Silverstein and Hopper Chapter 130: Thermal Burn Injury
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
39 Terms
What are the two major parameters used to assess burn wounds?
Depth of the injury
Percentage of body surface area involved
First Degree Burn Depth
Superficial (epidermis only)
Superficial (Epidermis Only) Burn Appearance
Erythematous
Painful to touch
Superficial (Epidermis Only) Burn Healing
Healing is rapid; reepithelializes in 1 week with topical wound management
No systemic effects
Second Degree Burn Depth
Epidermis and superficial part of dermis
or
Epidermis and deeper part of dermis
Epidermis and Superficial Part of Dermis Burn Appearance
Epidermis will be charred and sloughs; plasma leakage occurs
Hair follicles spared
Painful to touch
Epidermis and Superficial Part of Dermis Burn Healing
Healing by epithelialization from the wound margin with minimal scar in 10-21 days
May have systemic effects
Epidermis and Deeper Part of Dermis Burn Appearance
Skin appears black or yellow-white
Hair follicles destroyed
Decreased pain sensation
Epidermis and Deeper Part of Dermis Burn Healing
Healing by contraction and epithelialization but scarring is significant without surgical intervention
Significant systemic effects expected
Third Degree Burn Depth
Full thickness (entire epidermis and dermis)
Full Thickness (Entire Epidermis and Dermis) Burn Appearance
Skin is black, leathery; eschar insensitive to touch
Full Thickness (Entire Epidermis and Dermis) Burn Healing
Healing often requires extensive surgical intervention, possible skin grafts and flaps
May have life-threatening systemic effects
Fourth Degree Burn Depth
Full thickness (with extension to muscle, tendon, and bone)
Full Thickness (with Extension to Muscle, Tendon, and Bone) Burn Appearance
Skin is black, leathery; eschar insensitive to touch
Full Thickness (with Extension to Muscle, Tendon, and Bone) Burn Healing
Skin grafts and flaps usually required to prevent scarring that could restrict joint movements
How many days can it take a burn to “declare” itself?
It can take up to 3 days or more for the burn to "declare" itself and during that time thermal injury and circulatory compromise from thrombosed vessels can continue
Patients with burning involving what % of their total body surface area can have serious cardiovascular, pulmonary, and metabolic derangements?
More than 20%
Patients with what % of their total body surface area have a poor prognosis and euthanasia should be discussed?
More than 50%
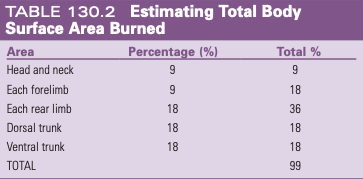
Rule of Nines
Total body surface area can be estimated in animals using percentages allotted to the body area using the rule of nines
Within how many days does skin form an eschar if severely burned?
Within 7-10 days
Eschar
Deep cutaneous slough of tissue composed of full-thickness degenerated skin
Appears as a black, firm, thick movable crust that separates from the surrounding skin
Purulent exudates often lie beneath the eschar
Metabolic Derangements from Burns
If more than 20% of a patient's TBSA is burned or if the wounds are classified as second or third-degree, hypovolemic shock often occurs
As a result of capillary thrombosis and plasma leakage, massive amounts of fluid are retained in the wound, often leading to burn wound edema
Results in loss of fluid and electrolytes, with the most dramatic losses occurring within the first 12 hours
By 48 hours after injury, plasma volume is mostly restored so patients are at high risk for generalized edema and fluid overload from the high initial demands for fluid replacement
What should a burn patient be assessed for from days 2-6?
Anemia, DIC, immune dysfunction, SIRS, and early burn wound infection
What should a burn patient be assessed for from day 7 on?
Hyperthermia or fever, hypoxemia, pneumonia, sepsis, and wound demarcation
After initial shock resuscitation, what should total fluid delivery rate during the first 24 hours be for a burn patient?
1-4 ml/kg body weight x %TBSA burned
Antimicrobial Therapy for Burns
Sepsis is one of the greatest threats to burn patients with extensive TBSA involvement because bacteria can colonize and proliferate in wounds that have lost the protective skin barrier
Prevent local and systemic skin infection by protecting the wound from contamination in the hospital environment and removal all necrotic tissue and purulent exudates from the wound surface as aggressively as possible through serial debridement
Systemic antimicrobials are not indicated unless the patient is immunocompromised, has pneumonia or pulmonary injury, or sepsis is suspected
Topical antibiotics are the antimicrobial treatment of choice
Most invasive burn wound infections are caused by Pseudomonas or other gram negative organs, antimicrobials against these bacteria are used until culture results are available
What can you do if a patient presents within 2 hours of the burn injury?
If the patient presents within 2 hours of the burn injury, cold water lavage for 30 minutes will often help to release heat from the skin and limit the depth of the injury or can submerge the affected area in a cold water bath
If large areas are affected must prevent iatrogenic hypothermia
Treatment in Patients with Superficial or Superficial Partial-Thickness Burns
Can use daily lavage and topical agents alone until the extent and depth of the wound is determined
Treatment for Deep Partial-Thickness and Full-Thickness Burns
Require debridement which can be done conservatively or surgically
Conservative often used for the first 3-7 days until the wound declares itself and the patient stabilizes
What should you use to lavage a burn wound?
When lavaging the wound use a 35 ml syringe and a 19 gauge needle to create a pressure of 8 psi
Higher pressures may induce tissue trauma and cause deeper seeding of bacteria into the burn
Treatment for Deep Partial-Thickness and Full-Thickness Burn Wounds
Aggressive surgical excision of an entire burn wound is indicated in deep partial-thickness and full-thickness burn wounds
Ideally close primarily, otherwise allow to heal by second intention and a flap or skin graft can be performed
What are the most common topical agents used for burns?
Aloe vera and SSD
Aloe Vera for Burns
Aloe vera cream has antithromboxane effects that prevent vasoconstriction and thromboembolic seeding of the dermal vasculature
Ideally using it within the first 24 hours can help prevent progression of superficial partial-thickness burns
SSD for Burns
Apply SSD after the first 24 hours
Has a wide spectrum of bactericidal activity against G+ and G- bacteria and Candida
Benefits of Medicinal Honey for Wounds
Benefits include antibacterial, antiinflammatory, antiedematous, and antioxidant effects
Healing Time for Superficial and Partial-Thickness Burn Wounds
Superficial and partial-thickness burn wounds have a favorable outcome with no surgical intervention
Reepithelialize quickly and can heal within 1-3 weeks
Healing Time for Deeper Burns Involving the Hair Follicles
Heal more slowly (3 weeks or longer)
Healing and Closure for Deep Dermal Partial-Thickness and Full-Thickness Burns
Deep dermal partial-thickness and full-thickness burns heal by contraction and epithelialization once a healthy granulation bed has been created
Can eventually be closed primarily
Full-thickness burns covering large areas of the body or on the limbs may require skin grafts or flaps for complete closure
Complications of Burns
Scarring and wound contracture are the biggest complications in patients with burn wounds left to heal by second intention