Exam 2
1/136
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
137 Terms
Neurodevelopment
Refers to the brain’s development of neurological pathways that influence performance OR function
These behaviors include intellectual functioning, reading ability, social skills, memory, attention and focus skills
Executive Functioning
A set of cognitive processes that allows individuals to plan, organize and execute a task, manage their thoughts/actions, and achieve goals (i.e., cognitive control)
What types of behaviors require the processes of executive functioning?
Working Memory - hold/manipulate information in your mind over short periods.
Flexible Thinking - ability to shift thinking when faced with novel information
Self-Control - ability to regulate emotions/behaviors/impulses. Aids in resisting distractions.
Planning - ability to map out steps to achieve a goal, and in a logical sequence
Self-monitoring - tracking one’s behaviors/performance
Time Management - ability to estimate time availability + time it takes to do a task
Organization - keeping things in a structured and logical order
Attention - ability to maintain focus on task/relevant information WHILE ignoring distractions
Developmental Milestones
A set of goals or markers that a child is expected to achieve during maturation.
4 Developmental Milestones to Identify
Cognitive
Social/Emotional
Language & Communication
Physical (Gross + Fine motor)
Cognitive Developmental Milestones
These milestones include ability in:
Thinking
Reasoning
Problem-solving
Social/Emotional Developmental Milestones
These milestones include ability in:
initiating peer contact
group play
adaptive skills (dressing, eating)
Language & Communication Developmental Milestones
These milestones include ability in:
Babbling/signing
Speaking
Physical Developmental Milestones
These milestones include ability in:
Gross Motor - use of LARGE muscle groups
walking
crawling
rolling over
Fine Motor - use of SMALLER muscle groups; more precise movements
Drawing
stacking
throwing/catching
Developmental Milestone “Red Flags” during early infancy
2 months - lack of fixation
4 months - lack of visual tracking
6 months - Failure to turn to sound/voice
9 months - Lack of babbling consonant sounds
24 months - failure to use single words
36 months - failure to speak in three-word sentences
Protection and Prevention of psychological disorders in children
Prenatal Care
Positive Parenting
Nutrition
Social Support
Trauma Awareness
Psychoeducation
Sleep
Postpartum depression/anxiety
Avoid substance use
Prevention programs
Prenatal Stress
Conceptualized as the combination of prenatal anxiety, perceived stress, and depression during a mother’s pregnancy period
Prenatal Stress and Child Development
Prenatal stress has been negatively associated with infant neurodevelopment (King and Laplante, 2005)
Fetal Programming Hypothesis
Because the fetal brain is exceptionally plastic, changes caused by intrauterine environment (in the womb) during critical periods of tissue growth can permanently alter organ structure, function and health outcomes for infants
Sleep Disorders
Conditions that disrupt normal sleep patterns
Sleep disorders and child psychopathology
Sleep disorders often mimic or worsen many symptoms of the major psychopathological disorders in children.
Trajectories of Sleep
Early Life - sleep patterns and needs drastically change
Newborns - Sleep 16-17 hours/day
Often experience night-waking issues
Toddlers - ~13 hours/day + daytime naps (1-2 hrs)
Adolescence - Increased need for sleep, but get less sleep than in early childhood
Older Adults - Sleep patterns shift, with many changes in their NREM sleep (negative changes!)
Overview of Sleep Disorders in Children
Sleep disorders in children can range from difficulties falling asleep to excessive sleepiness and sleep disruptions
Disorders include:
Insomnia
Hypersomnolence
Narcolepsy
Breathing-Related Sleep Disorders
Circadian Rhythm Sleep Disorder
Nightmares
NREM Sleep Arousal Disorders
Sleep Terrors
Sleepwalking
Prevalence and age of onset vary, with some disorders common among toddlers, preschoolers, or adolescents
Insomnia Disorder
Difficulty initiating OR maintaining sleep; Sleep that is not restorative (i.e., waking up tired); in infants, ID is accompanied by repetitive night waking + inability to fall asleep
Prevalence: affects 25-50% of 1-3 yos
Hypersomnolence Disorder
Excessive daytime sleepiness that is illustrated by prolonged sleep episodes or daytime sleep episodes
Prevalence: common among YOUNG CHILDREN
Narcolepsy
Neurological disorder that affects the brain’s ability to control sleep-wake cycles. Difficulty staying awake and randomly falling asleep + loss of muscle control (cataplexy)
Prevalence: <1% of children/adolescents
Breathing-Related Sleep Disorder
Sleep disruptions caused by sleep-related breathing difficulties, leading to insomnia or sleepiness
Prevalence: 1-2% of young children
Circadian Rhythm Sleep Disorder
Mismatch between internal sleep-wake cycles (circadian rhythm), and environmental schedule, causing insomnia or sleep disruptions.
Symptoms - late sleep onset, difficulty awakening in morning, sleeping in, resistance to sleep changes.
Prevalence: ~7% of adolescents (older children)
Nightmare Disorder
Repeated awakenings with detailed recall of long, frightening dreams; generally occur during 2nd half of sleep period
Prevalence: common among 3-8 yos
NREM Sleep Arousal Disorders
Sleep Terrors - abrupt awakenings with panic, crying, sweating, and distress during 1/3 of the sleep cycle; no memory of the terror episode
Prevalence - 3% of 18 mo-6 yos
Sleepwalking - episodes of walking during sleep, usually occurring in the 1/3 of the sleep cycle; no memory of the episode.
Prevalence - 15% of children have 1 episode; 1-6% have 1-4 attacks PER WEEK; rare in adolescence.
3 Treatments of Childhood Sleep Disorders
Natural Subsiding: sleep difficulties in infants/toddlers often resolve on their own
Strategies - reducing stress before bed and incorporating afternoon naps
Behavioral Interventions:
teach parents to attend to the child’s need for comfort
gradually withdrawing from the room to promote independent sleep.
Positive Reinforcement & Sleep Hygiene:
establishing good sleep hygiene (that fits the child’s development stage)
use of praise, star charts or other reinforcement methods to encourage consistent bedtime routine
Sleep Hygiene
Set of healthy habits and environmental factors that can help a child sleep better.
Signs of POOR sleep hygiene
Having a hard time falling asleep, experiencing frequent sleep disturbances, and suffering daytime sleepiness.
Ways to improve sleep hygiene
Set a sleep schedule - fixed wake up and bedtimes
Don’t force yourself to sleep
avoid caffeine, alcohol and nicotine
Avoid napping (adults)
Include naps (child)
Only use your bed for sleeping
Exercise and eat well
sleep in comfortable environment
Relaxation techniques
no dining late
dim the lights
unplug
Studies of environmental effects on sleep disorders in childhood
Impacts of COVID-19 lockdown on sleep in children with ASD
Found that changes due to quarantine resulted in significant changes in bedtime routine and showed increases in sleep disturbances
Juvenile Arthritis
Most common form of arthritis in child is Juvenile Idiopathic Arthritis (JIA)
Childhood Arthritis can cause permanent physical damage to joints. This can make it hard for the child to do daily task, and can result in disability
NOT A DSM-V DISORDER
Tic Disorders (2)
Tourette’s Disorder
Persistent Motor or Vocal Tic Disorder
Tourette’s Disorder
Definition - chronic neurodevelopmental disorder that causes people to have sudden, repetition and involuntary motor AND vocal burst, called “tics”. Has NOT been attributed to substance use or other medial conditions
Symptoms
the motor or vocal tics present during the illness
tics may wax and wane, but have persisted for more than 1 year since first tic onset
Onset - before 18 years old
Persistent Motor/Vocal Tic Disorder
Definition - a person has had motor OR vocal tics for at least 1 year. Does NOT have motor and vocal tics at the same time.
Symptoms
the motor or vocal tics present during the illness
tics may wax and wane, but have persisted for more than 1 year since first tic onset
diagnosed if child never met criteria for Tourette’s
Onset - before 18 years old
Case Vignette: Zandy (11-year-old; private school)
Primary Diagnosis
Generalized Anxiety Disorder (GAD)
Motor tic disorder (linked to anxiety)
Treatment Recommendations
“Cool Kids Anxiety Program” - structured cognitive-behavioral program that is designed to reduce anxiety in children
Behavioral interventions - introduce relaxation techniques or Habit Reversal Therapy (HRT) to help manage motor tics that increase with anxiety
HRT - replacing unwanted habits with other actions
Anxiety Management - exposure therapy, mindfulness techniques
Diabetes
Definition - chronic condition that occurs when the body doesn’t produce enough insulin or can’t use it properly.
Symptoms
Fatigue
Thirst
Hunger
Frequent urination
weight loss despite excessive eating
Treatments
daily treatment regime (e.g., blood-glucose monitoring; insulin injections)
dietary restrictions
NOT A DSM DISORDER
Health Issues that Occur with Diabetes
Insulin regulation
Too LITTLE/HIGH insulin = diabetic coma
Too LITTLE insulin = hypoglycemia
Hypoglycemia
episodes are unpleasant
can include irritability, headaches, and shakiness
Case Vignette: Brandon (14 y; ADHD, T1MD) — Parents referred
him for treatment due to difficulties with emotion dysregulation and social skills. He is also very smart but has slow processing speed scores. He struggles with organization skills, and his grades sometimes do not reflect his understanding because of these difficulties.
Diagnoses:
ADHD
T1MD
Behavioral Concerns
emotional dysregulation
social skills
slow processing speed scores
organizational skills
poor grades (despite good understanding of material)
Case Vignette: Brandon (14 y; ADHD, T1MD)
How might these two disorders play a role in his presentation?
Presentation
ADHD - contributes to difficulties with emotion regulation, organization and slow processing speed. This can affect social skills and academic performance despite intelligence.
T1MD - T1 diabetes; can affect mood/energy levels due to blood sugar fluctuations, potentially exacerbating emotional dysregulation, making it difficult to focus on task
Case Vignette: Brandon (14 y; ADHD, T1MD)
How are parents resources?
Parental Resources
ADHD: ADHD-specific support groups; educational workshops on managing ADHD in adolescents
T1MD: diabetes education programs for parents AND child; support groups for families
Case Vignette: Brandon (14 y; ADHD, T1MD)
IEP in place? How can the school help?
IEPs
IEP should address both child’s ADHD and processing speed issues:
School should provide extended time on tests/assignments; offer organizational/time management coaching
Obesity
Definition - chronic disease that occurs when someone has too much body fat
Prevalence - for children aged 2-19:
19.3% (~14.4M)
13% among 2-5 yo, 20% among 6-11 yo, and 21 among 12-19 yo
Obesity, Attention, and ADHD in childhood
Research links obesity to attention deficits and ADHD-like symptoms
Impulsivity and inattention may increase food intake, then weight gain
Sleep Difficulties associated with obesity may cause increase of inattention during the school day
Enuresis
Definition - repeated unloading of urine into bed/clothes
Symptoms
Occurs at least 2x a week for 3 consecutive months
distress
impairment in social, academic, or other important areas of functioning
Onset - 5 years old (or equivalent in developmental stage)
Behavior is not attributed to physiological effects of a substance or other medical conditions.
Encopresis
Definition - pooping/release of feces in inappropriate places
Symptoms
Occurs each month over 3 months
Onset - 4 years old (or equivalent in developmental stage)
Behavior is not attributed to physiological effects of a substance or other medical conditions (unless using constipation related medication)
Why are Enuresis and Encopresis included in the DSM?
These disorders can lead to psychological distress and limitations on social activities (think: 4 D’s)
negatively impacts self-esteem and can create social ostracism
Can indicate significant developmental, psychological or medical issues.
DSM is used to help diagnose these conditions to ensure appropriate treatment, and mitigate mental disorders.
Multi-method Assessment Approach
A way of using multiple types of test to gain knowledge about an individual or construct (i.e., novel disorders)
Incorporates data collected from a variety of informants from a variety of settings:
Clinical interviews
Observations
Checklist and Rating Scales
Testing
How does Multi-method assessment approach aid clinicians in diagnosing and treating intellectual disabilities in children?
Aids clinicians to formulate more detailed assessment
Develop more precise and targeted treatments/interventions for the child
identify problems that might otherwise go unnoticed
Child Clinical Assessment
An evaluation of a child’s emotional, social/behavioral, and cognitive functioning, as well as their family/school environments and functioning in these areas
Used to identify factors contributing to a child’s difficulties and strengths
What are the Two Types of Child Clinical Assessments?
Psychodiagnostic - determines if the child meets criteria for a disorder
Psychoeducational - focuses on understanding how and why a child is performing a certain way in school
What is the main goal of Child Clinical Assessment?
Enhance a child’s development and wellbeing
The assessment process tailors interventions to address both difficulties and strengths the child has, improving outcomes in emotional, cognitive, and social/behavioral areas.
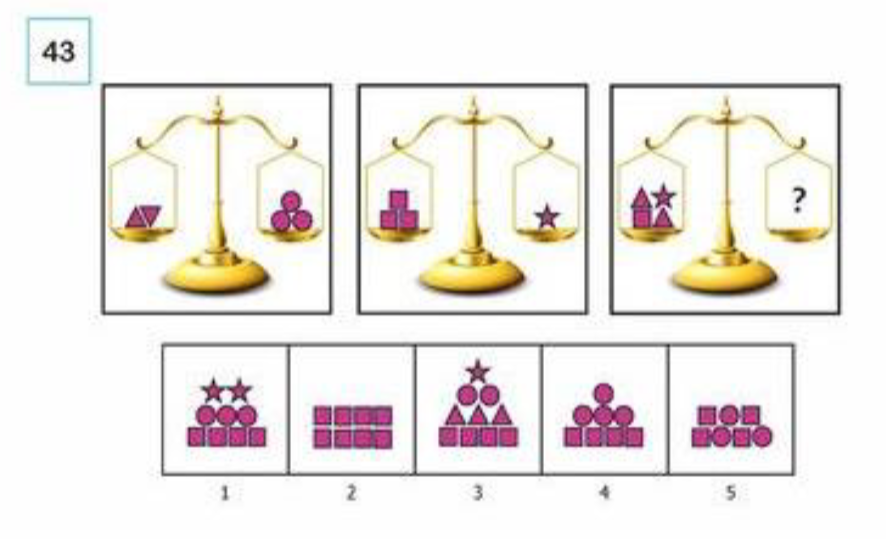
Non-verbal Reasoning Test (a type of cognitive assessment)
Used to evaluate problem-solving abilities, logic, and abstract thinking. Often included in intelligence tests or psychodiagnostic assessments for children to measure pattern recognition and visual-spatial processing.
Biases when assessing cognition in childhood: IQ Test
History - IQ tests have been historically used to assess intelligence, but have also shown biases AGAINST certain groups (racial/ethnic)
Bias in Black-White IQ Differences - research has found average point differences between Black/White test-takers IQ. These differences are influenced by socioeconomic, cultural and educational factors rather than pure cognitive ability
How has IQ test been used to discriminate against those with intellectual disabilities?
IQ tests were used to justify discriminatory practices, including eugenics, anti-disability laws, and immigration restrictions
How can we identify bias within a psychology test?
An identifying factor is if the test predicts different outcomes based on the group taking it, rather than accurately reflecting academic/cognitive ability across all groups
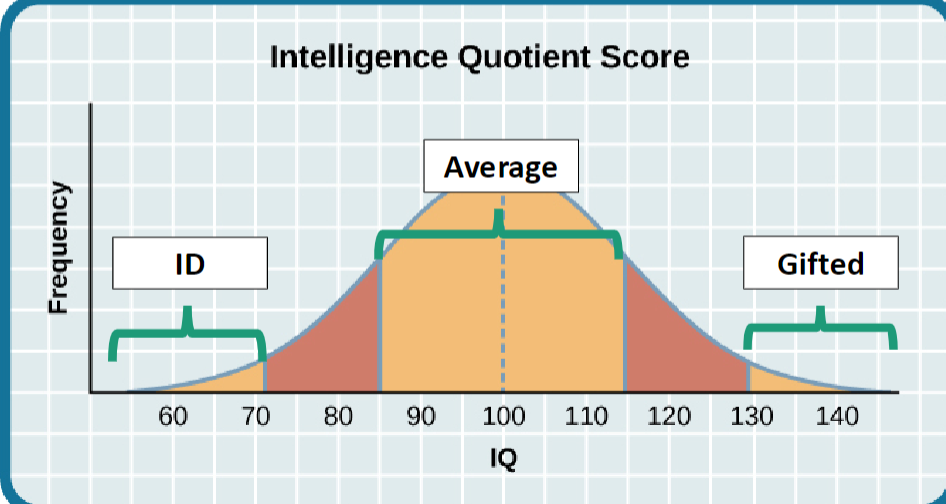
How was IQ Score Curve previously used to diagnose Intellectual Disability (ID)?
IQ score curve classified individuals with an IQ test score below 70 (~2SD below the mean) as having an intellectual disability.
However, later realized that adaptive functioning (personal independence + social skills) and age of onset needs to be considered before diagnosing ID.
Intellectual Disability
Characterized by deficits in intellectual functioning and difficulties in adaptive functioning that we expect to occur at a given developmental period
DSM-V Criteria for Intellectual Disability
THREE criteria must be met:
Deficits in intellectual functions, confirmed by BOTH clinical assessment and individualized intelligence testing (i.e., reasoning, problem-solving, planning, academic learning, etc.)
Deficits in adaptive functioning that result in failure to meet developmental AND sociocultural standards
Age of Onset of the signs identified in 1 and 2
Genetic vs Organic Disorders
Genetic disorders are caused by abnormalities in a person’s DNA, whereas organic disorders are caused by physical or biochemical changes in the body
Etiology of Intellectual Disability (origins)
Over 1,000 genetic disorders associated with ID, in addition to organic causes
Scientist are unsure of the causes of a majority of IDs, even mild ID
Categories of intellectual disabilities (FOUR)
Biomedical - related to biologic processes, such as genetic disorders or nutrition
Social - related to social/family interaction, such as child stimulation and adult responsiveness
Behavioral - harmful behaviors, such as maternal substance abuse.
Educational - related to availability of family and educational supports that promote mental development and gains in adaptive skills
Health and Other Related Disorders
Sleep Disorders
Juvenile Arthritis
Tic Disorders (Tourette’s and Persistence Motor/Vocal Tic Disorders)
Diabetes
Prevalence of intellectual disabilities in children
Overall -1-3%
Male to female ratio = 2:1
Mild ID is more prevalent among children of lower SES, and minority groups
At more severe ID these differences are almost equal among racial/economic groups
Prevention and Treatment of ID
No “cure”
abortion used to be presented as an option if it is detected that the baby is abnormaling developing during gestation
Can try to prevent ID in SOME cases (i.e., mitigating maternal infections, heavy metal exposure, etc.)
Early Intervention is the most beneficial and CRUCIAL for treatment of ID
Types of Intervention for childhood intellectual disabilities
EARLY INTERVENTION!!
Behavioral interventions
Family-based interventions
Types of treatment/intervention for children with intellectual disabilities
Treatment involves caregivers and other adults who participate in early, intensive, child-focused activities:
Behavioral Therapy and Management
Parent Training and Education
Language training for children
School support AND services (ex. accommodations)
What are some difficulties that came up in providing education for children with intellectual disabilities during the pandemic?
Limited Access to Resources - many children lacked access to technology and internet connectivity for online learning
Inconsistent Support - family support varied, affecting the consistency for educational engagement
Disruption of Routines - Changes in daily routines led to increased anxiety and difficulty focusing
Lack of Specialized Instruction -Difficulty to provide tailored support due to remove learning constraints
Social Isolation - reduced interaction with peers, which is crucial for social and emotional development
What are some ways in which psychologist respond to difficulties in education for children with intellectual disabilities?
Advocacy for Resources - promote policies that ensure equitable access to technology and educational resources
Individualized Support - develop tailored treatment plans that meet each child’s needs, and making it flexible to adapt to potential changes
Parental Guidance - provide parental training and resources for parents to support their child’s learning at home
History of Autism Spectrum Disorder
Ancient stories suggest children with ASF have been around for centuries
“Elfin children” were thought to be children that were left in place of real, human babies that were stolen away. These children were described as strange and remote, much like a child w/ ASD would be described.
Dr. Leo Kanner and Autism Research (1943)
Dr. Kanner was a psychiatrist who published the FIRST system description of childhood autism disorder
Children (w/ ASD) displayed:
more attention to objects than normal people
lacked social awareness
limited to no language
displayed stereotyped motor activities (i.e., preservation of sameness)
Preservation of Sameness
A behavioral characteristic of those with ASD, where the person exhibits a strong need for consistency and resists changes in routines, environments, or objects
Dr. Hans Asperger and ASD research (1944)
Dr. Asperger’s is noted for his early studies in atypical neurology, more specifically diagnosing milder forms of ASD in childhood.
Described a milder form of ASD that became known as Asperger’s Disorder; compared them to “absent-minded professors”
Asperger’s Syndrome
A form of Autism Spectrum Disorder (neurodevelopmental), characterized by:
Difficulty interacting socially, understanding social situations and body language.
Monotone voice
Repetitive behaviors and standing firm on beliefs
Onset - symptoms usually present around 3 yo, but official diagnosis doesn’t occur until age 7.
Childhood Disintegrative Disorder (CDD)
Children develop normally through age 3-4, then over a few months, they lose language, motor, social and other skills that they have already learned (ectopic development)
Pervasive Developmental Disorders (PDD)
Delays in the development of socialization/communication skills. Parents may see symptoms as early as infancy, although typical age of onset is before 3 yo (delayed development)
ASD and Classifications under DSM-5
Categories under ASD (DSM-5)
Autism
Childhood Disintergrative Disorder (CDD)
Asperger’s Syndrome (AS)
Pervasive Developmental Disorder (PDD)
DSM uses this classification because the symptoms and severity of the neurodevelopmental condition can vary widely between individuals, so there is a “spectrum” of presentations
NOS classification under DSM-5
“Not Otherwise Specified”
Used to described conditions/disorders that had symptoms that fit a general diagnosis, but don’t meet the criteria for a specific diagnosis
Behaviors of Autism Spectrum Disorder (DSM-5)
Persistent deficits in social communication and social interaction across MULTIPLE contexts
Restricted repetitive patterns of behavior, interests or activities
Present from early childhood
Impair or limit everyday functioning
May be comorbid with intellectual disability, but ID is NOT part of the diagnostic criteria for ASD
Development of Behavioral Symptoms and Atypical Neural Pathways of ASD (AT BIRTH)
Behavioral - Atypical Response to Social Cues
Decreased preference for social stimuli
Decreased social orienting (i.e., no response when name is called)
Decreased anticipatory pleasure associated with social stimuli (smiling at faces)
Neural Pathways - Decreased Activation of Neural Reward System
amygdala activation
prefrontal cortex (PFC) activity
Development of Behavioral Symptoms and Atypical Neural Pathways of ASD (12-18 MONTHS)
Behavioral - Impaired Social Communication
Inability to conduct Joint Attention
Inability of social imitation
Poor face processing
Neural Pathways - Impaired neural connections
Decreased activation/development of brain regions responsible for social perception and representations
Fusiform gyrus
Superior Temporal Sulcus (STS)
Language Regions
DSM Criteria for ASD - Social Communication Deficits (A)
Persistent Social deficits that manifest as ALL the following:
Deficits in social-emotional reciprocity - difficulties in back-and-forth conversation, reduced sharing of interests, and a failure to initiate/respond to social interactions
Deficits in nonverbal communication - abnormal eye contact, body language or lack of gestures
Deficits in developing, maintaining and understanding relationships - difficulties adjusting behavior in various social contexts
DSM Criteria for ASD - Restricted and Repetitive Behaviors (B)
Restricted and Repetitive behaviors that manifest as AT LEAST 2 of the following:
Stereotyped or repetitive motor movements, use of objects or speech (e.g., simple motor stereotypes, lining up toys, etc.)
Insistence on sameness, inflexible routines or ritualized patterns of verbal/nonverbal behavior
Highly restricted, fixated interests with abnormal intensities
DSM Criteria for ASD - Additional Diagnostic Requirements
(C) - Symptoms must be present in Early Developmental Period (these behaviors may not fully manifest until social demands EXCEED limited capacities or masked by learned strategies)
(D) - Symptoms cause significant impairment in social, occupational or other areas of functioning
(E) - Symptoms are not better explained by ID or global developmental delay (i.e., significant delay in 2+ domains of development)
Prevalence of ASD
CDC estimates ASD occurs in 1/68 births
Males-to-Females; 4:1
Intellectual Disability occurs in 31% of ASD cases (+25% of individuals in ""borderline” range)
Strong genetic component involved in the onset of ASD
Etiology of Autism (causes)
Used to be mother blaming - “refrigerator mother” (mother’s described as ‘emotionally cold” and “uncaring”; cause of ASD)
In recent times, ASD is now attributed to biology
Viruses, neurotransmitter and structural brain deficits
Recent increase in incidence caused them to look at environmental causes
Recent studies link older parent age, birth complications and pregnancies spaced <1 apart to increase risk of ASD
Are rates of autism really increasing?
Broader definitions + more acceptance of the disorder may lead to “increased” rates
Recategorization or “shifting” of people from ID to ASD category
While recent studies have observed environmental effects on onset of ASD, we must be skeptical of using these results on a broad scale
Potential difficulties that families may face when a member (more specifically, a child) has ASD
Communication difficulties (e.g., nonverbal, limited verbal skills)
Behavioral challenges
Social & Educational Integration
Transition to adulthood
Health & Mental health concerns (e.g., co-occurrences of conditions)
Microbiome and ASD
Microbiome (i.e., microorganisms that live within the body) has been seen to be a possible biological mechanism or explanation of ASD
ex. research in rodents link microbiome and ASD behaviors
Why is Early Identification important for people with ASD?
The earlier we identify autism, the earlier we can help children access services and the better their outcomes will be.
Identifying Autism (key, observable behaviors of those with ASD)
Avoiding eye contact
Having little interest in other children or caretakers
Limited display of language
Getting upset by minor changes in routine
KSADS - psychodiagnostic interviews
Autism Diagnostic Observation Schedule (ADOS)
Consultation
Do you think we’ll be able to diagnose children with autism solely using eye tracking technology (ETT)? If we can do it, should we? Why or why not?
ETT shows promise in helping diagnose ASD by tracking differences in gaze patterns (a sign of ASD). There are benefits and issues with this method:
Pros
Early detection - ETT could offer a more object indicator
Non-invasive - this technology is unobtrusive, making it easier to use with children
Cons
Limited Scope - ASD involves more than social gaze issues. Focus on ETT results may overlook other behaviors
Individual Differences - Not all children w/ ASD present the same way
False Positives/Negatives - over-reliance on a single tool could lead to misdiagnosis!
Overall, diagnosing ASD requires a COMPREHENSIVE EVALUATION, needing multiple test and observation to determine an appropriate diagnosis.
How do we treat autism?
Gold standard treatment = Applied Behavior Analysis (ABA)
TEACCH - program that helps people with ASD learn and enhance their skills
Reciprocal Imitation Training - treatment that helps children with ASD learn to imitate others in social context
Physical, Speech and Occupational Therapy (i.e., academic)
ABC Model (Behavioral-modification strategy)
Antecedent, Behavior, and Consequence
Antecedent - the event, action or circumstance that happens BEFORE the behavior. It can either trigger/be the root cause of the behavior
Behavior - the observable/measurable action that occurs
Consequence - the action, response or event that happens AFTER the behavior
Reinforcement vs Punishment Consequence (in ABC model)
Reinforcement - strengthens the Behavior
Punishment - decreased the Behavior
Antecedents (ABC Model)
Many parents don’t think to prompt for specific behaviors that they seek from their children. However, prompting can be an effect intervention strategy, especially since they can easily be changed.
Visual Schedules are 1 way to increase structure and prompt specific behaviors by specifically telling a child what to expect.
FOUR Types of Consequences
Reinforcement - INCREASE behavior
Positive - adding something desirable to increase the likelihood of a behavior
ex. child earns a sticker for completing homework. The sticker serves as a reward, increasing chance the child completing their homework
Negative - removing an averse stimulus to increase the likelihood of a behavior
ex. a buzzing noise is removed when the child behaves appropriately. The removal of the sound makes the child more likely to behave well.
Punishment - DECREASE behavior
Positive - Adding something unpleasant to decrease the likelihood of a behavior
ex. bed-wetting alarm sounds to wake up the child when they wet the bed. The addition of the alarm is a punishment and aids to decrease the negative behavior
Negative - removing something desirable to decrease the likelihood of a behavior
ex. a child loses their favorite toy when they misbehave. The removal serves as a punishment, and reduces chance of misbehavior
Which consequence type is most used within ASD treatment, and why is it seen as more effective than the latter?
Reinforcement (more specifically positive ref.)
P.reinforcement focuses on encouraging desired behaviors by rewarding them. This method builds a positive association with learning and behavior change.
Punishment is not used as it can increase stress/anxiety, may cause confusion and frustration, and reinforces negative before and consequences, never giving the child a chance to learn positive behaviors.
Susie is playing a game on the computer when her mother tells her that it is time for her to turn it off so she can start her homework. Susie falls to the floor, screaming and kicking. In an attempt to stop Susie from waking up her baby sister from her nap, Susie's mother tells her that she can have a few more minutes on the computer.
Use the ABC model to breakdown Susie’s reaction
Antecedent — Susie’s mother tells her to stop playing the game and to start her homework
Behavior — Susie falls to the floor, screaming and kicking (indicating she doesn’t want to stop playing her game
Consequence — In order to avoid waking the baby, Susie’s mother allows her to have a few more minutes on the computer
Susie is playing a game on the computer when her mother tells her that it is time for her to turn it off so she can start her homework. Susie falls to the floor, screaming and kicking. In an attempt to stop Susie from waking up her baby sister from her nap, Susie's mother tells her that she can have a few more minutes on the computer.
Based on the following behavior, does Susie’s mother’s response reinforce or mitigate her daughter’s behavior (possible function of the consequence)?
REINFORCEMENT
The consequence of Susie’s tantrum reinforces the behavior. By giving in and allowing more time on the computer, the mother unintentionally teaches Susie that tantrums are effective in getting what she wants, which may increase the likelihood of this negative behavior in the future
What are the benefits of using visuals to induce positive behaviors in children with ASD?
Visual Supports - pictures, symbols or written words used to communicate expectations or routines
Benefits
Reduces anxiety by clarifying tasks.
Helps children with ASD understand schedules, social cues, and transitions (ease them into change)
Encourages independence by offering clear, structured guidance