l2o amnesia
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
what is amnesia + what does it affect
• Disorders of memory with preserved intellect and language. Severe forgetfulness.
• Difficult to keep a job, maintain relationships, look after oneself and maintain an independent existence.
two forms of amnesia
• Anterograde amnesia - a problem in encoding, storing or retrieving information that can be used in the future (antero). (future from the trauma/disease)
• Retrograde amnesia - a problem accessing events that happened in the past.
can look at amnesia from a variety of perspectives eg
-cognitive - deficits
-biological - localisation
-individual differences
most common cause of amnesia
Alzheimer's disease (AD)
Not a pure form of amnesia because usually complicated by additional symptoms of dementia.( which can have symptoms of problems of languge, thinkin, problem solving)
other causes of amnesia
• Korsakoff syndrome: usually from chronic alcoholism and is mainly characterised by a memory impairment. Frequently studied, relatively pure form of amnesia.
• Herpes simplex encephalitis: a virus of the brain which can leave individuals severely amnesic. Very rare. E.g. Clive Wearing.
• Temporal lobe surgery: individuals become amnesic as a result of deliberate surgical procedures. E.g. H.M.
differences in onset between different amnesia causes
-AD + Korsakoff syndrome have gradual onset
-herpes and temporal lobe surgery lead to precise moment of onset
HM (what happended + why)
• Epileptic seizures at 10.
• Quality of life extremely poor, surgery at 27.
• Removal of the MTL, including the hippocampi.
• Good news - no more seizures; bad news - profound
memory problems.
it was observed (several years after his surgery that... )
H.M.: "does not know where he lives, who cares for him, or where he ate his last meal. His guesses as to the current year may be off by as much as 43 years... In 1982 he did not recognise a picture of himself taken on his 40th birthday in 1966"(Corkin, 1984, p.255)
-first evidence hippocampus involvement in memory
HM -amnesia forms
• Anterograde deficit extremely severe. • Retrograde deficit extends back to age 16 (11 years before surgery). -this is in no way as a big an issue
types of memory preserved in amnesia
-STM
-procedural memory
-implicit memory
STM preserved
e.g. digit span (Baddeley & Warrington, 1970).(HM could, but mintue or two after stopping rehearsal forgets
procedural memory preserved
e.g. mirror drawing task (Corkin, 1968). Mirror-reading, 3 daily sessions and retention 3 monthslater.
Cohen & Squire (1980).(kosaff synndrome- pretty similar to controls )
implicit memory preserved
a person's behaviour is influenced by a
previous experience despite not being consciously aware of it.
• Claparede (1911) handshake.
-would shake amnesia patients hands, one day put pin in hand, next day she refused but could not explicitly articulate why
• Warrington & Weiskrantz (1968) degraded pictures/words.
Same stimuli at a later time - marked improvement. Same for H.M. (Milner et al., 1968). (on right)
• Graf et al. (1984) given a list of words to read
(e.g. METAL). Either asked to recall the word
shown previously (explicit) or generate the
first word that comes to mind (implicit) e.g.
ME___. Only explicit impaired, implicit normal.
two bases/processes in episodic memory
• Typically episodic memory tasks use free-recall or recognition.
• According to dual-process models of memory two distinct bases for memory performance: ? (recollection and familiarity)
-with free recall you need recollection whereas for recognition task you could use either
amnesiac - recollection vs familiarity study (1 guy) CHECK
Performance on the Doors and People test by Jon and 2 controls. Baddeley et al. (2001)
-Jon is a developmental amnesic had since very early on), lack of oxygen in birth negatively affects hippocampus (anoxia)
-no clear deficit in recognition but is a ProFund when in recall
-specifically seems to be recollection.
Jons results
• Jon. Problems teaching him the R/K distinction. (remember know paradigm)
• After he declared he understood. He was tested.
• Used R/K categories as often as controls but unable to explain the basis of his R decisions. (eg I remember thinking about this)
• Used a strength rather than a recollective criterion. (made mental image, how strong it was, this is not correctly using the rk paradigm just looking at strength)
• Lacked the 'remember' component in an ERP study of memory (Duzel et al., 2001).(left pareital old new effect)
• Same deficit using a different task (PDP)
amnesiac - recollection vs familiarity study (type of patients) ADD?
Hypoxic patients
Yonelinas et al. (2002). 56 cardiac arrest patients, 55
healthy controls + other patients with hippocampal and other MTL damage.
-Hypoxia is low levels of oxygen in your body tissues
Yonelinas et al. (2002). results
-hypoxic patients issues with recollection not familiarity ( whereas other damage (hippocampal/mtl) both)
dual process model of memory - bio
Aggleton & Brown(1999)
-look at more bio areas of this -Hippocampus -recollection -Perirhinal regions - familiarity
dual process controversial as....
-There are hippocampal amnesics who have deficits in recall and recognition. e.g. papers by Squire.
Also dispute as to whether there are two processes: R & F or whether they just reflect strong versus weak memory traces.
testing retorgrade amnesia
• Need to test items learned prior to the onset of amnesia. Researcher has no control over the learning. • Scales have been developed to test a range of events: news, winners of classic horse races, TV shows...
-can give them questions based inn stroy lines etc if they know idividuals previous interests
• Probe method: river (recall a personal memory and then date it). •
Autobiographical Memory Interview (AMI).
Autobiographical Memory Interview (AMI).
Koppelman et al. (1990) developed
Ask participants to remember specific information from a range of time periods e.g. the name of their first school. Then recollect a specific personal event from the period. (scored based on what info + how specific)
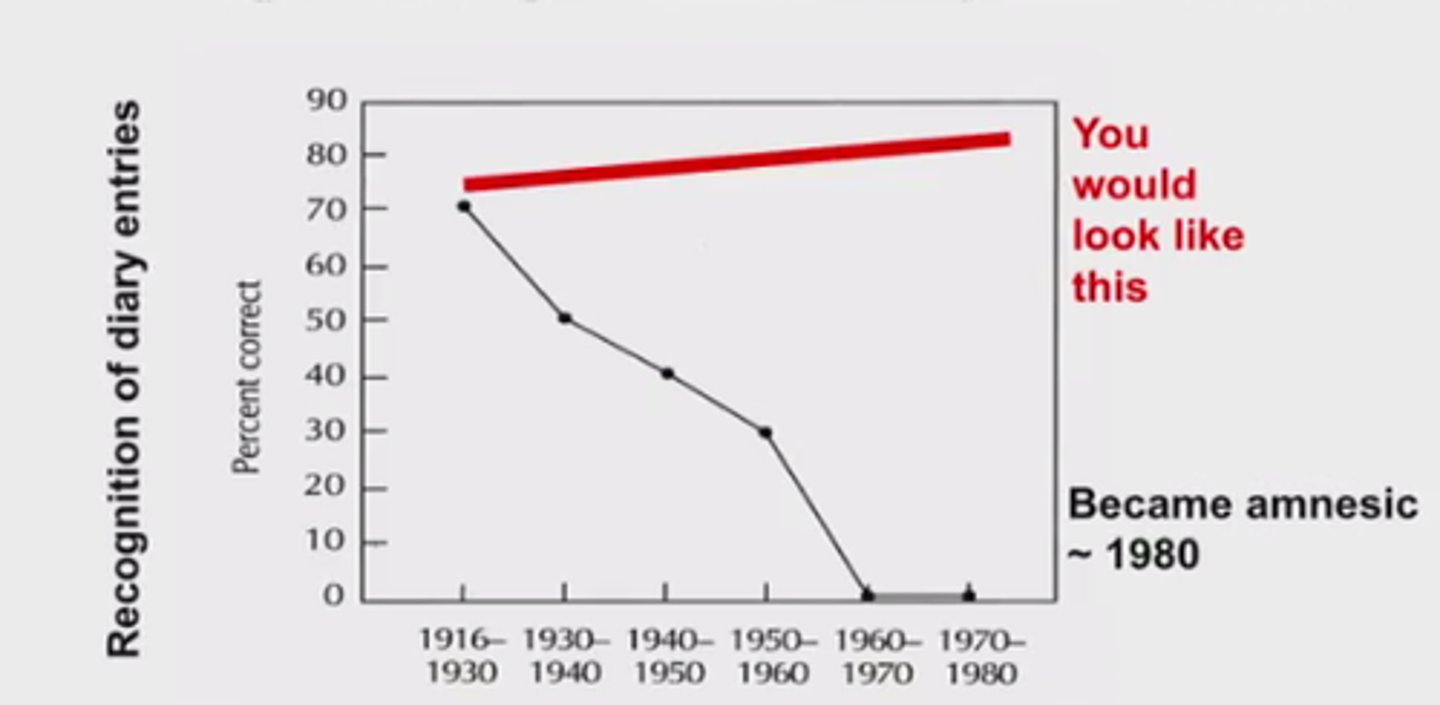
Temporal retrograde amnesia gradient
• For those with retrograde amnesia memories from earlier in life are easier to recall than those later on (Ribot's law).
amnesiac memoir case
Butters & Cermak (1986) report the case of P.Z.
-completed memoir before onset amnesia
ribots law Looks like an acute onset of amnesia.
However PZ had a history of alcohol abuse going back 35 years, could there be a progressive impairment in ability to register new memories?
- hard to retireve something if had impaired ability to encode it originally
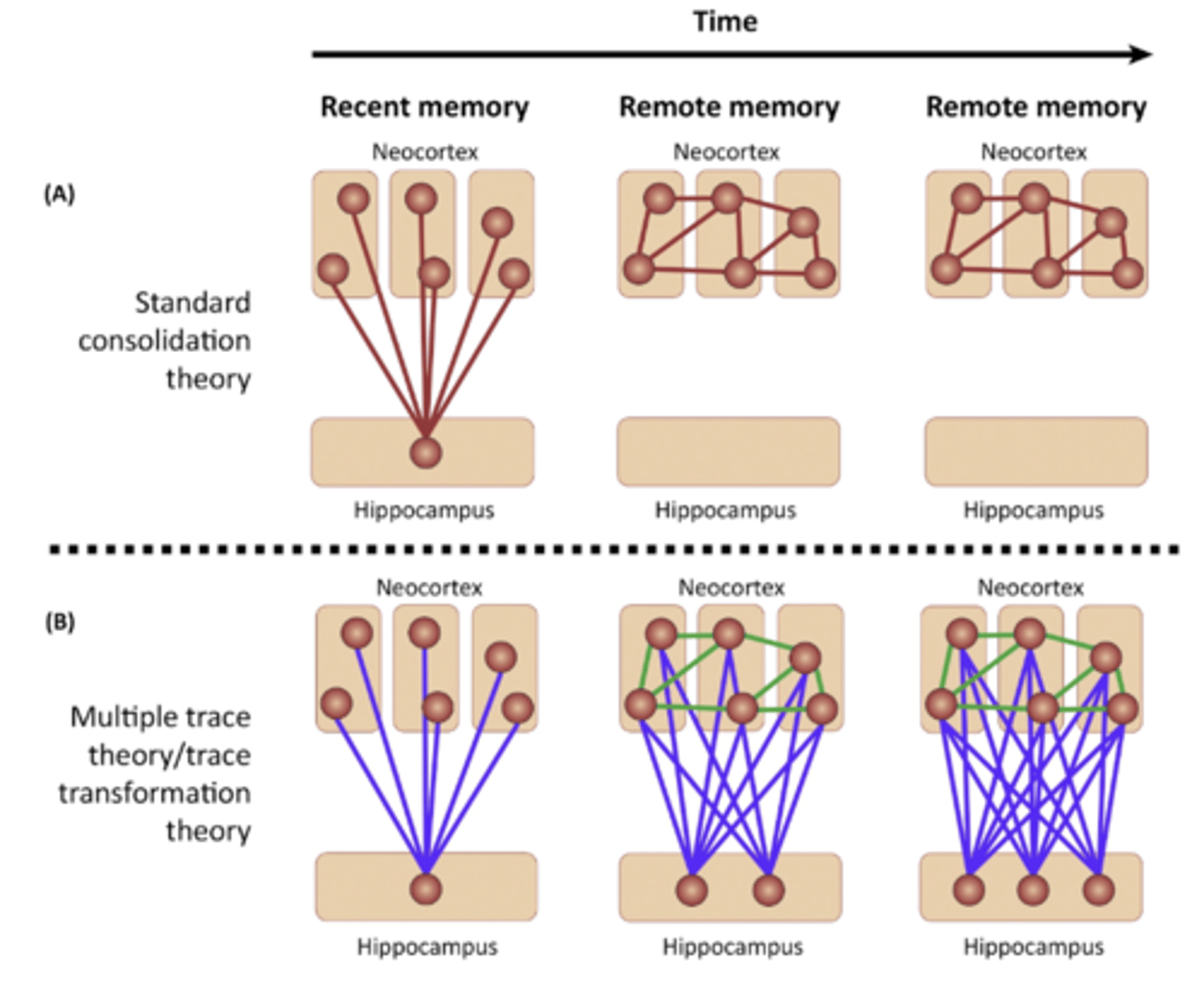
Explanations of retrograde amnesia (RA)
• Standard consolidation models e.g. Alvarez & Squire (1994)
• Multiple Trace Hypothesis e.g. Nadel & Moscovitch (1997;1998)
• Standard consolidation models e.g. Alvarez & Squire (1994)
• Assume information is consolidated by transferring it from one brain region to another (i.e. system consolidation).
-when experience somethings activates different cortical areas e smells, sounds etc
-no connection between areas at this point
-major method of consolidation is reactivation - when hippocampus reply's the neural activity associated with memory
-regions in cortex become connected
-eventually these cortical connections become stronger so more long term when we try to retrieve the memory we don't need the hippocampus
-explains Ribot's law as early memories don't require the hippocampus
• Multiple Trace Hypothesis e.g. Nadel & Moscovitch (1997;1998)
(B) Multiple trace theory states that a hippocampal-neocortical trace (left, blue lines and red spheres) is always required for a detailed episodic memory (middle, blue lines and red spheres), with repeated retrieval of this memory increasing the number of these permanent hippocampal traces (middle and right, red spheres). The intrinsic neocortical connectivity that emerges over time (middle and right, green lines) supports memories of a more factual and semantic nature that have been derived from repeated recall
-more robust against hippocampals damage because there are more connections and different pathways in hippocampus
Semantic memory of amnesias
• At first sight, no; amnesics retain knowledge of vocab and the world.
• Semantic deficits can result from dementia but what about damage to MTL?
• H.M. tested on ability to retrieve lexical knowledge (Kensinger et al., 2001).
Picture naming, spelling, ability to generate irregular word forms (e.g. Every day I dig a hole. Yesterday I ____ a hole). Performed within 1 SD of matched controls. • However, this knowledge acquired very early in life and generally early childhood memories are found to be well preserved in amnesic patients (Ribot's law).
evidence for deficits in acquiring new semantic knowledge in patients with MTL damage.
• H.M. unable to define words introduced since the onset of his amnesia e.g. Jacuzzi.
• The amount of damage to MTL corresponds to the magnitude of deficits in acquiring new semantic info (Verfaellie et al., 2000).
• H.M. can learn new info when it is anchored to premorbidly acquired knowledge. However less consistent access to semantic representations and learning can decay after a relatively short period of time (Skotko et al., 2004).
-doesn't happen normally need repition more exposures and not s consistent
-so may be small deficit
Developmental amnesia. deficits
Relatively preserved acquisition of semantic knowledge but profound episodic memory deficits e.g. Dzieciol et al. (2017), N = 18. • Why the difference? Because damage happens early in life is there a functional reorganisation of the brain?