BPK 241 Lecture 9
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
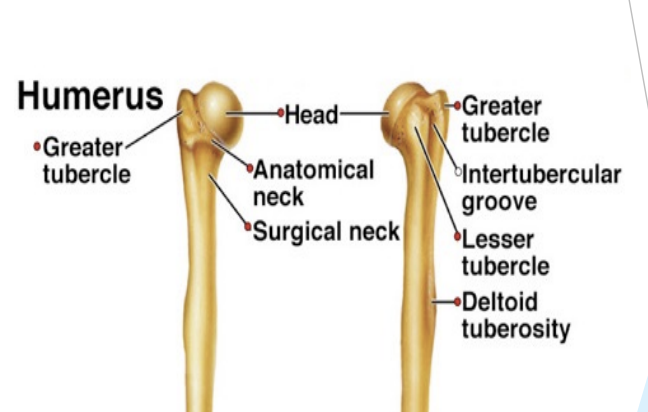
Humerus
Head
Anatomical Neck
Greater & Lesser Tubercles
Surgical neck
Shaft
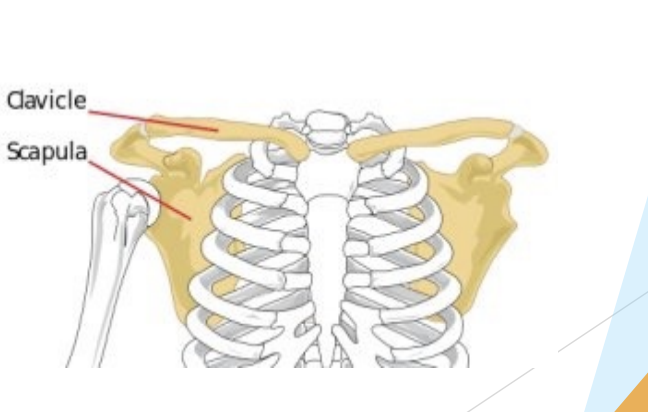
Clavicle
“Collar bone”
S shape
Subcutaneous
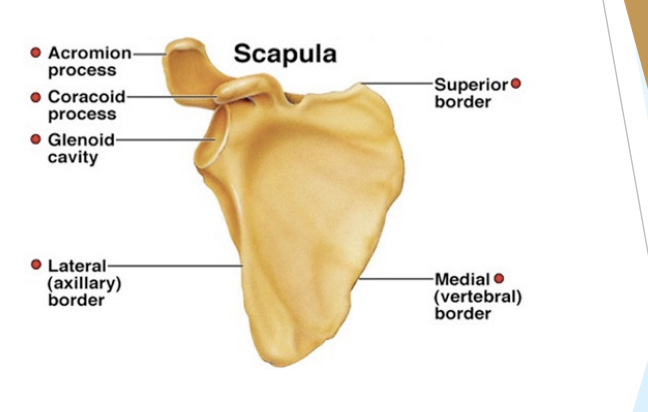
Scapula
“Wing bone”
Inverted triangle shape
Spine, acromion, glenoid process & cavity fossa, coracoid process
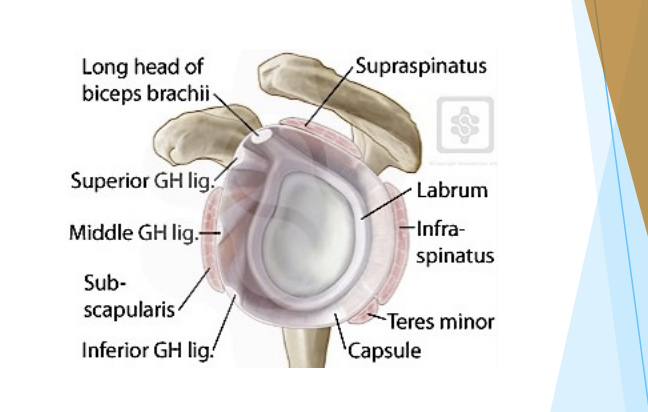
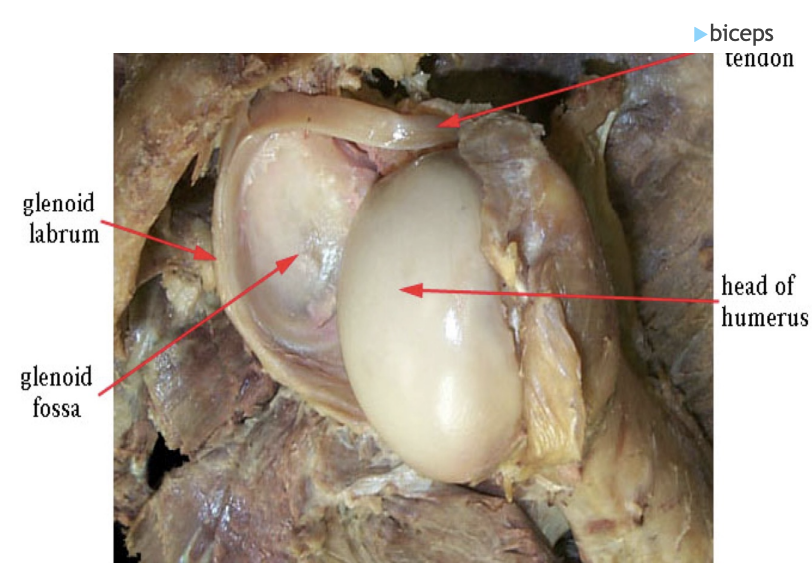
Glenohumeral joint (GH)
Type = Ball & Socket, synovial
Articulation = humeral head & glenoid cavity (N.B., glenoid labrum)
Sternoclavicular joint (SC)
Joint type = synovial
Articulation = manubruim & clavicle
Stability
Capsule
Anterior and posterior SC ligaments (downward pull)
Interclavicular ligaments (medial pull)
Costoclavicular ligaments (pull downward and medially)
Movements
Mainly rotation, plus elevation and retraction, during shoulder and arm movements
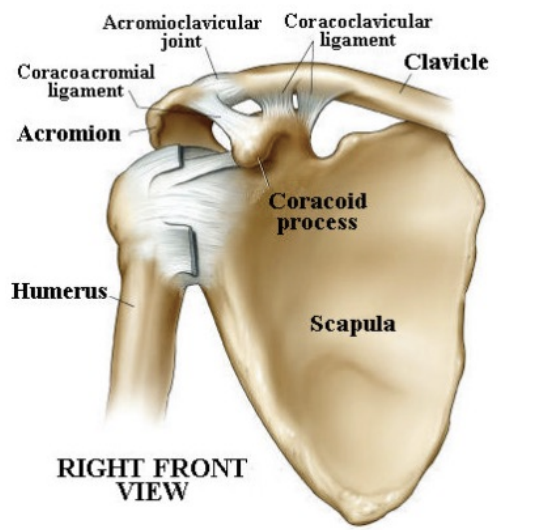
Acromioclavicicular joint (AC)
Joint type - synovial, gliding
Stability
Superior & inferior AC ligaments
Coracoclavicular ligament
Movements
Scapula (acromion process) & clavicle pivot upon each other (elevation, depression, retraction) in arm movements
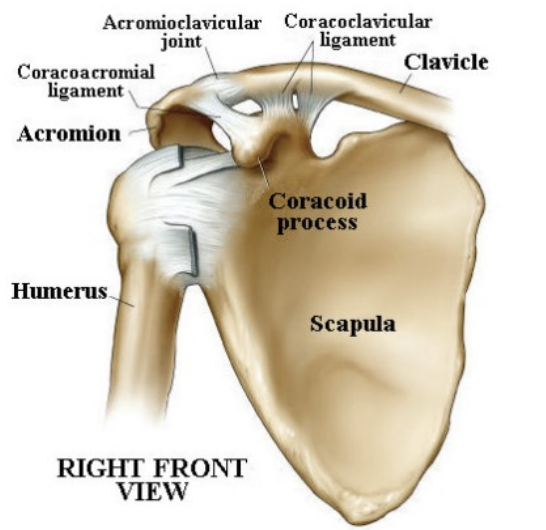
Coracoclavicular joint (CC)
Joint type = Syndesmosis
Stability
Coracoclavicular ligament
Assists in AC joint stability
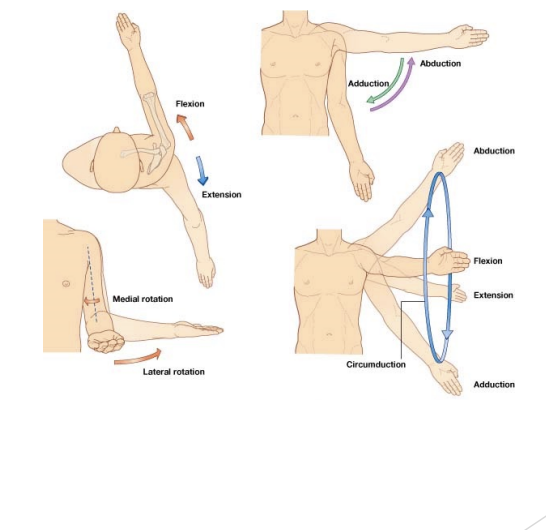
Shoulder Movements
Flexion & Extension, Abduction, Adduction, Internal Rotation and External Rotation
Hence circumduction
Stabilizers
Bony
Capsular & coracohumeral ligaments
Labrum
Superficial muscles
Tendon of long head of biceps humeri (in bicipital groove of humerus, to supraglenoid tubercle)
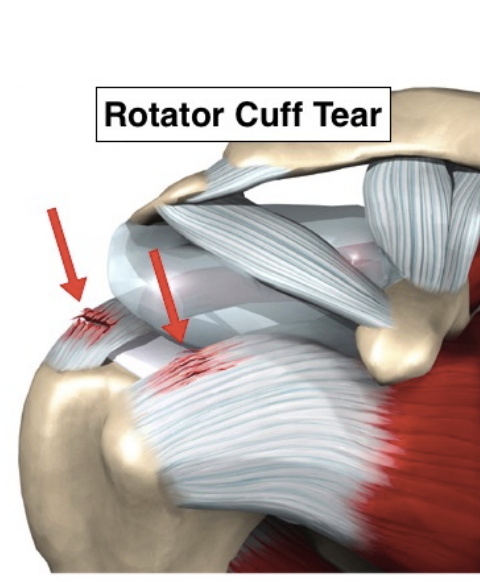
Rotator Cuff Muscles
Passive Stabilizers
Negative pressure
Adhesion between two moist cartilage
Adhesion Cohesion
Dynamic Stabilizers: Superficial muscles
All arise from thorax or scapulae
All insert on shaft of humerus
Deltoid (Abduction)
O = clavicle, acromion, spine of scapulae
I = deltoid tuberosity of humerus
Pectoralis major (Add, Flex, IR)
O = ribs, sternum, clavicle
I = anterior lip of bicipital groove
Latissimus dorsi (Add, Ext, IR)
O = thoracolumbar spine, ribs, ilium
I = anterior lip, bicipital groove
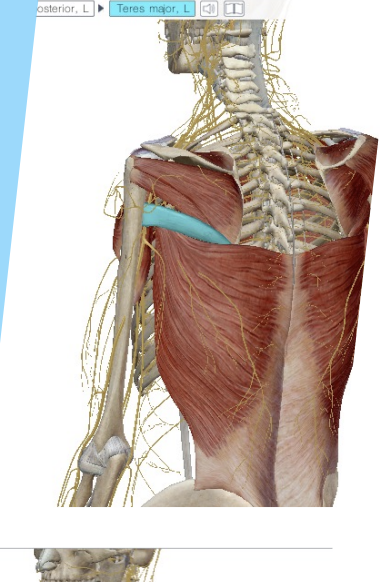
Teres major (Add, Ext, IR)
O = Lower 1/3 of lateral scapula
I = anterior lip, bicipital groove
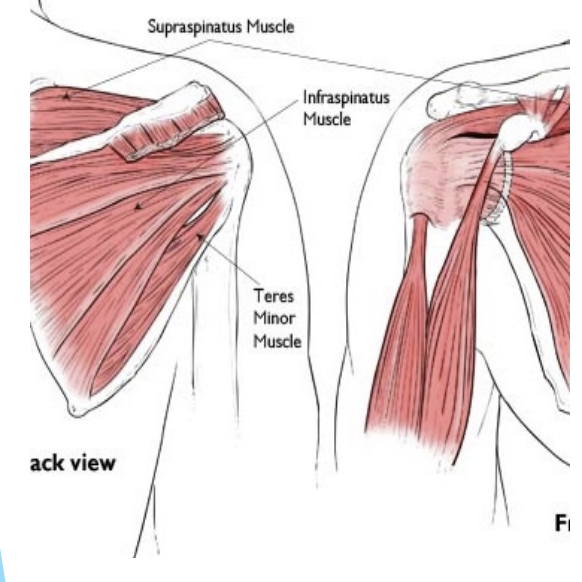
Dynamic Stabilizers: Deep group muscles
Aka “rotator cuff” muscles
All arise on scapula
All insert near humeral head
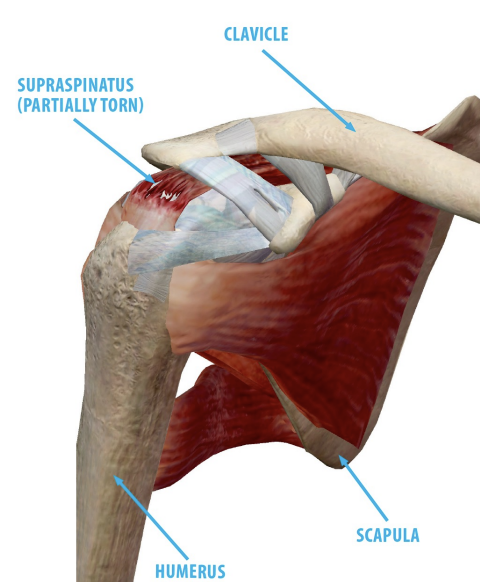
Supraspinatus (initial abd, stabilize head of humerus)
O = above spine of scapula
I = greater tubercle
Infraspinatus (ER)
O = below spine of scapula
I = greater tubercle
Teres minor (Add, ER)
O = upper lateral scapula
I = greater tubercle
Subscapularis (IR)
O = anterior (deep) surface of scapula
I = lesser tubercle
Force Couples
Forces working in opposite directions
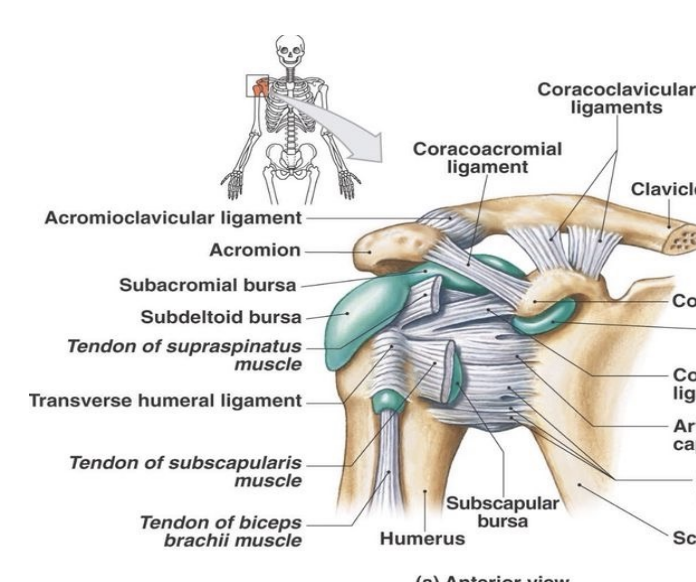
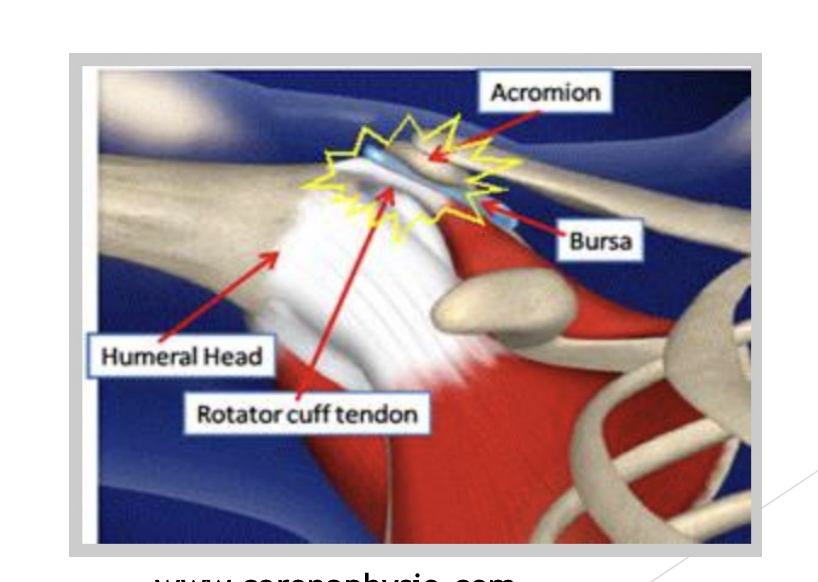
Bursae
Especially subdeltoid & subacromial
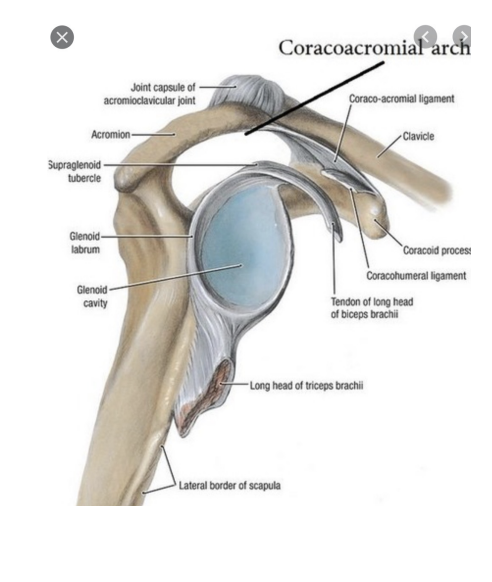
Coracoacromial Arch
The superior lateral extension of the scapula and is comprised of the acromion, coracoacromial ligament, and coracoid
Shoulder Injuries
Mechanisms
Throwing
Direct Blow
Resisting a force (especially in ABD/ER)
Fall on outstretched arm (FOOSH)
Shoulder Assessments
HX & PHX
Tenderness/ Pain level?
Observation/ Deformity?
ROM (active & passive)
Strength tests
Special tests
Palpation
Neurovascular status (brachial plexus, subclavian/axillary/ branchial artery)
Beware of rapid onset of “frozen shoulder” if immobilized due to pain, splint of inactivity!
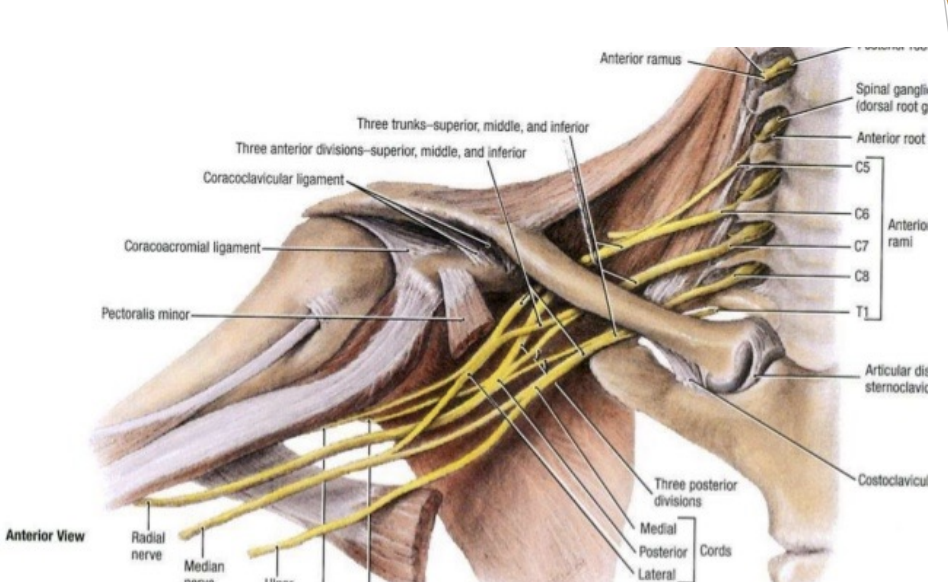
Brachial Plexus
Travels under clavicle from C5 to T1
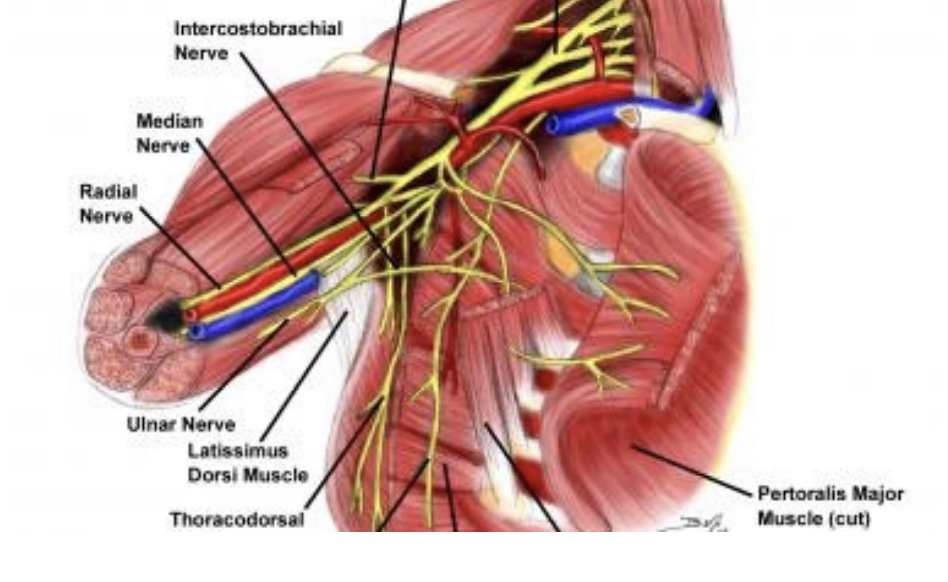
Neurovascular Bundle
Small collections of blood vessels (veins and arteries) and nerves which supply the tissues of the chest wall.

Contusion
Hx: direct blow
SSx:
Pain, tendernes
Reduced ROM
Bruising, swelling
DDx = fracture
Tx:
POLICE
Early ROM; physiotherapy
No massage! No heat!!
Strain
Hx = Resisting a force
SSx:
Pain, worse with active movement
Reduced ROM
Point tenderness, bruising?
Tx:
POLICE
Early ROM (passive, then active)
NSAIDs, tape
Physiotherapy & rehabilitation
Notes:
3rd degree strains may require surgery, and may not be obvious (. arthorogram, MRI, CT)
Tendonitis, tendinopathy is a common complication
Tendonitis (Tendinopathy)
Hx = acute strain or overuse; impingement (e.g., swimming)
SSx = as for acute strain (but prolonged duration)
Imaging X-Ray/ diagnostic ultrasound
Tx:
Adequate rest, ROM
NSAID (and/or corticosteroid injection) - rare
Physiotherapy, retraining, rehab
Surgery?

Pitching Mechanics Arm Acceleration
Pelvis rotation = 590º/s
Upper trunk rotation = 1140º/s
Knee extension = 380º/s
Elbow extension = 2720º/s
Shoulder rotation = 6950º/s
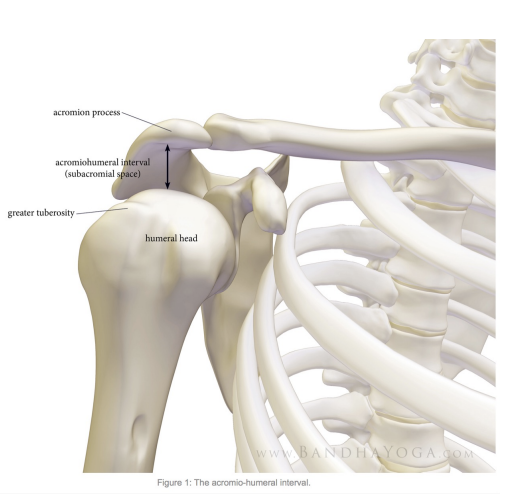
Subacromial Impingement Syndrome - SAIS
Pinching of the rotator cuff muscles
Risk factors for impingment
Overhead load and overhead work. Ex: Volleyball
Causes of Subacromial Impingement Syndrome
Intrinsic
Primary Impingement
Extrinsic
Dynamic Impingement
Primary Impingement
Subacromial space (AHD) measurement < 7mm is risk factor for impingement
Bone spurs
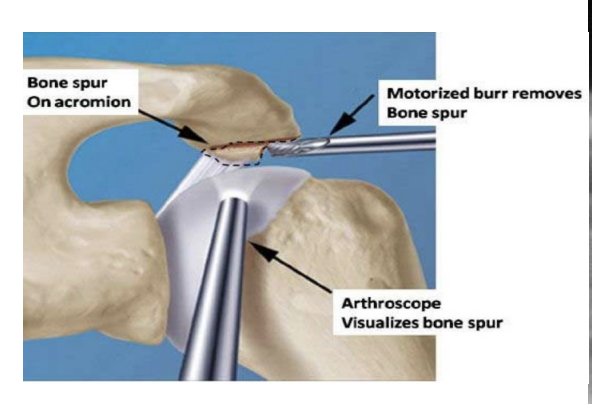
Primary Impingement Surgery
Tendon repair
Calcification
Osteophytes/ bone spurs
Subacromial decompression
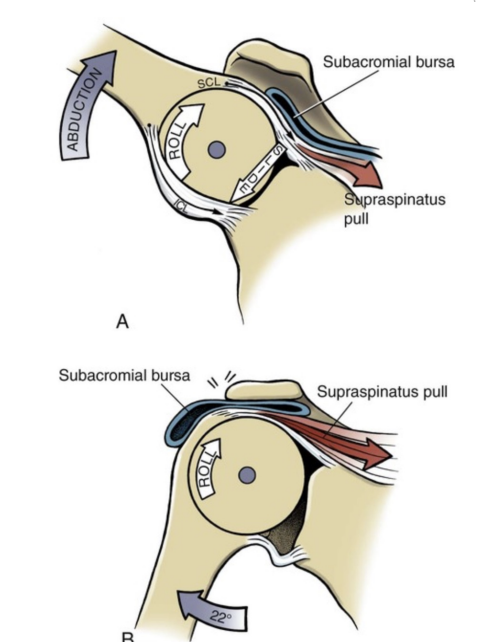
Dynamic Instability - Pathobiomechanics
Pain = Inhibition of lower rotator cuff muscles
Dynamic instability = Decreased subacromial space (SAS) during shoulder elevation compared to asymptomatic side
Result of upwards translation of humeral head during abduction
If we reduce fatigue in the rotator cuff muscles experimentally - results in the humeral head migrating upwards at the initiation of abduction
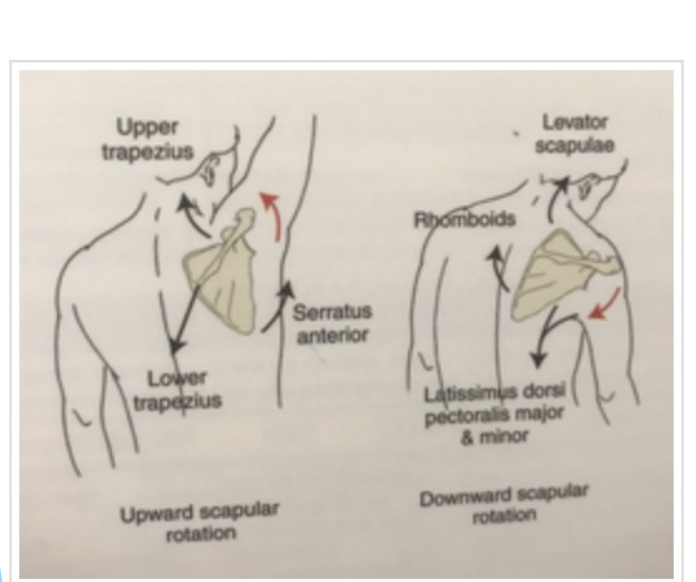
Tight pec major/ minor → anterior tilt of scapulae, limits scapular upward rotation, external rotation and posterior tilt = decreased SAS
Posterior capsule tightness → GIRD = decreased SAS
Small increase thoracic spine flexion = more elevation and anteriorly tilted scapulae at rest = decreased GH joint elevation
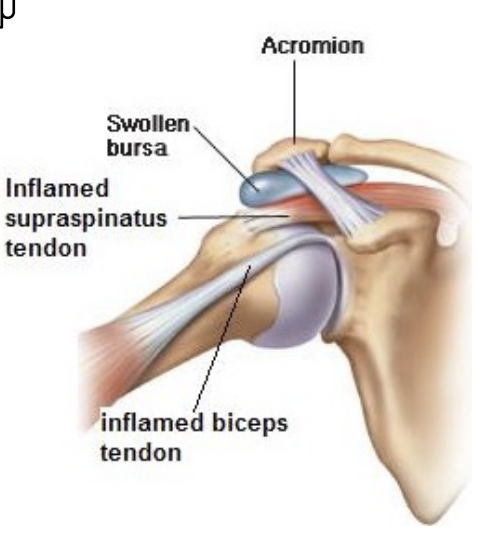
Bursitis
Hx: Acute trauma or overuse
SSx: Aching pain, tenderness, reduced ROM (abd) may lead to “frozen shoulder”
Tx = as for tendinopathy
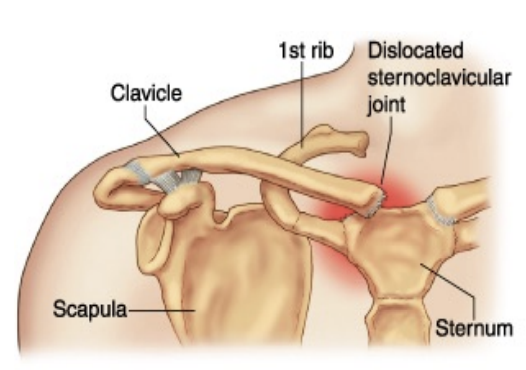
Sternoclavicular sprain (SC)
Hx = direct blow, torsion, fall
First degree
SSx = pain, tenderness, no deformity
Tx = rest, ice, NSAID, rehabilitation
Second degree
SSx = as above (worse), plus some deformity, crepitus, bruising, reduced shoulder ROM
Tx = sling (4-6 weeks), ROM, NSAID, physiotherapy, rehab
Third degree
SSx = as above (worse still), plus marked deformity
Tx = sling, stabilize, to hospital; follow up as above
Precautions: 2nd and 3rd degrees send to hospital for imaging, if clavicle is displaced posteriorly it may put pressure on blood vessels, esophagus or trachea
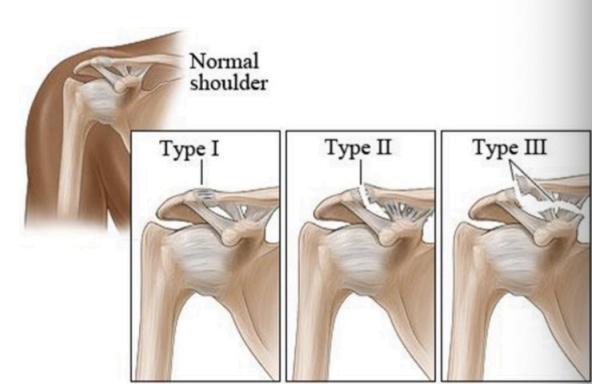
Acromioclavicular Sprain (AC)
Hx = direct blow, fall
First degree
SSx = pain, worse on movement
Point tenderness, swelling, mild deformity
Tx = POLICE, sling, ROM, physio
Second degree(rupture of AC ligament)
SSx = as above (worse) plus:
More deformity, crepitus?
Marked restriction in ROM
Tx = ice, sling, to hospital (X- Ray), then NSAID, physio, rehab
Third degree (rupture of AC & CC)
SSx = marked deformity (step defect), pain, etc..(“separated shoulder”)
Tx = as for second degree, surgery?

Glenohumeral Sprain (GH)
Hx:
Resisting a force (abd, ER)
Fall
Throwing
SSx = same as for rotator cuff strain, but pain is marked both on active and passive movement
Tx:
POLICE
Sling
Early ROM
NSAID
Physiotherapy
Note: Third degree GH sprain is a “shoulder dislocation”
Glenohumeral dislocation
Hx = as for GH sprain (+PHx?)
Forward (anterior, subcoracoid)(much more common)
SSx:
Humeral head palpable in axilla
Deltoid flat; indented; arm in abd
Severe pain and reduced ROM
Tx:
Check neurovascular status!
NPO, sling, to hospital ASAP(X-Ray, reduction; if recurrent, surgery)
Agressive rehabilitation
Downward (posterior, subglenoid)
SSx = same, except arm seems longer
Tx = same
Note; recurrence is common (70-90% after first, vs 2% post-op)
Glenohumeral Dislocation: Management
Immediate immobilization, sling
Reduction by physician
X-Ray to make sure no fractures
General body conditioning (biking, speed-walking, running)
Range of Motion - attempt to regain full, non-restricted pain-free ROM, try to regain at all surrounding joints as well as they work together
Muscular strength - isometric for IR and ER, then rubber tubing exercises, then dumbbells and other resistant devices as pain allows
Isotonic, isokinetic, plyometric, scapular stabilization exercises
Neuromuscular control - relearning to use injured extremity in coordinated highly skilled movement
Functional progressions - increasing resistance and difficulty of exercises when it is pain free and completely functional
Return to Activity - based on functional performance
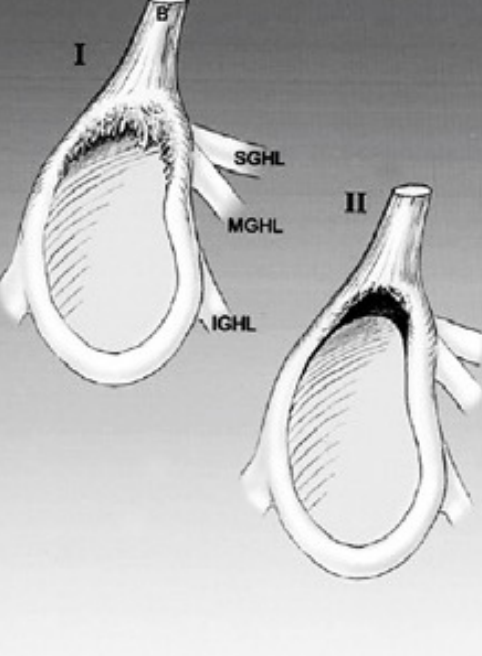
SLAP Tears
Superior Labral tear from anterior to posterior
Many different classifications (7 to 10 depending on classification system)
Types 1 to 4 most common
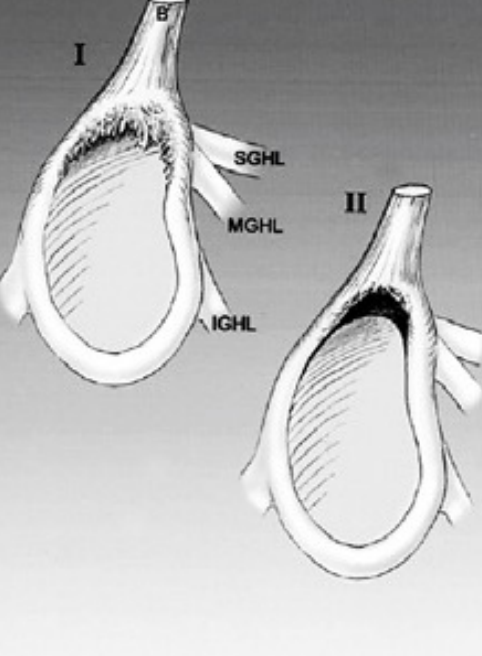
SLAP Type 1
Partial tear of labrum where edges are roughed but not completely detached
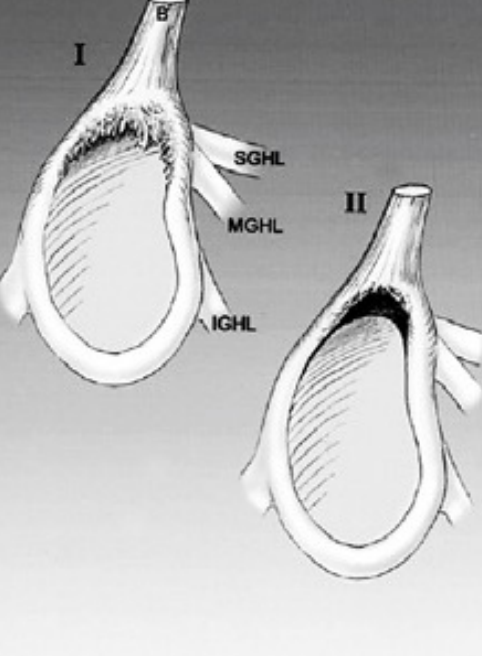
SLAP Type 2
Most common, labrum is torn off the bone due to injury (glenohumeral dislocation)
Tx is reattachment of labrum, done arthroscopically using suture anchors
SLAP Type 3
“Bucket handle” tear of labrum, torn piece hangs into GH joint and causes locking, popping, clunking
Tx involves removal of bucket handle segment, repair any remaining unstable labrum with anchors
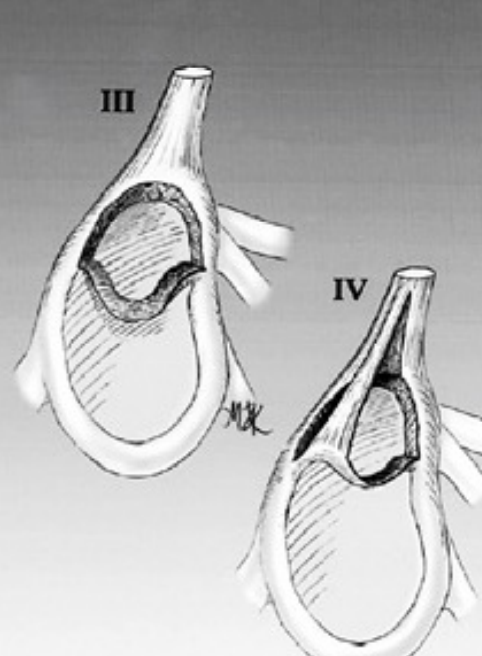
SLAP Type 4
Tear of labrum extends into the long head of biceps tendon
Tx involves reattachment of the labrum & repair of biceps tendon (biceps tenodesis)
Tear like cheese string
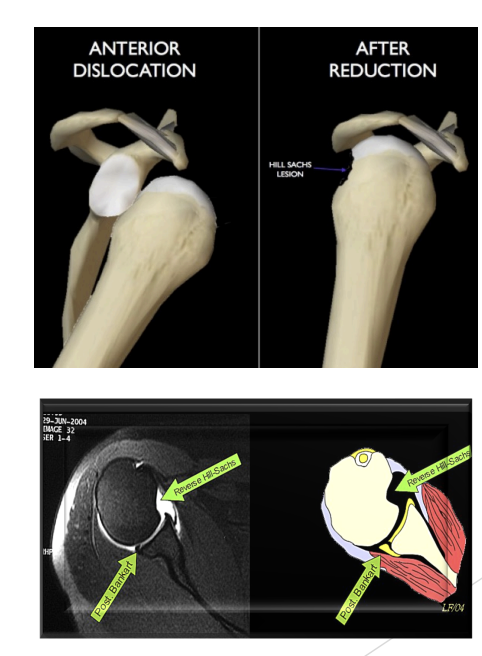
Glenohumeral Fractures
Hx = dislocation
SSx = as for dislocation
Types = head of humerus (Hill-Sachs) - hatchet defect
Glenoid process (Bankhart lesion)
Tx = hospital to assess; X-Ray, surgery?
Complications = neurovascular; arthritic
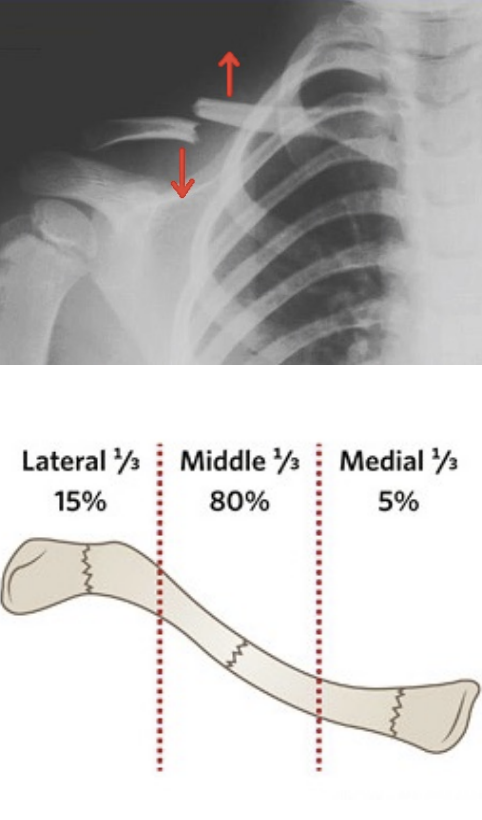
Clavicular Fractures
Hx = direct blow, fall (mid 1/3)
SSx = deformity, crepitus, pain, tenderness, swelling, marked reduction in ROM; positive X-ray
Tx = check neurovascular status, hospital to assess, sling (6 to 8 weeks), physiotherapy
Surgery rare