Exam 1: Infancy to Adolescence
1/152
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
153 Terms
International Classification of Functioning, Disability, Health (ICF)
Provide scientific basis for functional consequences of health conditions
Establish common language to improve communication amongst healthcare providers & general public
Coding system for diagnosis, documentation, health info systems
Permit comparison of data across countries, healthcare, disciplines, services, time
Body structures/functions, activity & participation, environmental factors
OTPF-4
Defines & guides practice/cornerstones of OT
OT's foundational document defining domains (areas of occupation) and processes to support engagement and participation in meaningful activities.
Articulates OT’s contributions to health & wellness through occupation
How do we use occupation? How does that fit into OT & helping our clients gain/regain a state of health & wellness? Designed for internal & external audiences
Domain of OTPF-4 (5 parts)
Occupation: ADL, IADL, sleep/rest, work, play, leisure, education, social participation, health management
Performance patterns: habits, routines, roles, rituals
Performance skills: motor, process, social interaction
Client Factors: values, beliefs, spirituality; body function & structures
Contexts: personal & environmental
An OTR observes a child jump on 1 foot. Which of the 5 areas of OT domain are they most likely assessing?
Performance skills: Motor skills
OT Process
Evaluation: finding out what client wants & needs to do; determining what they can do & has done; identifying supports & barriers to health, wellbeing, participation
Occupational profile & analysis of occupational performance, synthesis
Intervention: plan - identify goals & outcome measures, implement, review/re-evaluate
Outcomes: occupational performance, prevention, health & wellness, quality of life, participation, role competence, well-being, occupational justice; describe results clients can achieve through OT intervention
OT = Social & Medical Models of Disability
Recognize influence of environmental & social barriers on occupational participation
Social Model: context factors that create disability
Loss of function linked w/ health condition as an attribute of the social environment. Views disability as a socially created problem resulting from barriers in the environment & attitudes.
EX: One injured with a spinal cord injury becomes disabled NOT by the injury itself, but because they can’t access local stores, public transport, etc.
Medical Model: factors intrinsic to individual as source of disability
Disability is a feature of the person that requires medical care, professionals “correct” the problem. Views disability as a problem of the person that requires treatment/correction
Therapy clinicians identify impairments like weakness and develop strategies to improve one’s abilities or help them learn to compensate for the impairments (EX: One with a spinal cord injury is offered activities to strengthen muscles whilst being trained new ways to complete ADLs)
Infant Months: Trust VS Mistrust = Hope
0-3 mo: Early infancy
4-6 mo: Middle infancy
7-9 mo: Late infancy
10-12 mo: Transitional infancy
During infancy - 18 months, what’s the psychosocial crisis and virtue?
Trust: Learn to develop sense of trust when basic physical & emotional needs consistently met by caregivers (feeding, comfort, affection, safety)
Mistrust: difficulties w/ relationships & emotional regulation later in life
Virtue: Hope
Building trust through consistent, nurturing engagement in daily routines = foundation for healthy emotional & social development, secure attachment
OTs can support routines, sensory regulation, co-occupation (shared activities between infant & caregiver)

Early infancy, 0-3 mo: Gross Motor Skills @ 0 months
Fetal, flexed postures
Primitive reflexes

Early infancy, 0-3 mo: Gross Motor Skills @ 3 months
Lifting head in prone using antigravity extension
Midline, symmetrical postures
Hand to mouth: beginning of purposeful self-soothing & oral exploration
Looking at hands

Neonatal Infant Reflex: Rooting Reflex (Integration: ~3 mo)
Onset: Prenatal
Interested in head-turning
Stimulus: Stroke cheek
Response: Turn head toward stimulus, opens mouth
Purpose: Help locate breast/bottle for feeding
Problem if persistent: Interferes with eating, speech, midline head control

Neonatal Infant Reflex: Suck-swallow (Integration: ~2-5 mo)
Onset: Prenatal
Stimulus: Touch to lips or inside mouth
Response: Rhythmic sucking & swallowing
Purpose: Intake of nutrition
Problem if persistent: Neurological conditions, poor oral-motor control; difficulty transitioning to solids
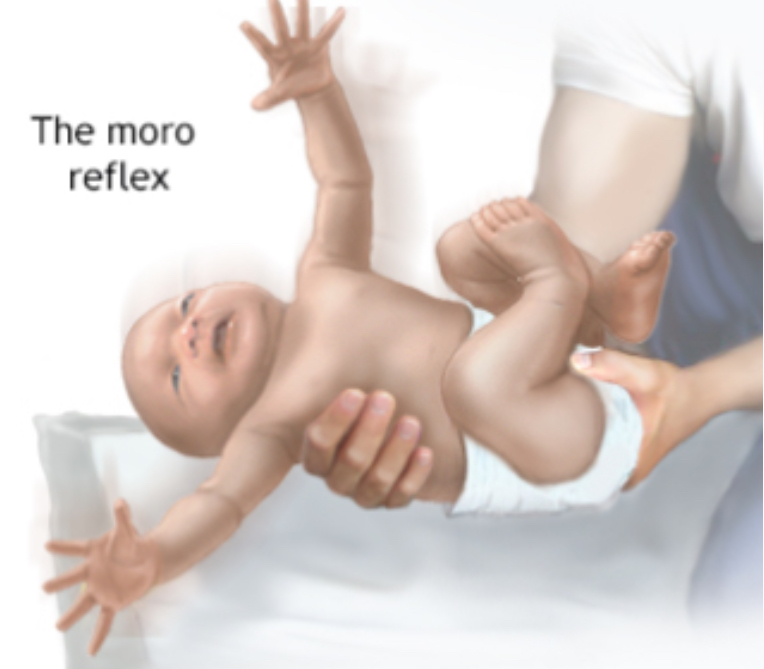
Neonatal Infant Reflex: Moro (Integration: ~4-6 mo)
Stimulus: Sudden head drop or loud noise
Response: Arms extend/abduct, then flex inward
Purpose: Protective/startle response
Problem if persistent: Poor sensory regulation, emotional reactivity, poor balance

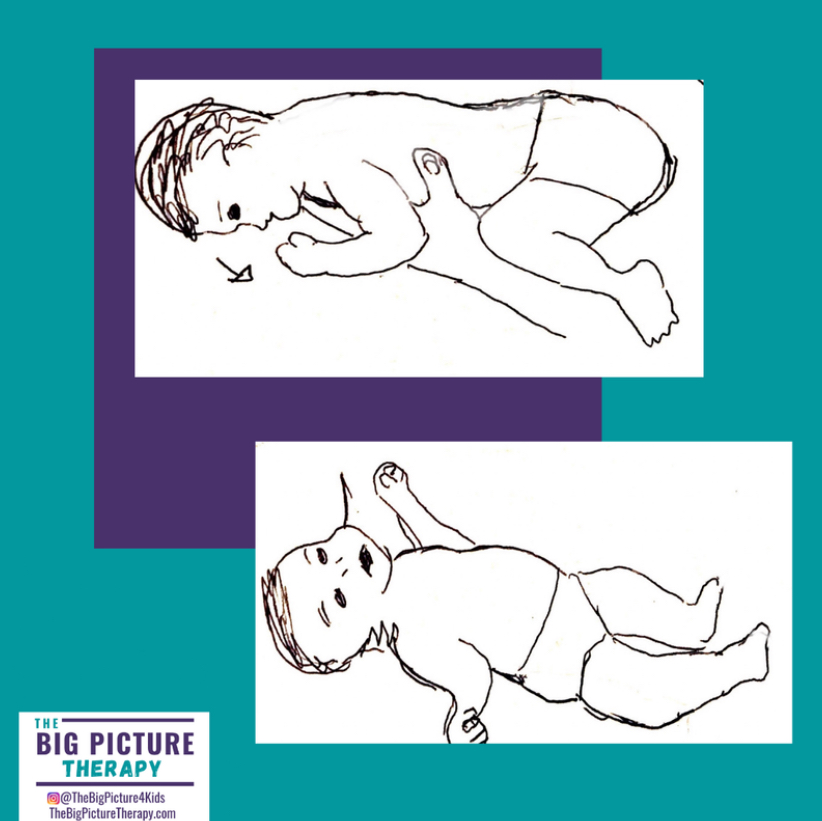
Neonatal Infant Reflex: Asymmetric Tonic Neck Reflex (Integration: ~4-6 mo)
Onset: At birth
Stimulus: Turn head to 1 side
Response: Arm/leg on face side extend, opposite limbs flex slowly
Purpose: Hand-eye coordination development
Problem if persistent: Difficulty with bilateral tasks, midline use, reading/writing, behaviors associated w/ ADHD


In the evaluation, the child demonstrates a retained ATNR. How would this present?
Rotation of the head to the right leads to extension of the right upper and right lower extremities
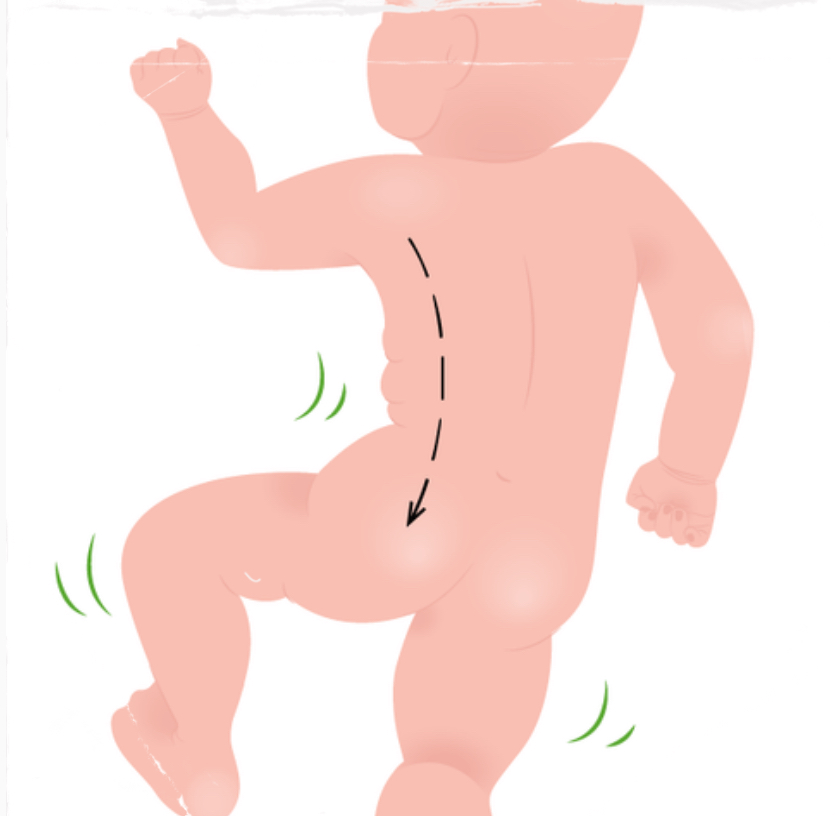
Neonatal Infant Reflex: Spinal Galant (Pre-natal onset, help get thru birth)
Stimulus: Stroke alongside spine (prone)
Response: Trunk curves toward stimulus
Purpose: Aids trunk movement for crawling, walking, birthing
Problem if persistent: Poor posture, fidgeting, bedwetting, attention issues
Neonatal Infant Reflex: Tonic Labyrinth Reflex (Integration: ~6 mo.; Onset: Birth)
Stimulus: Change head in position (prone VS supine)
Response:
Prone - body flexes
Supine - body extends
Purpose: Develop muscle tone, posture, balance
Problem if persistent: Poor head control, balance, delayed roll/sit, postural instability

Neonatal Infant Reflex: Palmar Grasp (Integration: ~4-6 mo.; Onset: Prenatal)
Stimulus: Pressure on palm
Response: Hand closes (grasp)
Purpose: Preps for voluntary grasp
Problem if persistent: Difficulty releasing objects, fine motor delays

When the OTR engaged the child by giving them a rattle to shake, they noticed that the child did not have a voluntary release of the object? Is this an expected behavior for a 12 month old child?
No, the palmar reflex is expected to integrate in late infancy (7-9 months)

Middle Infancy Milestones: 4-6 mo.
Anti-gravity behavior, postural control growth (holding head up in prone, bracing on 1 arm while reaching w/ the other)
Rolling over: belly to back first; increases independence & exploration
Hands to midline = brain lateralization, bilateral coordination
Palmar grasp, raking: purposeful grasp
Visually-guided reaching: reaching w/ intent
Middle & Late Infancy Milestones: 4-6 mo, 7-9 mo.
The Landau and Symmetrical Tonic Neck reflexes support?
Crawling
Postural balance
Protective responses as infants master voluntary movement & operate upright against gravity

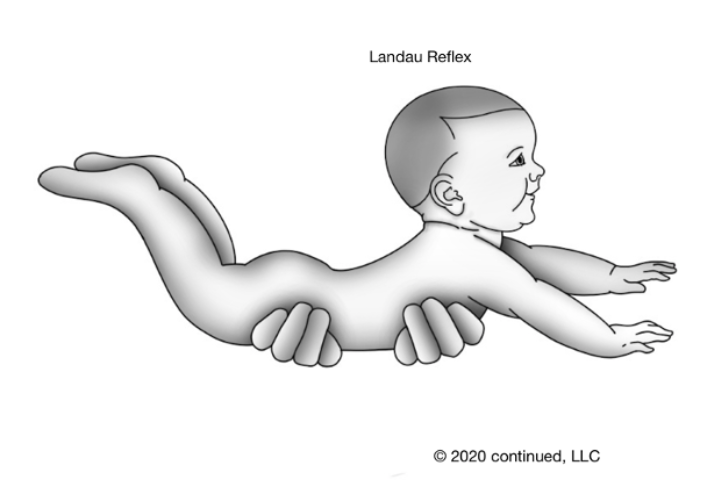
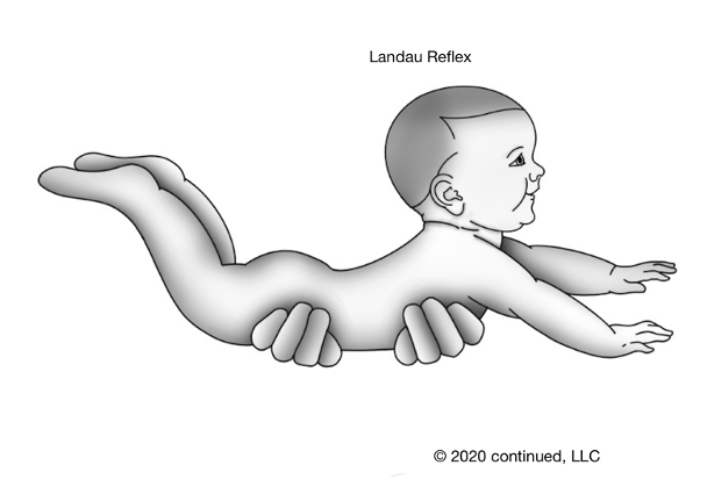
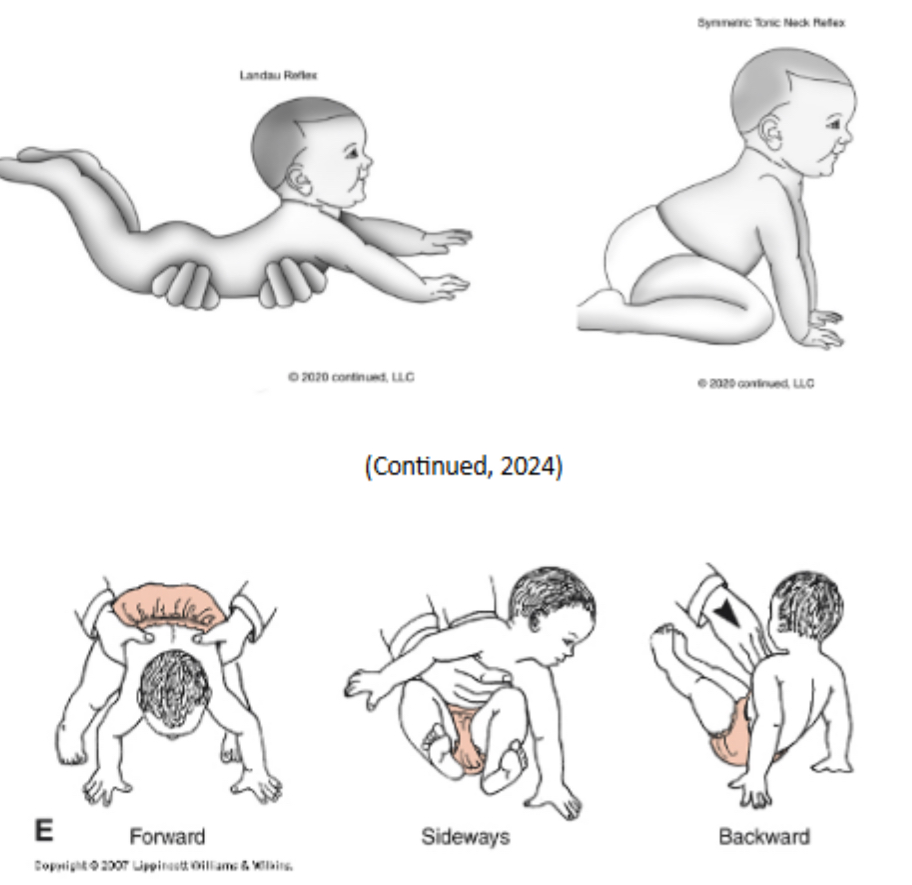
Middle & Late Infancy Reflex: Landau Reflex, Superman!
When held in horizontal prone suspension, baby extends head, trunk, & limbs
Supports: Anti-gravity posture, prone extension, trunk stability
Prepares for: Active play in prone & facilitates extensor muscle tone

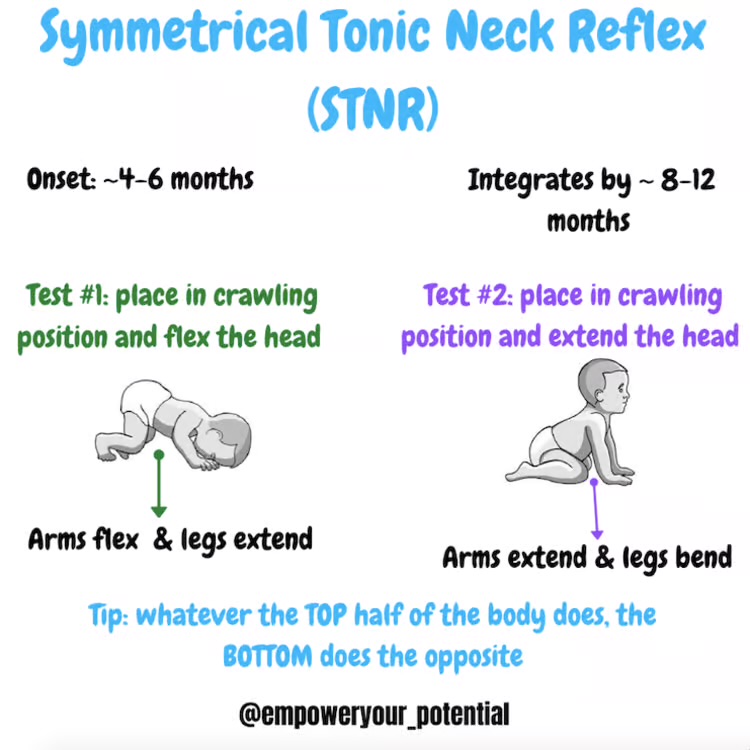
Middle & Late Infancy Reflex: Symmetrical Tonic Neck Reflex (STNR)
Triggered by neck movement
Neck Flexion (crawling): Arms flex, legs extend
Neck Extension: Arms extend, legs flex
Helps baby transition to independent sitting, begin quadruped positioning, dissociate upper & lower body to crawl
Integrated Reflexes
Normal developmental process when reflexes are absorbed into more complex, voluntary actions
Primitive, automatic movements are replaced by higher-level, voluntary control as the nervous system matures
Retained Reflexes
Involuntary movements continue existing beyond the typical 3-9 months instead of integrating into more complex, voluntary movements
Interferes with motor skills, learning, posture, sensory
How are reflexes different from righting reactions, equilibrium responses, & protective reactions?
Reflexes are basic, automatic responses to stimuli that are present from birth and integrated by early infancy...
Righting reactions, equilibrium responses, and protective reactions are more mature, voluntary-seeming postural reactions that emerge later and are maintained throughout life to help with balance and movement.

Middle Infancy, 4-6 mo: Labyrinthine Righting Reaction
Helps infant orient head & body in space + maintain head-body alignment
Vital for postural control & functional movement transitions (rolling, sit upright)
Emerges around 2-3 months of age; integrates by 24 mo.

Middle Infancy, 4-6 mo: Equilibrium Reaction
Maintain balance when body’s displaced by external force (being pushed)
Trunk adjustments & protective arm/leg movements to maintain or regain posture
Prep for standing, walking, fall prevention
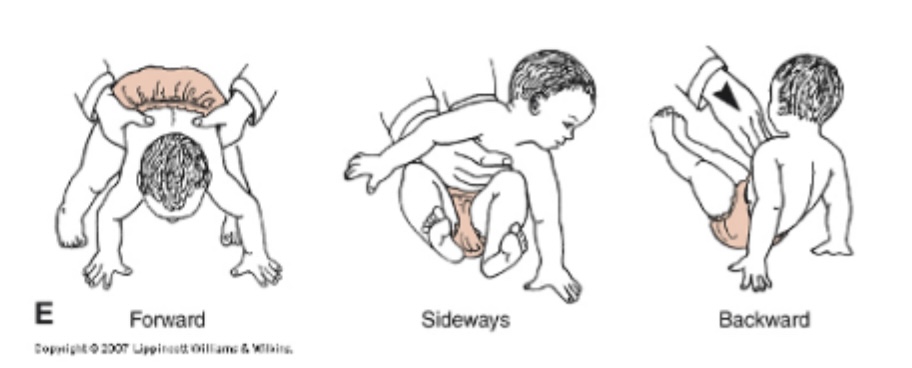
Middle Infancy, 4-6 mo: Protective Response, Parachute RXN 🪂
Prevent injury from falls/loss of balance; safety mechanism.
Forward protective extension: Baby reaches arms forward if falling face-first
Lateral protective extension: arms extend sideways when tipping
Backward protective extension: Arms extend behind to catch fall

Late Infancy: 7-9 mo, Motor Milestones “POP”
Prehension: Thumb differentiation & voluntary release; palmar grasp integrated
Oral: Manual self-feed, drink from sippy cup
Posture & Mobility: Sitting unsupported, lie-to-sit, crawling, bears weight on feet
Important for play, eating, exploration, social participation


Late Infancy: 7-9 mo, Social & Cognitive Milestones “ACL”
Attachment Behaviors: Protests separation, stranger anxiety (Ainsworth attachment & Erikson Trust vs Mistrust)
Cognition: Object permanence (Piaget, Sensorimotor Stage - birth to 18 mo.) infants understand objects exist even out of sight
Language: Reciprocal exchange & understand/respond to simple verbal cues
Knows familiar objects & words: Want milk!
Babbling, respond to words/sounds


Transitional Infancy, 10-12 mo, Milestones
Communication: 1-4 word vocab. Intentional words to express needs/familiar items
Motor skills - Walking
First steps (10-18 mo.)
Balance: leg strength, postural control
Standing: gross motor independence
Emerging pincer grasp
Use pads of thumb & index finger to pick up small objects like Cheerios
Self-feeding & fine motor precision

An OTR is evaluating an 18 month infant. When putting a toy in her hand, she grips it tightly but can’t let go to drop it in the bucket.
This behavior indicates: reflex retention of the palmar grasp due to difficulty releasing objects and fine motor delays
What occupation is disrupted: Play
Is this typical performance given child’s age: NO, the child is 18 months and should have integrated this neonatal reflex at around 6 months

The OTR’s motor milestone checklist for a 10-12 month old included all of the following EXCEPT:
First steps
Standing Balance
Rolling prone to supine (4-6 mo)
Neat pincer grasp

Transitional Infancy: 10-12 mo, Developmental Sequence
Timing & sequence of developmental milestone acquisition are used as key tools in assessing infants
Slow to acquire milestones = developmental delay
A 10-month-old infant is not yet crawling, but uses symmetrical rolling and shows normal muscle tone and posture.
This may be a motor delay, but development is otherwise typical.
Child demonstrates milestones out of sequence/qualitative differences in movement/behavior = abnormal development
A 10-month-old infant shows asymmetrical crawling, consistently using only one side of the body (e.g., left arm and left leg) and keeps the other side stiff or tucked.
This is a qualitative abnormality in movement, possibly indicating neuromotor dysfunction (e.g., early signs of cerebral palsy).
Toddlerhood (1-3 yrs): Theorists (6)
Gesell: Maturational Theory
Growth follows predictable motor & behavioral milestones
Piaget: Sensorimotor (Birth to 2 yrs) to Pre-operational (2-7 yrs)
Begin symbolic thinking & exploration thru play; centration/egocentrism
Vygotsky: Sociocultural Cognitive Development
Social interaction, guided learning, ZPD: caregivers’ role in skill acquisition
Ayres: Sensory Integration
Sensory processing key to motor planning & adaptive behavior
Erikson: Autonomy VS Shame/Doubt (18 mo-3 yrs) = Will
Seek independence, testing boundaries & developing self-control
Ainsworth: Attachment & Self-Regulation (Secure VS Insecure) = Early relationships
Toddlerhood (1-3 yrs): Gross Motor Milestones
Early, 1-2 yrs: Runs, climbs on play equipment, throws & kicks ball
Late, 2-3 yrs: Pedals a tricycle
Calibration: judges accurately
Force, speed, direction
Perceptual motor skills
Postural Stability
Balance, alignment, static VS dynamic, body axis rotation

Early Toddlerhood (1-2 yrs): Fine Motor Milestones
Uses tools
Marks w/ crayon
Bimanual tasks
Turn book pages 📚

Late Toddlerhood (2-3 yrs): Fine Motor Milestones
Snips w/ scissors ✂
Draws circle, traces
Builds tower >4 blocks
Strings beads


Toddlerhood (1-3 yrs): Visual Manual Skills
Discriminative Touch: Using touch to identify texture, shape, weight, temperature, etc. to accurately judge the object touched.
Haptic Perception: Combining touch and movement to understand objects without looking (uses discriminative touch plus memory of an object).
Bimanual Coordination: Using both hands together for stabilizing and manipulating tasks.
Precision Grasp: Refinement of fingertip grasp for small objects.
Hand Preference: Emerging hand dominance, becoming more consistent.


Toddlerhood (1-3 yrs): Language, Early Toddler (19-24 mo) 💬
Telegraphic speech: 2 word phrases “Lily tired”
First sentence
~12 words
Receptive (ability to understand) → expressive (ability to use words & sentences to communicate thoughts, needs, ideas)

Toddlerhood (1-3 yrs): Self-Care Skills
Adaptive skills, vary significantly by context
ADLs
Independent eating (mostly) 🥣
Assist in oral & toilet hygiene (imitate brushing teeth, may indicate need to go, attempts wiping) 🪥🚽
Assist in dressing (remove loose clothing, help push arms thru sleeves/legs) 👕
IADLs
Assist in household tasks (put away toys, mimic adult behaviors: wipe table) 🧸

Symbolic play is important in toddlerhood developmentally (emerges in 18-24 mo):
Language development: symbolic function
Decentering from self
Theory of Mind: enhances empathy & perspective-taking, understand others have different thoughts, beliefs
Engaging in roleplay helps children simulate & predict others’ mental states (ex: stick is magic wand)

Middle Childhood: 6-12 yrs, Overview
Children gain a better sense of self & culture beyond home as they become active participants in school & community
Increased independence & competence in ADLs and IADLs
Development of unique interests/personal expression through play/hobbies
Exploration of social world/virtual communities
Learn how to maneuver complex interpersonal and social worlds
Risks: bullying, stress-related issues, potential sport injuries
Those w/ developmental differences face increased challenge as children learn to compare themself with peers
Middle Childhood: 6-12 yrs, Theorists
Piaget - Concrete Operational Stage (7-11 yrs) 🥛
Organization & rational, logical thinking
Process environmental contexts logically
Begins to understand physics and conversation/classification/seriation (tall skinny and wide glass of water, same amount of water in both)
Erikson - Industry VS Inferiority [5-13; Virtue = Competency] (engage in meaningful occupation OR suffer in feeling inferior to peers)
Peer comparison, motivation from accomplishments
Collaboration & teamwork develop
Middle Childhood: 6-12 yrs, Neurological Development 🧠
Brain Development - Hemispheric specialization: dominance w/ various tasks
L: language & movement (Broca’s & Wernicke’s; rational & logical) 🗣
R: analyzing geometric shapes & elements (perceptual) ◼
Corpus callosum myelination improves processing: fatty covering sheath enabling efficient communication
Frontal & prefrontal cortex supports flexibility, reasoning
Middle Childhood: 6-12 yrs, Sensory Development
Visual acuity ~20/20 (see sharply unless visual deficit) 👀👓
Auditory processing → language comprehension, sound localization; improved sensory filtering
Process language
Hear/repeat/recall words, phrase, sequence numbers
Middle Childhood: 6-12 yrs, Physical Motor Development
Steady growth (2–3 in/year) 🤥
Stronger bones/joints (increased injury risk); calibrate & refined balance & postural control, coordination, timing, bilateral coordination, movement; handwriting improves; hand dominance solidified (~7 yrs).
Body composition
Increased muscle and skeletal mass to support greater height & weight, but is less abler to withstand impact
Refined balance and postural control; calibrate & refine movement (kick soccer ball) ⚽
Fine motor skills: finger dexterity, bilateral coordination, speed and dexterity increase, hand preference and dominance (cut scissors, write, throw) ✂
Middle Childhood: 6-12 yrs, Cognition/Mental Functions
Attention: greater focus, screens out distractions
Memory: working memory expands (5–7 bits, 15–20 sec); long-term memory grows 🧠
Perceptual: visual/auditory figure-ground, proprioception, stereognosis
Cognitive monitoring: self-checking and persistence with tasks
Cognitive maps: mental visualization and recall
Spatial & temporal awareness: body schema, timing, planning 🤔
Body schema: internalized sense of how much space my body occupies and the space around my body. “Will I fit through this tight space with my bookbag on?”
Temporal awareness: Passage of time as it relates to planning, sequencing, and altering movements. “How much time will it take to finish this snack so I don’t miss the bus?” ⏰🚌
Emotional function: self-regulation, self-concept, stress management (growth mindset important).
Asynchronous development: uneven growth across domains is normal; risk of “learned helplessness” (Repeated failures at a task that is not aligned with the child’s skills/context may lead to low confidence and task avoidance).

Adolescence (12+ yrs): Overview
Physical changes: brain maturation, increased physical development & need for sleep, puberty & sexuality, more complex motor & mental functions
Activities & participation: ADLs & IADLs, relationships, school & work, leisure
Prefrontal cortex HIGHLY connected w/ limbic system (emotions, memories) & striatal system (risk-taking)
Health issues: environmental factors, EDs, substance abuse, depression, anxiety
Romantic & family relationships
Adolescence (12+ yrs): Theorists (4)
Piaget: Formal Operational Stage (12+ yrs)
High symbolic thought & representation, appears when individual has been exposed to complexity in cognitive challenges; scientific & physics understanding, cause/effect
Erikson: Identity VS Role Confusion = Fidelity [13-21 yrs]
Importance of peer relations, separation from parents, tries out new roles, integration of previous resolutions
Freud: Genital Stage - awakening of sexuality
Resolution: sexual functioning, how adolescent relates to self & others
Gessel: Maturational Theory
All children go through the same stages of development in the same sequence. Growth progresses in a pattern
Each child moves through these stages at their own rate. Individual variation is normal.
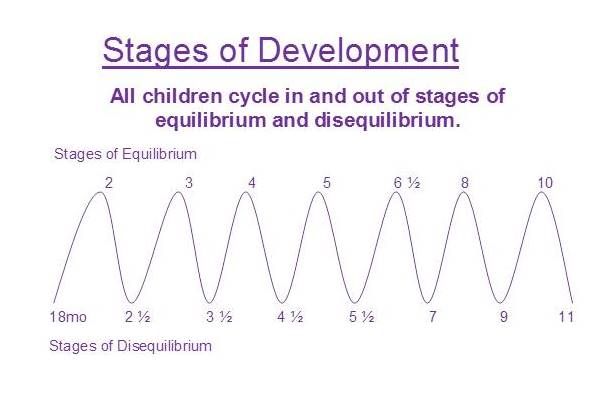
Equilibrium is followed by disequilibrium. Child can’t learn certain skills when their body and brain aren’t developed enough.
Skill regression is built into normal development! A child can start to do something good but can do it bad; continuous growth.
Established normative trends in motor, adaptive/cognitive, language, personal social behavior
A pediatric occupational therapist is evaluating a 12-month-old child referred for developmental delay. During the assessment, the therapist observes the child sitting independently, crawling, and beginning to pull to stand—but not yet walking. The parents express concern, as their friend’s child began walking at 10 months. The therapist explains that while some children walk earlier, others walk closer to 15 months. She assures the parents that the child is following a typical developmental sequence, and that individual variation in timing is normal. What theorist is this?
Gessel Maturational Theory
All children go through the same stages of development in the same sequence
Each child moves through these stages at their own rate
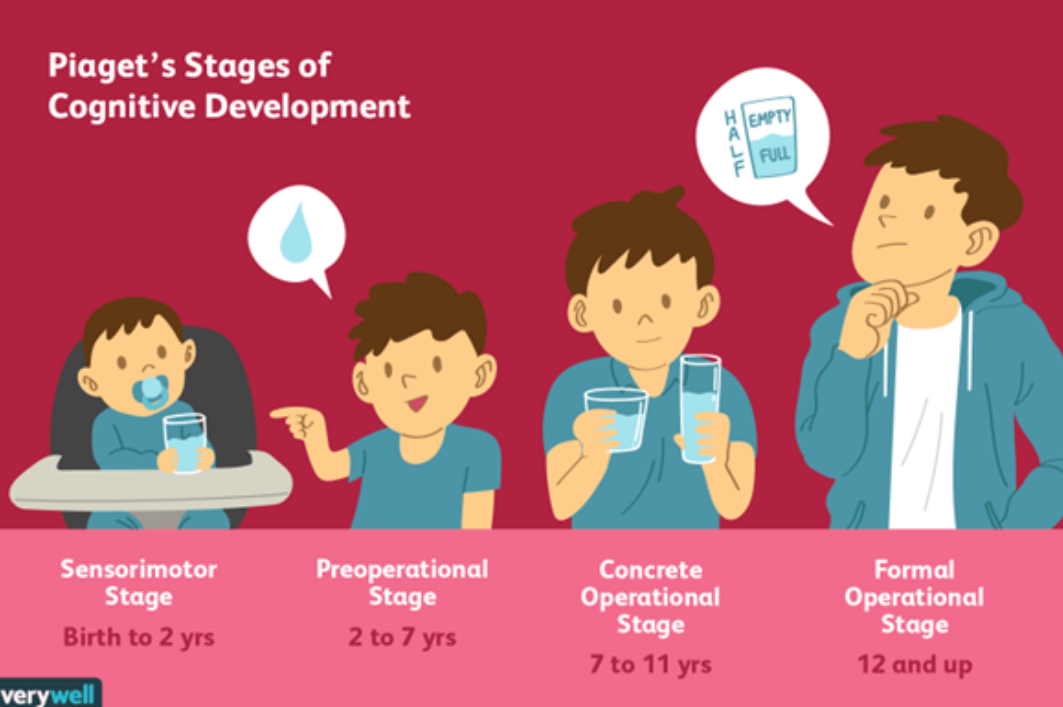
Piaget: Stages of Cognitive Development
Children’s thinking becomes progressively more advanced
Sensorimotor: birth to 18-24 months, object permanence, goal-directed action & cause-and-effect
Pre-operational: 2-7 years, symbolic thought (language, drawings, pretend play; egocentrism)
Concrete operational: 7-11 years, logical thought, conservation, physics, cause/effect
Formal operational: 12+ yrs, scientific thinking
Polly is 10 months old and cries when her ball rolls behind the couch where she can’t see it. She smiles again immediately after you hand her the ball.
Sensorimotor: birth to 18-24 months, object permanence
When her ball rolls out of sight, she cries because she knows it exists but can’t get it.
Object permanence: knowing objects continue existing when they can’t be directly observed or sensed
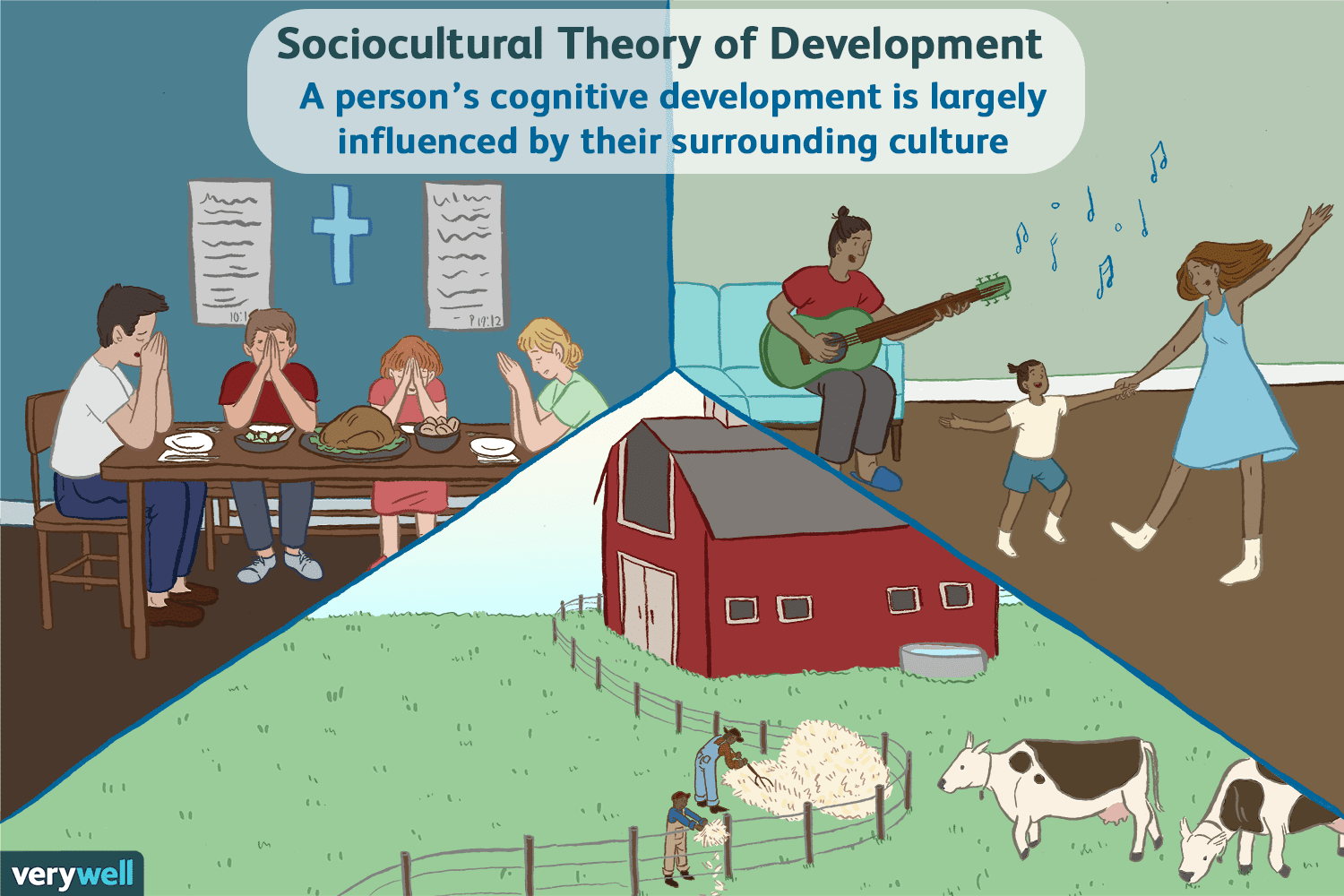
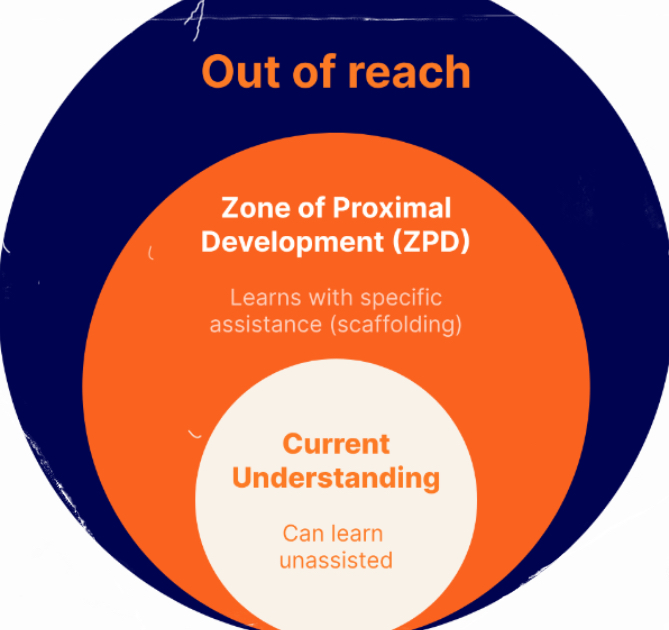
Vygotsky: Sociocultural Cognitive Development
Learning is a social process driven by culture and social interaction, where children learn through guidance from more knowledgeable others
Zone of Proximal Development: gap between what a learner can do without help and what they can achieve with guidance from a more knowledgeable person
Scaffolding: Learns w/ specific assistance/support from others
Private speech: talking to oneself; internalized mentally by 9
An OTR observes a 3 year old in daycare watching their teacher lace with beads to make a macaroni necklace using a 3 color pattern. The teacher lays out only 2 choices to help the child complete the pattern.
Vygotsky, Sociocultural Cognitive Development
Scaffolding: Learns w/ specific assistance/support from others
Zone of Proximal Development: gap between what a learner can do without help and what they can achieve with guidance from a more knowledgeable person
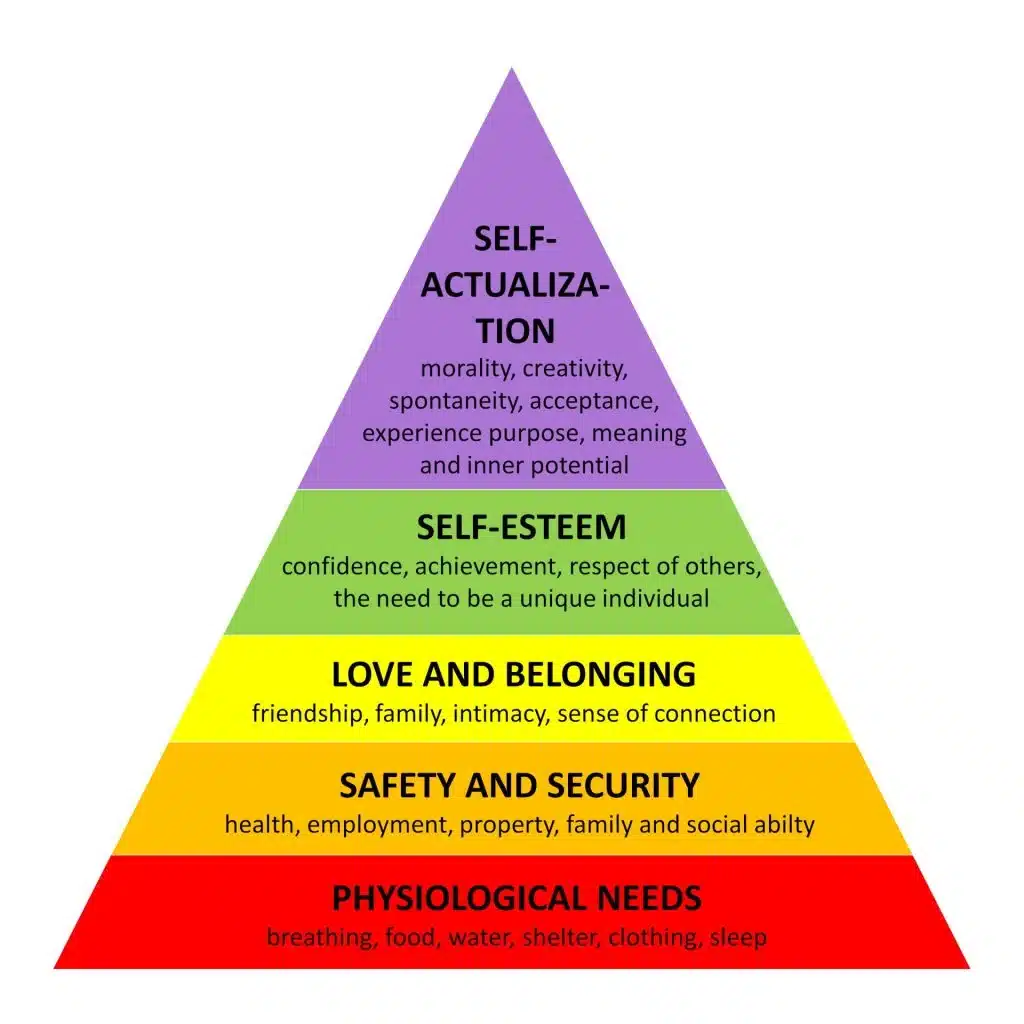
Maslow: Hierarchy of Needs
Person acts according to priority of needs at any given point in time. If basic need like food is denied, person will be obsessed w/ satisfying that need; if it’s available, they can seek higher-level needs
Self-actualization: Motivation to explore, play, learn; creativity & personal growth
Self-esteem: confidence, self-worth, encouragement to take initiative and engage
Love & Belonging: secure relationships w/ caregivers & peers
Safety & Security: emotional & physical safety @ home & school
Physiological Needs: sleep, nutrition, heath = foundation for attention & learning
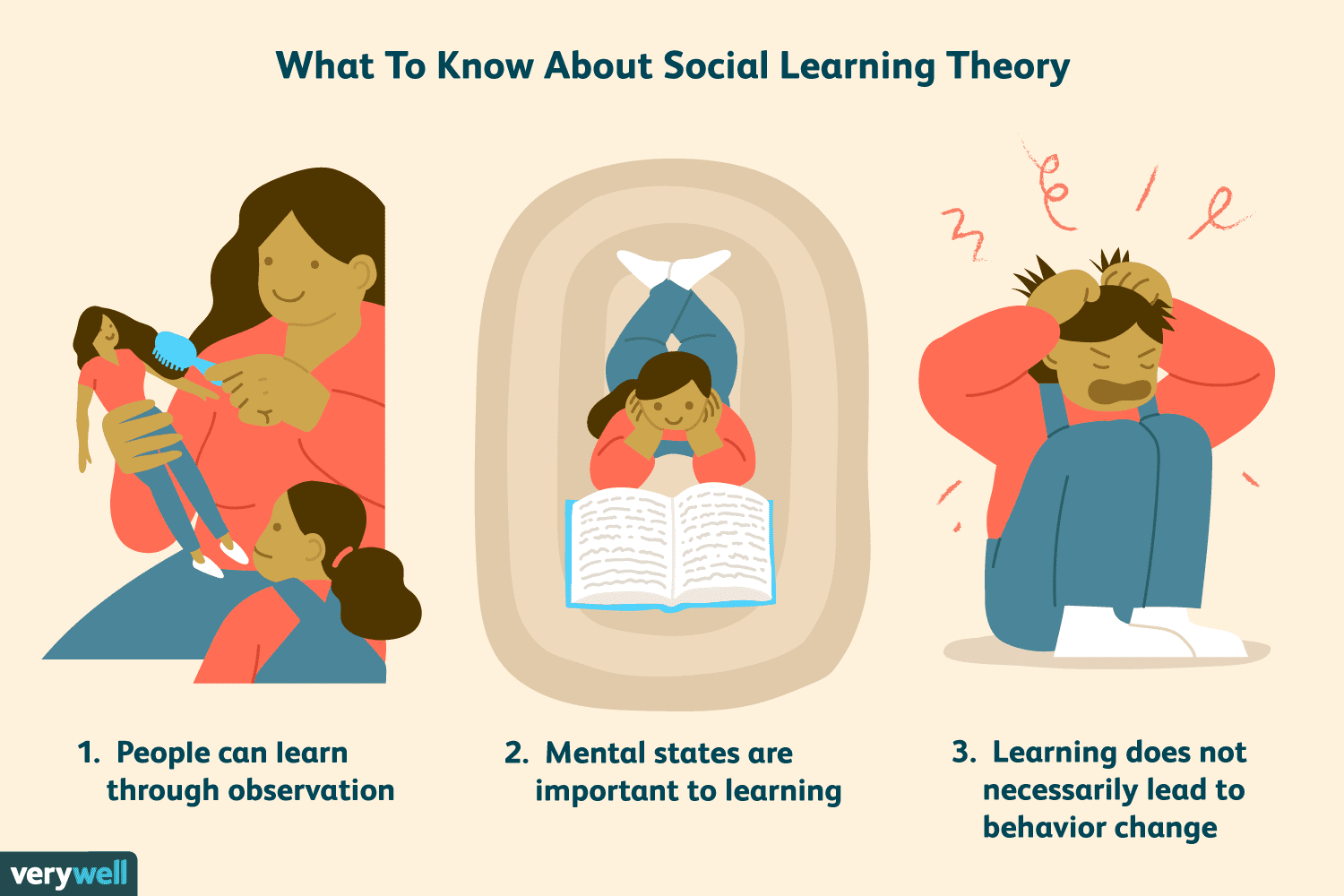
Bandura: Social Learning Theory
Learn through imitation/observation & modeling
Modeling: Observe others seen as ‘models’
Attention to model
Retention of past experiences
Ability to reproduce response physically
Motivation to produce response
Self-efficacy: one’s belief in ability to succeed in specific situations, influencing their motivation & performance
Vicarious reinforcement: observing others be praised, then imitating behavior


Ayres: Sensory Integration
The brain's ability to organize and interpret sensory input is essential for producing appropriate motor, behavioral, and learning responses.
Sensory Processing: The brain’s ability to receive, organize, and interpret sensory information from the environment and the body.
Key Sensory Systems:
Tactile: Touch and texture awareness
Vestibular: Balance, orientation
Proprioceptive: Body position-in-space, physical self awareness
Auditory: Sound processing
Visual: Sight and spatial awareness
Ainsworth: Attachment & Self-Regulation
Securely attached: seek to maintain proximity w/ caregiver, reacts negatively when she leaves. Upon return, the infant goes to her immediately. When mom is present, infants leave to explore the room, referencing back to her visually/approaching at intervals to ensure she’s there.
Avoidant: don’t seek proximity to mom, when she returns, ignores her
Ambivalent: seek contact w/ mom and distressed when she leaves, but when she returns they may display anger and resist comfort
Disorganized-Disoriented: show inconsistent behavior often self-contradictory; LEAST securely attached infants
An OTR observes a child in daycare protest their parent leaving, remain upset and dysregulated for 3 hours, and avoid the parent’s embrace upon their return.
Ambivalent: Seek contact with parent and distressed when she leaves, but when she returns, displays anger & resists comfort
When evaluating social interaction skills, the OTR notes the child does not seem to notice or protest when both mom and dad both leave the room? What theorist and concept is guiding the OTR’s evaluation?
Ainsworth, attachment theory, avoidant
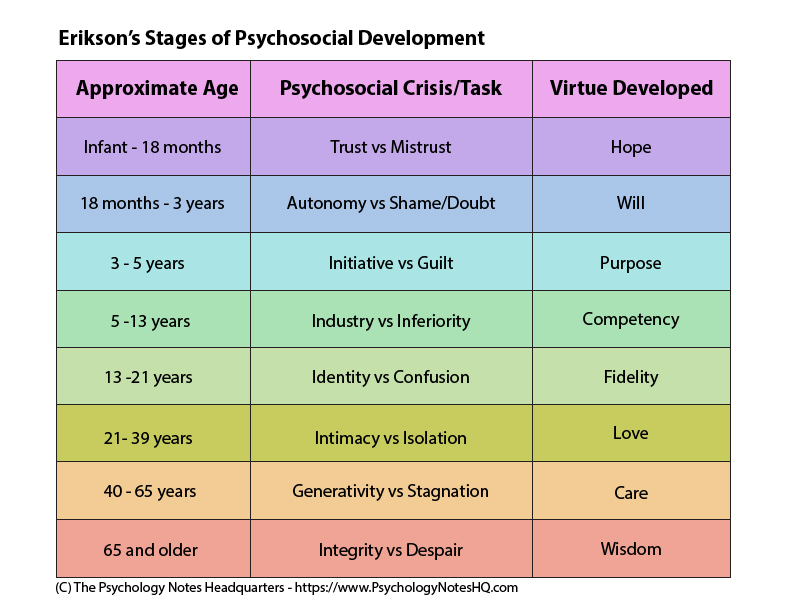
Erikson: 8 Stages of Psychosocial Development
Development is a series of conflicts/crises that must be resolved either in a positive or negative mode, determining future function
Infant - 18 months: Trust VS Mistrust; Hope
18 months - 3 years: Autonomy VS Shame/Doubt; Will
3-5 years: Initiative VS Guilt; Purpose
5-13 years: Industry VS Inferiority; Competency
13-21: Identity VS Confusion; Fidelity
21-39: Intimacy VS Isolation; Love
40-65: Generativity VS Stagnation; Care
65+: Integrity VS Despair; Wisdom
Preschool (3-5 yrs): Fine Motor Skills - Finger Dexterity, Translation
move object from palm of hand to fingertips & back to palm (paperclips)
Preschool (3-5 yrs): Fine Motor Skills
Bimanual coordination: Stabilize paper to cut w/ scissors
Oculomotor skills: eye movements and coordination needed for everyday tasks like reading, writing, and sports

Preschool (3-5 yrs): Fine Motor Skills - Graphomotor Skills
Conceptual/cognitive, visual perceptual, motor, somatosensory perception & perceptual motor skills in drawing & writing. At 5 yrs, can draw person w/ at least 6 body parts
Trace: eye-hand coordination to trace directly over lines on paper
Imitate: watch another draw a shape, then draw the shape
Copy: draw shape next to an example of the same shape
Create: draw intended shape without demonstration or sample to copy
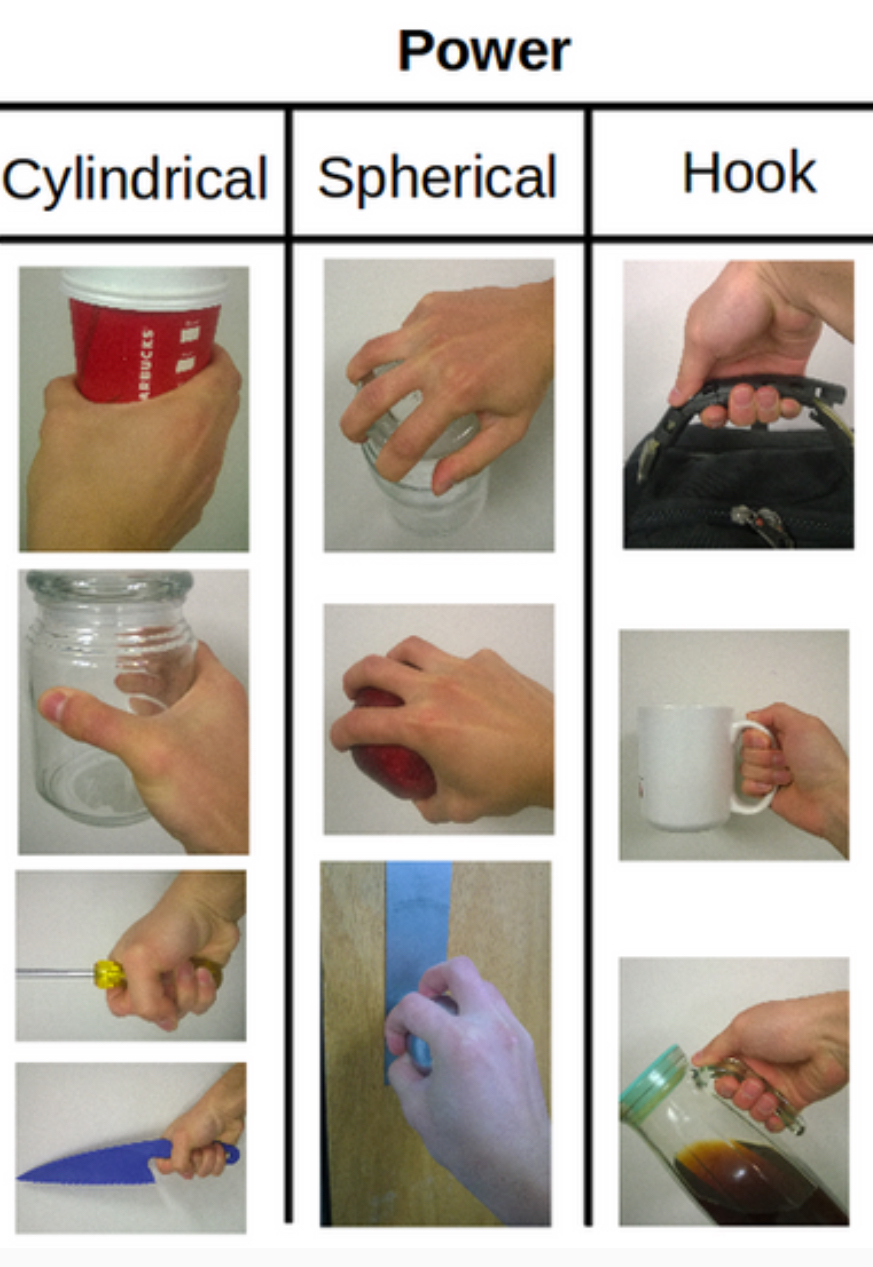
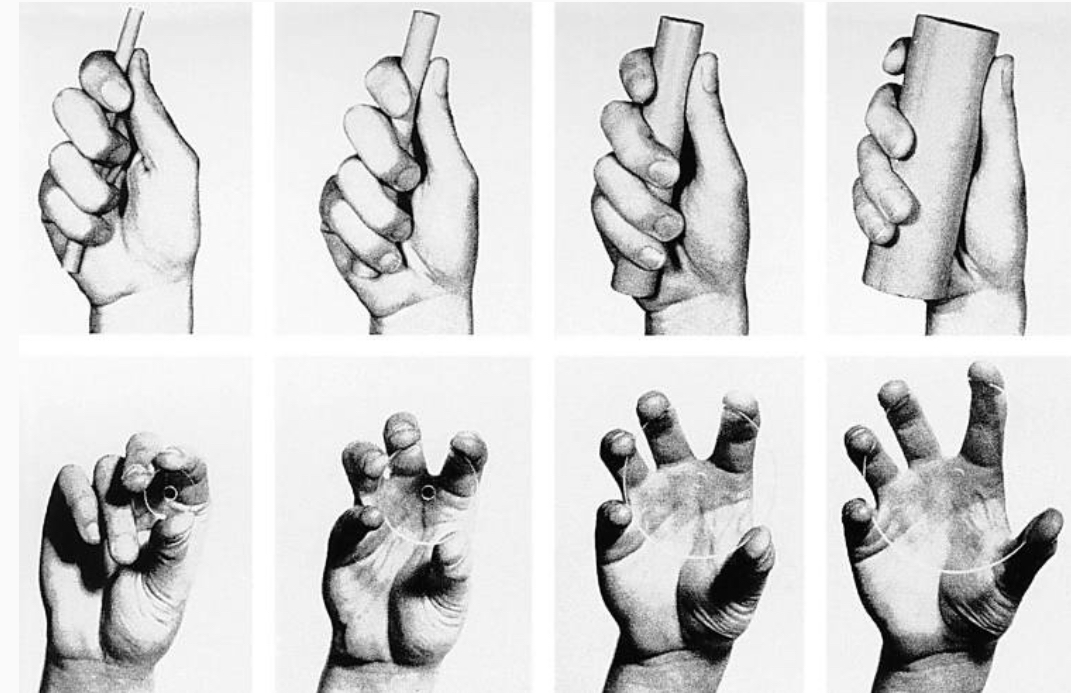
Power Grasps (1 year)
Object pulled into hand, rests on thenar muscles
Strong grip using partially flexed fingers and palm.
Thumb opposes the fingers, stabilizing object
All palmar surfaces (fingers and palm) involved in holding the object firmly.
Wrist typically in a neutral or slightly flexed position to maximize force generated by the larger extrinsic muscles of forearm
For holding or manipulating larger, heavier objects.
Cylindrical (go into palm), spherical (hold ball), hook grips (hold cup)
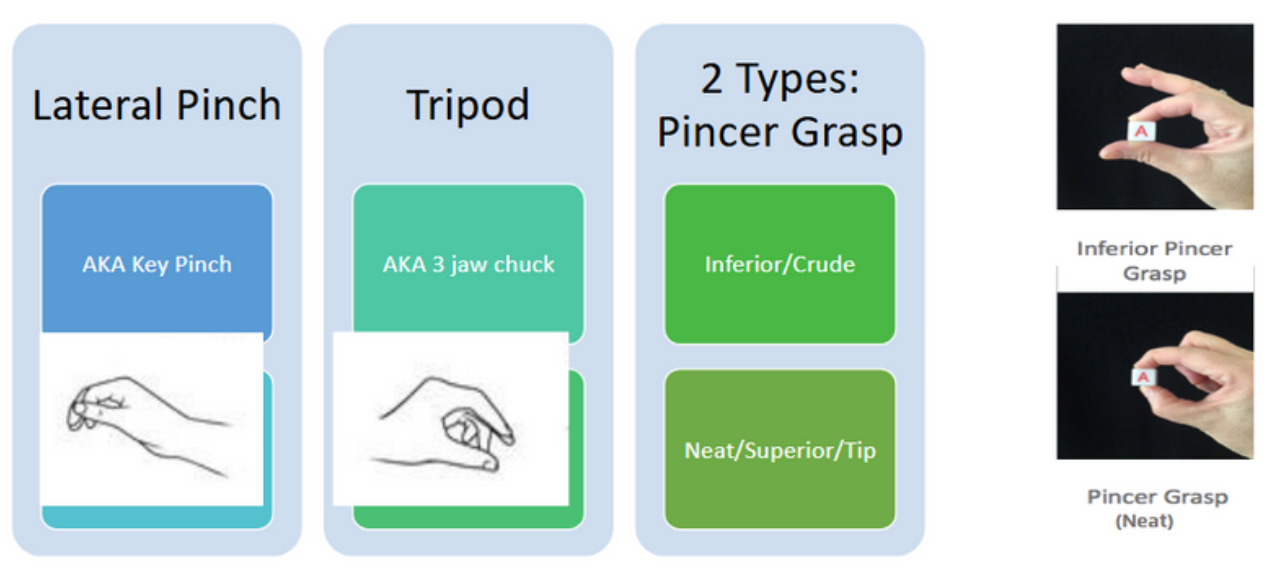
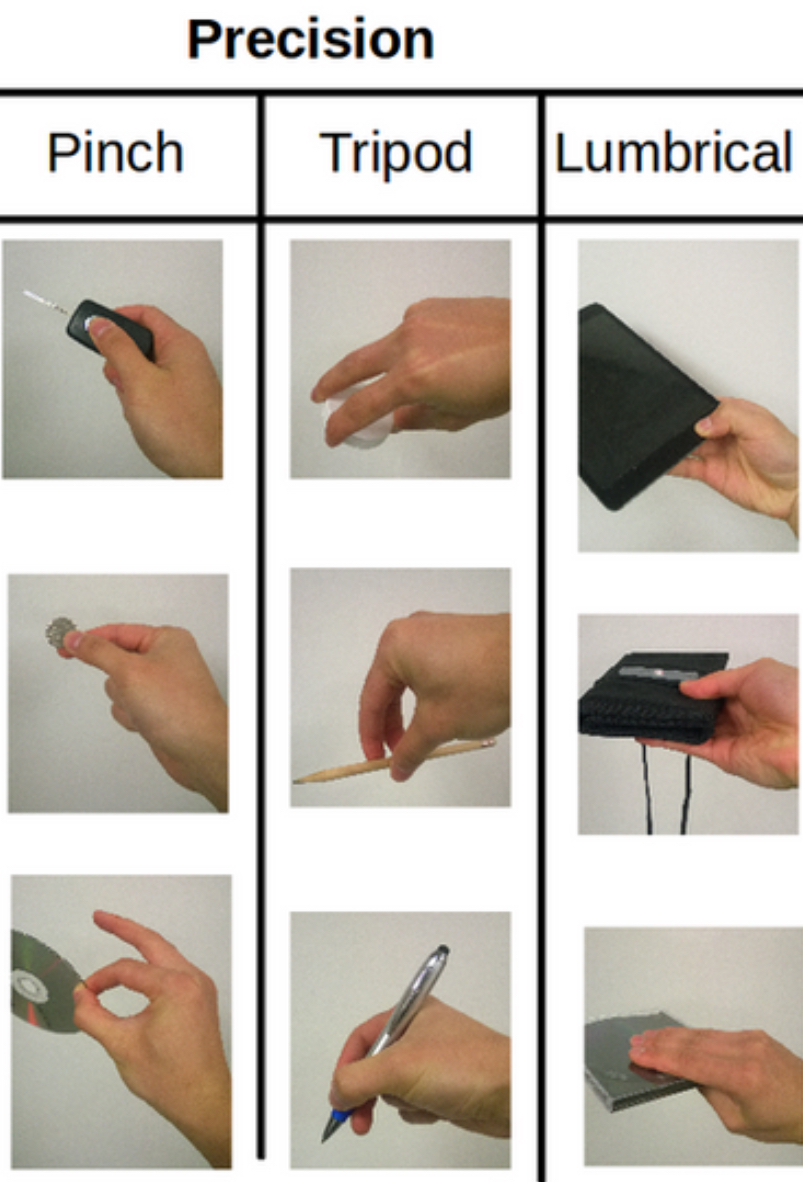
Precision Grasps (1 year): 3 kinds
Lateral prehension/key pinch: pad-to-side, key grip (turn car key ignition)
Tripod grasp: 3 jaw chuck, use all 3 fingers together - pencil
Pincer grasp: fingertips press against each other
Inferior/Crude: 8-9 mo. (use more pad, not as precise)
Neat, superior, tip: 10-12 mo. (all the way @ thumb, like threading needle)
Precision Grasps (1 year): Overview
Refinement period, all developed by 1 year age. Pre-school is for refinement, strengthening, coordination between 2 hands and practice.
Unsupported hand and active wrist extension
Thumb, index, and middle fingertips for fine control.
Thumb is in opposition, creating a tip-to-tip or pad-to-pad pinch.
Wrist usually in slight extension to optimize the use of the intrinsic hand muscles, allowing for delicate and precise movements.
Used for manipulating small objects or tasks requiring dexterity, such as writing or buttoning.
Pinch (key, disc), tripod (pencil), lumbrical

Pencil Grip: Pincer Grasp (10 mo)
Uses the thumb and index finger tips to pick up small objects
Important fine motor milestone, though not yet a pencil grasp.

Pencil Grip: Palmar Supinate (12-15 mo)
Whole fist wraps around the crayon or pencil, with the thumb on top
Forearm in Supination
Arm moves as one unit to make marks on paper.
Pencil Grip: Digital Pronate (2-3 yrs)
Fingers point down toward the paper, palm faces down in pronation
All fingers grasp the pencil, with the index finger extended down the shaft
Writing comes more from shoulder and elbow movement than fingers

Pencil Grip: Quadrupod (3-4 yrs)
Pencil held between the thumb, index, and middle finger, with the ring finger providing extra support
Increased control, though movement is still less refined.
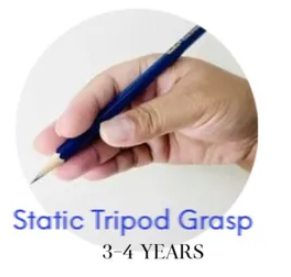
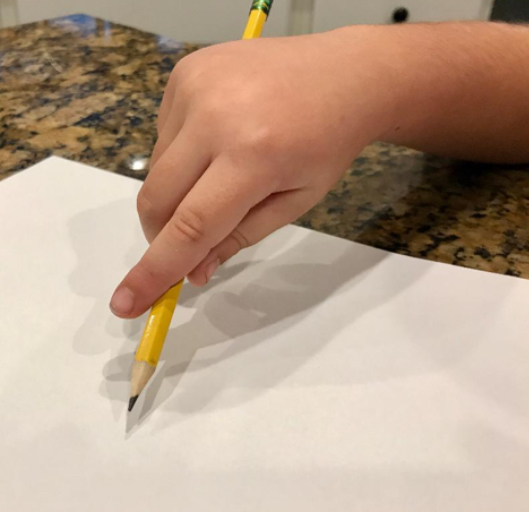
Pencil Grip: Static Tripod Grasp (3-4 yrs)
Pencil held with thumb, index, and middle fingers (three-point hold)
Fingers placed correctly, but movement is from the wrist or arm rather than the fingers (“static”)
Arm writing


Pencil Grip: Dynamic Tripod Grasp (5-6 yrs)
Mature pencil grasp: pencil held with thumb, index, and middle fingers, while ring and little fingers rest in the palm
Writing movement comes from small, coordinated finger movements instead of the whole arm
MOST efficient grasp for handwriting!
Open web space, 3 fingers, wrist in slight extension
Pencil rests on DIP of middle finger
Tip: Writing on a vertical surface puts wrist into extension (whiteboard)
Haptic Perception/Stereognosis 🪙
Discriminative touch combined w/ active memory of touch, texture, shape, temperature, volume/size, hardness, weight that allows children to tell you they have a penny in hand
Emergence of this parallels one of hand skills. Pairing of vision and touch sensations in brain lay foundation for development of haptic perception
Haptic exploration begins at 2 months when baby brings hand to mouth
Fine Motor Skills: Pre-school
Visual acuity: Ability to discern details when both person and target are static. Useful for reaching and grasping objects (basic hand skills needed in infancy + early preschool years)
Tested in standard eye exams, failure to correct issues hinder development of eye-hand coordination. As this develops, children experiment with hand movements and develop fine hand and eye control
Sharpness and clarity of your vision, typically tested by reading an eye chart from a specific distance. 20/20 = normal; clarity/sharpness of vision measured @ 20ft
Visual discrimination: ability to distinguish specific features of an object like shape, size, color. Precedes a child's ability to copy those forms in drawing tasks.
Visual scanning: short, rapid changes of fixation from 1 point in the visual field to another, used when searching for something and in reading
Rapid, jerky eye movements between 2 or more focal points
Visual pursuits: primary eye movements used in vision (tracking); slow, smooth movements used as the gaze follows a moving object
Short, rapid changes of fixation from 1 point in the visual field to another
Smooth, steady eye movement that tracks a moving object
Follow a ball in flight
Bimanual coordination
An OT is working w/ a preschooler on graphomotor skills. In the typical learning progression, which first step will the OTR have the child perform?
Trace: eye-hand coordination to trace directly over lines on paper
Lan is holding her pencil by wrapping all four fingers around one side and her thumb around the other. Further, you observe an open webspace with your wrist in neutral, as this grasp is a precursor to a tripod grasp. What type of grasp is this? At what stage is this a typical grasp?
Quadrupod grasp, 3-4 yrs

Why is play an important occupation developmentally?
Play is vital to learning & cognitive development; strong link between symbolic play & emergence of language. Enables children to operate within ZOPD. (Vygotsky, Sociocultural Cognitive Development)
Pleasurable activity, nervous system development, primary tool for learning
Adults can scaffold functional motor, social-emotional, language, executive functioning, math, self-regulation skills
Builds social-emotional resilience, executive functioning in adaptive behaviors at home, improves language & math skills, builds safe, stable, nurturing relationships to prevent toxic stress
Developmentally appropriate play w/ parents & peers promotes social-emotional, cognitive, language, self-regulation skills, and buffers against toxic stress
Supports formation of safe, stable, nurturing relationships with all caregivers
Enhances brain structure & function, promotes executive function (process of learning) to pursue goals & ignore distractions
Social Progression of Play
Unoccupied (0-3 mo): Play with body, discover how it moves
Solitary (0-2 yrs): play by oneself
Onlooker (2 yrs): child watches others play, may talk about it but don’t join in (often 1st type of social play)
Parallel play (2+ yrs): children play side-by-side, near each other, sometimes copy/mimic actions without direct interaction
Associative play (3-4 years): children play together & interact socially but without organized/cooperative efforts. Enjoy being w/ others, but focus more on social interaction than shared activity (jungle gym play, borrowing, showing toys)
Cooperative play (4+ years): children actively work together w/ shared goals or roles, showing interest in each other and activity
You notice a child watching with interest as 2 other children play in the sand box. What category of the social progression of play is demonstrated here, and at what stage would you first expect to see this behavior?
Onlooker play (2 years): child watches others play, may talk about it but doesn’t join in (often 1st type of social play)
Play type progression (A Baddie Only Starts Playing Games) 💅
Attunement: early social exchange (mutual gaze, facial expressions w/ caregivers) 🤰👶🏻
Body play (0-3+): gross & fine motor movement; build strength, coordination, body awareness; active rough & tumble activity
Object play, constructive (4 yrs): becomes more organized, with purposeful building and creation using materials like blocks, art supplies, or sand 🎨
Symbolic (begins 18-24 mo, late preschool): use objects, actions, ideas to represent something else (use stick as magic wand) 🍌
Pretense/sociodramatic: advanced symbolic play w/ role-taking & narrative; social interaction; playing family or doctor 🩺
Games with rules: simple, self-created, or loosely structured at first—requiring turn-taking, shared understanding, and emotional regulation. 🥅
What type of play most closely correlates with language development? 🍌
Symbolic play - subbing 1 object for another (banana as phone), suspends reality, imagines what’s not present
Language development
De-centering from self
Theory of mind: empathy & perspective taking
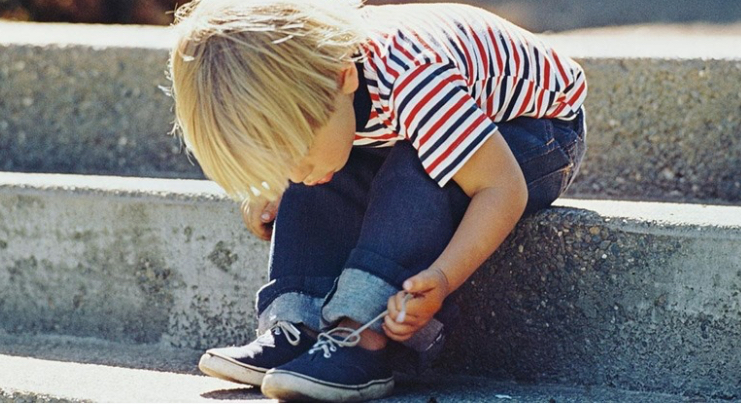
During an assessment, an OTR observes a child tying her shoes without assistance. What occupation is demonstrated here? At what stage does a child typically develop this skill (if culturally relevant)?
Occupation: ADL - dressing, 6-7 years old in middle childhood
A child is looking for the scissors in a messy drawer full of all types of art supplies. Which specific skill is required for this task? At what stage does this skill typically develop?
Visual figure ground develops in middle childhood (6-12 years). Ability to discriminate between the object of focus and the other objects that are also in view, using visual skills such as attention, visual memory, and other components of visual perceptual skills
Vital skill in reading, writing, learning, and retaining information 📖
Performance skill - Process skills: Searches/locates scissors (task object). Gather related task objects into the same work space.

Neurodevelopment: Toddlers (1-3 yrs) 🧠
Synaptic pruning begins in infancy, continues through childhood, refining neural connections by strengthening freq. used pathways & eliminating unused ones
Hemispheric lateralization (big increase during this stage): specialization of R & L brain functions, w/ L side dominating language processing
Myelination: enhances nerve signal speed, improving info processing, attention, cognition

Neurodevelopment: Pre-school (3-5 yrs) 🧠⬆
90% of adult size brain by 6 years; structural growth
More lateralization; handedness. Left hemisphere (language, academics) grows more dominant. Hand preference typically emerges by age 4, and true dominance by age 7.
Cerebellar-cortical connections growth, which supports refined motor control
Musculoskeletal: muscle size, power, stamina
Function: language, reasoning, calibration, fluidity, equilibrium, prehension

Neurodevelopment: Middle Childhood (6-12 yrs)
Hemispheric specialization: hand dominance (5-7); L hemisphere: language, movement, logic; R: shapes, perceptual abilities
Corpus callosum myelination: fatty covering sheath enabling efficient communication
Frontal + Prefrontal cortex growth: cognition, mental flexibility, rational thinking, higher level thought
Sensory development and refinement: inhibition, ability to focus, attention, memory, vision, kinesthetic function
Visual
Auditory
Higher level cognitive functions
Cognitive monitoring: persist in school tasks, cognitive sequencing/persistence
Cognitive maps: mental representations in brain
Spatial awareness: aware of own body, cues of depth and distance, body schema (how much space does my body occupy, and how much space is around it)
Visual-figure ground
Temporal awareness: passage of time in sequencing/altering movements (Do I have enough time to eat a snack before the bus comes?)

Neurodevelopment: Adolescence (12+ yrs)
Brain & Nervous System Development - Prefrontal Cortex Maturation
Limbic system: emotions & memories
Striatal system: risk-taking; activated by rewarding/novel stimuli
Developing prefrontal cortex highly involved w/ striatal system & limbic system, causing motor accidents, substance abuse, high-risk physical activities often associated with teens
Temporal discounting: common decision making pattern in adolescence that reflects immature executive functions; discounting potential long-term implications of a decision; focus on immediate rewards (accidental pregnancy, crime involvement, low educational achievement, drinking then realizing you must drive home
Mental Function
Memory: semantic memory - memory of concept & word meanings
Teens gain more experience about world, learn new concepts thru application
Reasoning: metacognition - self-evaluate; higher order reasoning; still lack of reasoning skills as seen in adults (not accurate perception of risks VS benefits)
Judgement: striatal system more sensitive, which skews judgment & reasoning
Motor control & flow, asynchronous skeletal growth
Pre-school Stage Occupations (3-5 yrs)
Play: Symbolic and imaginative play. Social play with peers (cooperative, parallel, and associative play). Rough-and-tumble and gross motor play
Self-Care (ADLs): Dress self completely, brush teeth, toilets independently, feeding, eating
IADLs
Cuts soft foods w/ knife
Sets table
Folds washcloths
Crosses street safely
Education: pre-academic skills (color, cut, early writing), follow routines & class rules, attend/participate in group activities
Social participation: interacting w/ peers and adults, develop communication & social problem-solving skills, learn to share, take turns, manage conflicts
Rest & sleep: establishing consistent sleep routines, managing transitions like nap time


Kindergarten Readiness
Motor/physical skills: gross motor control, fine motor skills to grasp tools, use utensils; perceptual-motor integration for early pre-writing tasks (color, cut); maintain postural stability & coordination
Cognitive skills: understanding of basic ideas like colors, shapes, numbers, spatial relations, multi-step directions, problem-solving
Adaptive skills: functional independence w/ age-appropriate ADLs and IADLs (toilet, dress, eating w/ basic manners, manage personal belongings); safety awareness in school environment (cross street, stay w/ group)
Social/emotional skills: self and co-regulation (follow rules, manage emotions, recover from stress); sustain attention in stimulating, distracting areas (sensory processing, attachment patterns); skills for sharing & turn taking
Communication skills: expressive, receptive, nonverbal to interact w/ peers and adults; ask for help, participate in group activities; good for peer relations, classroom participation, behavior regulation
Middle Childhood (6-12 yrs): Skills/Behaviors
Bullying, stress-related issues, potential sport injuries, interpersonal relationships, social referencing
Higher level cognitive functioning

Middle Childhood (6-12 yrs): Occupations
ADLs: independent in most by mid–middle childhood (e.g., shoe tying ~6–7).
IADLs: chores, money management (allowance, small jobs), digital literacy
Education: organization, exams, responsibility, identity, peer diversity
Play & Leisure: hobbies, sports, games (rule-making & rule-breaking, group play, conflict resolution).
Communication: adapt language to listener, maintain conversation, emotional expression.
Social Participation: independence from caregivers, peer importance, teamwork, role exploration, developing loyalty and values in friendships.
Adolescence (12+ yrs): Occupations
ADLs: hygiene refinement, appearance/attractiveness.
Community mobility: growing independence (driving, transport).
Identity formation: occupational identity, personal values.
Coping & resilience: adaptive vs. palliative coping; may involve “negative occupations” (substance use, disordered eating).

Adolescence (12+ yrs): Skills/Behaviors
Coordinated + sophisticated flow and motor control
More complex memory & reasoning, but reasoning & judgment still lacking
Temporal discounting for immediate reward, risk-taking behaviors
Reference group to form behaviors & habits, romantic and familial relationships, health issues (depression, EDs, substance abuse)
Autism Spectrum Disorder (ASD) 🧩
Challenges in social interaction, communication, and sensory processing.