Looks like no one added any tags here yet for you.
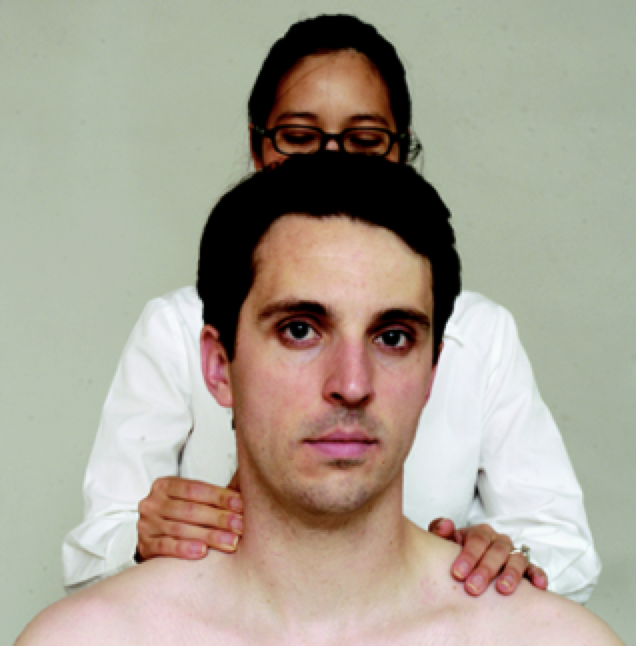
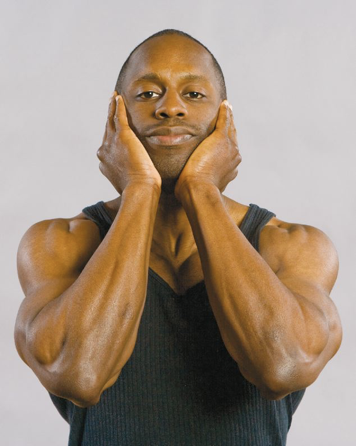
Brachial Plexus Compression Test
-Procedure: Patient is seated, apply firm compression to brachial plexus by squeezing plexus under the thumb or fingers
-Positive test if pain radiates into shoulder or upper extremity
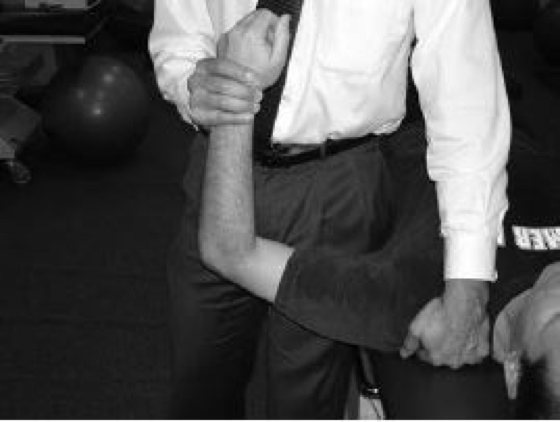
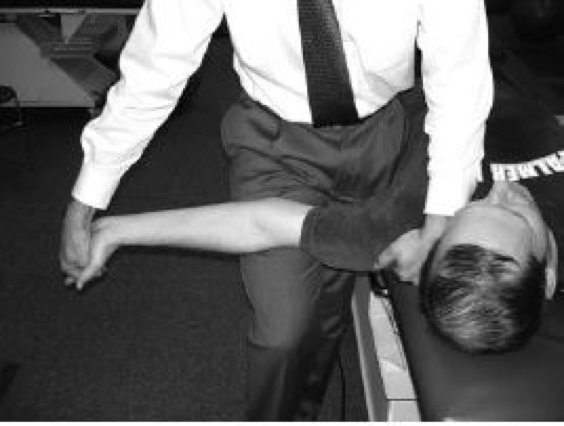
Brachial Plexus Provocation Test
-Procedure: Patient lies supine, examiner abducts the patients shoulder to 90 degrees with elbow flexed and wrist extended, examiner then extends elbow
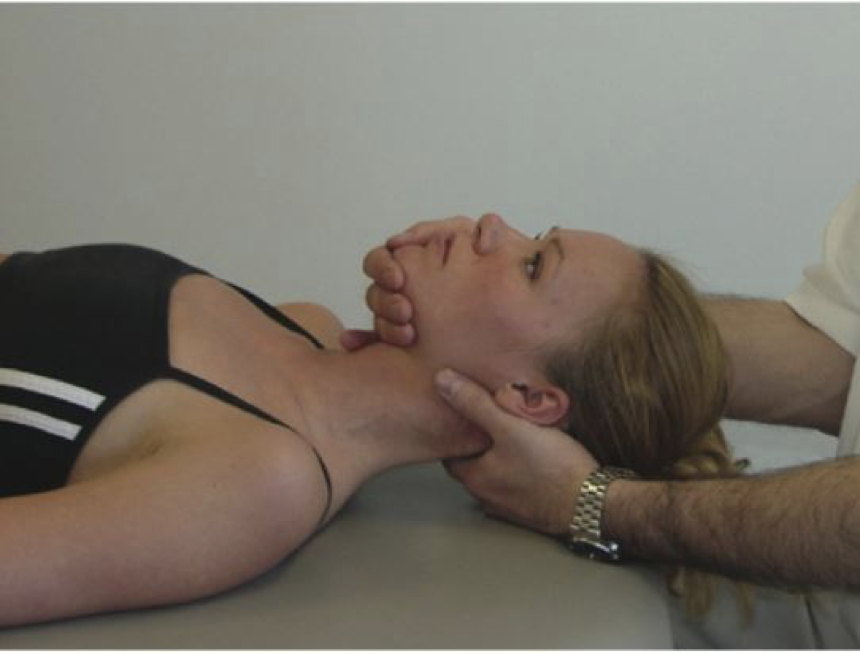
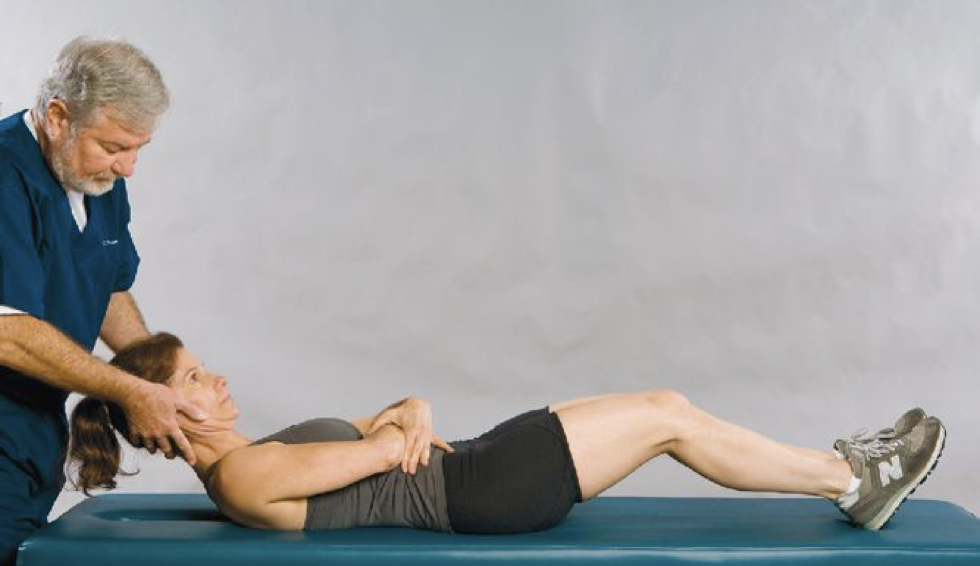
Cervical Distraction Test
-Assesses for cervical radiculopathy
-Procedure: Patient supine, examiner grasps patient under chin and occiput while slightly flexing patients neck while applying distraction force
-Positive if radicular symptoms are reduced
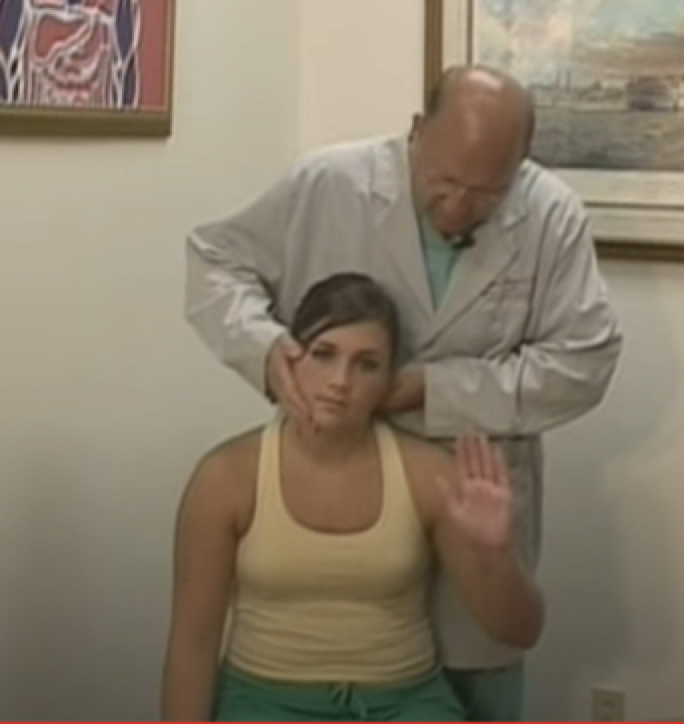
Cervical Compression Test
-Assessment for cervical radiculopathy
-Procedure: Patient seated with examiners standing behind patient, patient flexes head on uninvolved side to one side, examiner exerts pressure straight down on head
-Positive if familiar upper extremity pain is reproduced
Jackson’s Compression Test (AKA Spurling Test A)
-Provokes nerve root symptoms (Assesses for Cervical Radiculopathy)
-Procedure: Patient rotates head to uninvolved side first, examiner applies downward force to head, repeated on involved side
-Positive test if pain radiates into arm
Cervical Flexion-Rotation Test
-Assesses for Cervicogenic Headache
-Procedure: Patient Supine and the cervical spine passively maximally flexed. the examiner passively rotates head left and right
-Positive if patient reports onset of pain or if examiner encounters firm resistance at an estimated range of motion that is reduced by more than 10 degrees from normal of 44 degrees
Spurling Test B
-Assessment for Cervical Radiculopathy
-Procedure: Patient seated, the neck is passively placed in a combination of lateral bending, rotation and extension toward the symptomatic side and examiner applies pressure
-Positive if symptoms are reproduced
Bakody Sign (Shoulder Abduction Relief Test)
-Assessment for cervical nerve root compression
-Procedure: Patient seated and places the palm of the affected extremity on top of the head (this position decreases tension on the lower trunk of the brachial plexus, particularly C4-C6)
-Positive if radicular pain is decreased
Upper Limb Tension Test A (Come back to this)
-Assessment for Cervical Radiculopathy
-Procedure: Patient is supine, examiner preforms scapular depression, shoulder abduction to 90 degrees, forearm supination, wrist and finger extension, shoulder external rotaion
Libman’s Test
-Assessment of patients pain threshold
-Procedure: Apply gradual increasing pressure to the mastoid process
-Positive test is indicated by increased pain, patient will indicate to stop
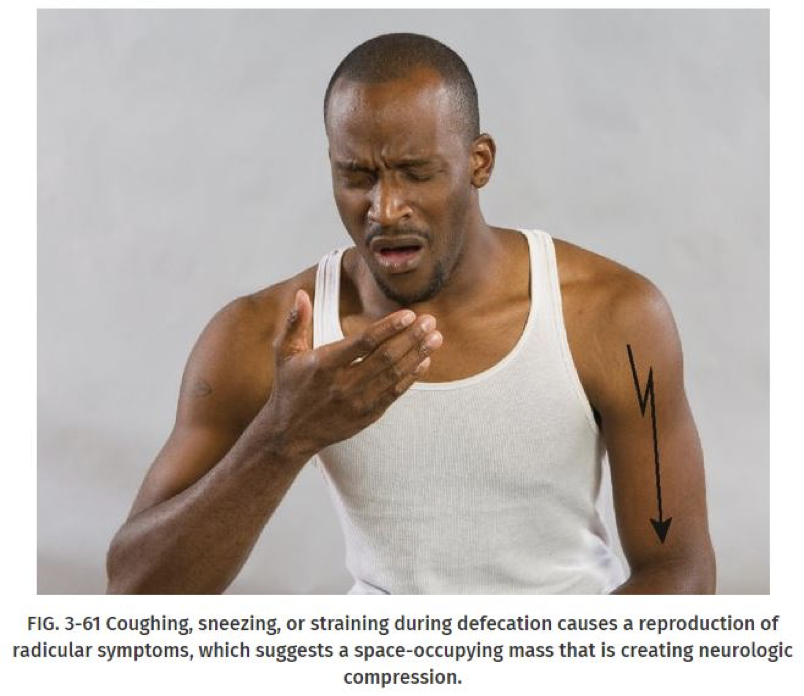
Dejerine’s Triad
-Assessment for Radicular symptoms caused by space occupying lesion
-Procedure: Coughing, sneezing, and straining during defecation may aggravate radiculitis symptoms
Valsalva Maneuver
-Assessment for Space-Occupying Lesion
-Procedure: Patient takes a deep breath and holds it while bearing down abdominally
-Positive test is indicated by increased pain caused by increased intrathecal pressure
Brudzinski Sign
-Assessment for meningeal irritation or inflammation
-Procedure: Patient is in supine position, and examiner passively flexes the patients head
-Positive if flexion of both knees occur
Kernig Sign
-Assessment for meningeal irritation or inflammation
-Procedure: Patient is supine, examiner flexes the patient’s hip and knee of either leg to 90 degrees, examiner attempts to completely extend the patient’s leg
-Positive if the maneuver causes pain, sign is present
O’Donoghue Maneuver
-For Differentiation between cervical strain vs sprain
-Procedure: Patient is seated with head in neutral position, patient attempts to Actively rotate head against the examiners resistance (checking for strain), Next examiner passively rotates head and reproduction of pain is suggestive of ligamentous sprain
Romberg Test
-Assessment for Dorsal Column Disorder (Proprioception)
-Procedure: Examiner asks patient to stand with feet together and arms by the sides with eye open, Next have patient close the eyes for atleast 20 seconds.
-Positive romberg if the patient sways or falls to one side when the eyes are closed (indicates intracranial lesion, posterior column problems, or proprioceptive problem)
Rust Sign
-Procedure: If the patient spontaneously grasps the head with both hands when standing, lying down or when arising from a recumbent position (this is a positive sign indicating severe sprain, RA, fracture, or severe upper cervical instability
Sharp-Purser Test
-Assessment for atlantoaxial instability
-Procedure: place one hand over the patient’s forehead while the thumb of the other hand is placed over the spinous process of the axis to stabilize it , Patient slowly flexes the head while doing this examiner presses backward on the forehead with the palm
-Positive test is indicated if the examiner feels the head slide backward during the movement
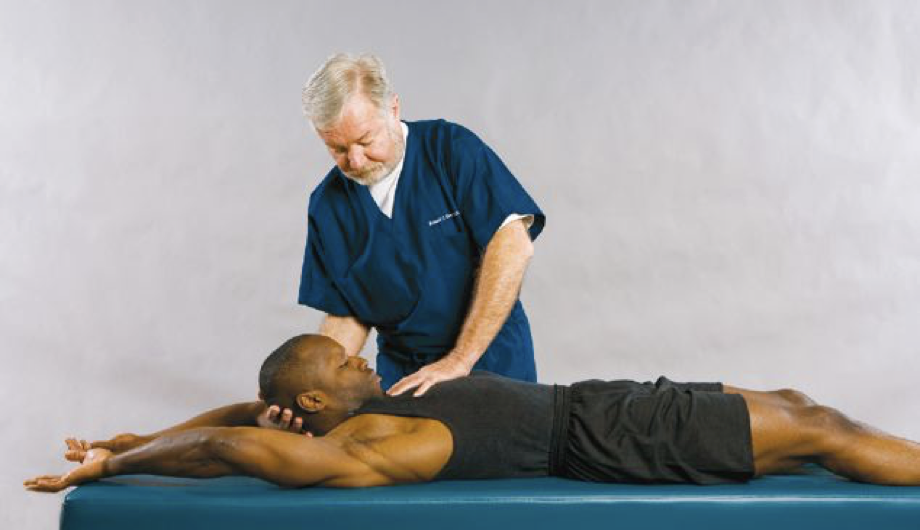
Soto-Hall Test
-Assessment for cervical spine exostoses, disc lesions, strain, sprain, fracture, or meningeal irritation (DO NOT PREFORM IF PATIENT HAS SUSPECTED C-SPINE FRACTURE)
-Procedure: Patient is supine with legs fully extended and arms extended over the head, doctor supports patients head with one hand while stabilizing the patient’s chest with other hand, head and neck are passively flexed
-Positive if pain is localized to cervicothoracic spine
Thoracic Outlet Syndrome Tests
-Adson Test
-Allen Maneuver
-Costoclavicular Maneuver
-Reverse Adson’s (Halstead Maneuver)
-Reverse Bakody Maneuver
-Roos Test (EAST test)
-Tinel’s Test
-Wright Test (Hyperabduction maneuver)
Adson Test
-Procedure: Patient is seated examiner locates the radial pulse, patient’s head is rotated to face the test shoulder, Patient extends the head while the examiner laterally rotates and extends the patient’s shoulder, patient takes deep breath and hold it
-Positive if pulse disappears
Allen Maneuver
-Procedure: Patient’s elbow is flexed 90 degrees, Shoulder is abducted and externally rotated, doctor palpates radial pulse and patient rotates the head away from the involved extremity
-Positive if pulse disappears when the head is rotated
Costoclavicular Maneuver
-Procedure: Doctor palpates radial pulse while the patient’s shoulders are drawn down and back, cervical spine is flexed maximally
-Positive test by obliteration of the pulse and implies possivle thoracic outlet syndrome
Costoclavicular Maneuver (alternative method)
Reverse Adson’s (Halstead Maneuver)
-Procedure: Doctor palpates the radial pulse and applies downward traction on the affected extremity while the patient’s neck is hyperextended and the head is rotated to the opposite side
-Absence or disappearance of a pulse indicates positive for TOS
Reverse Bakody Maneuver
-Procedure: Patient is seated and places the palm of affected extremity on top of the head (same as bakody sign)
-Positive when the radiating pain is elicited or worsened with this maneuver (cervical radicular compression if pain goes away)
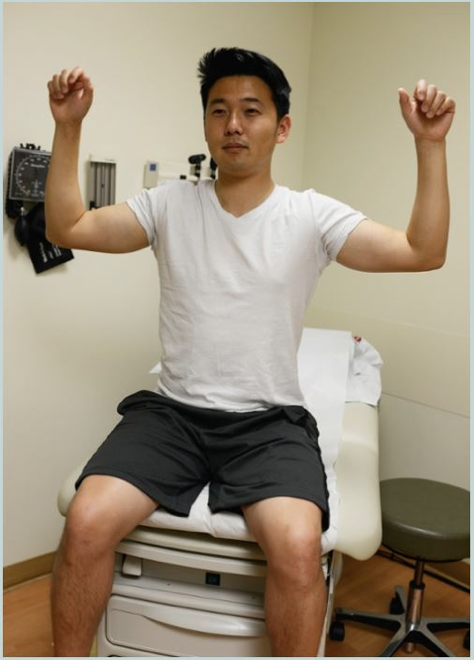
Roos Test (Elevated Arm Stress Test)
-Procedure: Patient holds arm at right angles and the forearm flexed to 90 degree, patient is instructed to open and close his fist at moderate speed for 3 minutes.
Tinel Test
Procedure: Lightly tapping over the nerve to elicit a sensation of tingling or ‘pins or needles’ in the distribution of the nerve
-Positive when tingling or prickling sensation painful paresthesias radiate into forearm or hand
Wright Test (Hyperabduction Maneuver)
-Procedure: Patient is seated with both arms hanging at the sides, doctor palpates radial pulse and passively abducts the arm to 180 degrees, Doctor notes angle of abduction at which the radial pulse diminishes or disappears on the affected side
-Positive if pulse is obliterated
Upper Limb Tension Test A
-Assessment for cervical radiculopathy
-Procedure: Patient is positioned sequentially through 6 positions
-Positive if paitents radicular symptoms are reproduced, the side-to-side difference in elbow extension is greater than 10 degrees, contralateral neck side bending increases symptoms, ipsilateral side bending decreases symptoms
Upper Limb tension Test A (Step 1)
-Scapular depression
Upper Limb tension Test A (Step 2)
-Shoulder abduction
Upper Limb tension Test A (Step 3)
Forearm Supnation
Upper Limb tension Test A (Step 4)
-Shoulder External Rotation
Upper Limb tension Test A (Step 5)
-Elbow extension
Upper Limb tension Test A (Step 6)
-Contralateral cervical side-bending
Upper Limb tension Test A (Step 7)
-Ipsilateral cervical side-bending
Extension Rotation Test
-Assesses Vertebrobasilar artery insufficiency
-Procedure: Patient is supine with head above edge of the table, doctor supports patients head then brings head into extension, hold for 30 seconds
-Positive test if any changes in speech or changes in eye movement
Vertebral Artery Test
-Assesses for vertebrobasilar artery insufficiency
-Procedure:
Part 1: Patient is supine with head maximally rotated to one side and have them count backward from 10,
Part 2: have patient turn head back to neutral position and position the patient to the edge of the table with head in extension and have patient count backward from 10
Part 3: Have patient return to neutral position with the head on the table then have patient extend and rotate the head and count backward from 10
-Positive test when any of the 5 D’s and 3N’s are present
Hautant Test
-Procedure: Patient is sitting and have arms straight out for 10-30 seconds while eyes are closed, patient then rotates and extends the neck with arms straight while eyes are still closed
-Test is positive when the upper extremities drift during rotation and extension of the neck
Barre-Lieou Test
-Procedure: Patient is sitting and asked to slowly rotate the head first to one side then the other.
Pronator Drift Test
-Procedure: Patient is standing with arms straight out and forearms supinated (Palms up), patient is asked to close their eyes and hold the position for 10-20 seconds
-Positive if 1 arm slowly drifts down and pronates (vascular dysfunction)
Underberg Test
-Procedure: Patient is standing with both upper extremities straight out with forearms supinated, patient closes their eyes and rotates and extends there head and marches in place for 10 seconds,
-Positive if 1 arm drops down, forearm pronates, or there is a loss of balance (Positive for vascular dysfunction)