PERSONALITY (EXAM #3)
1/98
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
99 Terms
What is Personality Judgement?
Attempts to accurately perceive other people’s traits
What we all do
Using your intuition, friends, family, etc
Based on stereotypes
What is Personality Assessment?
“Professional” personality research
What personality psychologists do
Using validated measurement systems
Personality Judgement VS Assessment
“Amateur” personality research VS “Professional” personality research
What is the general correlation between self and other judgments?
r = .20 - .40
People who know you well (friends, family, partners) are more accurate because:
they have a higher quantity and quality of information
Judgments by "close friends/family"
observed you across multiple environments (work, home, social) rather than just one setting
What is the general correlation between close others (friends/family)?
r = .49
What are weak siuations?
hanging out at home where your true personality is more likely to emerge
What are strong situations?
like a job interview, you are not able to read someone where they are masking their true selves
What are the challenges to accuracy?
Self-presentation biases
Deception
Basing trait inference off of state observation (observable actions or emotions)
What are self-presentation biases?
Motivated, often unconscious, strategies used to control how others perceive us
What is deception?
Actively hiding a trait or lying about their behavior
What is the idea of basing trait inference off of state observation?
Interpreting an individual’s immediate, observable actions or emotions to infer enduring personality traits
States VS. Traits
A temporary, situational behavior (ex: being "Stressed at Work" or "Happy at a Party")
Fluctuates
VS.
A consistent, enduring pattern (ex: being "Consistently Outgoing")
Stable over time
Accuracy is determined by:
The Judge
The Target
The Trait
The Information (Data)
Who are Good Judges?
People who assume positive traits
Agreeable, consistent, and content
Not anxious, power-oriented, or hostile
Who is a Good Target?
Some people are easier to judge than others
What you see is what you get
Transparent in thoughts and feelings
Low in self-monitoring
Extraverted, agreeable, conscientious, and emotionally stable
What are Good Traits?
Some traits are easier to judge people on than others
More visible
Self-other knowledge asymmetry (SOKA model)
Ex: Extraversion vs. Rumination
What is Good Information?
More information (data) is better than less
Better when across multiple domains
Quality: Better is better
How long does it take to make an accurate judgment about a person?
As short as TWO seconds
What is Self-other knowledge asymmetry? (SOKA model)
Less visible = higher self-accuracy (anxious)
Ex: You are the most accurate judge of your own anxiety or self-esteem. While you might appear confident to a "Friend," only you know if your internal state is actually one of worry or doubt.
More visible = higher other-accuracy (talkative)
Ex: Friends are often more accurate judges of your intelligence, wit, or rudeness
What are Thin Slices?
Very quick inferences about the state, characteristics or details of an individual or situation with minimal amounts of information
Very brief observations of faces/behavior
These judgments are often nonconscious, automatic, and intuitive.
Judgments based on thin-slicing can be as accurate, or even more so, than judgments based on much more information.
Can be as accurate as ones made after months of interaction
Body language is a stronger indicator of personality than verbal communication
Thin Slices: Familiar VS. Unfamiliar Interactions
Involves the subject interacting with someone they know (a friend or partner). This slice reveals how a person acts when they are comfortable and their "baseline" personality is on display.
VS.
Involves interacting with a stranger. These slices are often better for seeing social skills, anxiety, or "first impression" traits. Because the situation is new, the subject's behavior is more reactive, revealing how they navigate social uncertainty.
How are people able to make such accurate personality judgments from thin slices?
Fusiform Face Area (FFA)
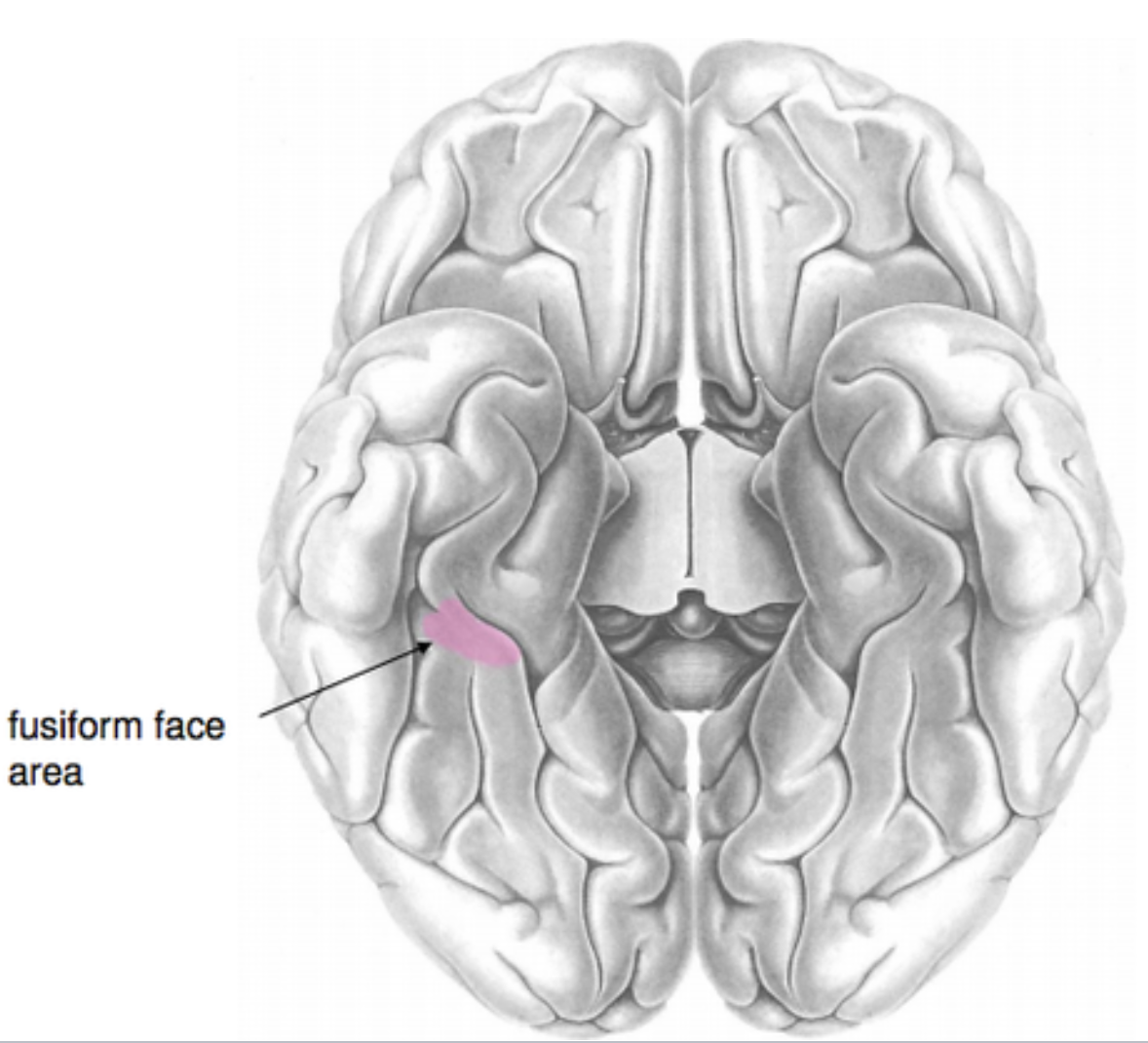
What is the Fusiform Face Area (FFA)?
A dedicated "module" in the human brain specifically evolved to process faces.
A neural function that is hard-wired to prioritize and rapidly decode social information from faces.
It recognizes identity, emotional expression, and social cues.
face processing is automatic and lightning-fast
The FFA allows us to bypass slow, analytical thinking and move straight to a social "gut feeling"
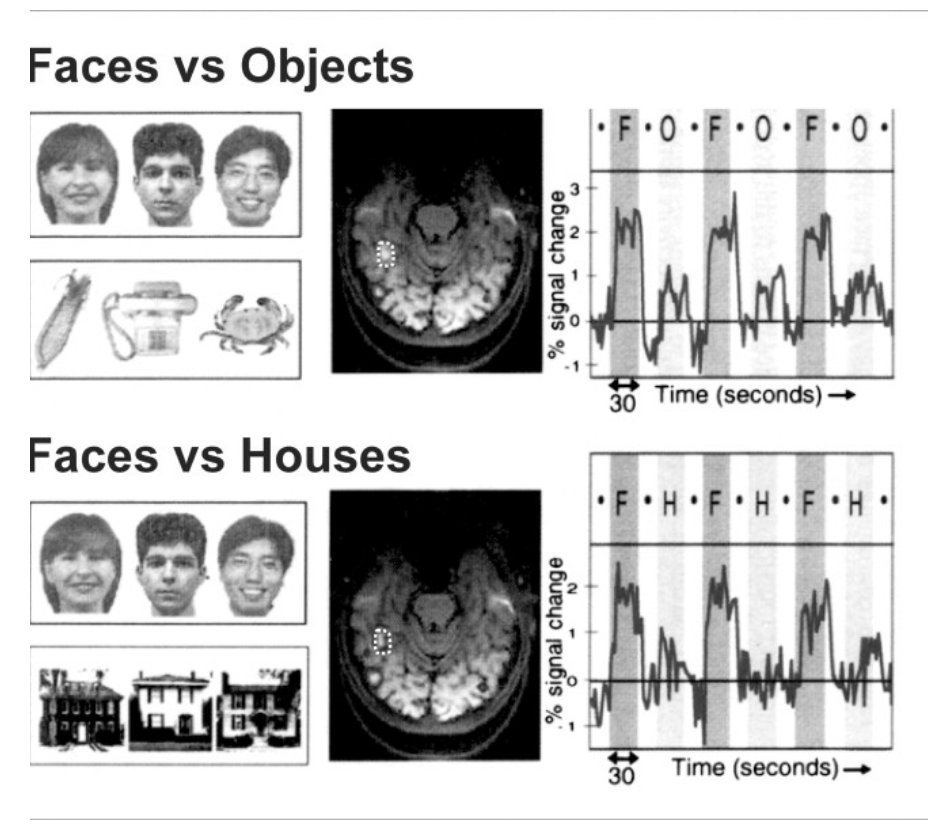
FFA: Faces vs. Objects vs. Houses
When the subject sees a Face (F), the FFA activity spikes massively.
When they see an Object (O) or a House (H), the activity drops significantly.
Our brains treat social information (faces) as fundamentally different from physical information (objects).
We are "hard-wired" to prioritize social data.
Personality judgments predict real-world outcomes. True or False
TRUE
Creating the stereotypic faces of the Big Five:
If I imagine a 'Highly Agreeable' person, what does their face actually look like to me?
High Extraversion: Note the subtle differences. These faces often appear "brighter," have slightly wider smiles (or more "upturned" mouths), and more open eyes.
Low Extraversion: These often appear more "flat" or neutral in expression.
We all share a remarkably similar "visual stereotype" for what these traits look like. When many people do this study, they tend to produce very similar-looking "High Extraversion" faces.
Creating the stereotypic faces of the Big Five: 2D → 3D image
Allows them to mathematically "crank up" or "dial down" specific facial features to see exactly which muscle movements or bone structures signal a specific Big Five trait.
They used computer software to digitally "average" the faces of the top 10% and bottom 10%. (Took 2D photograph → 3D Face Recognition → Variations of the 2D photograph overlaid on top)
Helps pinpoint exactly what it is about a face that makes us judge someone as "Conscientious" or "Agreeable" in a thin slice.
What are Expectancy Effects?
Self-fulfilling prophecies
Our expectations of others can lead them to behave in ways that confirm those expectations
Ex: Bloomers Study (Teachers' expectations influence student performance)
Teachers were warmer
Gave better feedback
Taught harder material
Gave more opportunities
Thin slice personality judgements are powerful enough to predict the winners of major political elections with startling accuracy. True or False?
TRUE
Personality disorders can be self-diagnosed. True or False?
FALSE
What is a personality disorder?
Extreme levels of traits
Very high and low amounts
symptoms become traits
What are maldaptive traits?
Traits that can start to cause problems for you or others around you
Extreme Levels of Traits Can Be Maladaptive
Long term symptoms
What is the research question for the Rogers Biesanz reading?
Does the "Good Judge" of personality actually exist, and under what conditions can we see their skill?
How did they answer the research question in the Rogers Biesanz reading?
They used Round-Robin groups (where everyone rates everyone else) and watched videos of people interacting.
they looked for an interaction between the Judge and the Target
What did they conclude in the Rogers Biesanz reading?
Yes, the Good Judge exists, but they need a "Good Target" to shine.
A "Good Judge" is only significantly more accurate when they are judging a "Good Target" (someone who is open and expressive)
What is an example of adaptive withdrawl?
Someone who thrives in their own company, but engages with others
What is an example of maldaptive withdrawl?
Someone who is socially isolated and detached from others with no positive social contact
Personality disorders are stable over time. True or False
TRUE
When do personality disorders normally begin?
Adolescence / Emerging Adulthood
What is the DSM?
The Diagnostic and Statistical Manual
Cookbook approach to diagnosing psychological disorders
Lists ingredients (e.g., symptoms)
If you have enough of them, you get a diagnosis
The AMPD is a part of the DSM-5. True or False?
TRUE
What is the AMPD?
Alternative Model for Personality Disorders
6 disorders
NO clusters
Why do we have the DSM?
Standardization and Insurance
What are the major groups for personality disorders in the DSM-IV?
Cluster A: odd or eccentric patterns of thinking
Cluster B: impulsive and erratic patterns of behavior
Cluster C: anxious and avoidant emotional styles
What are the 10 major personality disorders in the DSM-IV?
Cluster A:
Paranoid PD
Schizoid PD
Schizotypal PD
Cluster B:
Antisocial PD
Borderline PD
Histrionic PD
Narcissistic PD
Cluster C:
Avoidant PD
Dependant PD
Obsessive Compulsive PD
What does the AMPD look at?
Life impairment due to traits
Levels of maldaptive traits
Schizotypal Personality Disorder (SPD)
Odd thoughts, strange ideas, unconventiional behavior, superstitious beliefs, difficulty in close relationships
Similar to schizophrenia when the PD is at extremes
Stable throughout life
What is the prevelance of Schizotypal PDs?
0.6–4.6%
More common in males
Antisocial Personality Disorder (ASPD)
Often incorrectly called psychopathy or sociopathy
Unlawful behavior
Deceitfulness
Impulsivity/failure to plan ahead
Irritability or aggressiveness
Repeated physical fights/assaults
Reckless disregard for safety
Lack of remorse/Indifferent to hurting and mistreating others
What is the prevelance of Antisocial PDs?
3% in males, 1% in females
More prevelant in ages 18-49
Specifically 25-34 (3.9%)
ASPD + _______ _______ + low ________ + low ___________ = Psychopathy specifiers
Attention Seeking
Withdrawal
Anxiousness
AMPD includes ‘Psychopathy specifier’. True or False
TRUE
Narcissistic Personality Disorder (NPD)
Excessive self-love
Strong self-importance, entitlement, & superiority
Need to be admired
Lack of empathy
Fragile self-esteem (the narcissistic paradox)
Envy of others
What is the prevelance of Narcissistic PDs?
6.2%
Majority are men
Borderline Personality Disorder (BPD)
Instability of relationships, emotions, and self-image
Identity disturbance
Fears of abandonment
Prone to self-harm
Feel anything v. feel something else
Impulsive
Splitting: Seeing people as all good or all bad
What is the prevelance of Boderline PDs?
1.6%-5.9%
Mostly in women and adolescents/younger adults
How can you treat BPD?
dialectical behavioral therapy
Teaches skills for emotional self-control
Avoidant Personality Disorder (APD)
Fear of failure, rejection
Sensitive to criticism
Activities are restricted (to avoid embarrassment)
Need reassurance
What is the prevelance of Avoidant PDs?
2.4%
Split 50/50 between females and males
Likely starts in childhood
Obsessive Compulsive Personality Disorder (OCPD)
Preoccupied with order, rules, details
Perfectionistic
Workaholic
Rigid, Stubborn, Inflexible
‘Pack rat’
Someone who loves to collect things and hates to get rid of them
NOTTTT the same as OCD
What is the prevelance of OCPD?
2.1% -7.9%
men get diagnosed double compared to women
How can you diagnose PDs?
Clinical Impressions
Unstructured and structured interviews
Self-reports
MMPI: Self report questionnaire, usually answered in a book format or online
What are the types of Clinical Impressions?
Unstructured interviews:
A natural, free-flowing conversation where the clinician looks for "tells" (body language, tone, logic) that aren't on a checklist.
Structured Interviews:
Using a standardized set of questions (like the AMPD) to ensure they cover every possible symptom.
What are the strengths and weaknesses with clinical impressions?
Strengths: The clinician can see "blind spots" that the patient might not notice
Faults: a clinician is a human who can misinterpret a patient's behavior based on their own biases or limited experience.
A clinician only sees you in a quiet office for 50 minutes. You might be on your "best behavior," it’s a snapshot, not a full movie of your life.
Personality disorders can be Ego-Syntonic. True or False?
TRUE
What does mean to have an Ego-Syntonic PD?
Maladaptive traits seen as normal, even valued
Think that others have a problem
Can make treatment challenging
Labeling
Misleading
No one fits exact criteria
Can limit understanding
Not an explanation
Can be useful and are necessary
What are the main issues with the concept of personality disorders?
Categorical
Overlap among disorders (mode = 4)
Confusing labels & explanations
Schizoid, schizotypal, schizophrenic
OCD vs. OCPD
Biases & cultural differences
What’s normal vs abnormal?
What tool is used to diagnose personality disorders?
the DSM-V
How many personality disorders are in the AMPD?
6 PDs
What are the challenges with the DSM-V?
Ego-Syntonic
Labels can be stigmatizing, misleading, confusing
Categorical, but categories overlap
Biased
What is the research question for the Widiger et al reading?
Can personality disorders be understood as extreme, maladaptive versions of general personality traits rather than distinct mental illnesses?
How did the Widiger et al reading answer the research question?
They reviewed decades of data showing that every major personality disorder matches up with the Five-Factor Model (FFM), which is the standard way scientists describe "normal" traits
What was the conclusion in the Widiger et al reading?
Treating personality disorders as "extreme traits" is better because it allows for more personalized treatment, reduces the shame of a "disorder" label, and helps doctors see a patient's natural strengths alongside their struggles.
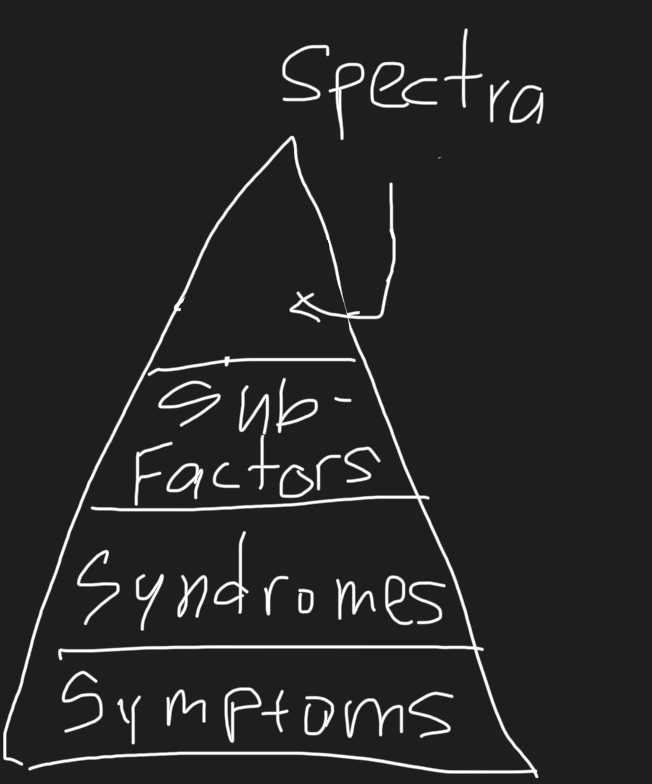
What is HiTOP?
New model of the major dimensions of psychopathology
What is Psychopathology?
Mental Illness
Includes personality disorders
What problems does HiTOP fix within the DSM?
Categorical → Dimensional
Clinical Impressions -→ Empirically derived model of the major dimensions of psychopathology
HiTOP is NOT Hierarchical. True or False
FALSE
List the four main levels of HiTOP (Low to High on Triangle)
Symptoms
Syndromes
Sub Factors (within spectra)
Spectra
How is HiTOP Hierarchical?
Organizes psychopathology hierarchically via factor analysis by four levels
Symptoms VS. Traits
Temporary, short term states VS. Long-term, persistent thoughts, feelings, and behaviors
Symptoms/Traits
Symptoms (if they occur long enough they can become maladaptive traits)
Deviant/violent behavior
Substance abuse
Law breaking
Ex: “crying”, “sleeplessness”, “worthlessness”
Syndromes
Groupings of symptoms/traits
Ex: Substance use/substance problems, physical aggression, destruction of property, fraud, and theft
Spectra
Groupings of Syndromes
Mapping co-occurring disorders
Either Internalizing OR Externalizing
Sub-Factors
Some spectra present in different forms
Internalizing manifesting as “Distress” vs. “Fear”
Ex: Substance Abuse and Anti Social behavior
The BAD Five is a part of AMPD of the DSM-V, NOT HiTOP. True or False
TRUE
What is the BAD Five?
Correlate with the BIG FIVE
Pathological representation
Value Judgement
“You shouldn’t have too much or too little of something!”
We don't do that in personality psych
What are the BAD Five Traits?
Detachment
Disinhibition
Antagonism
Negative Affectivity
Psychoticism
Detachment
Very Low Extraversion
Lack of pleasure
Depression
Suppressed emotions
Avoiding intimacy
Withdrawal
Suspicion
Disinhibition
Very low consciousness
Distracted
Impulsive
Risk-taking
Perfectionism
Irresponsible
Antagonism
Very low agreeableness
Grandiose
Callous
Deceitful
Manipulative
Attention-seeking
Negative Affect
Very high neuroticism
Anxious
Hostile
Submissive
Perseveration
Separation anxiety
Emotional stability
Psychoticism
Very high openness to experiences
Eccentric behavior
Strange beliefs
Perceptual dysregulation
The BIG Five is the foundation for what?
HiTOP & AMPD
What is the research question for the Hopwood reading?
If personality disorders are defined only by traits that also appear in other mental health issues, does the specific category of "Personality Disorder" actually exist as a distinct concept?
How did they answer the research question for the Hopwood reading?
Because traits are not unique to personality disorders, we must instead define these conditions by a patient's level of "personality functioning" (sense of self) or their specific interpersonal challenges during treatment.
What was the conclusion for the Hopwood reading?
To remain clinically useful, personality disorders should be viewed as "interpersonal disorders" that alert doctors to relationship difficulties and treatment obstacles rather than just a list of extreme traits.