3 functions of the kidneys
Excretion (filtration, reabsorption, secretion): eliminates wastes, like urea and other toxic molecules
Balance: regulates blood volume, blood pressure, ion/solute concentration, & the pH of the extracellular fluid
Production: erythropoietin (RBCs) and vitamin D (blood Ca++ level)
Urinary System Anatomy (diagram)
Location of the kidneys: retroperitoneal on the posterior abdominal wall on either side of the vertebra & they are protected by the lumbar vertebra and 11th and 12th ribs
Which kidney is slightly lower?
Right is lightly lower than left
External Anatomy of the Kidneys
Renal capsule: fibrous connective tissue that surrounds the kidney
Perirenal fat: fat that engulfs the renal capsule & acts as cushioning
Renal fascia: a thin layer of tissue that anchors the kidneys and surrounding adipose to the abdominal wall
Hilum: the location of renal artery and nerve entry & renal vein and ureter exit
Internal Anatomy of the Kidneys
Cortex: outer layer of kidney
Medulla: inner layer of the kidney
Renal columns: cortical tissue that extends into the medulla
Renal pyramids: cone shaped structures that make up the medulla
Base is at cortex-medulla boundary
Renal papilla: the apex of the renal pyramids
Minor calyx (8-20): the tip of the renal papilla
Major calyx (2-3): where several minor calyces converge
Pelvis: the chamber formed by the major calyces
Ureter: the vessel that transports urine from the renal pelvis to the bladder
What are the contents of the cortex and medulla?
Cortex: glomeruli, renal columns (partly), nephrons (partly), collecting ducts (partly)
Medulla: renal pyramids, renal papillae, calyces, renal pelvis, & renal columns (partly), nephrons (partly), collecting ducts (partly)
The apex of the renal pyramid is called the
A. major calyx.
B. minor calyx
C. renal papillae.
D. renal pelvis.
C. renal papillae.
What is a nephron?
the functional unit of the kidney that is made up of the renal corpuscle, proximal tubule, loop of Henle, and distal tubule
What does the renal corpuscle (RC) do?
filters blood
What does the proximal tubule (PCT) do?
returns filtered substances filtered substances to the blood
What does the loop of Henle (LH) do?
helps conserve H2O and solutes
What does the distal tubule (DCT) do?
rids the blood of additional waste
What is the path urine takes from the nephron to the bladder?
nephron → collecting ducts → papillary ducts → minor calyces → major calyces → renal pelvis → ureter → bladder
How many nephrons are in each kidney?
approximately 1.3 million
2 types of nephrons
Juxtamedullary: the renal corpuscle is near the cortical-medullary border & the loops of Henle extend deep into medulla
Cortical: the renal corpuscle is near the periphery of cortex & the loops of Henle do not extend deep into medulla
What percentage of total nephrons are juxtamedullary nephrons?
15%
What two things make up the renal corpucle?
Bowman’s capsule
Glomerulus: a tangled network of capillaries that serves as the filtration unit of the nephron
2 layers of the Bowman’s capsule
Parietal layer made out of simple squamous epithelium
Visceral layer made out of specialized podocytes that wrap around glomerular capillaries)
Where does blood enter/exit the glomerulus?
Enters: afferent arteriole
Exits: efferent arteriole
What 3 structures make up the filtration membrane of the renal corpuscle?
podocyte cell processes
basement membrane
capillary endothelium
Filtration slits
gaps between the the podocyte cell processes of the renal corpuscle’s visceral layer
Fenestrae
window-like openings in the capillary endothelium that make the glomerular capillaries highly permeable
What does the filtration membrane do?
filters the blood so that the fluid from it moves across the filtration membrane and into the lumen of the Bowman’s capsule
Collectively, the capillary endothelium, basement membrane, and podocytes form the
A. filtration membrane.
B. glomerulus.
C. nephron.
D. renal corpuscle.
A. filtration membrane.
What type of muscle are both the afferent and efferent arterioles lined with?
a layer of smooth muscle
Juxtaglomerular apparatus
a structure made up of juxtaglomerular cells & the macula densa that secretes renin and plays an important role in filtrate (fluid from the filtered blood) formation and blood pressure
Juxtaglomerular cells
a ring of smooth muscle around the afferent arteriole
Macula densa
specialized cells of the distal tubule
After filtration in the glomerulus, urine formation takes place in the _____.
renal tubule
Proximal tubule
the first section of the renal tubule that is made of simple cuboidal epithelium with many microvilli for reabsorption/secretion
Descending limb of the loop of Henle
the second part of the renal tubule, now called the nephron loop, in which the first part is similar to proximal tubule then the latter part becomes thinner because it’s made out of simple squamous epithelium & H2O diffuses out
Ascending limb of the loop of Henle
a continuation of the nephron loop in which the first part is thin and made of simple squamous epithelium, like the descending limb, then becomes thicker and simple cuboidal epithelium replaces the simple squamous epithelium
Distal tubule
the last part of the nephron loop, that is made of simple cuboidal epithelium with very few microvilli, and is shorter than the proximal tubule.
What do the distal tubule and collecting ducts do?
actively reabsorbs Na+, K+, and Cl-
Collecting ducts
the convergence of many distal tubules that are made of simple cuboidal epithelium & form medullary rays that lead to papillary ducts
Vasa recta
special capillaries around the proximal and distal tubules that extend deep into the medulla and surround the nephron loops and collecting ducts
Circulation Through the Kidney (10 steps)
Arterial supply: heart → abdominal aorta
Renal artery
Segmental arteries
Interlobar arteries (ascend within renal columns toward cortex)
Arcuate arteries (branch and arch over base of pyramids)
Interlobular arteries project into cortex and give rise to afferent arterioles
Urine Formation
Afferent arterioles
Glomerulus
Efferent arterioles
Peritubular capillaries (form a plexus around proximal and distal tubules)
Vasa recta
Interlobular vein
Arcuate veins
Interlobular veins
Renal vein → inferior vena cava → heart
Ureters
tubes made of transitional epithelium through which urine flows from the kidneys to the urinary bladder
Urinary bladder
hollow muscular container made of transitional epithelium that is much thicker than the ureter wall because of the smooth detrusor muscle
What does the urinary bladder to expel urine?
contracts
Male VS female urethra
the male urethra is longer, extending through the penis VS the female urethra, which is shorter and opens into the vestibule anterior to the vaginal opening
Trigone
the triangular area between the ureters and urethra of the urinary bladder that expands less than rest of bladder because it is made of a different kind of tissue than the rest
Internal urinary sphincter
a ring of smooth muscle that prevents urine leakage from the urinary bladder, and in males, contracts to keep semen from entering the urinary bladder during ejaculation
External urinary sphincter
a ring of skeletal muscle that surrounds the urethra as it extends through pelvic floor and acts as valve to control the flow of urine
The micturition reflex (urination)
Urine in the urinary bladder stretches the bladder wall.
Action potentials produced by stretch receptors are carried along pelvic nerves (green line) to the sacral region of the spinal cord.
Action potentials are carried by parasympathetic nerves (red line) to contract the smooth muscles of the urinary bladder.
Ascending pathways carry an increased frequency of action potentials up the spinal cord to the pons and cerebrum, increasing the conscious urge to urinate.
Before 2-3 years of age, the descending pathways facilitate the reflex when stretch of the urinary bladder produces the conscious urge to urinate, reinforcing the micturition reflex. After, they carry action potentials to the sacral region of the spinal cord to tonically inhibit the micturition reflex, preventing automatic urination when the bladder is full.
The brain voluntarily controls the external urethral sphincter through somatic motor nerves (purple), causing the sphincter to relax or constrict.
What is the primary function of the kidney?
regulation of body fluid composition
The kidney sorts the substances from the blood for either _____.
removal in urine or return to the blood
What is the smallest structural component that produces urine?
the nephron
What are the steps filtrate goes through after leaving the renal corpuscle? (9 steps, with filtrate concentration and reabsorption percentages)
Approximately 180 L of filtrate enters the nephrons each day. The filtrate concentration is 300 mOsm/kg.
Approximately 65% of the water and NaCl in the original filtrate is reabsorbed in the proximal convoluted tubule. The filtrate concentration is 300 mOsm/kg.
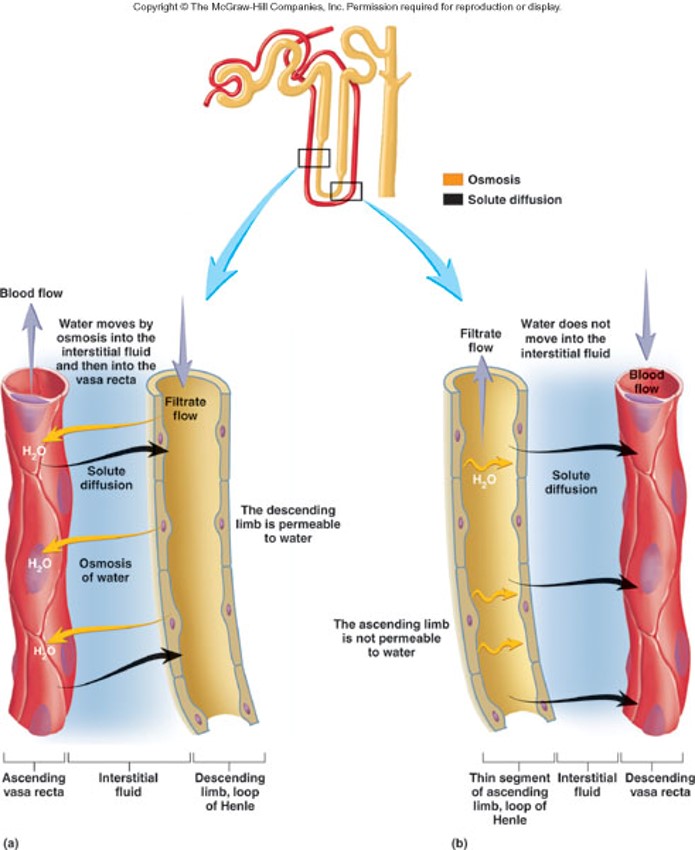
Approximately 15% of the water is reabsorbed in the thin segment of the descending limb of the loop of Henle. At the tip of the renal pyramid, filtrate concentration is 1200 mOsm/kg, which is equal to the interstitial fluid concentration.
The thin segment of the ascending limb of the loop of Henle is not permeable to water. Sodium chloride diffuses out of the thin segment.
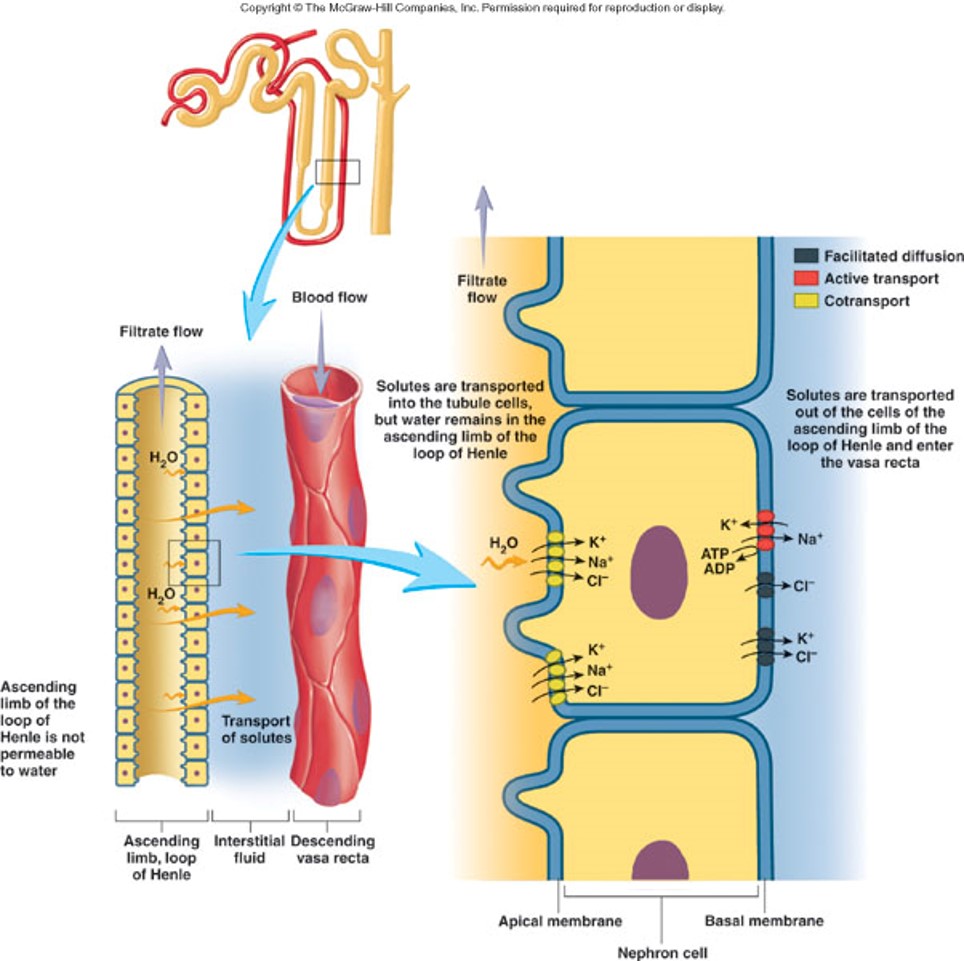
The thick segment of the ascending limb of the loop of Henle is not permeable to water either. But this time, sodium ions are actively transported into the interstitial fluid and Cl– follow by diffusion.
The volume of the filtrate does not change as it passes through the ascending limb, but the concentration is greatly reduced. By the time the filtrate reaches the cortex, the concentration is 100 mOsm/kg, and an additional 25% of NaCl has been reabsorbed.
The distal convoluted tubules and collecting ducts reabsorb water and NaCl.
If ADH is present, water moves by osmosis from the less concentrated filtrate into the more concentrated interstitial fluid. By the time the filtrate reaches the tip of the renal pyramid, an additional 19% of water and 9–10% of NaCl has been reabsorbed.
One percent or less of the filtrate remains as urine when ADH is present (see “Hormonal Mechanisms” later in this chapter).
What are the 3 major processes of urine formation?
Filtration: the movement of fluid across the filtration membrane into the Bowman capsule & glomerulus to form filtrate
Tubular Reabsorption: when solutes are reabsorbed (purple arrow) across the wall of the renal tubule into the interstitial fluid by active transport and cotransport & water is reabsorbed (orange arrow) across the wall of the renal tubule by osmosis. Water and solutes pass from the interstitial fluid into the peritubular capillaries.
Tubular Secretion: when solutes are secreted (green arrow) across the wall of the renal tubule into the filtrate
What forces filtrate across the filtration membrane?
pressure
What is the importance of filtration indicated by?
the large percentage of blood (cardiac output-CO) that is sent through the kidneys (the renal fraction)
What is the renal fraction equal to?
average 21% of total blood volume
Renal blood flow rate
renal fraction (21%) * CO (5600 mL/min) = 1176 mL/min
What is the renal blood flow rate often used to do?
to determine if the kidneys are functioning properly
Renal plasma flow rate
renal blood flow rate (1176 mL/min) * fraction of blood that is plasma (55%) = 650 mL/min
Filtration fraction
renal blood flow rate (650 mL plasma/min) * the amount of plasma removed from the blood when it’s filtered through the glomerulus (19%) = 123.5 mL plasma/min
Glomerular filtration rate (GFR)
the amount of filtrate produced each minute (125mL/min or 180 L/day)
Average urine production per day
the 1% of filtrate that is not reabsorbed into the blood (1-2 L)
Table 26.2: Calculation of Renal Flow Rates
Which of these is not a general process involved in the production of urine?
A. Absorption
B. Filtration
C. Secretion
D. Reabsorption
A. Absorption
What prevents blood cells and proteins from entering the lumen of the Bowman’s capsule, but allows H2O and small molecules to easily pass?
the filtration membrane
What 2 molecules enter the filtrate, then are reabsorbed and metabolized by the proximal tubule?
albumin and small hormone proteins
Filtration pressure
the pressure gradient in the renal corpuscle that’s responsible for the formation of filtrate, because it forces fluid from the glomerular capillary across the membrane and into the lumen of the Bowman’s capsules
What is the formula for filtration pressure?
Filtration pressure (10 mmHg) = GCP (50 mmHg) – CHP (10 mmHg) – BCOP (30 mmHg)
Glomerular capillary pressure (GCP)
outward pressure (BP) from blood pressing on the capillary wall, that forces fluid & solutes out of the blood into the Bowman’s capsule (approximately 50 mmHg)
Capsular hydrostatic pressure (CHP)
inward pressure from the accumulation of filtrate in the Bowman’s capsule (approximately 10 mmHg)
Blood colloid osmotic pressure (BCOP)
inward pressure due to osmotic force of plasma proteins in glomerular caps (approximately 30 mmHg)
Where is BCOP greater, and why?
at the end of a glomerular capillary, because more proteins are concentrated there
What are 3 blood flow conditions that result in high GCP?
High resistance in efferent arterioles (b/c vessels have a small diameter-constricted)
Low resistance in afferent arterioles (b/c vessels are dilated)
Low resistance in glomerular capillaries
Which of these cells or molecules in the blood normally cross the filtration membrane?
A. RBCs
B. WBCs
C. Amino Acids
D. Large Proteins
C. Amino Acids
REMEMBER: tubular reabsorption is
the return of water and solutes filtered from the blood at the renal corpuscle back to the blood (from nephron → interstitial fluid)
What 3 molecules leave the nephron and enter the interstitial fluid?
Inorganic salts
Organic molecules
Approximately 99% of the filtrate volume
What 8 solutes are reabsorbed from the lumen of the nephron to the interstitial fluid?
amino acids
glucose
fructose
Na+
K+
Ca2+
HCO3-
Cl-
What are 5 mechanisms of tubular reabsorption?
Diffusion
Facilitated diffusion
Active transport
Symport
Osmosis
Which tubule is responsible for the majority of reabsorption?
the proximal tubule
3 surfaces of the tubule wall cells
Apical surface (faces filtrate)
Basal surface (faces interstitial fluid)
Lateral surface (the surface between the cells)
What does the active transport of Na+ from the nephron to the interstitial fluid occur across, and what is it linked to?
the basal membrane, reabsorption of most solutes
What does the movement of Na+ from filtrate to the nephron occur across
the apical membrane
How do other substances, like ions or molecules, move from the filtrate into the nephron cell?
they symport by way of the energy provided by the Na+ concentration gradient
Once substances are transported through the apical membrane, how do they cross the basal membrane? (3 ways)
facilitated diffusion
symport
osmosis (water)
What limits the rate of transport in tubular reabsorption?
the number of carrier proteins
How does diabetes mellitus exemplify the limiting factor of the number of carrier proteins?
the concentration of glucose in the filtrate exceeds the rate of transport, resulting in a high concentration of glucose being left in the urine
What happens to the filtrate volume by the end of the proximal tubule in someone with diabetes mellitus?
it’s reduced by 65% due to osmosis
When the loop of Henle descends into the medulla, is the interstitial fluid high or low in solutes?
high
How permeable is the descending thin segment of the loop of Henle to water, urea, sodium, and other ions?
highly permeable to water
moderately permeable to urea, sodium, and other ions
By what percentage is filtrate volume reduced by in the descending thin segment of the loop of Henle?
another 15%
Permeability of the ascending thin loop of Henle
not permeable to water, but is permeable to solutes (tubule → interstitial fluid → vasa recta)
Osmole
A measure of the number of particles (atom, ion, molecule) in a solution
A milliosmole (mOsm) is
1/1000 of a osmole
Permeability of the ascending thick loop of Henle
not permeable to water or solutes, which allows Na+ to establish a concentration gradient via active transport on the basal membrane & K+ and Cl- to symport with Na+ on the apical membrane
What is the concentration inside the nephron by the end of the loop of Henle?
100mOsm/kg
What is the concentration in the interstitial fluid in the cortex by the end of the loop of Henle?
300mOsm/kg
Is the filtrate in the DCT or the interstitial fluid around it more dilute?
the filtrate (100 vs 300)
The ascending limb of the loop of Henle is __________ to water.
A. impermeable
B. moderately permeable
C. permeable
A. impermeable
Permeability of the distal tubule
variable, depending on the presence of ADH (but water moves by osmosis into the more concentrated interstitial fluid, at some degree, while solutes like Na+, Cl-, and H+ continue to be reabsorbed)
What effect does the presence of ADH have on urine volume and concentration?
ADH present: low volume, high concentration
ADH absent: high volume, low concentration
On what side of the nephron tubule does active transport take place during tubular reabsorption?
the basal surface
How much urea is passively reabsorbed?
walls of the nephron are not as permeable to urea so only 40%-60%
Why is the concentration of urate ions, creatinine, sulfates, phosphates, and nitrates high in urine?
because they are only partially reabsorbed