C1: Somatosensory
5.0(1)
Studied by 2 peopleCard Sorting
1/90
Earn XP
Description and Tags
Last updated 1:49 AM on 12/7/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
1
New cards
function of the sensory system is to provide information to the CNS about
external world (sound, light, smell, shape)
internal environment (pain, hunger O2, temperature, receptors)
position of body in space (determine where your limbs are when eyes are closed)
internal environment (pain, hunger O2, temperature, receptors)
position of body in space (determine where your limbs are when eyes are closed)
2
New cards
translation of information from the environment is the function of the ...
receptor organs (gated channel)
when the proper stimulus arises, channels open, depolarize the membrane to reach action potential
when the proper stimulus arises, channels open, depolarize the membrane to reach action potential
3
New cards
function of receptor organs (PNS)
convert mechanical, photic, chemical, and other forms of energy into action potentials (a form of information that can be used by the nervous system)
4
New cards
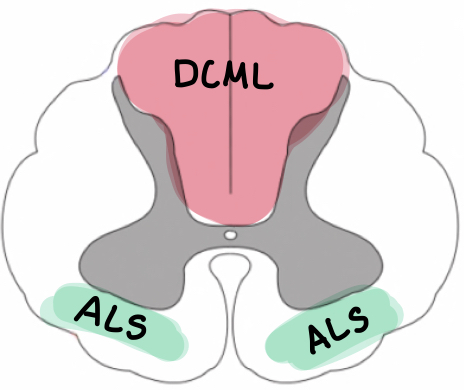
what does DCML stand for?
dorsal column medial lemniscus
5
New cards
what does ALS stand for?
anterolateral system (spinothalamic)
6
New cards
four somatic modailities
1. touch
2. proprioception
3. pain
4. thermal
2. proprioception
3. pain
4. thermal
7
New cards
what somatic modalities have encapsulated disk receptors?
1. touch
2. proprioception
mechanoreceptors (hair follicles)
2. proprioception
mechanoreceptors (hair follicles)
8
New cards
what somatic modalities have free/bare nerve ending receptors?
1. temperature
2. pain
2. pain
9
New cards
T/F distribution of receptors varies in different portions of the body
TRUE
areas are more sensitive than others (fingers vs. toes)
areas are more sensitive than others (fingers vs. toes)
10
New cards
What do Ruffini's endings (corpuscles) respond to? What kind of nerve ending?
pressure
encapsulated
encapsulated
11
New cards
What do Pacinian corpuscles respond to? What kind of nerve ending?
pressure
encapsulated
encapsulated
12
New cards
What do krause's end bulbs respond to? What kind of nerve ending?
pressure
encapsulated
encapsulated
13
New cards
What do meissner's corpuscles respond to? What kind of nerve ending?
light touch
encapsulated
encapsulated
14
New cards
What do merkel disks respond to? What kind of nerve ending?
fine touch
encapsulated
encapsulated
15
New cards
What do root hair plexus respond to? What kind of nerve ending?
fine touch
encapsulated
encapsulated
16
New cards
touch is elicited by...
mechanical stimulation of body surface
encapsulated disk
encapsulated disk
17
New cards
proprioception is elicited by...
mechanical displacements of the muscles and joints
encapsulated disks
encapsulated disks
18
New cards
pain is elicited by...
noxious (tissue damaging) stimuli
free nerve endings
free nerve endings
19
New cards
thermal is elicited by...
cool and warm stimuli
free nerve endings
free nerve endings
20
New cards
transduction
converting environmental changes to action potentials
21
New cards
somatosensory receptors are specialized parts of a...
first order neuron
22
New cards
frequency coding
temporal summation
stimulus is proportional to frequency of AP (how things are perceived)
firing 100x/sec would cause more pain than firing 10x/sec
stimulus is proportional to frequency of AP (how things are perceived)
firing 100x/sec would cause more pain than firing 10x/sec
23
New cards
population coding
spatial summation
number of receptors increase the stimulus
pain signaled by 1000 receptors would cause more pain than if signaled by 5 receptors
number of receptors increase the stimulus
pain signaled by 1000 receptors would cause more pain than if signaled by 5 receptors
24
New cards
rapidly adapting receptors
phasic
respond to CHANGING stimuli - doesn't matter if it's at, above or below baseline, only respond when it's changing
provide information about rapid changes
respond to CHANGING stimuli - doesn't matter if it's at, above or below baseline, only respond when it's changing
provide information about rapid changes
25
New cards
slowly adapting receptors
tonic receptors
sustained stimuli = sustained AP
any difference from baseline
sustained stimuli = sustained AP
any difference from baseline
26
New cards
examples of tonic receptors
nociceptors and proprioceptors
muscle spindles
muscle spindles
27
New cards
examples of phasic receptors
receptors for pressure, touch, and smell
28
New cards
parallel organization
multiple paths that information can take getting to the brain
if there is a lesion in the main pathway, it can take a parallel pathway that will be less precise
if there is a lesion in the main pathway, it can take a parallel pathway that will be less precise
29
New cards
hierarchal organizaiton
information transmitted sequentially via several order of neurons
processed at each relay nuclei
as information is processed, it is narrowed down to focus
processed at each relay nuclei
as information is processed, it is narrowed down to focus
30
New cards
first order neuron
1. remain ipsilateral
2. peripheral branches as their receptor organ (bare nerve or encapsulated disk)
3. cell body to dorsal root ganglion (psuedounipolar)
2. peripheral branches as their receptor organ (bare nerve or encapsulated disk)
3. cell body to dorsal root ganglion (psuedounipolar)
31
New cards
dermatome
Area of skin supplied by a single dorsal root (1st order neuron)
32
New cards
second order neuron
1. cell bodies in dorsal horn (ALS) or relay nuclei of medulla (DCML cuneate or gracile nuclei)
2. CROSSES THE MIDLINE
3. terminate in specific thalamic nuclei
2. CROSSES THE MIDLINE
3. terminate in specific thalamic nuclei
33
New cards
third order neuron
cell bodies in thalamus
axon project to S1, from the CONTRALATERAL side
2 cell bodies:
ventroposterior lateral (VPL)
ventroposterior medial nucleus of thalamus
axon project to S1, from the CONTRALATERAL side
2 cell bodies:
ventroposterior lateral (VPL)
ventroposterior medial nucleus of thalamus
34
New cards
Termination of 2nd order from the VPL come from where?
trunk and extremities
35
New cards
Termination of 2nd order from the VPM come from where?
face
36
New cards
primary somatosensory cortex is located
post central gyrus of the parietal lobe
37
New cards
primary somatosensory cortex is concerned with?
discriminative aspects of reception and appreciation of somatic sensory impulses
38
New cards
organization of primary somatosensory cortex medial - lateral
leg
trunk
arms
face
teeth
tongue
esophagus
trunk
arms
face
teeth
tongue
esophagus
39
New cards
distortion of sizes and representation on the primary somatosensory cortex reflects?
difference in innervation density in different areas of the body
areas most sensitive to touch have the largest respresentation
areas most sensitive to touch have the largest respresentation
40
New cards
disturbances within the somatosensory system can be localized clinically because of the direct relationship between ...
anatomical organization of the brain and specific perceptual and motor function
41
New cards
representation of the body map is _______________
use dependent corticoplasticity
42
New cards
can the shape/size of the representation of a particular body part be modified?
yes!
in response to peripheral injury, training, etc.
in response to peripheral injury, training, etc.
43
New cards
direct pathways
precise information flows directly from periphery --> CNS
44
New cards
what are the two direct pathways?
dorsal column medial lemniscus pathway (encapsulated) = DCML
anterolateral pathway (spinothalamic, bare nerve) = ALS
anterolateral pathway (spinothalamic, bare nerve) = ALS
45
New cards
what information does the DCML carry?
fine touch
sensory
conscious proprioception
position in space
vibration
sensory
conscious proprioception
position in space
vibration
46
New cards
what information does the ALS system carry?
pain and temperature = bare nerve endings
47
New cards
indirect pathways
less direct, longer, less precise
NOT HELPFUL CLINICALLY
NOT HELPFUL CLINICALLY
48
New cards
stereognosis
highly discriminative tactile sensation
ability to recognize object only by touch
ability to recognize object only by touch
49
New cards
what sensations are carried in the DCML pathway AND in parallel pathways?
vibration
static tactile discrimination
conscious proprioception
static tactile discrimination
conscious proprioception
50
New cards
describe the path of the DCML
1st order: come from extremities, enter through dorsal column, travel up through spinal cord, and synapse at gracile (lower) and cuneate (upper) nucleus
2nd order: cross over in internal arcuate fibers and up through CONTRALATERAL medial lemnsicus to synapse in the VPL (trunk/extremities) or VPM (face)
3rd order: go from VPL or VPM to corresponding area in the somatosensory cortex
2nd order: cross over in internal arcuate fibers and up through CONTRALATERAL medial lemnsicus to synapse in the VPL (trunk/extremities) or VPM (face)
3rd order: go from VPL or VPM to corresponding area in the somatosensory cortex
51
New cards
Draw the path of 1, 2, and 3 order neurons in the DCML pathway
do it
52
New cards
DCML is carried in what column
dorsal
53
New cards
where do the fibers of the DCML cross over?
internal arcuate fibers in the medulla oblongata
54
New cards
Where do 2nd order neurons in the DCML pathway synapse if its from the trunk/extremity?
ventral posterolateral nucleus of thalamus (VPL)
55
New cards
DCML first order neurons from the UPPER extremities travel through the spinal cord in the ____ to synapse at the ____
CUNEATE fasciculus
CUNEATE nucleus
CUNEATE nucleus
56
New cards
DCML first order neurons from the LOWER extremities travel through the spinal cord in the ___ to synapse at the ___
GRACILE fasciculus
GRACILE nucleus
GRACILE nucleus
57
New cards
what are the receptors for the ALS system?
free nerve endings
58
New cards
ALS pathways ascend in the...
spinothalamic tract
59
New cards
T/F the pathways for the ALS system are segregated and do not run together
TRUE!
60
New cards
how would you test loss of function from the ALS system?
response to pin prick
thermal discrimination
thermal discrimination
61
New cards
describe the path of the ALS
1st order: come from extremities and synapse in the dorsal root ganglion (lamina II), remain IPSILATERAL
2nd order: enter spinal cord and immediately cross over and ascend through the lateral spinothalamic tract to the thalamus (do not go thru gracile or cuneate) (CONTRALATERAL)
3rd order: go from thalamus to corresponding area in the somatosensory cortex
2nd order: enter spinal cord and immediately cross over and ascend through the lateral spinothalamic tract to the thalamus (do not go thru gracile or cuneate) (CONTRALATERAL)
3rd order: go from thalamus to corresponding area in the somatosensory cortex
62
New cards
pain and temperature sensations from the face and cranium are carried by
trigeminal system
63
New cards
second important function of the ALS
parallel channel for transmission of tactile information, including simple touch and static-discriminative modalities
64
New cards
paresethesia
abnormal sensations, numbness, tingling
65
New cards
CLINICAL CASE:
abrupt onset of pain followed by paresthesia
and loss of feeling in a rather circumscribed area along the lateral aspect of his left thigh.
a localized area of decreased perception of pinprick (pain), temperature, and touch, confined to this limited area. Results of the remainder of the examination were normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
abrupt onset of pain followed by paresthesia
and loss of feeling in a rather circumscribed area along the lateral aspect of his left thigh.
a localized area of decreased perception of pinprick (pain), temperature, and touch, confined to this limited area. Results of the remainder of the examination were normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
peripheral lesion
left side of body
ALS and DCML pathways
1st order
left side of body
ALS and DCML pathways
1st order
66
New cards
how would you know if a lesion is in the periphery?
the area affected is very localized and does not spread to other parts of the body
67
New cards
The distal axons of the peripheral sensory neurons mediating all types of afferent input are ______ in peripheral nerves
intermingled
68
New cards
A lesion that affects peripheral nerves would be expected to produce a variable sensory loss for?
all modalities
since motor axons (efferents) are also contained in the same peripheral nerves, weakness and a loss of muscle stretch related reflexes would also be noted.
since motor axons (efferents) are also contained in the same peripheral nerves, weakness and a loss of muscle stretch related reflexes would also be noted.
69
New cards
CLINICAL CASE:
progressive loss of sensation in an area involving the shoulders and both upper extremities.
limited sensory loss involving only pain and temperature in this area.
no changes in motor performance, strength, or deep tendon reflexes.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
progressive loss of sensation in an area involving the shoulders and both upper extremities.
limited sensory loss involving only pain and temperature in this area.
no changes in motor performance, strength, or deep tendon reflexes.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
1. central spinal cord where 2nd order from UE crossover so pathways from all other parts of body are intact
2. bilateral
3. ALS pathways (since DCML pathways would still be intact) - COMMISSURAL SYNDROME
4. 2nd order
2. bilateral
3. ALS pathways (since DCML pathways would still be intact) - COMMISSURAL SYNDROME
4. 2nd order
70
New cards
Syringomyelia
abnormal longitudinal cavities in the spinal cord cause paresthesias and muscle weakness
71
New cards
commissural syndrome
bilateral pain/temp loss at LEVEL of lesion
specific type of segmental deficit that can result from a lesion involving the central regions of the spinal cord, usually over several segments
interruption of the second-order neurons as they decussate to form the spinothalamic tracts. As the lesion enlarges, other adjacent tracts become involved.
specific type of segmental deficit that can result from a lesion involving the central regions of the spinal cord, usually over several segments
interruption of the second-order neurons as they decussate to form the spinothalamic tracts. As the lesion enlarges, other adjacent tracts become involved.
72
New cards
CLINICAL CASE:
knife wound to the back.
weakness of the lower extremity
loss of pain and temperature perception on the right side from about the level of his navel downward
Vibration, joint-position sense, and discriminatory function (fine touch) are reduced in the left leg.
Touch (crude) was normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
knife wound to the back.
weakness of the lower extremity
loss of pain and temperature perception on the right side from about the level of his navel downward
Vibration, joint-position sense, and discriminatory function (fine touch) are reduced in the left leg.
Touch (crude) was normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
1. spinal cord (after ALS crosses over and before DCML crosses over)
2. left side of body
3. ALS & DCML --> BROWN SEQUARD SYNDROME
4. 1st of DCML; 2nd of ALS
2. left side of body
3. ALS & DCML --> BROWN SEQUARD SYNDROME
4. 1st of DCML; 2nd of ALS
73
New cards
brown-sequard's syndrome
a complete hemisection of the spinal cord
ipsilateral dorsal column deficit, ipsilateral motor deficit, and contralateral loss of pain and temperature senses.
Incomplete lesion stab wound
ipsilateral dorsal column deficit, ipsilateral motor deficit, and contralateral loss of pain and temperature senses.
Incomplete lesion stab wound
74
New cards
CLINICAL CASE:
complaining of a progressive difficulty in walking in the dark.
a decreased position sense in his arms and legs bilaterally, decreased vibratory sensation in both upper and lower extremities, and decreased ability to perceive discriminative tactile sensation bilaterally.
Pain and temperature sense were normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
complaining of a progressive difficulty in walking in the dark.
a decreased position sense in his arms and legs bilaterally, decreased vibratory sensation in both upper and lower extremities, and decreased ability to perceive discriminative tactile sensation bilaterally.
Pain and temperature sense were normal.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
1. spinal cord
2. bilateral
3. DCML
4. 1st order (projecting to both gracile and cuneate)
2. bilateral
3. DCML
4. 1st order (projecting to both gracile and cuneate)
75
New cards
what happens to the ALS and DCML pathways when there's a complete lesion in the dorsal columns
ALS = completely untouched
DCML = 1st order completely lost
DCML = 1st order completely lost
76
New cards
tabes dorsalis
Degeneration of dorsal columns and dorsal roots due to tertiary syphilis, resulting in impaired proprioception and locomotor ataxia.
Associated with charcot's joints, shooting (lightning pain) , Argyll Robertson pupils (Reactive to accommodation but not light), absence of DTRs, positive romberg, and sensory ataxia at night.
Associated with charcot's joints, shooting (lightning pain) , Argyll Robertson pupils (Reactive to accommodation but not light), absence of DTRs, positive romberg, and sensory ataxia at night.
77
New cards
lesions at the spinal level typically produce:
segmental sensory deficit
intersegmental sensory deficit
intersegmental sensory deficit
78
New cards
lesions at the spinal cord: segmental sensory deficit
sensory deficit limited to one level of the body and usually caused by involvement of the nerve roots or spinal nerves
79
New cards
lesions at the spinal cord: intersegmental sensory deficit
sensory deficit involving all the body below a specific level due to interruption of an ascending pathway
80
New cards
CASE STUDY:
hypertensive man awoke one morning noting that he was unable to feel anything over the entire left side of his body.
motor strength and reflexes were normal, as were the visual field
did not respond to pinprick, temperature, or touch over the left side of his face, trunk, and extremities
could not perceive joint motion or vibration in his left arm and leg.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
hypertensive man awoke one morning noting that he was unable to feel anything over the entire left side of his body.
motor strength and reflexes were normal, as were the visual field
did not respond to pinprick, temperature, or touch over the left side of his face, trunk, and extremities
could not perceive joint motion or vibration in his left arm and leg.
Level in NS?
Side of body?
Pathway(s) involved?
Wallerian Degeneration?
1. thalamus --> CNS
2. left side
3. DCML and ALS
4. 3rd order
** symptoms in the face indicate a brainstem lesion
2. left side
3. DCML and ALS
4. 3rd order
** symptoms in the face indicate a brainstem lesion
81
New cards
in a thalamic lesion, why can't it be a spinal cord or medial lemniscus lesion?
spinal cord = because the face is involved
medial lemniscus = no loss of motor strength
medial lemniscus = no loss of motor strength
82
New cards
lesions in the thalamus
lesion affecting a specific sensory nuclei of the thalamus causes a complete loss of all forms of general somatic afferent sensation in the contralateral face, trunk, and limbs.
83
New cards
lesions at the brainstem level
characterized by a contralateral loss of sensory function in the trunk and limbs because of interruption of the ascending pathways
84
New cards
lesions at the level of the medulla are often associated with
a sensory loss (usually pain and temperature) over the ipsilateral face because of segmental involvement of CN V (trigeminal) or its descending tract and nucleus
85
New cards
suprathalamic lesions
lesions that involve the thalamo-cortical projections or the cortex itself
associated with somatosensory deficits to the contralateral side of the body
are associated with only minimal involvement of pain, temperature, touch, and vibratory sensibility but a severe deficit in joint position sense, touch location, two-point discrimination, and stereognosis
associated with somatosensory deficits to the contralateral side of the body
are associated with only minimal involvement of pain, temperature, touch, and vibratory sensibility but a severe deficit in joint position sense, touch location, two-point discrimination, and stereognosis
86
New cards
intact thalamocortical pathways are needed for the full appreciation of ______ whereas the primary modalities of superficial sensation are perceived and integrated at the ____ level.
discriminative sensations
thalamic
thalamic
87
New cards
are you aware of a stimuli before it reaches the cortex?
yes
88
New cards
where are the branches of the first order neurons?
peripheral nervous system
89
New cards
at what order do DCML and ALS pathways cross the midline?
second order
90
New cards
third order neurons that synapse in the ventral posterlateral (VPL) complex of the thalamus come from
trunk and extremities
91
New cards
third order neurons that synapse in the ventral posteromedial (VPM) complex of the thalamus come from
the face