Lecture 12: General Issues in Psychotherapy
1/79
Earn XP
Description and Tags
By Jordana Burstein for Clinical Psychology
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
80 Terms
Does Psychotherapy work is a question of _____ (Does Psychotherapy Work?)
vital importance
What form did most evidence take in the mid-1900s regarding psychotherapy? (Does Psychotherapy Work?)
Most evidence was in the form of anecdotes, testimonials, and case studies, which were subjective descriptions of individual clients' progress, typically written by therapists themselves.
When did controlled studies on psychotherapy start appearing regularly, and who was responsible? (Does Psychotherapy Work?)
Controlled studies began appearing regularly in the 1950s, and Hans Eysenck was responsible for one of the first landmark studies published in 1952.
He published study concluding that most clients got better without therapy and that psychotherapy was generally of little benefit.
How have Hans Eysenck's methods been received? (Does Psychotherapy Work?)
Eysenck's methods have been criticized and overturned, though his work inspired thousands of subsequent empirical studies on therapy outcomes.
When did meta-analyses begin to appear in psychotherapy research? (Does Psychotherapy Work?)
Meta-analyses began to appear in the late 1970s and 1980s.
What is meta-analysis? (Does Psychotherapy Work?)
Meta-analysis is a statistical method that combines the results of many separate studies—sometimes hundreds—to create numerical representations of the effects of psychotherapy across various settings, therapists, and clients.
What results have meta-analyses yielded regarding psychotherapy effectiveness? (Does Psychotherapy Work?)
Meta-analyses have consistently yielded supportive results, confirming that psychotherapy is effective, with the effects no longer being in doubt.
Whose opinion should researchers seek when evaluating the results of therapy, and why? (Whom Should Researchers Ask?)
Researchers should seek the opinions of multiple people involved in therapy—such as the client, therapist, and possibly others (e.g., family members)—because each person may have a different vantage point on the results of therapy.
Who is Hans Strupp? (Whom Should Researchers Ask?)
Hans Strupp is a legendary and pioneering psychotherapy researcher.
What did Hans Strupp identify in his research? (Whom Should Researchers Ask?)
Hans Strupp identified three parties that have a stake in how well therapy works, each of which may have different opinions about what constitutes a successful therapy outcome.
He called it the tripartite model.
What is the tripartite model, and what are the three viewpoints it acknowledges? (Whom Should Researchers Ask?)
The tripartite model acknowledges the viewpoints of three parties in therapy:
The client
The therapist
Third parties (e.g., society, family, or managed-care companies)
What is the first viewpoint in the tripartite model of therapy outcome evaluation? (Whom Should Researchers Ask?: client)
The first viewpoint is the client's perspective, as they are those whose lives affected by therapy, and improving their lives in a meaningful way is the focus of therapy.
Client’s opinions are _____, but could also be _____. (Whom Should Researchers Ask?: client)
valuable, biased
Do clients who are overly eager to see positive results overestimate or underestimate the benefits of therapy? (Whom Should Researchers Ask?: client)
Clients who are overly eager to see positive results, especially after investing time and money, tend to overestimate the benefits of therapy.
Do clients who are negatively influenced by the factors that brought them into therapy overestimate or underestimate the benefits of therapy? (Whom Should Researchers Ask?: client)
Clients who are negatively influenced by their initial issues, such as depression and distorted thinking, tend to underestimate the benefits of therapy.
What is the second viewpoint in the tripartite model of therapy outcome evaluation? (Whom Should Researchers Ask?: therapist)
The second viewpoint is the therapist's perspective, as they have more professional experience in mental health in comparison to the client, and can assess a client’s progress based on their expertise.
Why might therapists have more accurate expectations about therapy outcomes? (Whom Should Researchers Ask?: therapist)
Therapists typically have more experience in mental health than clients, allowing them to set realistic and informed expectations about progress and treatment effectiveness.
Therapists’ views can be _____ as well. (Whom Should Researchers Ask?: therapist)
biased
How can therapists' views on therapy outcomes be biased? (Whom Should Researchers Ask?: therapist)
Therapists' views can be biased because:
They only see a fraction of their clients’ lives.
They may feel that a client’s negative evaluation reflects poorly on their therapeutic skills or the client’s progress.
What is the third viewpoint in the tripartite model of therapy outcome evaluation? (Whom Should Researchers Ask?: society)
The third viewpoint is society’s perspective, representing outsiders who have an interest in how therapy progresses.
Who is included in the third-party viewpoint of the tripartite model? (Whom Should Researchers Ask?: society)
This includes:
The general public
The legal system
Clients’ family and friends
Clients’ employers
Managed-care companies that pay for therapy
What is the advantage of the third-party perspective in therapy evaluation? (Whom Should Researchers Ask?: society)
The third-party perspective tends to emphasize the client’s ability to function in a stable, predictable, and unproblematic way, providing an objective, functional view of therapy outcomes.
When should researchers ask if psychotherapy works? (When Should Researchers Ask?)
Timing of assessment is crucial, as the OBVIOUS answer would be that therapy benefits can be evaluated immediately after therapy ends. But really it could be at various points during therapy, or even long after therapy has concluded.
Why is immediately after therapy ends not the most obvious answer for evaluating its effectiveness? (When Should Researchers Ask?)
Because:
The duration of benefits varies—effects might last for months or years, or they might fade.
Improvement can occur before therapy ends, meaning benefits could be noticeable at different points throughout treatment rather than only at the end.
What are the two methods researchers use to ask if psychotherapy works? (How Should Researchers Ask?)
The two main methods are:
Self-report – Gathering opinions through questionnaires or interviews.
Behavioral measures – Directly observing a client’s behavior to assess changes.
What is self-report in psychotherapy research? (How Should Researchers Ask?)
Self-report is a method where researchers solicit opinions from an interested party (e.g., client, therapist, or third parties) using questionnaires or interviews to evaluate therapy outcomes.
What are behavioral measures in psychotherapy research? (How Should Researchers Ask?)
Behavioral measures involve directly observing a client’s actions in real-life settings (e.g., school, home) to assess behavioral changes, rather than relying on subjective reports.
ADHD treatment is an example: rather than asking the client, their therapist, their parents, or their teachers. Researchers could directly observe the boy at school or at home to determine whether their behavior has changed
How many categories do empirical studies of psychotherapy fall into, and what are they? (Efficacy Versus Effectiveness of Psychotherapy)
Empirical studies fall into two categories:
Efficacy – Measures therapy success in controlled settings.
Effectiveness – Measures therapy success in real-world clinical settings.
What is efficacy in psychotherapy research? (Efficacy Versus Effectiveness of Psychotherapy)
Efficacy is the success of a particular therapy in a controlled study, conducted with carefully selected clients who meet specific study criteria.
What do efficacy studies maximize, and how? (Efficacy Versus Effectiveness of Psychotherapy)
Efficacy studies maximize internal validity by controlling as many variables as possible to ensure accurate cause-and-effect conclusions.
What do efficacy studies typically feature? (Efficacy Versus Effectiveness of Psychotherapy)
Efficacy studies typically feature:
Well-defined groups of patients (meeting criteria for only one disorder).
Manualized treatment guidelines (to reduce therapist variability).
Random assignment to control and treatment groups.
What is effectiveness in psychotherapy research? (Efficacy Versus Effectiveness of Psychotherapy)
Effectiveness is the success of therapy in real-world (actual) clinical settings, where client problems are more diverse and not strictly controlled.
What do effectiveness studies measure? (Efficacy Versus Effectiveness of Psychotherapy)
Effectiveness studies measure the extent that therapy works in real-world conditions, such as clinics, hospitals, and private practices.
Methods better match therapy that actually takes places in clinics, private practices, hospitals, and other realistic settings.
What do effectiveness studies maximize? (Efficacy Versus Effectiveness of Psychotherapy)
Effectiveness studies maximize external validity, ensuring that their methods reflect real-life therapy conditions.
What do effectiveness studies typically feature? (Efficacy Versus Effectiveness of Psychotherapy)
Effectiveness studies typically feature:
A wider range of clients (often with complex diagnoses).
Greater variability in therapists’ methods (less strict protocols).
May or may not include a control group for comparison.
Does psychotherapy work according to efficacy studies? (Results of Efficacy Studies)
Yes, thousands of efficacy studies and meta-analyses consistently conclude that psychotherapy works.
What was the landmark meta-analysis study by Smith, Glass, and Miller (1980) about, and what did it find? (Results of Efficacy Studies)
The study analyzed 475 psychotherapy efficacy studies and found that:
The average effect size for psychotherapy was .85.
“The average person who receives therapy is better off at the end of it than 80% of those who do not.”
What are the three key benefits of psychotherapy? (Results of Efficacy Studies)
Psychotherapy:
Endures over long periods.
Exceeds placebo effects in effectiveness.
Creates clinically significant improvements in clients’ well-being.
What is psychotherapy not? (Results of Efficacy Studies)
Psychotherapy is not a panacea—it does not work perfectly for everyone. Some clients may worsen, drop out, or experience only short-lived benefits.
Why do the negative effects of psychotherapy appear to be the exception rather than the rule? (Results of Efficacy Studies)
Because the vast majority of studies and meta-analyses show overwhelmingly positive results, with only a small minority of clients experiencing negative outcomes.
Where is there a gap in psychotherapy research and practice? (Bridging the Gap Between Research and Practice)
There is a gap between those who conduct efficacy research on psychotherapy and those who practice psychotherapy in real-world settings.
What causes the gap between psychotherapy research and practice? (Bridging the Gap Between Research and Practice)
The gap exists because:
Researchers conduct studies that are often artificial, contrived, or irrelevant to real-world clinical practice.
Practitioners may resist scientific data and refuse to adjust their therapy methods based on research findings.
What have efforts to bridge the gap between research and practice focused on? (Bridging the Gap Between Research and Practice)
Efforts have focused on:
How much reluctance therapists have in adopting research findings.
Why that reluctance exists in the first place.
How much reluctance is there among therapists to incorporate research findings? (Bridging the Gap Between Research and Practice)
A lot. Surveys show that:
Efficacy studies have little influence on therapists’ clinical decisions/choices.
Personal clinical experience has a much stronger impact.
Even therapists who follow evidence-based approaches still prioritize their own judgment over research.
Why are therapists reluctant to adopt psychotherapy research findings? (Bridging the Gap Between Research and Practice)
Therapists value their own intuition and judgment more than methodically and scientifically collected data.
What do efficacy studies indicate about psychotherapy? (Results of Effectiveness Studies)
Efficacy studies indicate that psychotherapy works when tested in controlled settings with carefully selected participants.
What do effectiveness studies indicate about psychotherapy? (Results of Effectiveness Studies)
Effectiveness studies indicate that psychotherapy works as it is commonly applied in real-world/realistic clinical settings with diverse clients and therapist approaches.
How did infighting among psychotherapy orientations begin? (Which Type of Psychotherapy is Best?)
Infighting began after it was established that psychotherapy works, as different therapy orientations started competing over which approach was the most effective.
Why did infighting occur among psychotherapy approaches? (Which Type of Psychotherapy is Best?)
Different therapy schools (Freudians, cognitivists, humanists, behaviorists, etc.) viewed each other as competitors rather than allies, arguing over which "brand" of psychotherapy was superior in controlled experiments.
What were the collective surprising findings from studies pitting different types of therapy against each other? (The “Dodo Bird Verdict” and Common Factors)
The studies found that different types of therapy work about equally well, leading to a virtual tie in effectiveness.
What did Luborsky, Singer, and Luborsky (1975) find and do? (The “Dodo Bird Verdict” and Common Factors)
They found that different therapies produce similar outcomes and coined the term "Dodo Bird Verdict" after the dodo bird in Alice in Wonderland, which declared, "Everybody has won and all must have prizes."
What is the Dodo Bird Verdict? (The “Dodo Bird Verdict” and Common Factors)
It is the research finding that different forms of psychotherapy are roughly equally effective, despite their theoretical differences.
How does the Dodo Bird Effect apply to therapy outcomes? (The “Dodo Bird Verdict” and Common Factors)
Even though therapy approaches differ greatly (e.g., psychoanalysis, humanism, cognitive, behavioral), they still tend to produce similar positive outcomes in clients.
What are common factors in psychotherapy? (The “Dodo Bird Verdict” and Common Factors)
Common factors are elements shared by all forms of psychotherapy that actively contribute to client improvement, potentially explaining the Dodo Bird Verdict in psychotherapy outcome research.
How do different therapy approaches share fundamental components? (The “Dodo Bird Verdict” and Common Factors)
While proponents of each therapy school emphasizes its unique aspects, they all share core components that contribute to their effectiveness.
What is the notion behind common factors? (The “Dodo Bird Verdict” and Common Factors)
The idea is that different therapies benefit from the same underlying mechanisms, which contribute to positive outcomes regardless of the specific approach.
How do common factors function in all forms of psychotherapy? (The “Dodo Bird Verdict” and Common Factors)
They serve as “active ingredients” that drive therapeutic success, ensuring that different therapy types produce similar benefits.
What is the most important common factor in psychotherapy? (Common Factors Therapeutic Relationship/Alliance)
The therapeutic relationship/alliance—a partnership between therapist and client working in a trusting relationship toward a mutual goal.
What is the therapeutic relationship/alliance? (Common Factors Therapeutic Relationship/Alliance)
A coalition or partnership between therapist and client, built on trust and collaboration, working toward shared therapeutic goals.
What does research indicate about the relationship between the therapeutic alliance and therapy outcomes? (Common Factors Therapeutic Relationship/Alliance)
Studies show that the quality of the therapeutic relationship strongly contributes to therapy success, regardless of client age (adults, children, or families) or therapy format (individual or group).
What is the most crucial aspect of therapy?(Common Factors Therapeutic Relationship/Alliance)
The therapeutic relationship—it is considered the best predictor of therapy outcomes.
What two things has the therapeutic relationship been argued to do? (Common Factors Therapeutic Relationship/Alliance)
Best predictor of therapy outcome
Accounts for more variability in therapy success than techniques specific to any approach.
What do surveys find that clients tend to prefer in their therapist? (Common Factors Therapeutic Relationship/Alliance)
Many surveys find that clients prefer a warm therapist with whom they can related to over a treatment with empirical support
Is the therapeutic relationship vital to therapy no matter how much emphasis the therapist places on it? (Common Factors Therapeutic Relationship/Alliance)
Yes, the therapeutic relationship remains vital to therapy success, no matter how much a therapist emphasizes it.
How do therapists vary in their emphasis on the therapeutic relationship? (Common Factors Therapeutic Relationship/Alliance)
Behaviorists tend to deemphasize the therapy relationship.
Cognitive therapists place a moderate emphasis on it.
Humanists and psychoanalysts focus heavily on it.

What remains a vital component of therapy for clients in psychotherapy? (Common Factors Therapeutic Relationship/Alliance)
The therapeutic relationship, regardless of the therapist’s approach.
What did Arnow (2013) do, and what did he find? (Common Factors Therapeutic Relationship/Alliance)
Study: Split chronically depressed adults into brief supportive therapy and cognitive-behavior therapy (CBT) groups.
Finding: The correlation between clients' ratings of the therapeutic relationship and therapy outcome was high for both groups, but higher for CBT, even though CBT theoretically places less emphasis on the relationship than brief supportive therapy.

How does the therapeutic relationship contribute to successful therapy, according to Kazdin (2007)? (Common Factors Therapeutic Relationship/Alliance)
The connection between a good therapeutic relationship and client improvement isn’t necessarily one-way.
Three possibilities:
A good alliance facilitates client improvement.
As clients improve, they feel a stronger relationship with their therapist.
A reciprocal relationship exists where both influence each other.
Is therapy a one-way street? (Common Factors Therapeutic Relationship/Alliance)
No, therapy involves a dynamic relationship, where both the client and therapist influence each other.
What are the three possibilities for how the therapeutic relationship contributes to success? (Common Factors Therapeutic Relationship/Alliance)
A good alliance leads to client improvement.
Client improvement strengthens the relationship.
A reciprocal relationship where both influence each other could exist.
What does "correlation does not equal causation" mean for the therapeutic relationship and therapy success? (Common Factors Therapeutic Relationship/Alliance)
Just because a strong therapeutic relationship is linked to client improvement doesn’t mean the relationship directly causes the improvement—other factors may be involved.
What did Beutler (2006) say about the controversy between therapist techniques and the therapeutic relationship? (Common Factors Therapeutic Relationship/Alliance)
Beutler (2006) argued that the debate over whether client change is due to therapist techniques or the therapeutic relationship is based on a flawed either/or assumption. Instead, both technical and interpersonal factors must be considered in the complex process of change.
What are the two other common factors besides the therapeutic relationship/alliance? (Other Common Factors)
The two other common factors are hope and attention.
What is hope in the context of psychotherapy? (Other Common Factors)
Hope refers to the positive expectations or optimism provided by therapists, which can help clients believe that improvement is possible, even before specific therapeutic interventions are implemented.
What is attention in the context of psychotherapy? (Other Common Factors)
Attention refers to the focus the therapist and client direct toward the client's issues, which may be a novel approach to problems that the client had previously tried to ignore. Simply acknowledging and focusing on the problem with the therapist can lead to improvement.
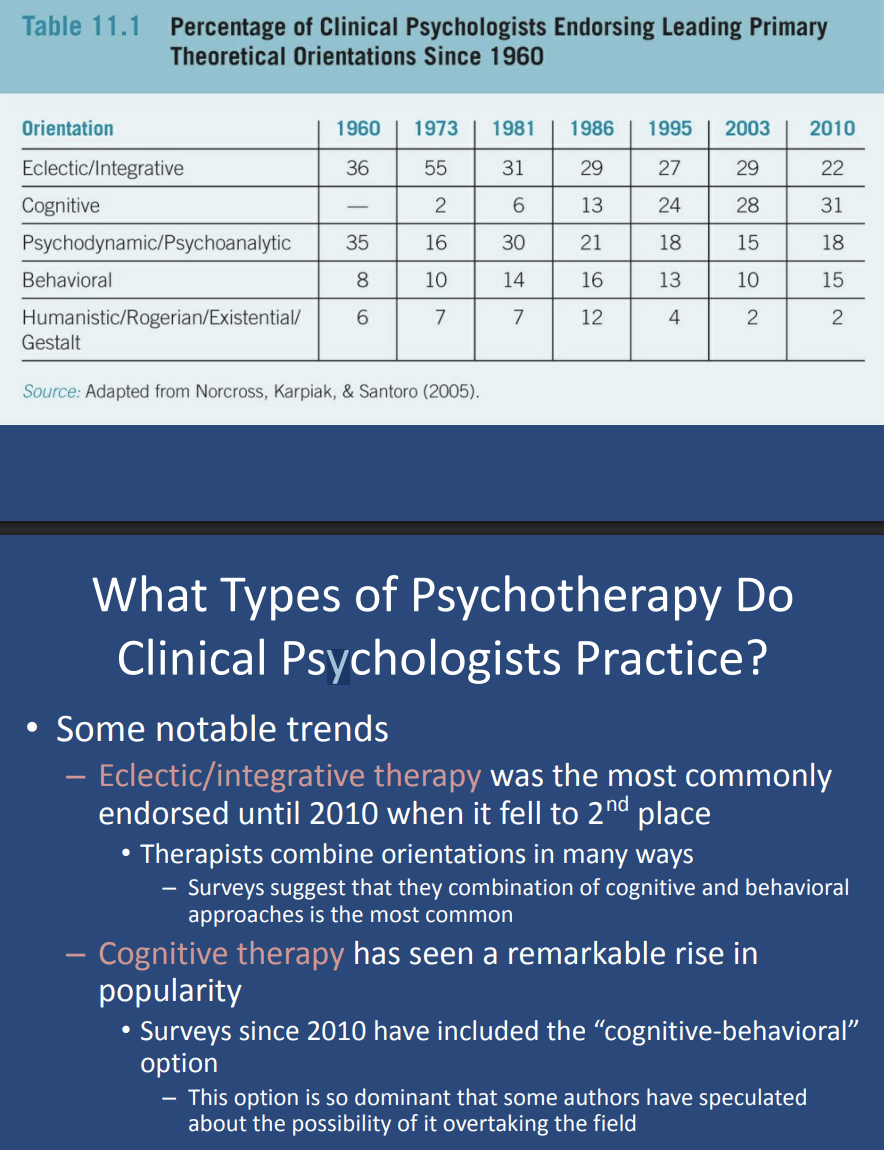
What type of therapy was most commonly endorsed until 2010? (What Types of Psychotherapy Do Clinical Psychologists Practice?)
Eclectic/integrative therapy was the most commonly endorsed type of therapy until 2010, when it fell to second place.
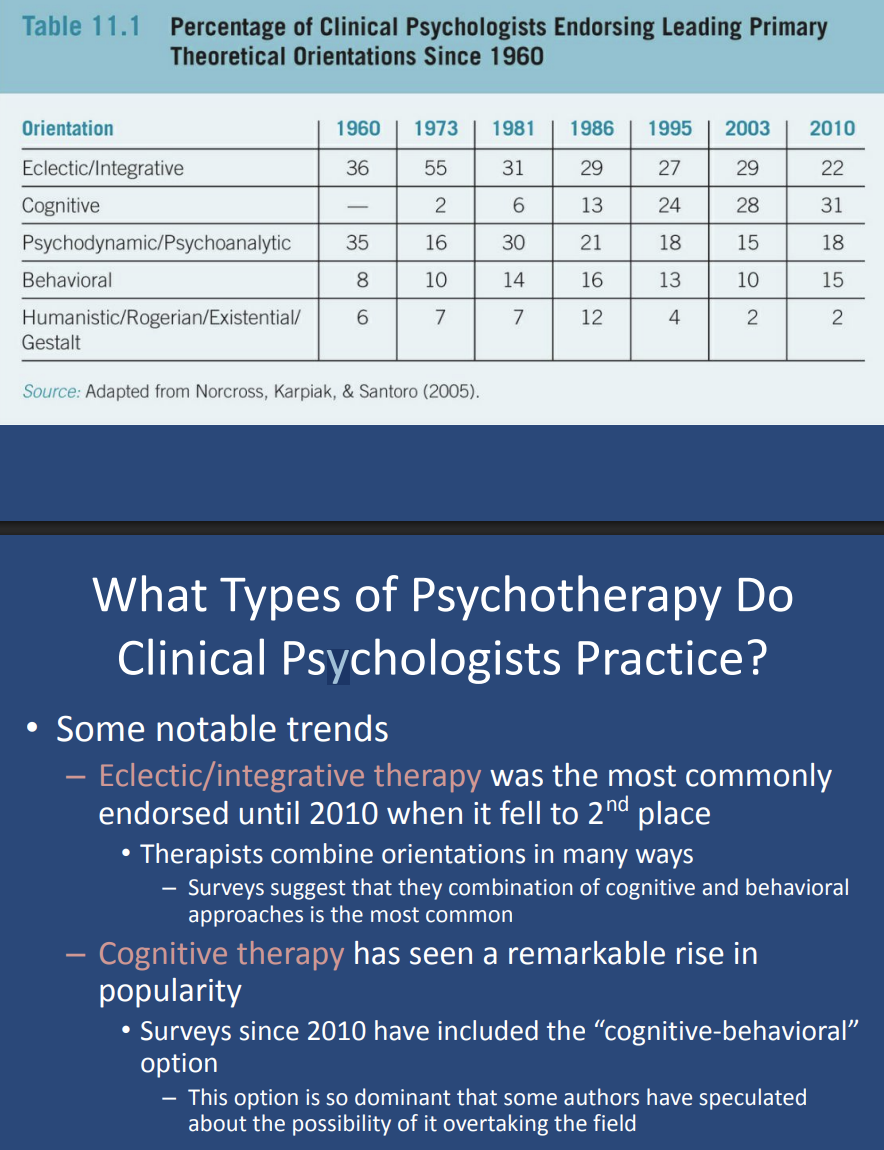
Surveys suggest that they combination of _____ and _____ approaches is the most common (What Types of Psychotherapy Do Clinical Psychologists Practice?)
cognitive, behavioral
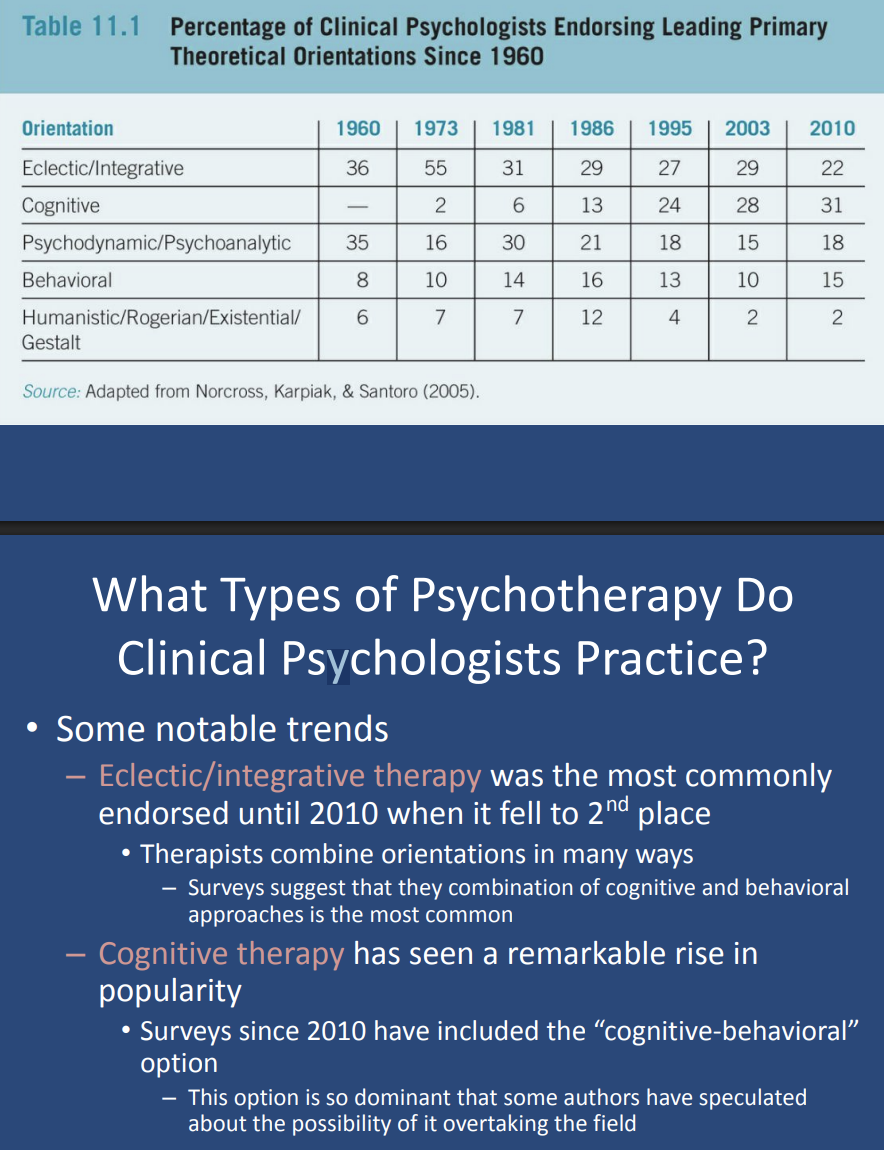
What type of therapy has seen a remarkable rise recently? (What Types of Psychotherapy Do Clinical Psychologists Practice?)
Cognitive therapy has seen a remarkable rise in popularity, especially since 2010.
Surveys since 2010 have included the “cognitive-behavioral” option
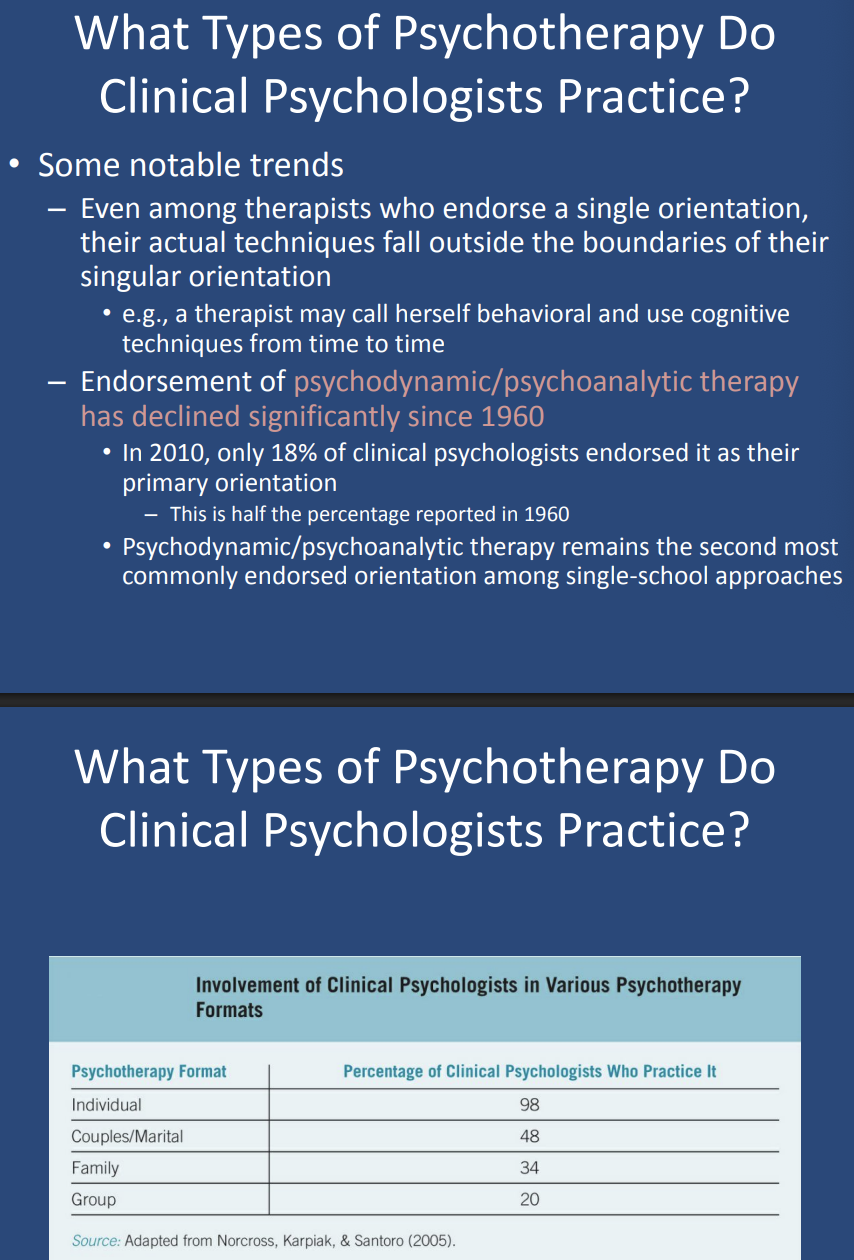
What are some other notable trends in psychotherapy practice? (What Types of Psychotherapy Do Clinical Psychologists Practice?)
Other notable trends include:
Therapists often combine cognitive and behavioral approaches, which is the most common combination.
Even therapists who endorse a single orientation may use techniques outside of that approach (e.g., a behavioral therapist using cognitive techniques).
Endorsement of psychodynamic/psychoanalytic therapy has declined significantly, from 36% in 1960 to only 18% in 2010.
Endorsement of _____ therapy has declined significantly since 1960. (What Types of Psychotherapy Do Clinical Psychologists Practice?)
psychodynamic/psychoanalytic