which is beneficial for cardiovascular health
-buoyancy: reduces weight-bearing stress, beneficial for pts with MSK pain or joint issues
-reduction of vital capacity (the total amount of air that can be exhaled after a full inhalation): hydrostatic pressure can limit the expansion of the lungs
o pts with conditions like COPD or asthma: beneficial as it provides gentle support to the chest and helps reduce the effort needed to breathe, making it easier to take deeper breaths without requiring as much effort
o pts that rely on maximal lung expansion: may find the water's resistance somewhat challenging (SOB), like those with healthy lungs or athletes
-temperature effects
o cool water: vasoconstriction can increase BP in people with cardiovascular conditions, such as HTN
o warm water: vasodilation can be helpful for individuals with chronic pain or muscle tightness but may need to be monitored in pts with cardiovascular instability (drop in BP)
What are the cardiovascular implications and precautions during pregnancy?
normal CV changes in pregnancy
-increased= HR (by 10-15 bpm) & cardiac volume/output
-physiological anemia: dilution of RBCs due to excess volume, not true anemia (look at lab values)
-cardiac arrhythmias (more common but usually not dangerous)
maternal response to aerobic exercise
-similar to a normal person, a lot of it depends on their pre-pregnancy exercise habit
-warm-up and cool-down should be longer
-avoid overheating (early morning/evening workouts)
-use RPE scale for intensity (cardiac arrhythmias)
-third trimester acts as a restrictive lung disease (SOB, great oxygen utilization bc they are breathing for 2)
what is preeclampsia/how would it be discovered in a pt?
-high BP (monitor closely); refer to BD is BP elevates
why must a pregnant woman avoid the supine position for longer than 5 minutes in the second and third trimester?
-compression of the IVC (left side lying is best)
What are the cardiovascular complications associated with eating disorders?
-first talk to them, assess severity of ED; low BMI? tachycardic?
-electrolyte disturbances: low levels of potassium, sodium, and magnesium can disrupt the normal electrical activity of the heart
-dehydration: can lead to reduced blood volume and low BP (hypotension)
-bradycardia: body is trying to conserve energy in response to starvation
-tachycardia: release of stress hormones (catecholamines)
-hypotension: dizziness, fainting, and increase the risk of falls and injuries
-ventricular arrhythmias: due to electrolyte disturbances
-mitral valve prolapse: heart murmurs, palpitations, mitral regurgitation
-cardiomyopathy: dilated heart, impairing its ability to contract and pump blood effectively (ipecac use)
o ipecac (a substance used to induce vomiting)
-cardiac failure: heart is so weakened that i cannot pump blood effectively
-diabetes insipidus: characterized by excessive urination and extreme thirst
What are the cardiovascular implications associated with substance abuse?
-immediate referral to a physician if the pt shows withdrawal symptoms= sweating, anxiety, shaking, slurred speech, impaired coordination or judgement, seizures, sleep disturbances, fluctuating consciousness, hallucinations
-if the pt is not in withdrawal and not in a tx program, refer to appropriate services (ie. inpatient rehab programs, 12-step programs, etc.)
What are the cardiovascular precautions associated with a patient who has end stage renal disease?
-schedule exercise sessions around dialysis; often the day before and the day of dialysis are the pt's weakest days
o intermittent exercise, with work-to-rest ratios of 1:1, may be appropriate initially, although most pts can gradually increase to 30-45 minutes of continuous exercise over time
-overall this group has low exercise tolerance--> probably due to lower arterial oxygen content bc of the following:
o lower hematocrit and hemoglobin values for oxygen transport
o altered stroke volume affected by the disease or its treatment
-the Borg perceived exertion scale works well in evaluating these pts
How are cancer treatments potentially cardiotoxic? What signs or symptoms would be present?
page 46
How would you modify physical therapy intervention for a patient receiving cancer treatment?
-monitor vital signs
-use the RPE scale instead of HR-based training
-avoid high-intensity exercise if cardiac function is impaired; if new or worsening cardiac symptoms occur, refer back to the medical team
-fatigue--> energy conservation techniques (spaced-out, rest breaks)
-no heavy straining or breath-holding to prevent undue cardiovaascular stress
How does the tilt table help diagnose autonomic nervous system dysfunction?
assessing how the body responds to changes in posture, particularly the transition from a horizontal to a vertical position
-normal response:
o increase HR, blood vessels constrict to prevent blood pooling in LEs
o stable BP
-autonomic system testing: not functioning properly, the HR may not increase sufficiently, or BP may drop too much leading to dizziness, fainting, or other symptoms (commonly used to evaluate orthostatic hypotension)
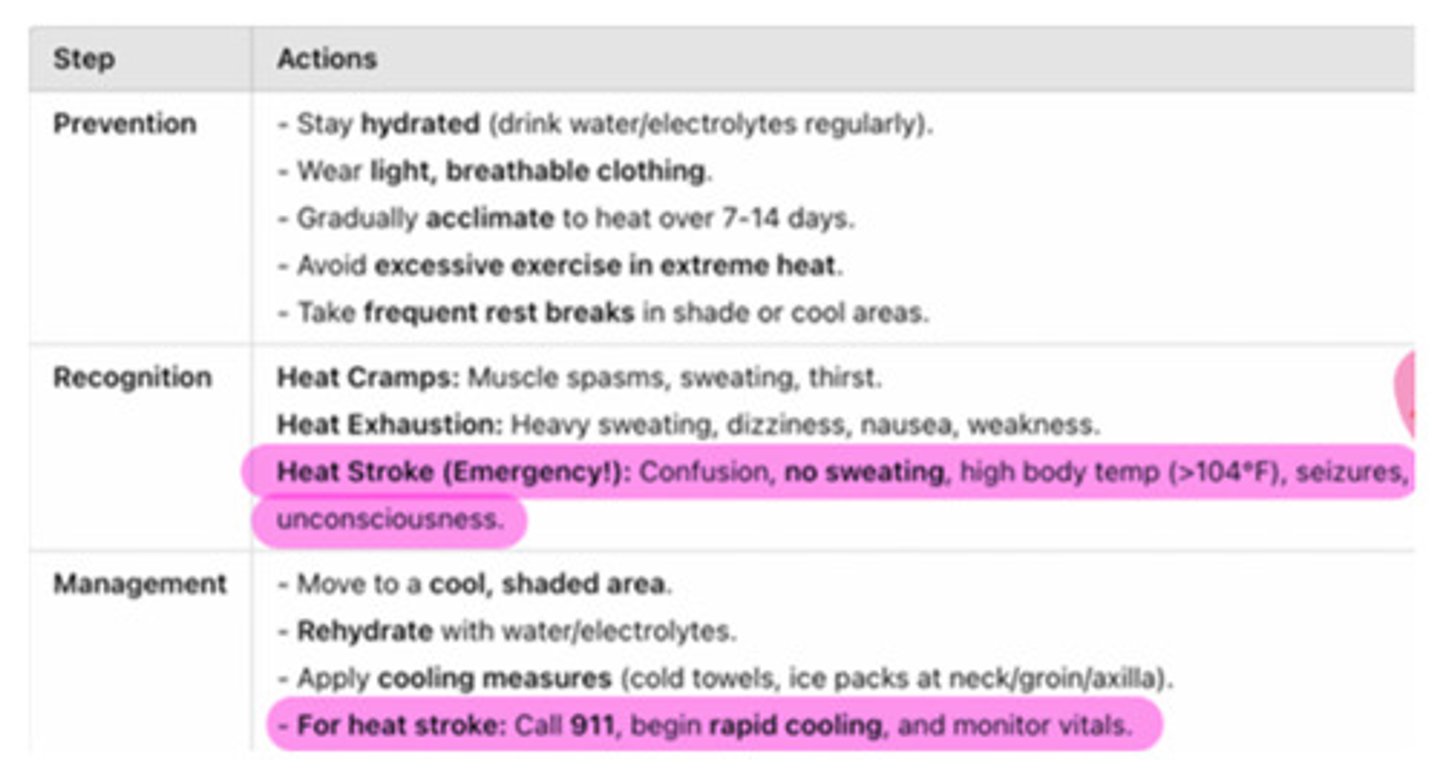
How could you prevent, recognize, and deal with heat illness?
TACO method: tarp assisted cooling oscillation
heat stroke= delirium
-stop activity!
-call them out of the game/practice
-rectal temperature is MOST accurate
What cardiac conditions might have implications for athletes?
-hypertrophic cardiomyopathy
-coronary artery anomalies
-Marfan syndrome: genetic disorder--> do they have a family hx?
-aortic rupture
-rhythm disturbances
-valve dysfunction
-myocarditis: inflammatory condition--> asymptomatic for COVID-19 but positive for myocarditis
-arrhythmogenic RV dysplasia: nonfunctional cardiac tissue--> turns into fatty of fibrotic tissue
-coronary artery disease: common cause of sudden death in older athletes
-sickle cell trait and acute sickling: cells clump together
-commotio cordis
-trauma to the chest wall that cause disruption of electrical impulses to the heart which can lead to v-fib
MD EMERGENCY! recognition and immediate response; importance of emergency care; use of the AED!
How does cardiac assessment relate to preventing sudden death in athletes?
-sudden cardiac death in athletes is often caused by undiagnosed heart conditions that become life-threatening during intense physical activity
-proper cardiac assessment helps identify at-risk individuals and prevent fatal events
-MFHX: hx of syncope, angina, palpitations, SOB with exercise
-physical examination: check for murmurs, dysrhythmias, or abnormal BP response--> exercise stress testing (for high-risk individuals)
Be familiar with advanced cardiac interventions and their physical therapy implications.
• Intraaortic Balloon Pump
• Ventricular Assist Device
• Extracorporeal Membrane Oxygenation (ECMO)
page 48
Be familiar with the diseases and treatments associated with arterial and venous conditions.
What precautions should be taken for individuals diagnosed with arterial or venous disease?
Describe ways to prevent a patient from developing a DVT.
movement, pneumatic pumps, compression, stockings, elevation, medication (anticoagulant)
-if suspected, PT is POSTPONED!
-associated with pain due to vein inflammation (deep ache)
-caused by an obstruction of the blood flow in the vein secondary to a collection of coagulated blood
o Homan's sign: pain upper calf with forced DF
o DVT--> pulmonary embolism--> death
-venous condition
Demonstrate understanding of the clinical practice guidelines for a patient with DVT or PE.
refer out if undiagnosed, stop all treatment--> both break off
What would be your exercise prescription for someone with intermittent claudication?
-frequency: 3-5 times/wk
-intensity: moderate intensity to the point of moderate pain (2-3 pain out of 4) or from 50-80% of max walking speed (not excruciating pain)
o get to the pain, don't stop before! rest and continue (get to MOD pain)
-time: 30-45 min/day (excluding rest periods) for a min of 12 weeks, may progress to 60 min/day
How would you differentiate between arterial and venous insufficiency?
venous insufficiency
-can lead to lymphedema
-needs to be treated!
-usually confined to the LEs (wounds on the medial aspect of the foot are commonly found)
-incompetent valves causing venous reflux
o clinical signs: edema, erythema, dermatitis, stasis pigmentation called hemosiderin (rusty reddish color from staining the skin due to RBC rusting)
venous insufficiency: results from weakened vein walls or valves, leading to blood pooling, edema, & ulcers with irregular borders, often around the ankle
-swollen, warm to touch, hemosiderin (iron)
arterial insufficiency: involves poor blood flow due to blockages in the arteries, causing pain, pale skin, & ulcers with defined borders
-diminished pulse, brittle nails, shiny skin
varicose veins: incompetent valves which produce increased venous pressure (leads to over stretched veins)
-tx: compression socks, exercise, procedures to close the veins
-s/s: edema, erythema, dermatitis, hemosiderin
-venous condition
chronic venous insufficiency treatment: edema reduction, preventing leg ulcerations, skin care, ambulation
-venous condition

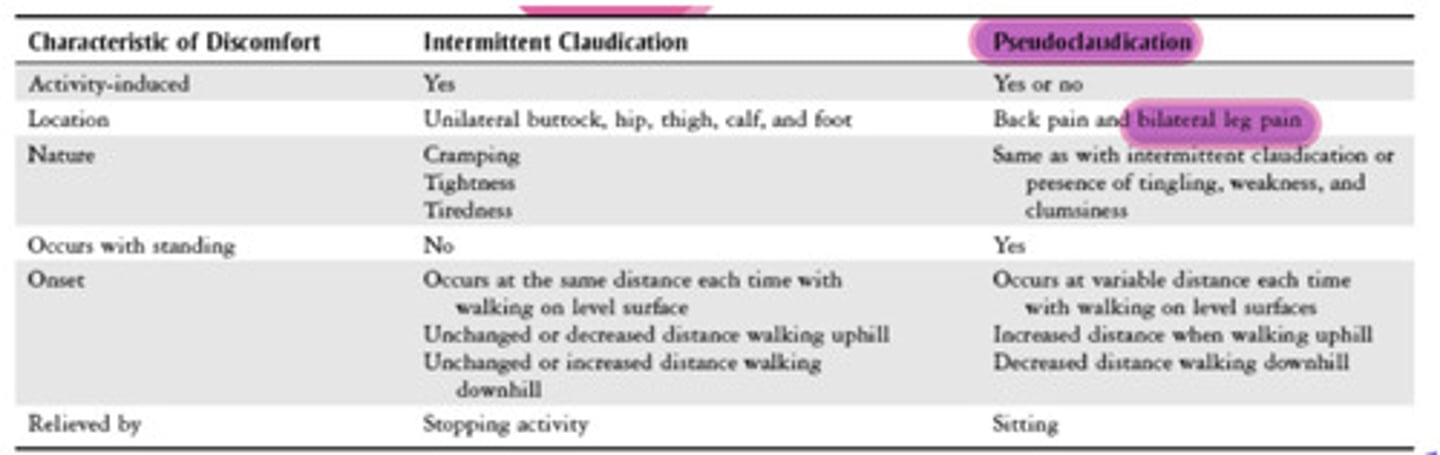
What is the difference between intermittent claudication and pseudoclaudication?
-true intermittent claudication (vascular supply & demand): painful cramping in LE, relieved with rest, consistent timing
-pseudoclaudication (neurological, spinal stenosis): flexion bias (uphill is better), bilateral
o stenosis causing pain
o relief with forward flexion and rest
What is protective sensation and how would it be tested?
the ability to feel minor sensations that protect the body from injury
-essential in pts with diabetes, peripheral neuropathy, or SCIs which may impair sensation, as they are at risk for unnoticed injuries
-testing
o sharp/dull test
o monofilament testing
o pinprick or pressure sensations
What is temporal arteritis? How is temporal arteritis treated?
-inflammation of the temporal artery
-tx: anti-inflammatory drugs (protozoan)
-s/s: artery popping out, pain, headache, face pain down the jaw, pain with chewing due to activation of muscles, neck pain, visual disturbances (relieved with rest)
o tends to happen to pts that have polymyalgia rheumatica, an autoimmune disease affecting primary people over 50 y/o (strong correlation btwn the two)
-REQUIRE IMMEDIATE ATTENTION--> ER!
o if left untreated the pt could go blind
-arterial condition
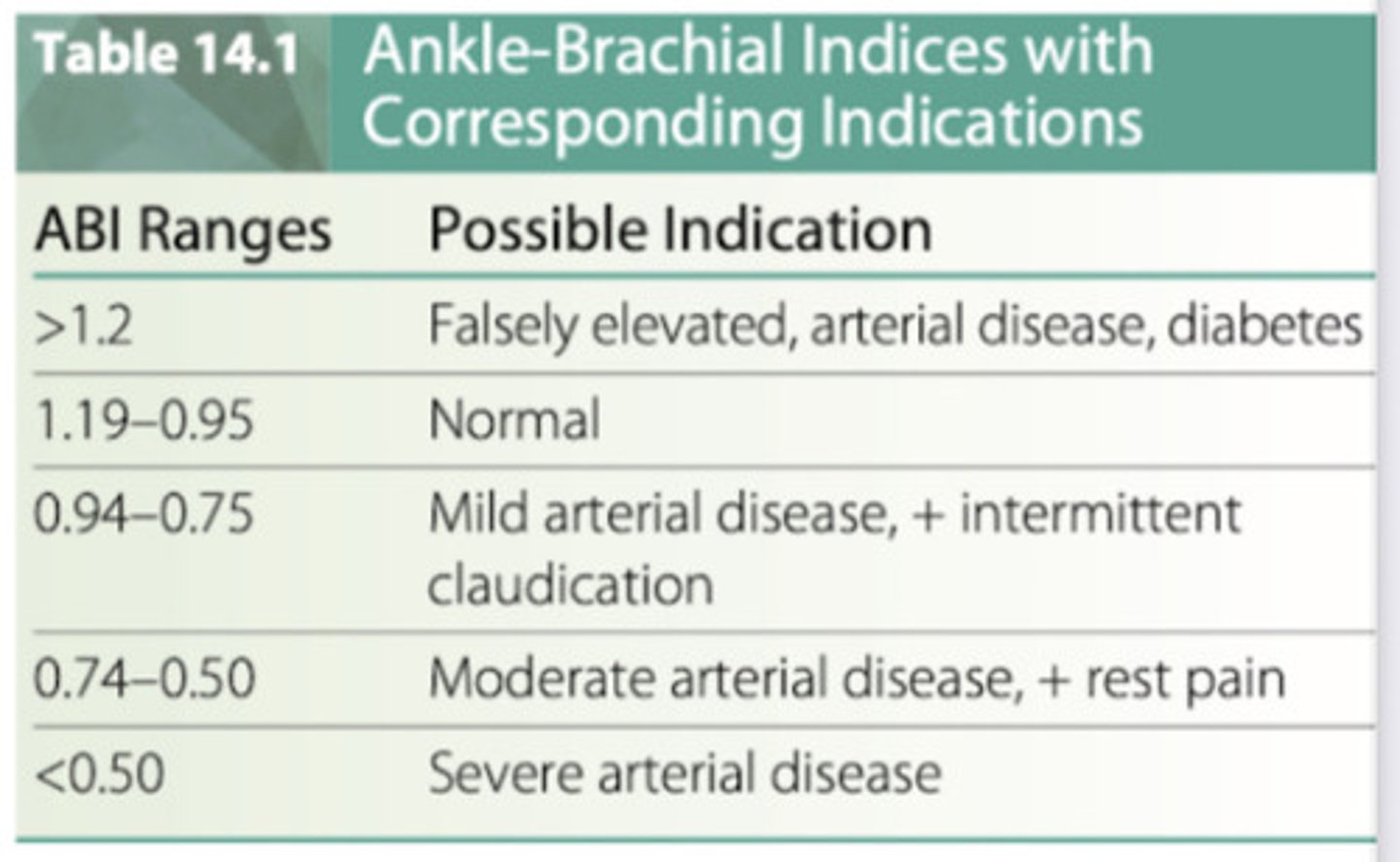
What is the ankle-brachial index and how does it relate to arterial health?
the ABI is the most frequently performed test using Doppler ultrasound
-noninvasive test that compares the BP obtained with a Doppler probe in dorsalis pedis or posterior tibial artery to BP in the higher two brachial pressures
-BP cuff is inflated to occlude blood blow temporarily & is then deflated as the examiner listens for the return of blood flow
-the ABI is a ratio of the LE pressure divided by the UE pressure
o normal ABI= 0.95-1.19
o severe arterial occlusive disease: <0.50
-Doppler exam
o used to detect blood blow; it shows whether a pulse is present & whether there is blood flow to a limb
Be able to identify the different hematologic disorders. Signs and symptoms? PT precautions?
page 12
Following a blood transfusion, what precautions should a physical therapist take with a patient?
PT should monitor vital signs, watch for transfusion reactions (fever, chills, SOB), begin with low-intensity activity, and ensure the pt is medically stable before therapy
-if any of these occur: stop therapy immediately and notify medical staff
How would having anemia impact the patient's exercise tolerance?
-pt may fatigue easier and quicker
-c/o headaches or dizziness
-always monitor vitals
What are the signs and symptoms of sickling?
-severe pain (bones, joints, chest, abdomen), shortness of breath, or fever during therapy
-PT action:
o stop tx immediately
o allow the pt to rest
o notify medical staff
How does having the sickle cell trait relate to athletes?
the CDC explains that most athletes with SCT have no problems, but certain conditions can increase the risk of exercise-related illness, including
-dehydration
-overheating
-sudden increases in exercise intensity
-high altitude
-exercising while sick or extremely fatigued
What precautions should be taken in a patient experiencing nadir?
nadir: the period after chemotherapy or radiation when blood cell count (especially WBCs) are at their lowest, which puts the pt at high risk for infection
-main precaution is preventing infection bc the pt's immune system is suppressed; this involves strict hygiene, limiting exposure to pathogens, monitoring for infection, and modifying therapy as needed
How would you respond if the patient is demonstrating signs and symptoms of leukemia?
if leukemia is suspected, the therapist should hold treatment, monitor the pt, and immediately refer the pt to medical staff for further evaluation
What precautions should be taken with a patient who has hemophilia?
-watch for muscle hemorrhages, especially the iliopsoas, gastrocnemius, and flexor surface of the forearm
-progress appropriately
o start with PROM and then AROM
o WB activities can be dangerous
o watch for signs of JOINT EFFUSION (warmth and edema)
Be able to explain appropriate skin care to your patient.
-keep the skin clean and dry
-moisturize daily
-prevent pressure injuries
-inspect skin daily
-manage moisture
-protect against friction
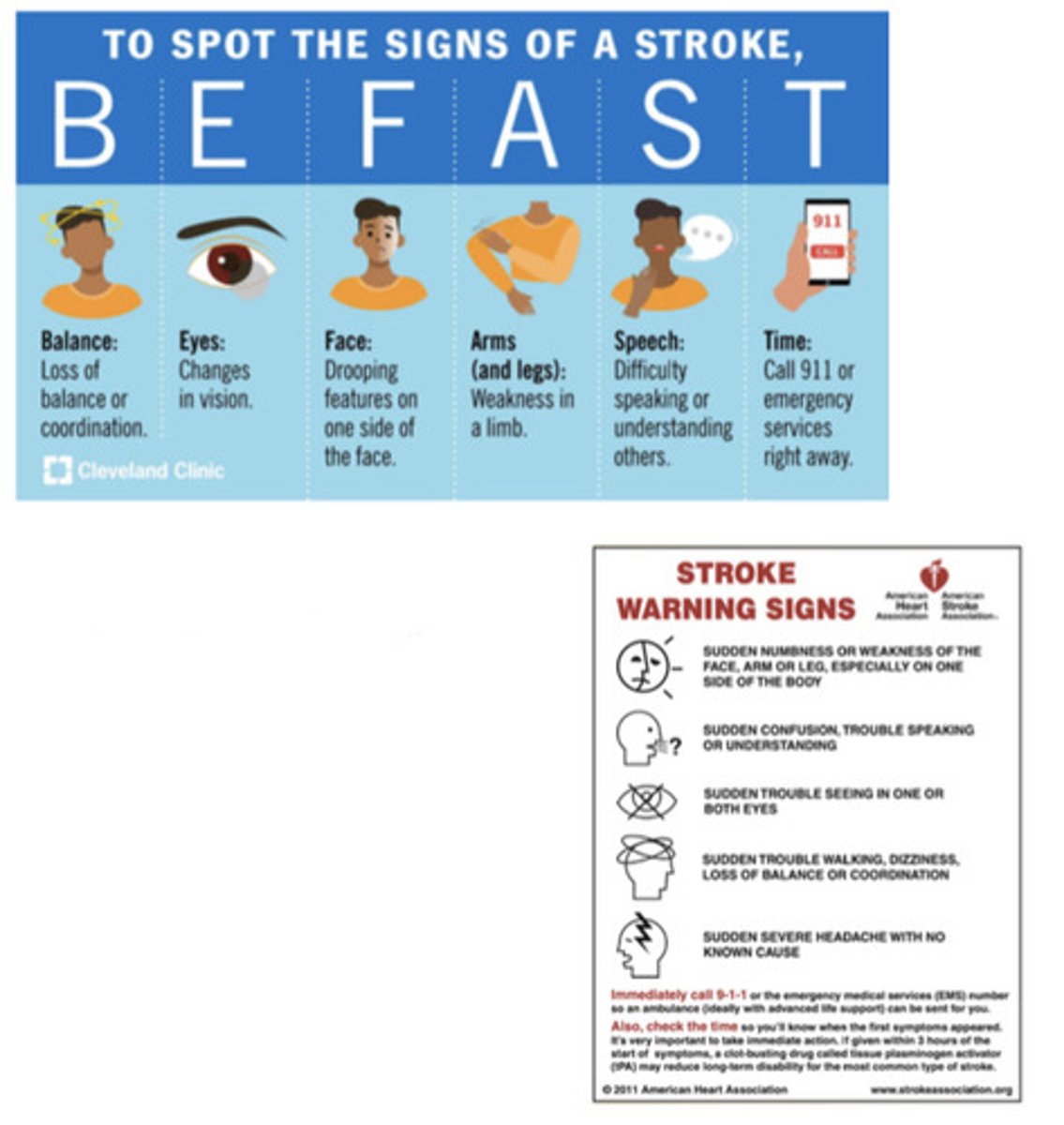
Understand general knowledge concerning CVA, including signs and symptoms, and emergency intervention.
-there are 2 main mechanisms of stroke
o ischemic: result of a thrombus, embolism or low systemic perfusion
o hemorrhagic: abnormal bleeding into the brain
-s/s
o sudden severe headaches
o sudden weakness of the face, arm or leg, especially ONE SIDED
o loss of speech
o changes in vision
o unexplained balance and coordination issues
-specific to women
o sudden hiccups that won't go away
o N/V
o SOB
o hallucinations
IF SUSPECTED, CALL 911 OR TAKE PT TO ER IMMEDIATELY!!
How does a TIA relate to a CVA?
TIA: temporary interruption of blood flow to the brain; symptoms usually resolve within minutes to hours (typically <24 hours)
CVA (stroke): a prolonged interruption of blood flow that causes permanent brain damage
What is an aneurysm? How could an abdominal aortic aneurysm be screened?
aneurysm: a localized bulge or ballooning in the wall of a blood vessel, usually caused by a weakness in the vessel wall
-to screen for triple A>> pt lays supine and the examiner attempts to feel for a widened, pulsatile aorta; the further away from umbilicus, the fainter the pulse should feel; if pulse still feels strong, a AAA should be suspected
Be familiar with the basic structure and function of the lymphatic system.
functions
1) immune defense: part of our surveillance system; once inside the lymph nodes, our WBC, lymphocytes, and macrophages work to destroy pathogens
2) fat transportation in GI
3) transport and draining of excess fluids, proteins, and cellular debris: cellular debris can be pain provoking, making movement and breathing very important to promote good functioning of the lymphatic system
4) "sanitation system" of the body to get rid of junk
structure
-return interstitial fluid to the circulatory system (this close relationship means that if there is an issue with the venous system there will be complications with the lymphatic system)
-the lymphatic system includes: lymph vessels, lymph fluid, and lymph tissues and organs (lymph nodes, tonsils, spleen, thymus, thoracic duct)
*fluid flows one way into capillary by way of a pressure gradient
*right lymphatic duct: drains the R side of the head, neck, and entire UE-->flows out of the subclavian veins--> drains head, neck, UE
*thoracic duct: largest lymph vessel, drains the rest of the body-->flow out of the subclavian veins-->drains rest of body
*thymus produces T-cells or T-lymphocytes
*spleen recycles RBC and helps with immunity
-both the R lymphatic duct and the thoracic duct flow in R/L subclavian veins= this is why issues with venous system creates issues with lymphatic system
How would you describe normal lymph nodes?
normal
-less than 1.5 cm
-non palpable
-soft, squishy
-not tender to touch
-mobile
abnormal
-enlarged
-hard or fixed (non-mobile) and matted
-significant difference between left and right
-red, warm, painful, tender
What is Filariasis?
transmitted by mosquitoes: nematode worm larvae live a full life cycle in the lymphatic system, causing inflammation and blocked lymphatic vessels; Stage 3 (elephantitis) is commonly linked to filariasis
-tropical and subtropic areas of the world
-non surgical cause of lymphedema
Be familiar with the prevention and treatment of lymphedema.
caused by:
-disturbance of the water and protein balance across the capillary membrane
o increased concentration of proteins draws greater amount of water into interstitial spaces
o exceeds transport capacity of the lymphatic system, leading to lymphedema
o excessive and persistent accumulation of extravascular and extracellular fluid and proteins in tissue spaces
prevention
-should be a PRIORITY of pt management
precautions/risks
-no pricks on the affected side (needles)
-caution when heavy lifting
-cutting of skin
-burning skin
-no BP cuff on lymphedema arm
tx
-manual lymphatic drainage: PROXIMAL congestion in the trunk, groin, butt, or axilla is cleared FIRST
What are the causes of lymphedema?
1) congenital malformation*
2) infection and inflammation**
3) obstruction or fibrosis**: trauma, surgery, neoplasms, radiation therapy
4) surgical dissection of lymph nodes** (very common after cancer surgery)
5) chronic venous insufficiency**: veins in the legs have difficulty returning blood to the heart, leading to pooling of blood in the LEs
6) obesity** (can be 2nd cause of lymphedema)
*primary lymphedema: congenital or hereditary
**secondary lymphedema: injury to one or more components of the lymphatic system (blocked, dissected, fibrosed, or otherwise damaged/altered)
What are the clinical signs and symptoms of lymphedema?
-decreased ROM, flexibility, and function
-usually unilateral (think of their dominant side)
o unless bilateral= ex. double mastectomy; have to be aware of hand dominance bc of swelling (take BP on leg)
-worse after prolonged dependency: work situation that forces them to stand for long periods of time
o prolonged dependency refers to a position where the affected limb is kept hanging down for an extended period, leading to fluid pooling
-edema usually not relieving by elevation
-numbness and tingling
-fibrotic changes to dermis (orange peel skin)
-no discomfort or a dull, heavy sensation; sense of fullness or skin tightness
*scrotal lymphedema is possible for men!
What are some possible unique findings that can be found during tests and measures for lymphedema?
-Stemmer's sign, skin texture changes, skin folds, fibrosis, increase in girth, papules, lymph leakage, and elephantiasis
-lymphoscintigraphy is a noninvasive special test using radioactive tracers and a gamma camera to show where the tracer has been absorbed by the lymphatic system
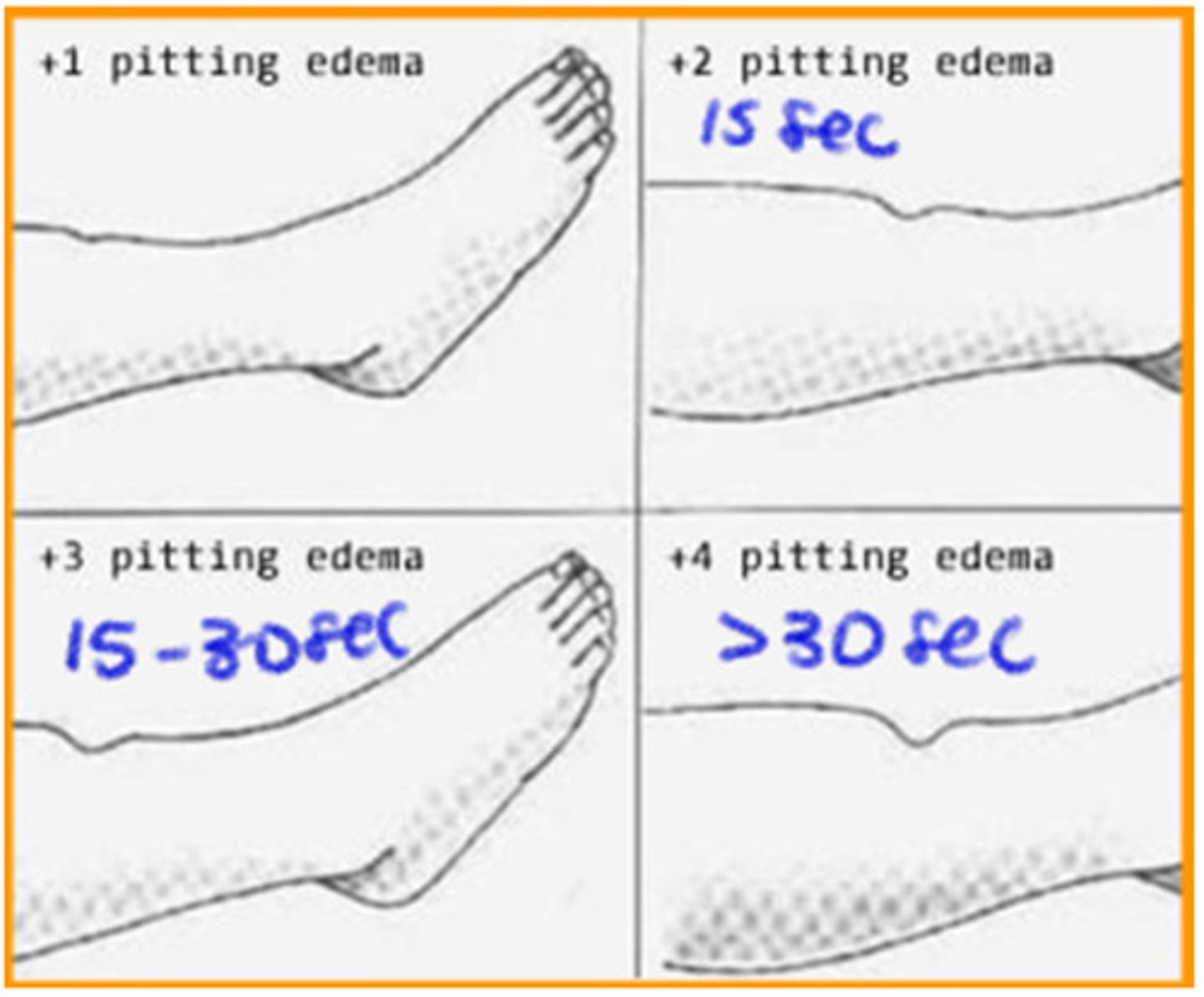
What are the different stages of lymphedema?
-stage 0 latency: edema free; tissue looks normal; transport capacity impaired
-stage 1 reversible stage: small fibrotic changes; pitting edema that resolves with elevation
-stage 2 irreversible stage: brawny, hard swelling, non pitting edema that does NOT reverse with elevation
-stage 3 lymphostatic elephantiasis:
o extensive amount of lymphedema and fibrosis along with abnormal skin changes such as papillomas & deep skin fold
o (+) stemmer sign
What are the different types of lymphedema?
helps determine severity along with asymmetry in the limbs
-pitting edema: short duration edema (can be timed to see how long it takes to go back to normal)= finger indentation of the skin
-brawny edema: tissue feels hard upon palpation, indicates fibrotic changes
-weeping: fluid leaks, wound healing is impaired; occurs mostly in the LE
What is Axillary Web Syndrome and how would this condition be treated?
-it is characterized by painful, tight, and rope-like cords that develop in the axilla (armpit) and UE
-cording of the lymphatic tissue
-common after breast cancer surgery
-can be cosmetically displeasing
-s/s: pain radiating down arm and decreased ROM with shoulder ABD and elbow extension
-tx: gentle stretching & soft tissue release of the lymphatic cord
How should a physical therapist respond if a patient has suspected lymphangitis?
acute inflammation of the subcutaneous lymphatic channels
-commonly the result of a bacterial infection (usually cellulitis: swollen, hot, red) from an abrasion or local trauma
-red streak under the skin radiating from the infection site in the direction of the regional lymph nodes
-fever, chills, malaise, anorexia, pain, slow healing wound, swollen lymph nodes, discomfort (SYSTEMIC MANIFESTATIONS)
In what order should exercises be performed in a patient with UE lymphedema?
1) diaphragmatic breathing is performed prior to lymphatic drainage exercises
2) trunk, pelvic, hip, and cervical exercises= proximal comprtments first to open channels!
3) proximal to distal from shoulders to fingers (in LE, hips to toes)
-exercises should follow a particular sequence to assist lymph flow
-should be performed with compressibe bandages or garment
o warm up: deep breathing, cervical motions, shoulder shrugs, knee to chest (inguinal's firing), crunches (abdominals firing)
-use dowels
-low intensity cardiopulm endurance activities
What signs and symptoms are associated with excessive exercise and reason to stop?
increased swelling during or right after exercise, pain, pins and needles, fatigue, shortness of breath or dizziness= STOP! check vital signs!
-remember to always take measurements
-if pt is not ready to progress, it might increase girth
What type of bandages are used for lymphedema compression?
non-stretch, non-elastic or low-stretch elastic bandages (short stretch)
-sports bandages, such as ACE wraps, are NOT recommended
-use bandages until you get the limb to a definitive size (meaning it is not changing anymore)
-after you get to the definitive size, you order compression garments
o Lymphedema Treatment Act: Medicare covers cost for prescribed lymphedema compression supplies
-use of a sequential, pneumatic compression pump on a daily basis may be recommended; they are more efficient when the arm is elevated
bandages
-worn for 23 hours a day, so they must be comfortable
-short stretch
o appropriate for lymphedema
o low resting pressure: when the muscles are at rest, the bandage does not exert much pressure (comfortable to wear for extended period)
o high working pressure: when the muscles contract, the bandage provides strong resistance (more tolerable for the pt during activity)
-long stretch (ACE wraps)
o not for lymphedema
o high resting pressure (tight at rest)

What type of pressure is used during manual lymph drainage?
-slow, very light, repetitive stroking bc lymph nodes are superficial
-go proximal to distal (trunk, groin, axilla, buttock) CLEARED FIRST
-direction is towards specific lymph nodes--> lymphedema increases risk of skin breakdown, infection, and delayed wound healing; protect and inspect the skin!
Case Study: A patient has been receiving physical therapy for lymphedema in her left arm. Following a treatment session, which included exercise, the patient reports that her arm felt achy and was throbbing. She also stated that she felt very fatigued and had to rest for an extended period following her treatment session. Upon girth measurements, the therapist notes slightly increased edema compared to the last session. How should the therapist respond to this situation?
1) stop any further exercise and allow the pt to rest
2) assess for signs of complications, such as infection (redness, warmth, fever)
3) elevate the arm to encourage lymphatic drainage and reduce swelling
4) apply gentle manual lymphatic drainage (MILD) to promote fluid movement (proximal to distal)
Describe medical tests related to pulmonary diagnosis. For example, what is flexible bronchoscopy?
-medical procedure to look inside the lungs and airways and uses a flexible fiber optic tube (a bronchoscope, it's a camera that goes down)
o it's both diagnostic (taking biopsies) and therapeutic (removing mucus plugs, suctioning secretions--> think of cystic fibrosis pts)
-it the pt is on a ventilator: bronchoscope is inserted through the endotracheal or tracheostomy tube (already in place to help with breathing)
-if the pt is breathing on their own: local anesthetic is sprayed with light sedation through an IV; the bronchoscope is guided through the nose
o rigid bronchoscope: more invasive, surgical version used in the OR
What is CT-PA?
-special type of CT scan that uses contrast to get a clear image of the pulmonary arteries (computed tomographic pulmonary angiography)
o it is the preferred test to detect blood clots in these arteries and diagnose acute pulmonary embolism (PE)
-CT-PA is PREFERRED bc it is widely available, delivers quick results, high sensitivity (it's good at detecting even small clots), non-invasive (uses IV contrast, no sx)
What is ventilation-perfusion scan?
-diagnostic imaging test used to assess pulmonary function and rule out conditions like pulmonary embolism (PE) or other respiratory abnormalities
o used to evaluate lung health in preoperative and postoperative lung transplant pts
-ventilation scan: inhalation of inert of radioactive gases and aerosols (air getting INTO alveoli)
-perfusion scan: sensitive to reduced or absent blood flow (blood REACHING the alveoli)
o conditions associated with perfusion defects: pulmonary embolism (PE= high V/Q= deadspace), asthma, emphysema, alveolar filling lesions, destructive or space-occupying lesions in the lungs, hypoventilation
Understand lung volumes and capacities.
key lung volumes
-tidal volume (TV): the amount of air inhaled or exhaled during normal resting ventilation
-inspiratory reserve volume (IRV): the additional air that can be inhaled
-expiratory reserve volume (ERV): the additional air that can be exhaled
-residual volume (RV): air remaining in the lungs after maximal exhalation
key lung capacities
-vital capacity (VC)= TV + IRV + ERV
o total volume of air under volitional control (volitional means something is done on purpose or by choice)
o max amount of air that can be exhaled after a max inhalation
-total lung capacity (TLC)= TV + IRV + ERV + RV
o total volume of air in the lungs after max inhalation
-functional residual capacity (FRC)= ERV + RV
o volume of air remaining in the lungs after resting expiration
-inspiratory capacity (IC)= TV + IRV
o max amount of air that can be inhaled after resting expiration
Be able to identify comparisons between normal, obstructive, and restrictive conditions.
obstructive pulmonary disease
-difficulty exhaling air
-cause: increased airway resistance, narrowing, or blockage
-examples: COPD, asthma
-symptoms: wheezing, SOB, prolonged exhalation
restrictive pulmonary disease
-difficulty inhaling
-causes: decreased chest wall compliance or increased lung stiffness
-example: pulmonary fibrosis
-symptoms: shallow breathing, increased breathing effort
Which position causes decreased vital capacity?
supine position due to reduced diaphragmatic movement and lung expansion (compared to sitting or standing)
How does COPD impact residual volume?
-air trapping and difficulty fully exhaling (COPD, asthma, emphysema)
-this contributes to hyperinflation, making breathing less efficient
What does FEV1 indicate? What is a normal value?
-forced expiratory volume in 1 second (FEV1): the amount of air forcefully exhaled in the first second of a forced vital capacity (FVC) maneuver
-normal FEV1 value: >70%