Exam 3 Study Material
1/194
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
195 Terms
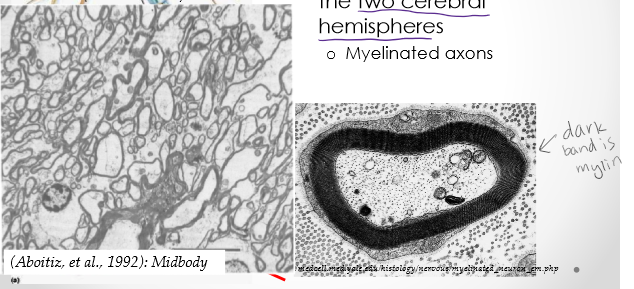
What is the corpus callosum?
Largest white matter tract that crosses and connects the two cerebral hemispheres. Myelinated axons. Composed of: 200-350×106 fibers. These axons constitute only 2% of all neocortical neurons.
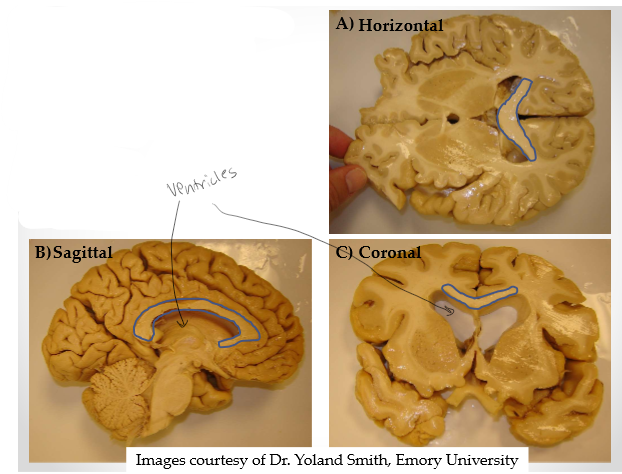
One brain structure, three different views
Spaces are lateral ventricles
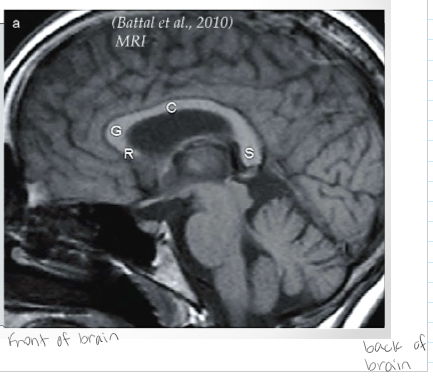
How is the corpus callosum organized?
Generally into 4 parts: 1. Rostrum 2. Genu 3. Corpus/Body/Trunk 4. Splenium *Be able to label them*
General overview of the functional connectivity of the corpus callosum
Most are homotopic interconnections
o Connecting the same functional areas of the brain
• Some are heterotopic fibers
o Linking functionally different cortical areas
• Majority are excitatory
o Integrate information across hemispheres
• Some are inhibitory
o Hemispheres inhibit each other to maximize independent functions
• In healthy individuals all fibers are present at birth
o The actual functional connectivity through the CC increases as
fibers increase their myelination
o Occurs from about 4 months of age to young adulthood. Amount of myelin on axon changes over time.
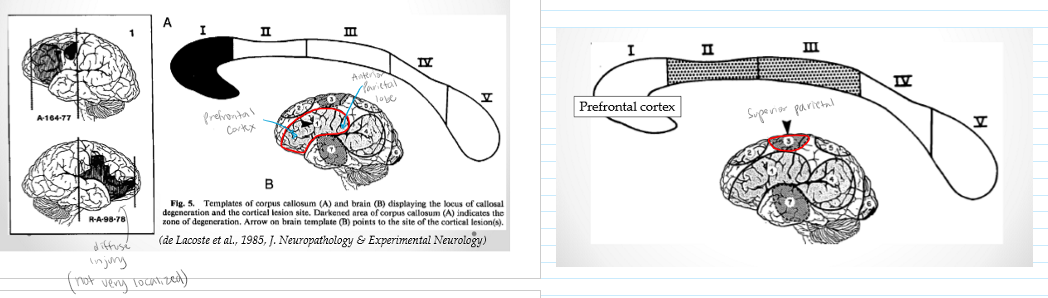
How did we first know what the corpus callosum connects?
13 Patients with unilateral focal cortical lesions due to:
o Ischemic Infarctions
• Stroke and cell death due to oxygen/ blood supply cut off
o Circumscribed Contusions
• Form of traumatic brain injury; Defined area of bruising of brain
• Crude Method: Examined the degeneration of fibers in CC to determine what parts of the cortex cross through each area of the CC.
• Note: after examination of brains, some lesions were more diffuse than expected
Ischemic Infarctions
Stroke and cell death due to oxygen/ blood supply cut off
Circumscribed Contusions
Form of traumatic brain injury; Defined area of bruising of brain
Crude Method
Examined the degeneration of fibers in CC to determine what parts of the cortex cross through each area of the CC.
Homotopic Interconnections
Connecting the same functional areas of the brain
Heterotopic fibers
Linking functionally different cortical areas
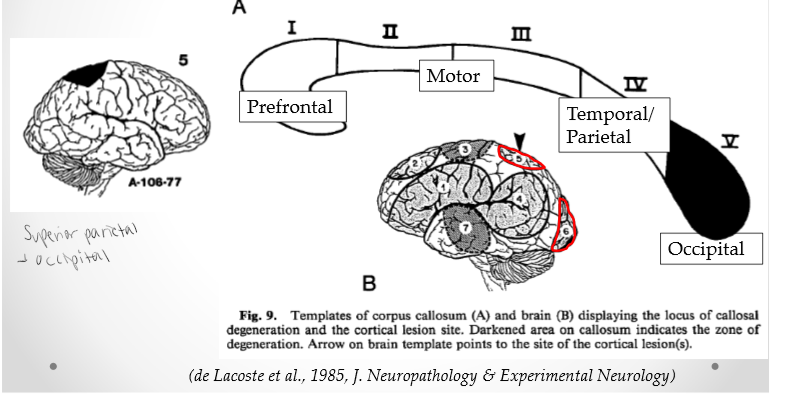
Prefrontal and anterior parietal region
Rostrum and genu. Prefrontal area
Posterior Superior frontal area
Rostral and mid body. Connecting motor areas of the brain. Motor area
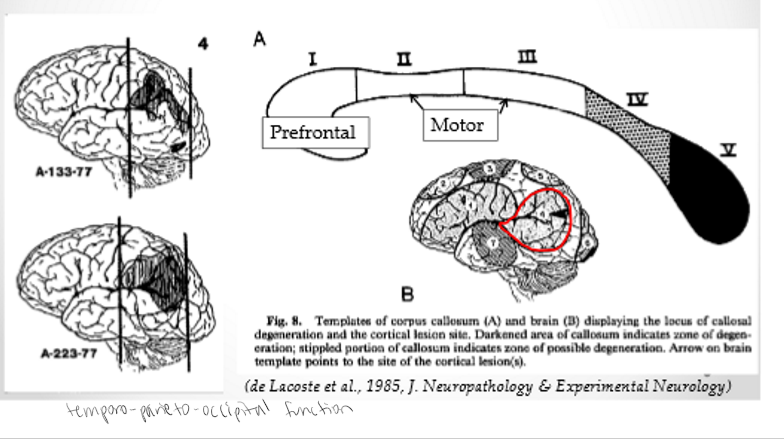
Temporo-Parieto-Occipital Junction
Caudal body and splenium. Temporal/Parietal lobe
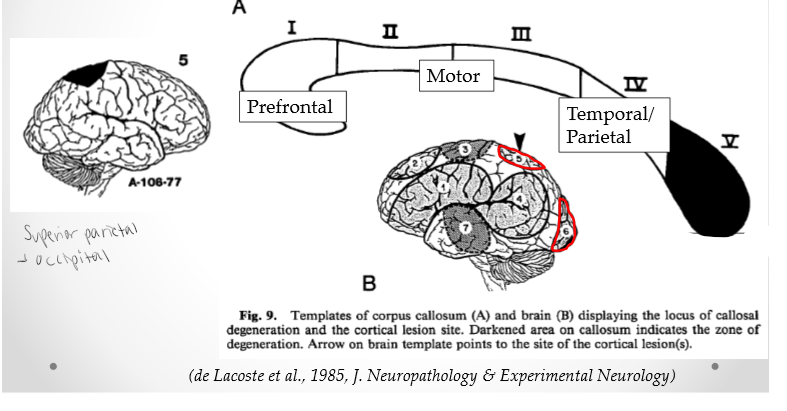
Superior-Parietal and Occipital Cortices
Splenium. Occipital lobe
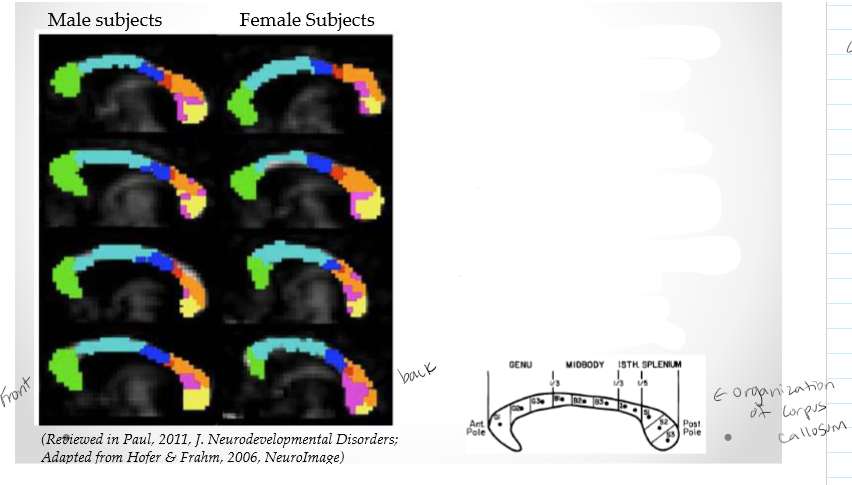
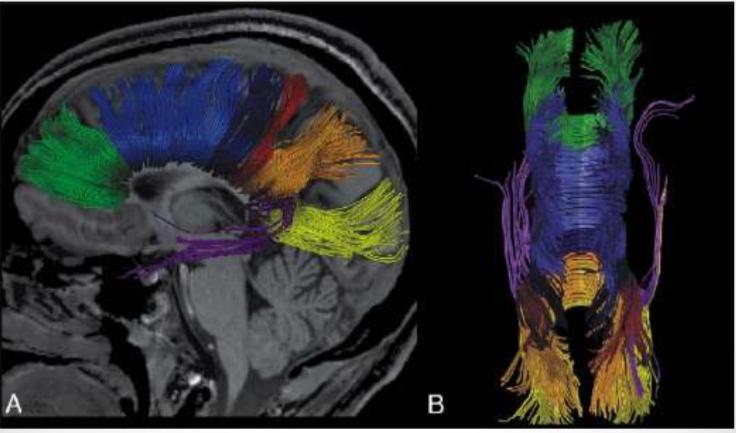
Summary of connections using newer techniques
Functional maps of the CC (slightly modified from earlier studies):
• Green: Prefrontal lobe
• Light Blue: Premotor & supplementary motor areas
• Dark Blue: Primary motor cortex
• Red: Primary Sensory cortex
• Orange: Parietal lobe
• Violet: Temporal lobe
• Yellow: Occipital lobe
Not that much is different between male and female
What are some characteristics of each of these areas? (CC)
20 Human subjects
• Thin fibers most dense in genu & splenium (<0.2μm)
o Low myelination, slow conductance velocities
• Large fibers most dense in mid-body(>0.2μm)
o High myelination, high conductance velocities
Measure density of corpus callosum from front to back of brain. Density of fibers. Thin fibers most dense diameter of corpus callosum. Motor areas have highest myelin and conductance and thickest diameters.

How did we come to understand the functions of the corpus callosum & lateralization of the brain?
Dr. Roger Sperry & Dr. Michael Gazzaniga (student at the time) at California Institute of Technology. Dr. Sperry had been observing those with lesions in the left hemisphere were speechless. Was there something unique to each hemisphere or do they both perform the same functions? 1960s: Way to treat grand mal epileptic seizures: Severe the corpus callosum, but no obvious side effects!
What are some other complications of being a split-brain patient?
Joe. Blocks the interhemispheric transfer of perceptual, sensory, motor and other forms of information. Memory of split-brained patients is generally lower than normal. Two different attentional systems in the two hemispheres. Overall though, you would never know when meeting someone that they have a split-brain.
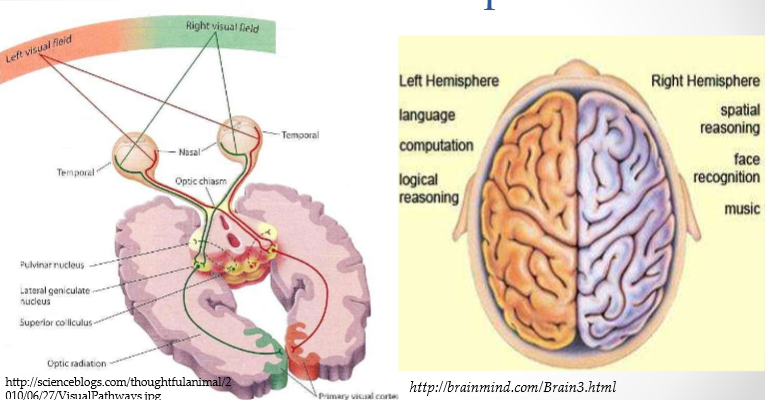
Language: A Rare Asymmetrical Neural Action
Broca’s Area: Language output; speech
• Wernicke’s Area: Language inputs; comprehension
• BOTH found in the left hemisphere
• Around Sylvian fissure, creates the arcuate fasciculus= Our overall concept of language
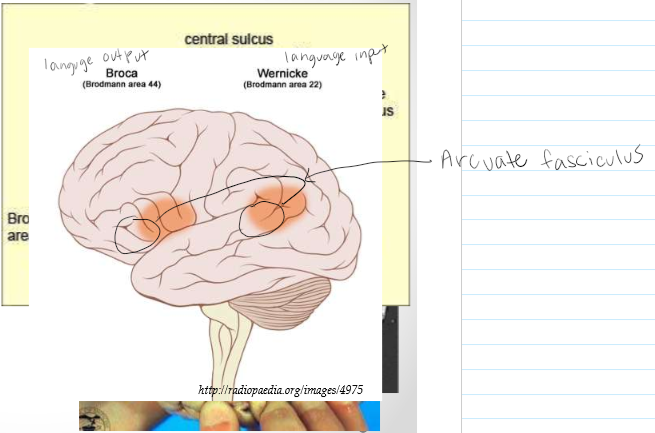
Arcuate fasciculus
Concents Broca’ and Wernicke’s area
Broca’s Area
Language output; speech
Wernicke’s Area
Language inputs; comprehension
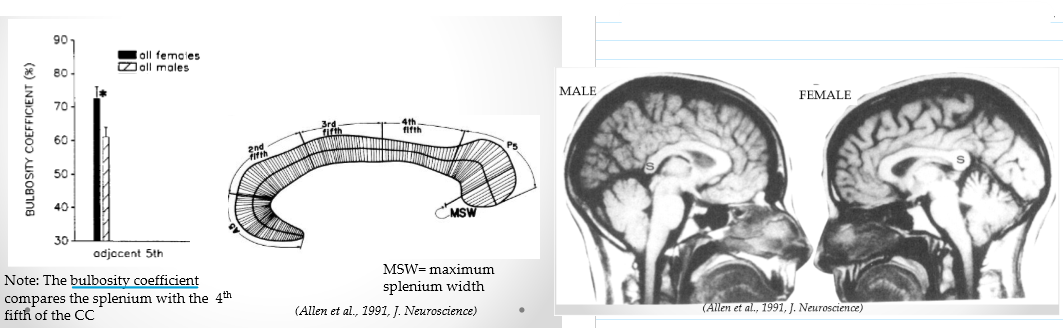
Sex differences in the corpus callosum?
Using MRI of 73 age-matched pairs of males & females. Splenium in females is a little thicker than males. Females have higher bulbosity coefficient in splenium than males. Brains are usually about the same size between males and females.
How we look at the corpus callosum
MRI: Magnetic resonance imaging. dMRI or DTI: Diffusion tensor magnetic resonance imaging. Map connectivity of the brain noninvasively. Diagnose conditions affecting integrity of nervous tissue. Measures: 1. Anisotropy: measures the direction and axon alignment. Higher anisotropy=greater alignment of fibers. 2.Diffusivity: Measures the degree to which cells restrict movement of water within a fiber sample. Higher diffusivity=less developed cellular structure (i.e., reduced myelination)
What does DTI look like?
Early DTI images. Color superimposed on images
Agenesis of the Corpus Callosum
Lack or partial lack of the CC. Fibers migrate ipsilaterally & course along the lateral ventricles forming Probst bundles. Not connected. Can function without the corpus callosum. Few observable symptoms.
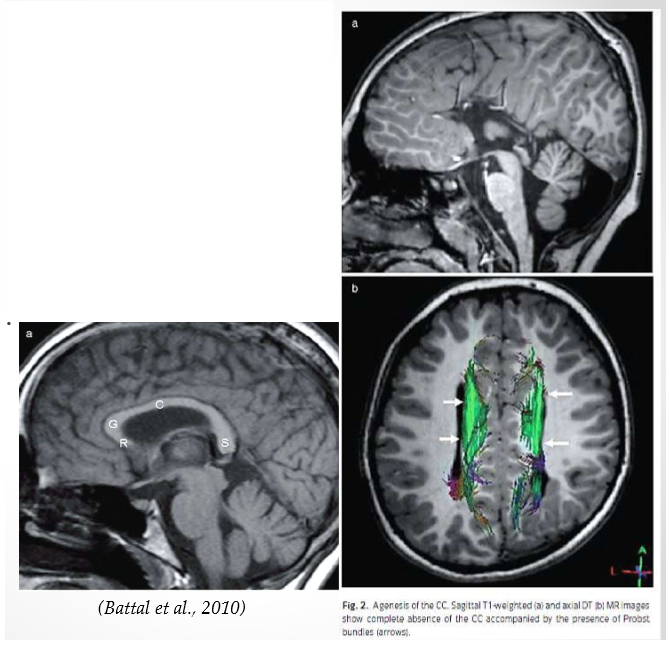
Ipsilaterally
Make more connections on same side of brain instead of across
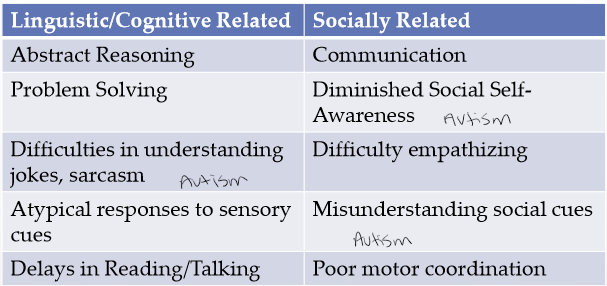
Agenesis of the CC (AgCC)
1:4000 live births. Few observable symptoms…is there compensation by other connections (i.e., the anterior commissure)? Actually perform better than adults on the split-brain test. Developmentally not the same, however have average IQ scores. These symptoms occur in various combinations and severity. Spectrum of how effected you are and of symptoms. Sounds similar to Autism.
Famous quote from Dr. Sperry
Sperry concluded (1974): “each hemisphere is indeed a conscious system in its own right, perceiving, thinking, remembering, reasoning, willing, and emoting, all at a characteristically human level, and . . . both the left and the right hemisphere may be conscious simultaneously in different, even in mutually conflicting, mental experiences that run along in parallel.”
Tramatic Brain Injury (TBI)
Occurs when an external mechanical force causes brain dysfunction. TBI usually results from a violent blow or jolt to the head or body. An object penetrating the skull, such as a bullet or shattered piece of skull, also can cause tramatic brain injury. Mild traumatic brain injury may cause temporary dysfunction of brain cells. More serious traumatic brain injury can result in bruising, torn tissues, bleeding and other physical damage to the brain that can result in long-term complications or death.
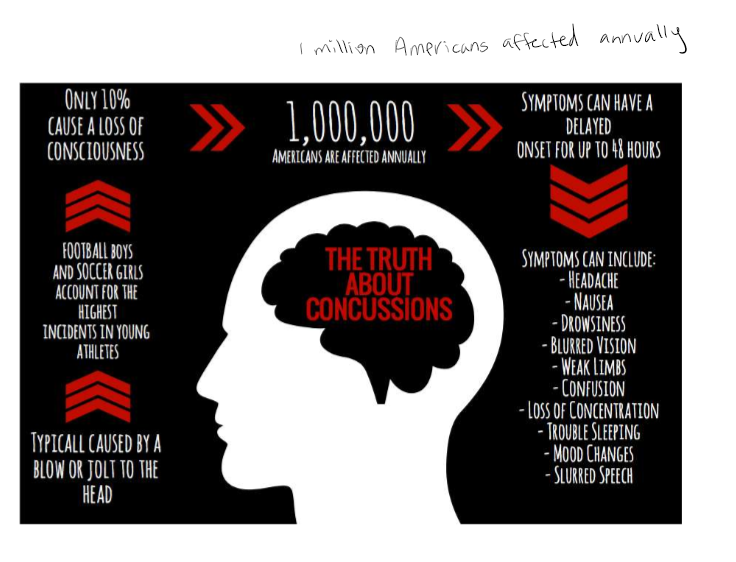
Concussion
Has occurred any time you have had a blow to the head that caused you to have symptoms for any amount of time. You do NOT need to have lost consciousness to have a concussion.
Symptoms of Concussion
Blurred or double vision; seeing stars; sensitivity to light or noise; headache dizziness, or balance problems; nausea, vomiting; trouble sleeping, fatigue; confusion, difficulty remembering, difficulty concentrating, or loss of consciousness.
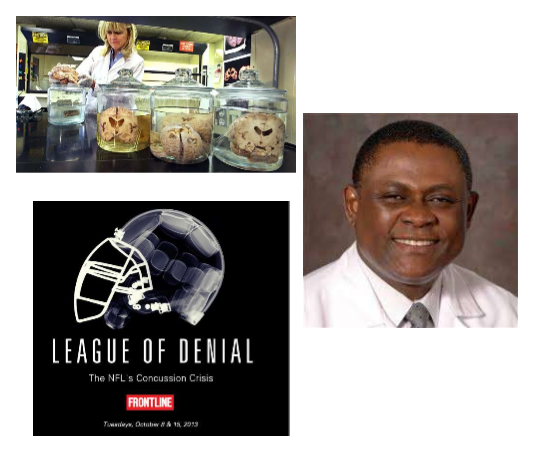
Chronic Traumatic Encephalopathy Case
One of the leading experts: Dr. Ann McKee. First noticed in NFL players: Dr. Bennet Omalu. Pittsburgh Steelers - Mike Webster. Brain looked like it was someone in there 70’s or 80’s and looked like Alzheimers. Neurodegeneration
What is Chronic Traumatic Encephalopathy
A progressive degenerative disease of the brain found in people with a history of repetitive head impacts (RHI), including symptomatic concussions as well as asymptomatic non-concussive hits that do not cause symptoms. Often incurred during contact sport play, military service, employment as a first responder, and other activities that involve repeated blows to the head. Non-concussive hits are routine in many sports, including checking in ice hockey and heading the ball in soccer.
• Also recognized as neurodegenerative p-tau pathology or a tauopathy.
• CTE has been known to affect boxers since the 1920’s (when it was initially termed punch drunk syndrome or dementia pugilistica). (pet trace ligand to trace phosphorylated tau)
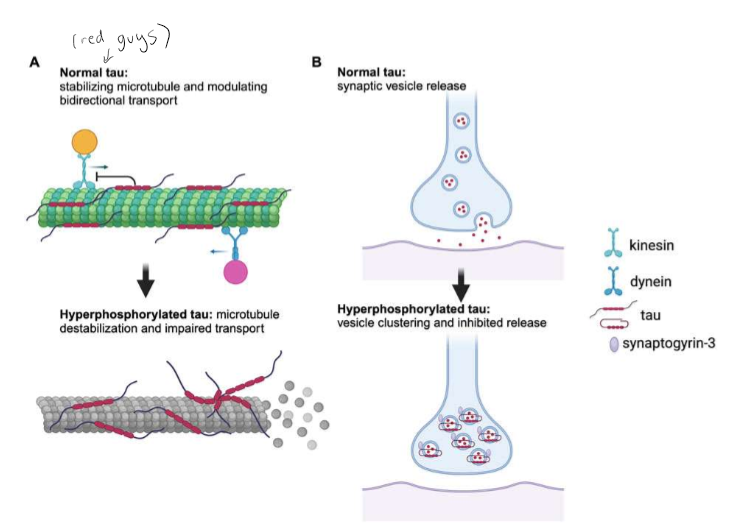
What is tau?
Tau is a microtubule-associated protein generated from the MAPT
gene on chromosome 17. Tau exists as a highly soluble and natively unfolded protein that interacts with tubulin and promotes its assembly into microtubules, which helps to stabilize their structure. Tau exerts an essential role in the balance of microtubule‐dependent axonal transport of organelles and biomolecules by modulating the anterograde transport by kinesin and the dynein‐driven retrograde transport. However, when tau becomes hyperphosphorylated, that is when neurofibrillary tangles can develop, resulting in neuronal death.
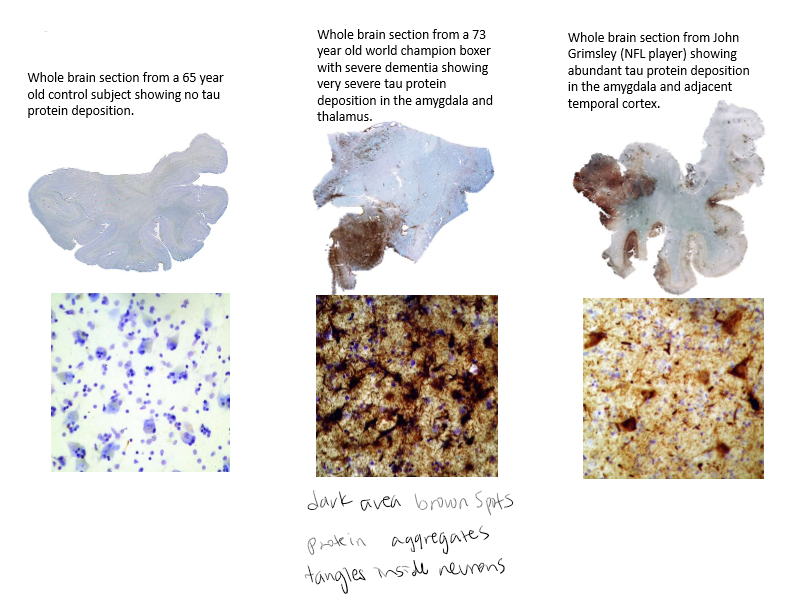
Tau immunostained sections of medial temporal lobe from 3 individuals
Tau stained brown. Cell nuclei stained blue.
Symptoms of CTE
Memory loss. Confusion. Impaired judgment, impulse control problems. Aggression, depression, anxiety, suicidality, Parkinsonism, and, eventually, progressive dementia. These symptoms often begin years or even decades after the last brain trauma or end of active athletic involvement. Personality change occurs. Occurs at younger state than what we would see with Alzheimers.
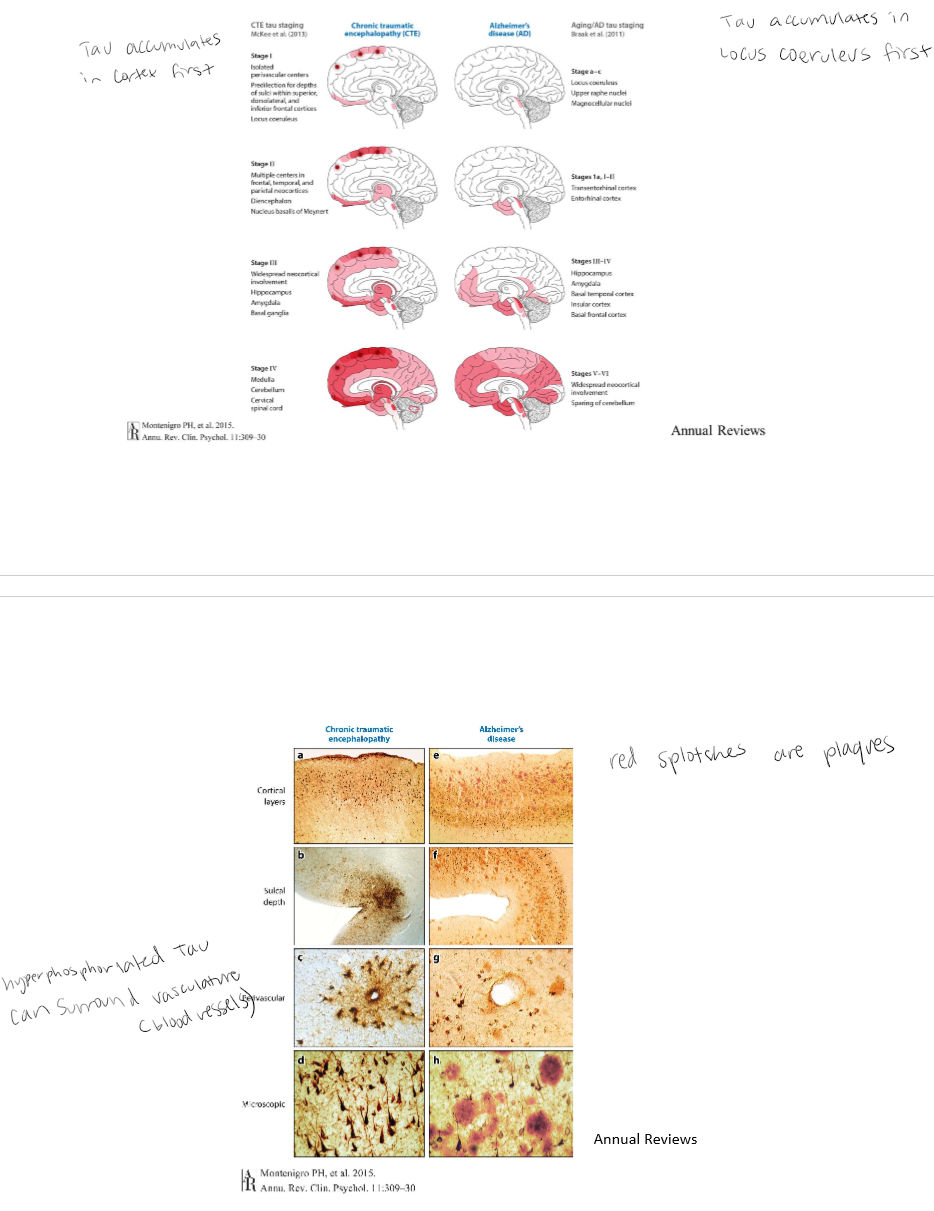
Comparison of hyperphosphorylated tau progression
CTE: Tau accumulates in cortex first. Hyperphosphorylated tau can surround vasculature (blood vessels). Azheimers: Tau accumulates in Locus Coeruleus first. Red splotches are plaques.
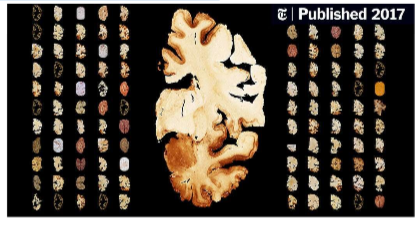
Staggering numbers
In 2017, Dr. McKee’s group published a study that made the NY Times: “A neuropathologist has examined the brains of 111 N.F.L. players — and 110 were found to have C.T.E., the degenerative disease linked to repeated blows to the head.
Dr. McKee & the UNITE Brain Bank
UNITE Brain Bank, part of the BU CTE Research Center- about 1500 brains. The CTE Center has three main divisions of research, Pathological Research, Clinical Research, and Molecular Research. Cannot completely diagnose while alive yet. Based on symptoms reported for the most part. PET scan if available. Does not have diffinitive diagnoses until postmortem.
When diagnosing CTE doctors take into consideration
Years of play and age.
1. Inflammation first with RHI
2. Vascular Permeability- especially in white matter
3. White matter loss-oligodendrocytes
4. Neurobehavioral symptoms
5. Tau pathology
6. Atrophy
7. Cognitive decline
8. TDP-43: TAR DNA-binding protein 43;
9. Functional decline (comes later- 40s or 50s)
1-4: Early on, acute, probably progressive
5-9: CTE: chronic, progressive
Aaron Hernandez
Heavy brain. Ventricular enlargement. Atrophy of the fornix. P-tau-containing tangles around blood vessels. Stage 3, severe frontal lobe involvement. (Dr. Ann McKee Webinar, 2024). Brain was heavier than it should have been.
Importance of Vasculature
Source of nutrients: Glucose and O2 (not stored). If blood supply is disrupted then stroke can occur.
Stroke
A stroke occurs when the blood supply to part of your brain is interrupted or severely reduced, depriving brain tissue of oxygen and nutrients. Within minutes, brain cells begin to die. Two major categories: Ischemic stroke and Hemorrhagic stroke
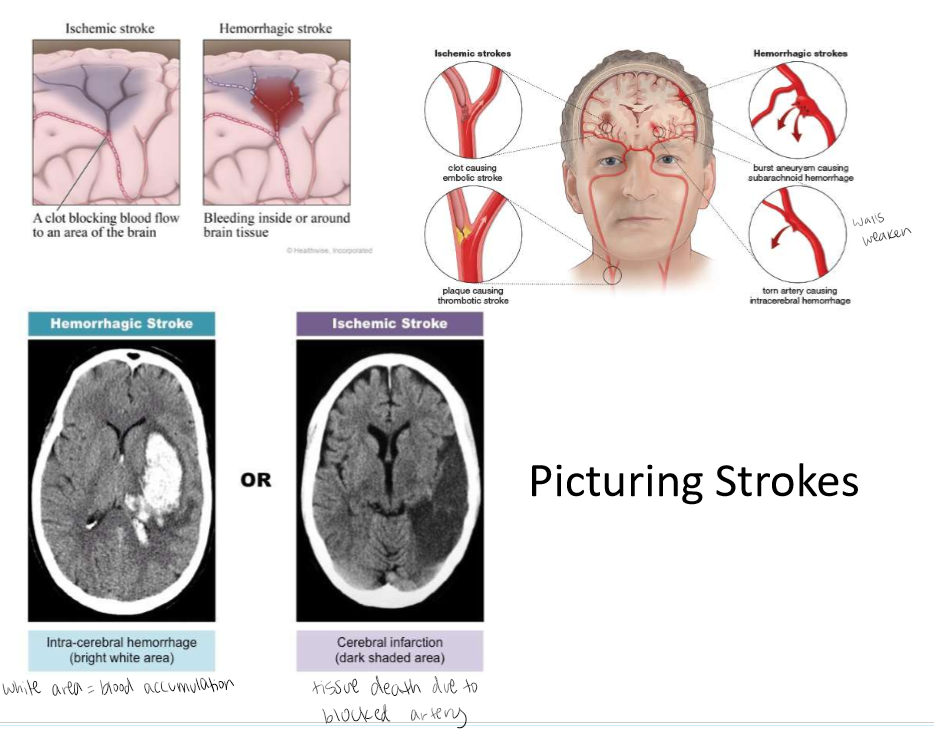
Ischemic Stroke
TIA: transient ischemic attack (brief decrease in blood flow, loss of function). Infarction: ischemia persistent and not corrected - could lead to tissue death. Blocking blood flow or a clot.
Hemorrhagic Stroke
Artery ruptures, releases blood. Aneurysm: ballooning of an artery due to weakening of muscular wall rupturing. Hemorraging - bleeding out. Blood vessels and artery walls get weaker and thinner.
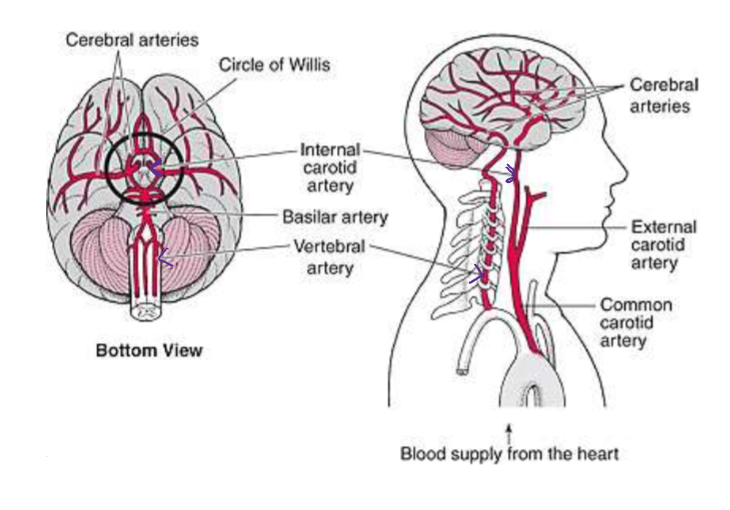
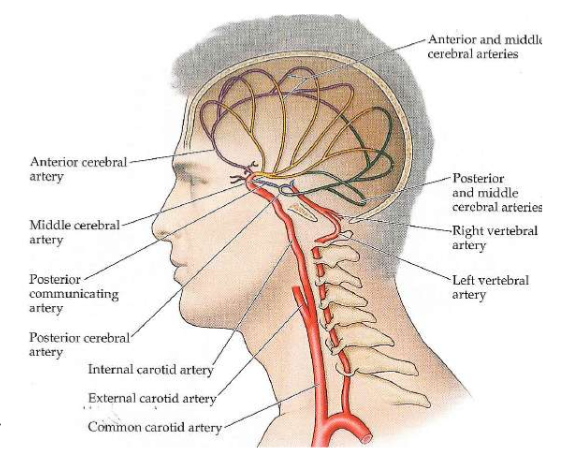
Vasculature Overview
Two main sources: 1. Internal carotid artery 2. Vertebral Artery
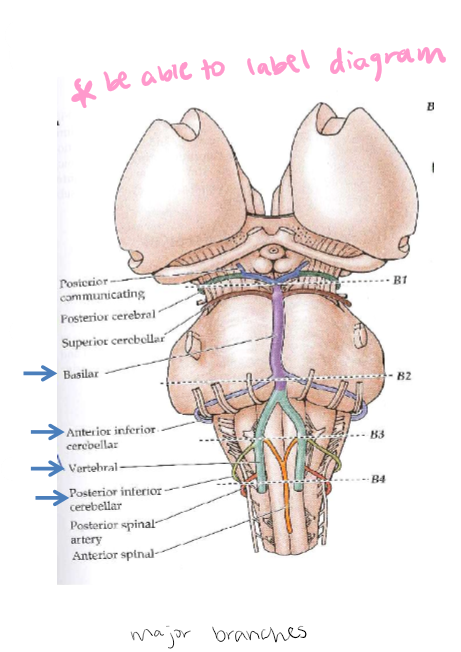
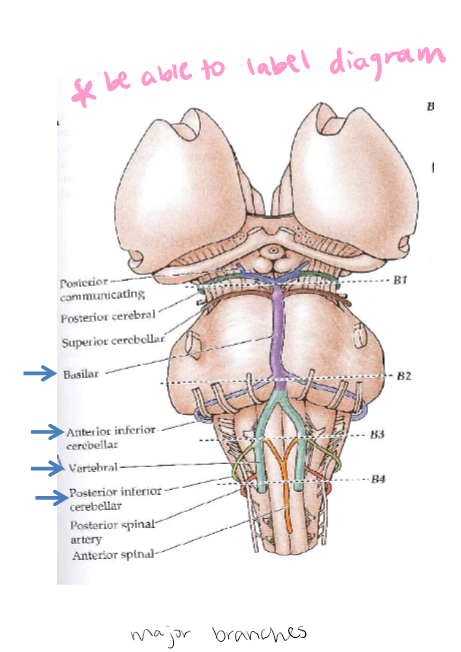
Vertebral Arteries
2 vertebral arteries join to form Basilar Artery: At medulla-pons interface, branches of the basilar artery also supply blood to pons. PICA: Posterior inferior cerebellar artery nourishes medulla: arises from vertebral artery. AICA: Anterior inferior cerebellar artery nourishes the pons: arises from basilar artery. (vertebral artery-green, basilar artery - purple, PICA comes off vertebral artery - red, AICA comes off basilar artery-light blue)
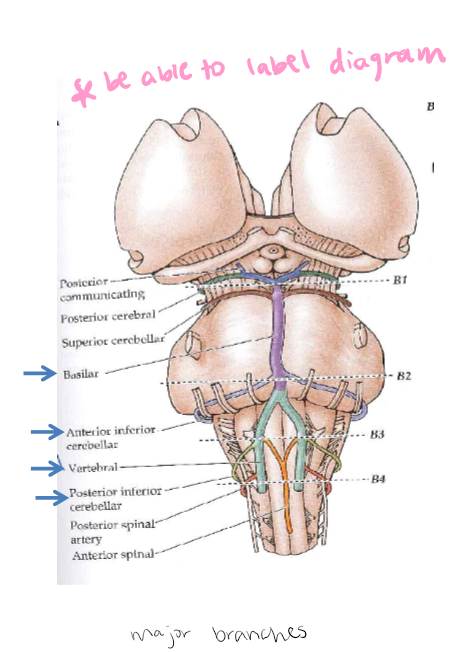
PICA: Posterior inferior cerebellar artery nourishes medulla
Arises from vertebral artery
AICA: Anterior inferior cerebellar artery nourishes the pons
Arises from basilar artery.
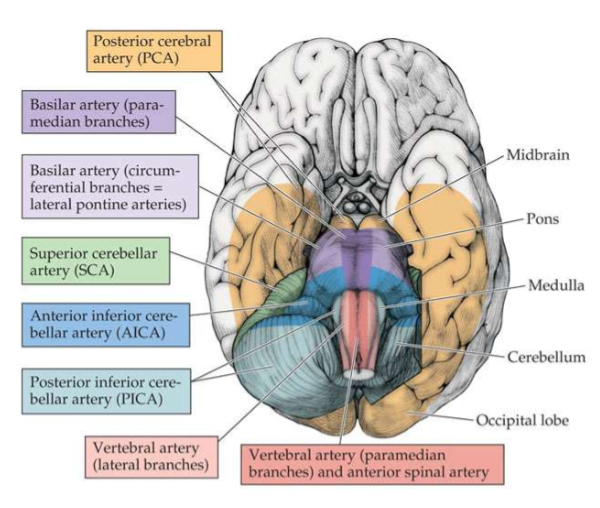
Brainstem and Midbrain Blood Supply
Ventral surface of the brain
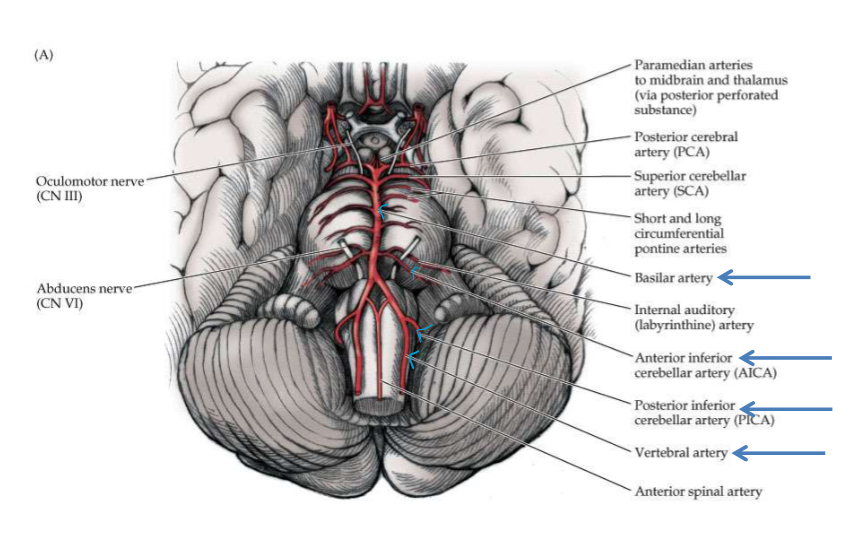
Ventral Brain Blood Supply
Internal Carotid Artery: 4 Portions
1.Cervical 2.Intrapetrosal 3. Intracavernous 4. Cerebral. Intracavernous and cerbral make up the carotid siphon.
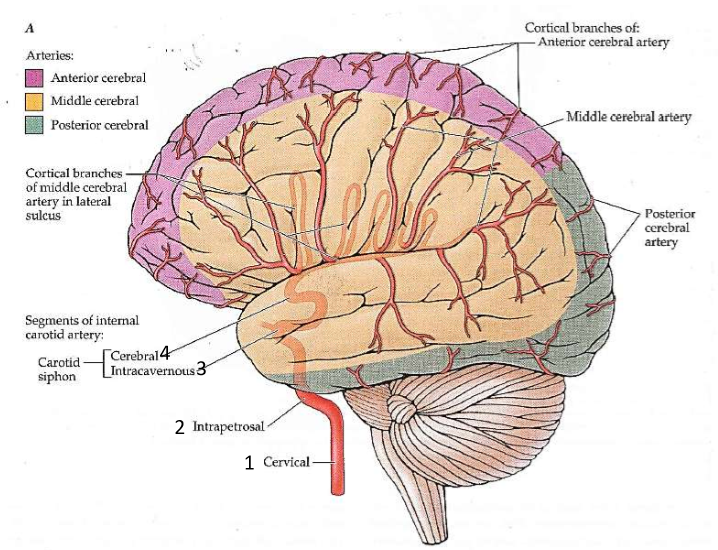
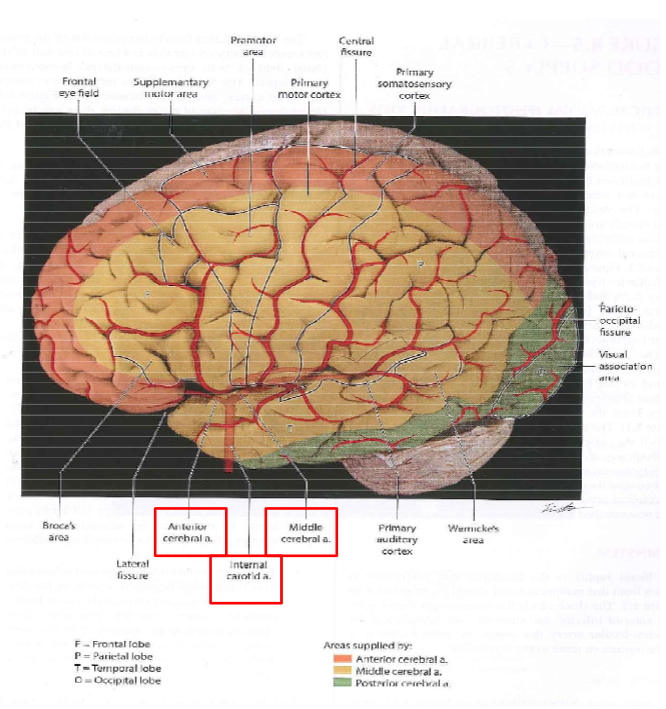
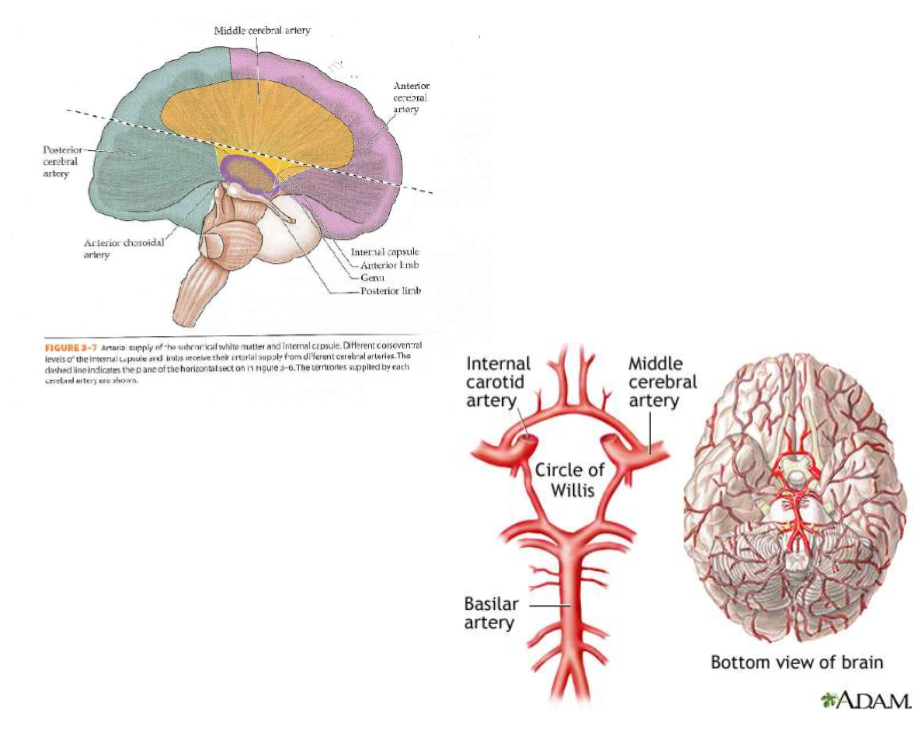
The Cerebral Artery Subdivisions
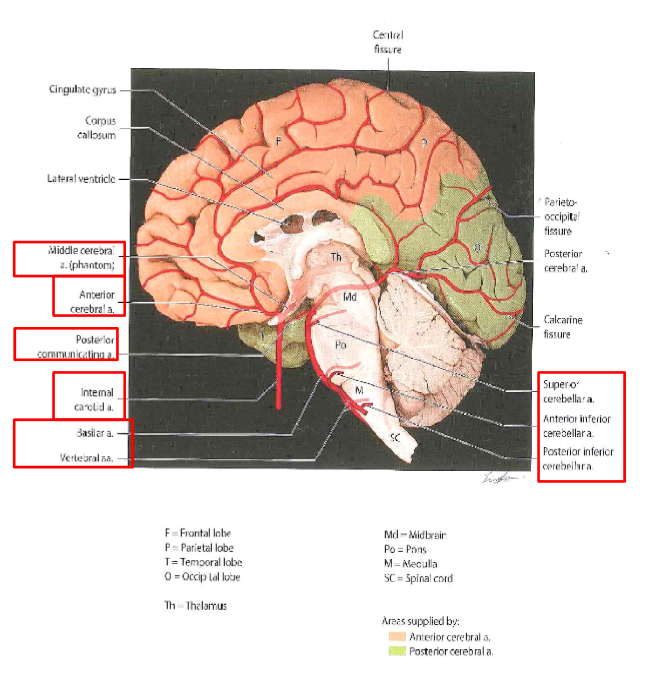
Their branches supply blood to cortex and subcortical structures. 1. ACA: Anterior cerebral arteries (purple) 2. MCA: Middle cerebral arteries (yellow) 3. PCA: Posterior cerebral arteries (green)
Another view of cerebral blood flow
Sagittal View of Cerebral blood flow
Collateral circulation provided by
1.Circle of Willis: The interconnection of the ACA, MCA, PCA
2.Terminal branches of the cerebral arteries
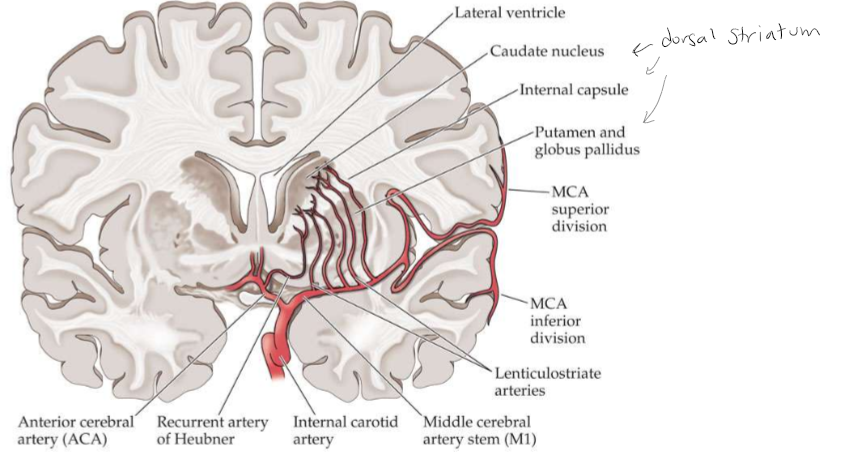
Lenticulostriate Arteries or Striate Arteries
Coronal section showing the lenticulostriate arteries arising from the proximal middle cerebral artery and supplying the basal ganglia and internal capsule. The recurrent artery of Heubner arises from the anterior cerebral artery.
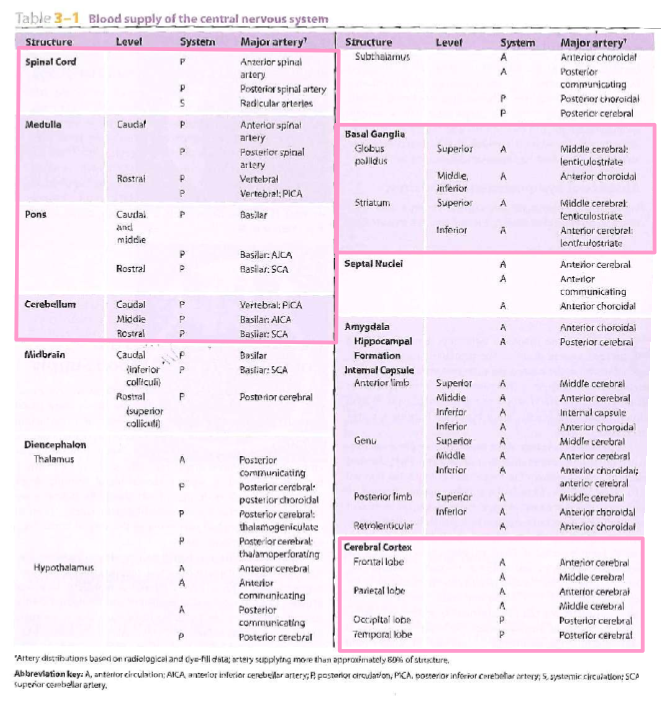
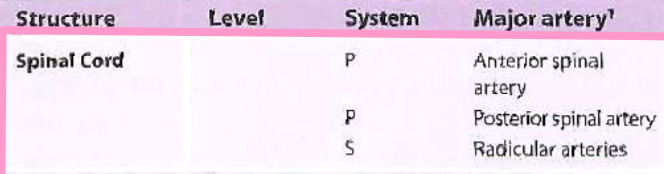
Blood Supply of Central Nervous System
*Know the ones in pink boxes* Spinal cord, medulla, pons, cerebellum, basal ganglia, cerebral cortex
Spinal Cord
System: P, P, S
Major Artery: Anterior spinal artery, posterior spinal artery, radicular arteries
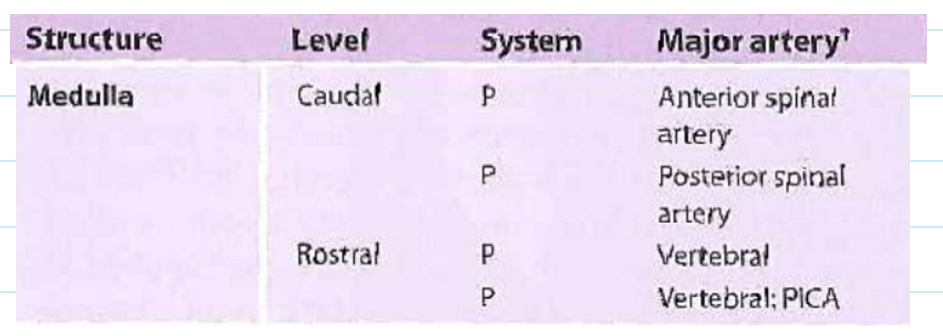
Medulla
Level: Caudal - Rostral
System: P, P - P, P
Major Artery: Anterior spinal artery, Posterior spinal artery - Vertebral, Vertebral; PICA
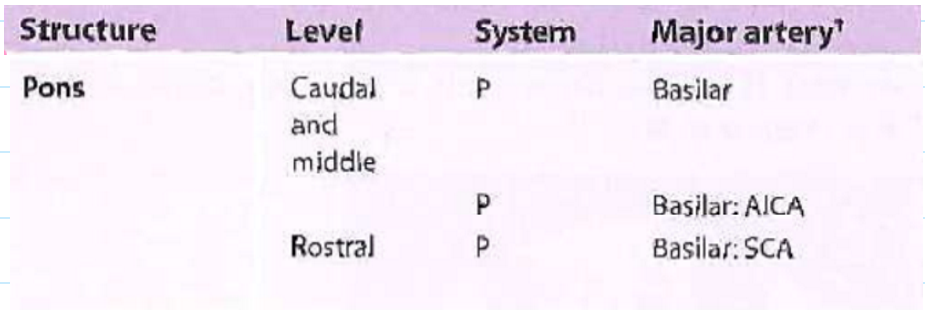
Pons
Level: Caudal and middle - Rostral
System: P - P, P
Major Artery: Basilar - Basilar: AICA, Basilar: SCA
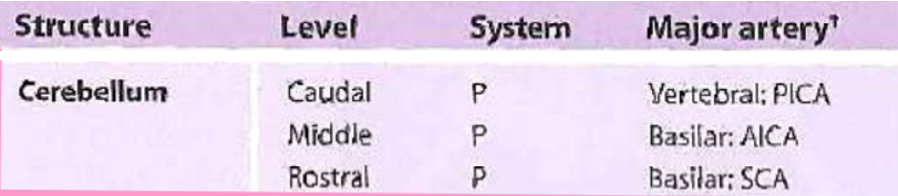
Cerebellum
Level: Caudal, Middle, Rostral
System: P, P, P
Major Artery: Vertebral: PICA, Basilar: AICA, Basilar: SCA
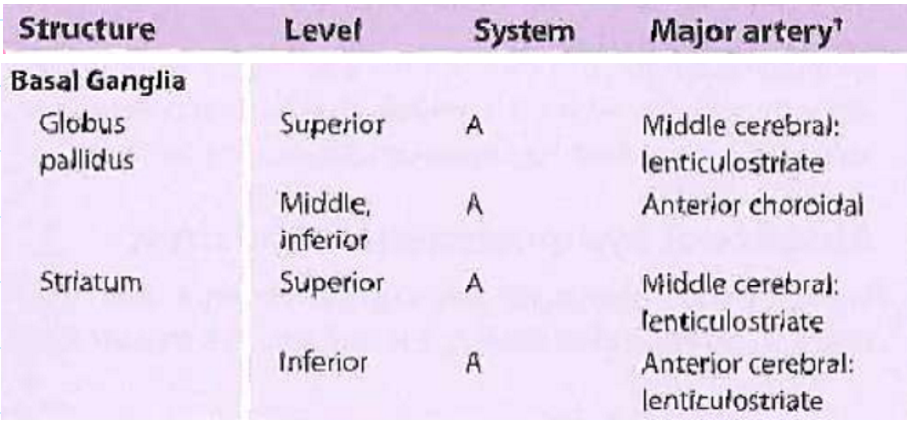
Basal Ganglia
Structure: Globus pallidus - Striatum
Level: Superior, Middle Inferior - Superior, Inferior
System: A, A - A, A
Major Artery: Middle cerebral lenticulostriate, Anterior choroidal - Middle cerebral lenticulostriate, Anterior cerebral lenticulostriate
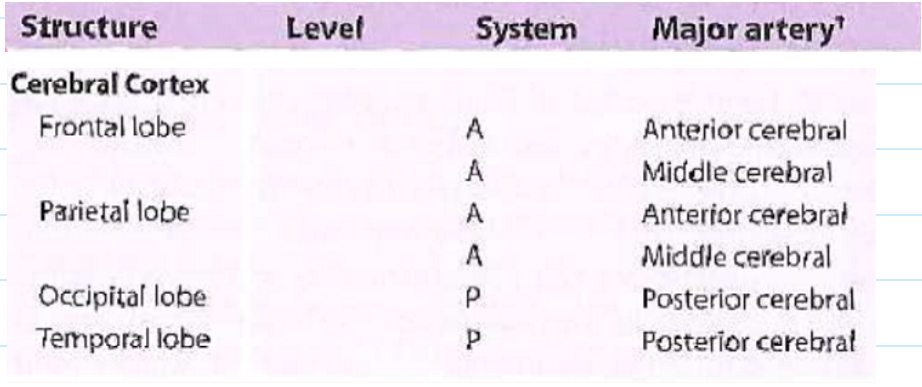
Cerebral Cortex
Structure: Frontal lobe; Parietal lobe - Occipital lobe; temporal lobe
System: A, A; A, A - P; P
Major Artery: Anterior cerebral, Middle cerebral; Anterior cerebral, middle cerebral - posterior cerebral; posterior cerebral
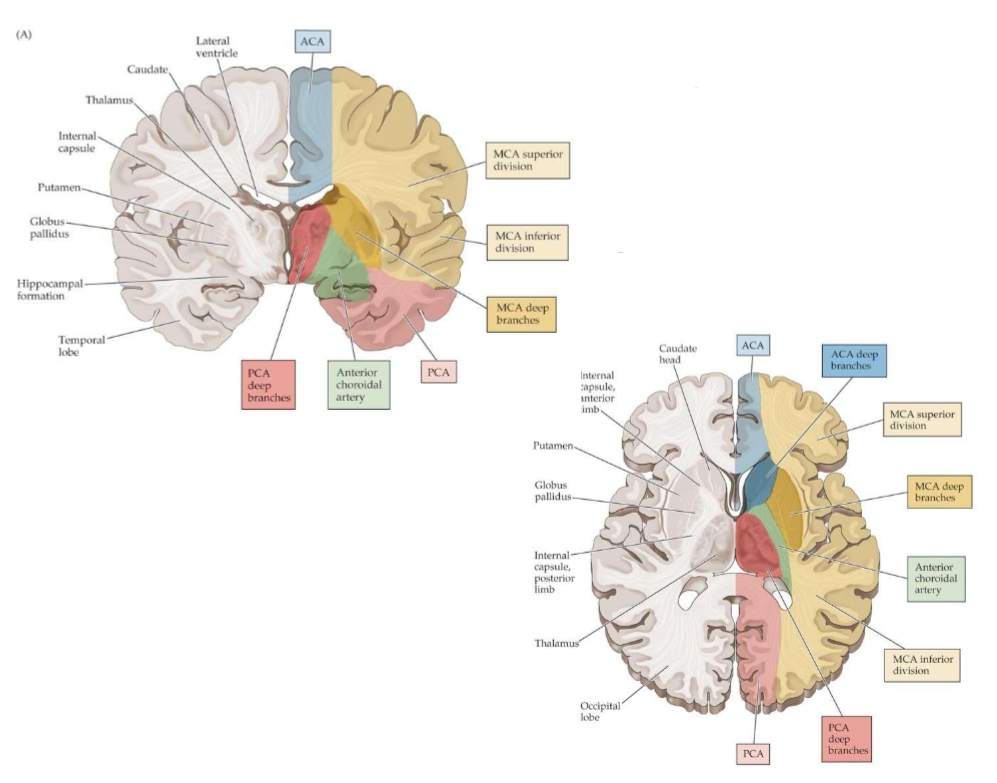
Summary of Superficial and Deep blood supply to the cerebral hemispheres
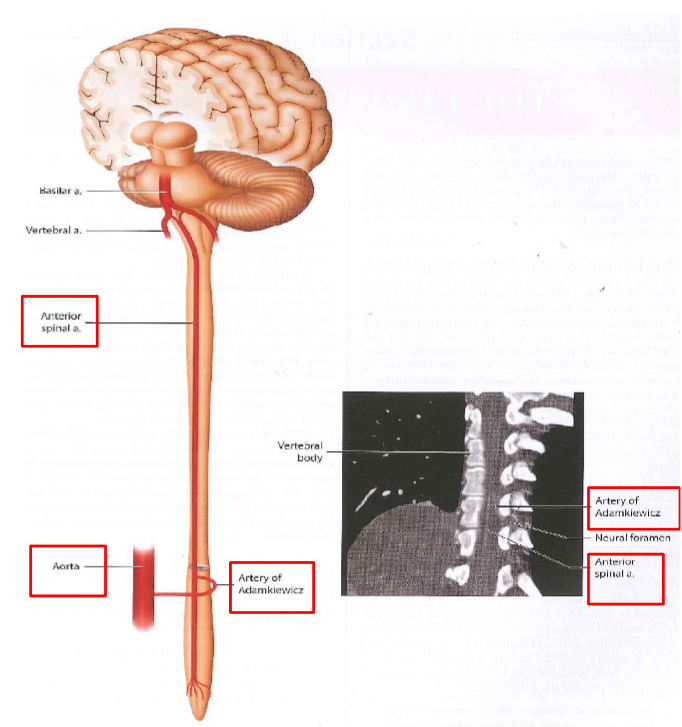
Spinal Blood Flow
Anterior Spinal artery - towards your chest not your back
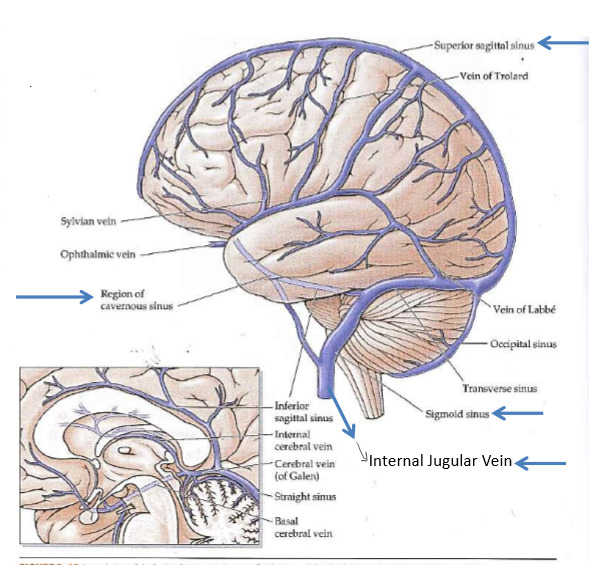
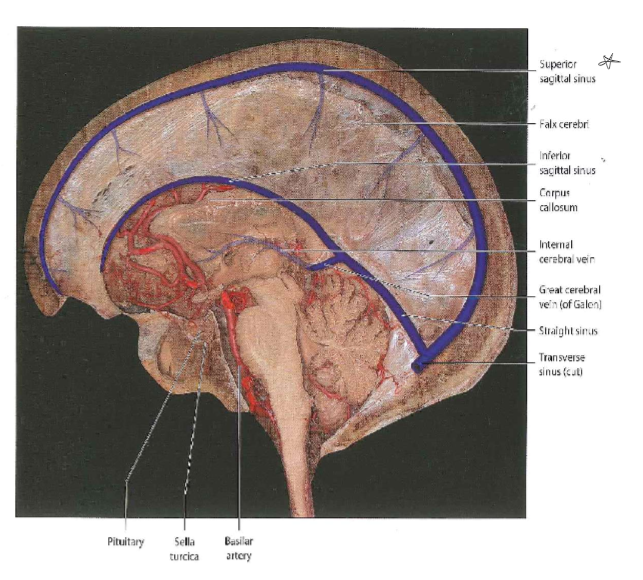
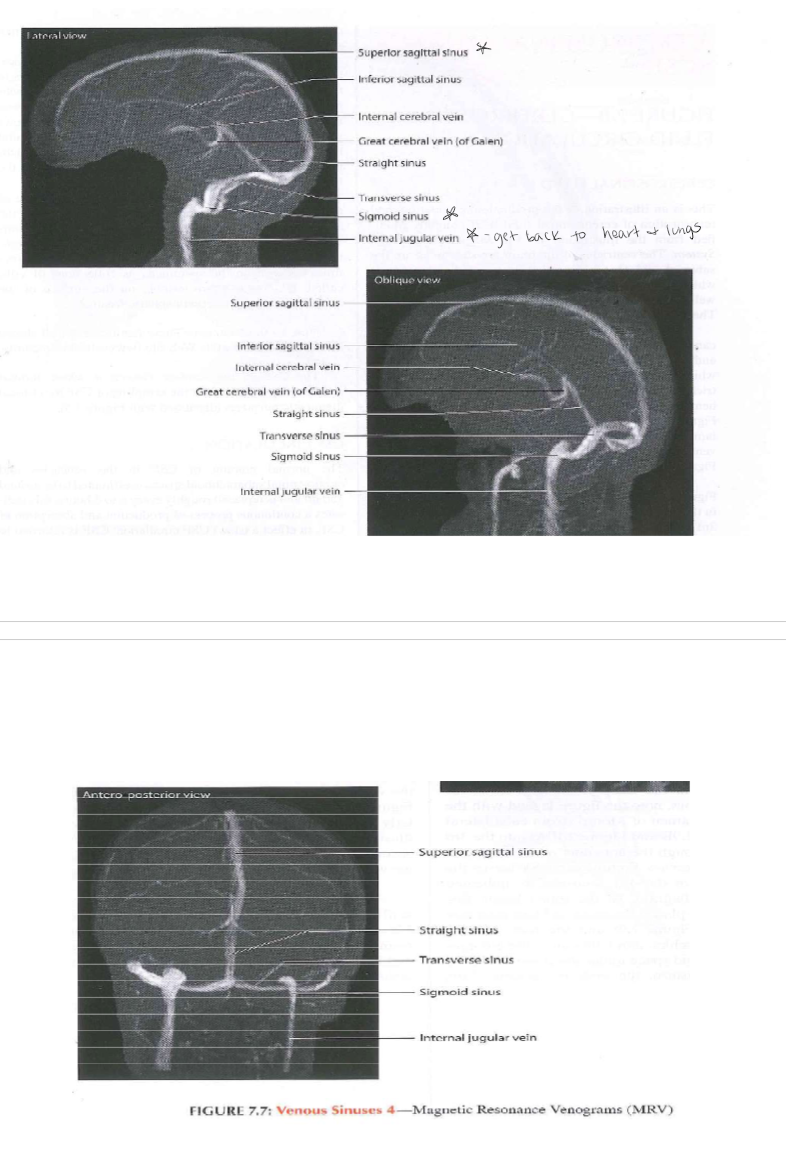
Venous Sinuses (veins)
Involved in CSF and blood flow. Both the superficial veins and the deep venous system empty into the Dural sinuses. They carry blood and CSF back to the sigmoid sinus and then jugular vein and thence to the heart. Less pressure than arteries. *Know the arrowed ones*
Picture of veins and arteries
Basal arteries in red and veins are in blue
Images on veins
Blood vessels in mouse brain
As described by Dr. Gareth Howell and colleagues: the image shows blood vessels visualized with an antibody against laminin (red) in a region of the parietal cortex from a 12 month old mouse. Also shown are pericytes (using an antibody against PDFGRB (green) and cell nuclei DAPI (blue). Pericytes are cells present at intervals along the walls of capillaries (and post-capillary venules). In the CNS, they are important for blood vessel formation, maintenance of the blood-brain barrier, regulation of immune cell entry to the central nervous system (CNS) and control of brain blood flow.

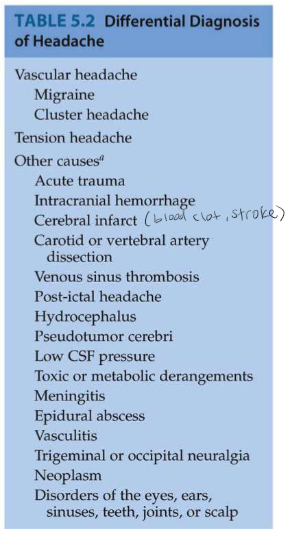
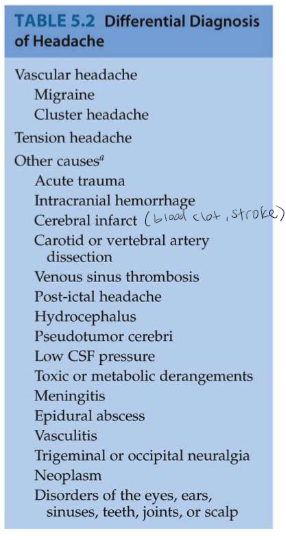
Headaches Caused by
Mechanical traction, inflammation, or irritation of other structures in the head that are innervated, including the blood vessels, meninges, scalp, and skull.
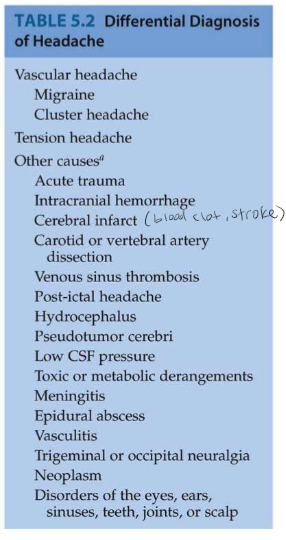
2 Major Classification of Headaches
Vascular and tension
Vascular Headaches
Inflammatory, autonomic, 5HTergic, neuroendocrine and other blood vessel caliber. Migraines: could be genetic basis. - Foods, stressors, eye strain, menstrual cycle, sleep. - Aura: visual blurring, shimmering, fortification scotoma (visual loss bordered by zigzagging lines resembling a fort). - Often unilateral. - Light, sound, sudden movement. - Nausea, vomiting, tender scalp. - 30 min to 24 hours. - Treatment: NSAIDs, ergot derivatives, anti-emetics, 5HT agonist, rest. - CGRP inhibitors (new class of drugs, calcogonin gene related peptides).
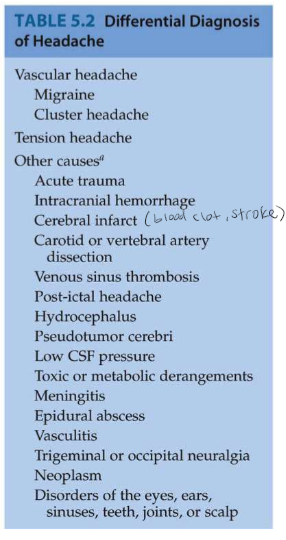
Tension Headaches
Steady dull ache (bandlike sensation), usually shorter in duration, possibly related to contracted head and neck muscles, chronic daily headaches: treated with NSAIDs, muscle relaxation, analgesics, TCAs.
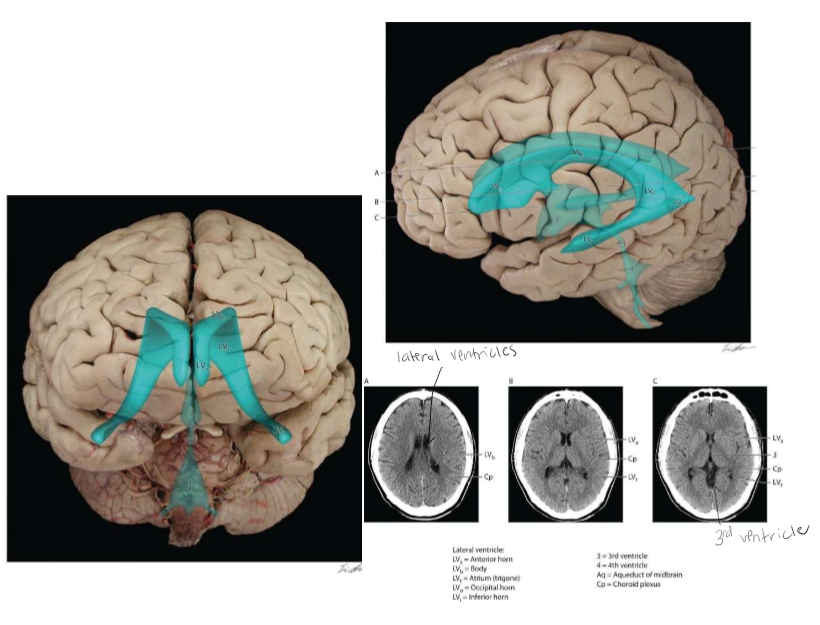
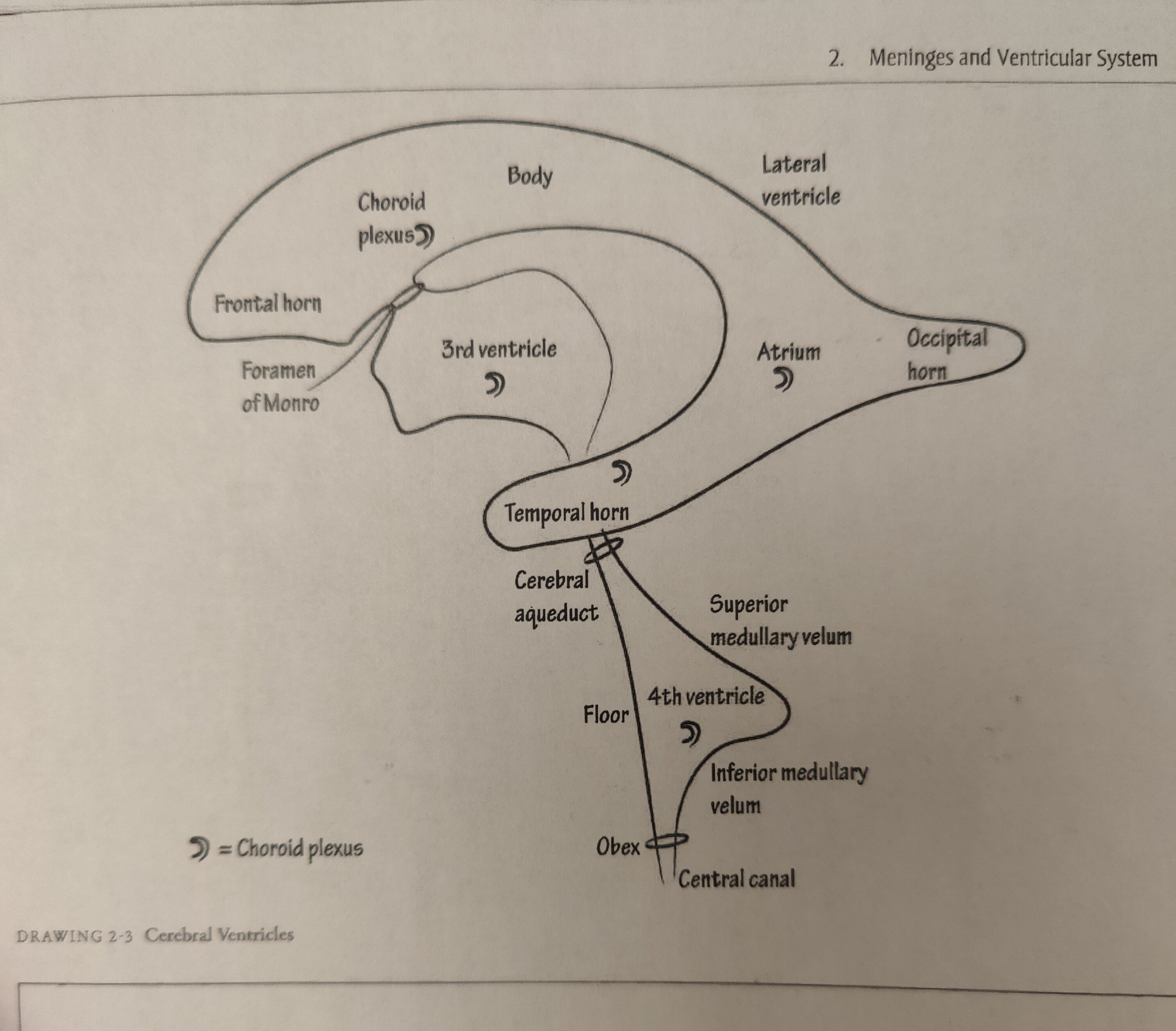
The Ventricles
*Diagram handed out in class is on exam 3
*know flow of ventricles for exam 3
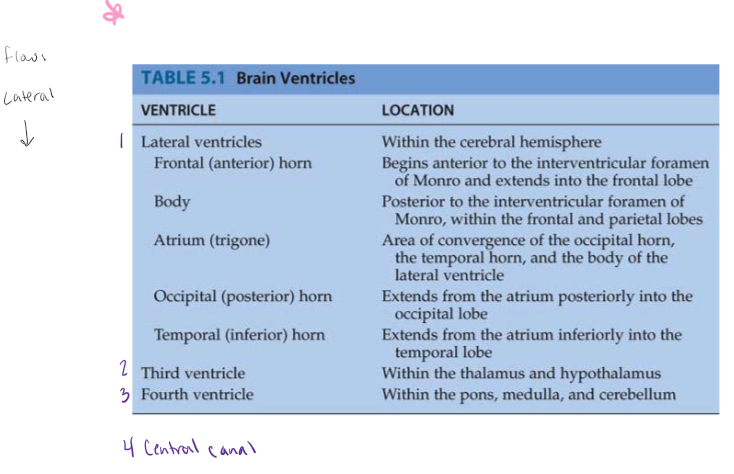
Cerebral Spinal Fluid (CSF) and the Ventricles
CSF is a clear fluid, similar to blood plasma. Formed in the choroid plexus. Foind in each lateral ventricle and the third and fourth ventricle. Composed of cuboidal epithelial cells resting on a basal lamina which are adjacent to highly fenestrated blood vessels separated by the stroma (lots of blood flow there). The tight junctions located between the apical parts of the choroid plexus epithelial cells form the blood-cerebrospinal fluid barriers (separation between 2 systems). CSF flows from the lateral to third to fourth ventricle to central canal or between meninges. CSF reabsorbed in arachnoid space between meninges and brain and spinal cord. CSF circulating at all times.
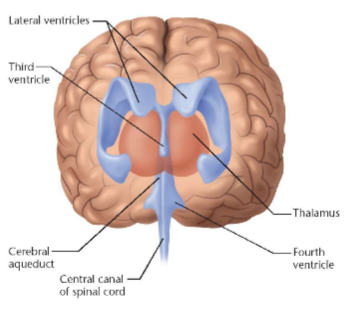
The Ventricular System
CSF Functions
Buoyancy, Protection, Chemical Stability, Prevention of brain ischemia
Buoyancy
The actual mass of the human brain is about 1400 grams; however, the net weight of the brain suspended in the CSF is equivalent to a mass of 25 grams.
Protection
CSF protects the brain tissue from injury when jolted or hit. (CSF provides some protection)
Chemical Stability
Allows for homeostatic regulation of the distribution of neuroendocrine factors, to which slight changes can cause problems or damage to the nervous system. For example, high glycine concentration disrupts temperature and blood pressure control, and high CSF pH causes dizziness and syncope (fainting). Too much CSF causes hydrocefellus
Prevention of Brain Ischemia
The prevention of brain ischemia is made by decreasing the amoint of CSF in the limited space inside the skull. This decreases total intracranial pressure and facilitates blood perfusion. Balance between vascular system and blood and CSF in the brain so there isn’t to much pressure in the brain.
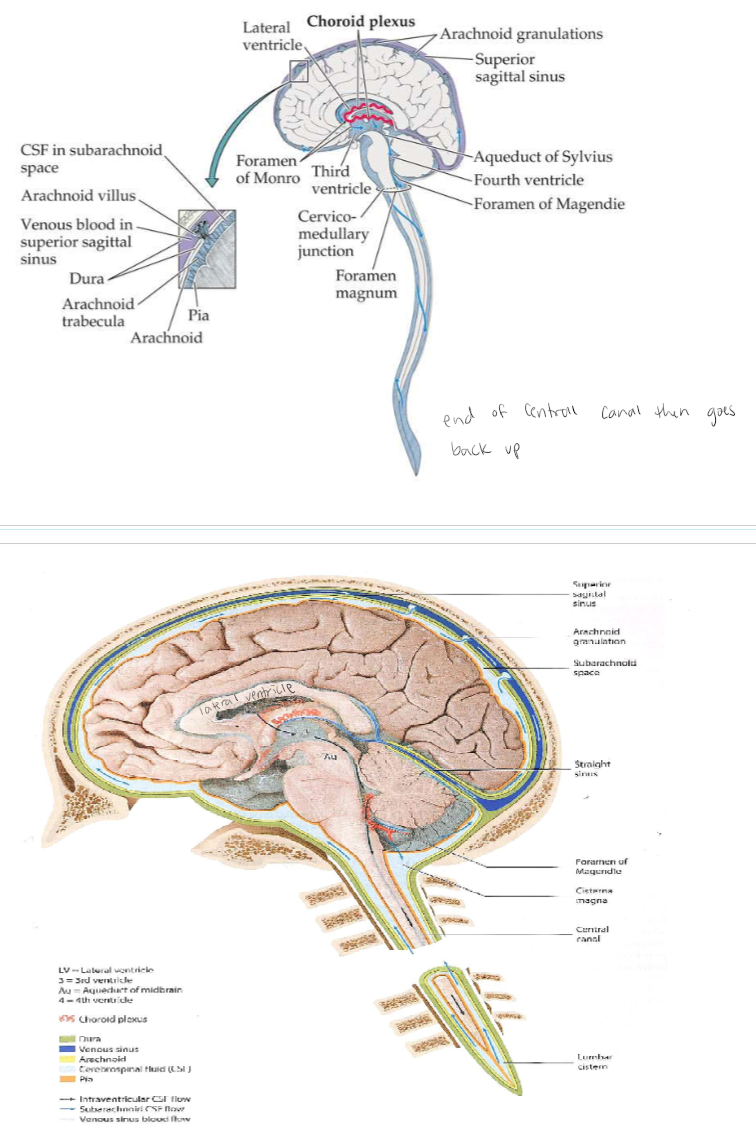
Cerebrospinal Fluid Circulation
red wave = choroid plexus. Foramen of Monro = connects lateral ventricle to 3rd ventricle. Central canal space surrounding spinal cord. In between meningal layers. CSF goes down and comes back up in subarachnoid space meningal layer.
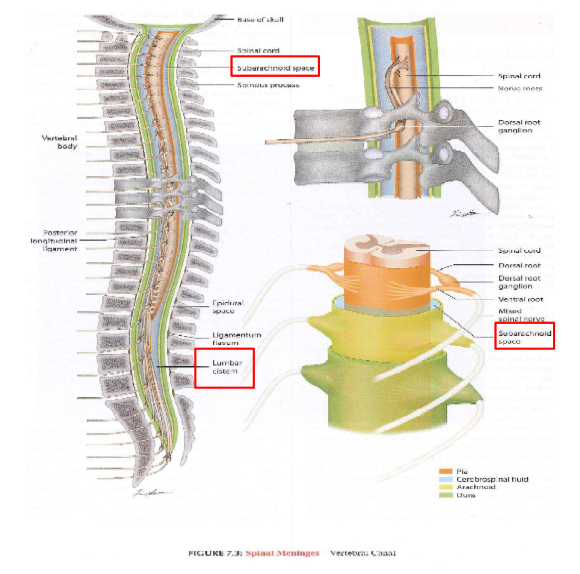
Spinal Ventricles
Lumbar cistern - area they aim for when taking CSF sample (cauda equina area)
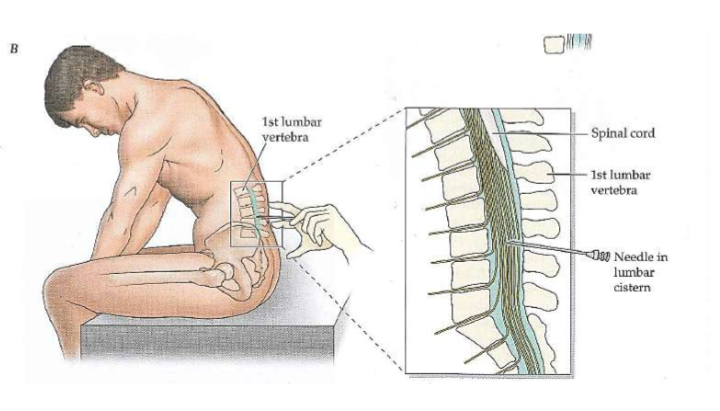
Spinal Tap
From the lumbar cistern
Handout from class on exam 3
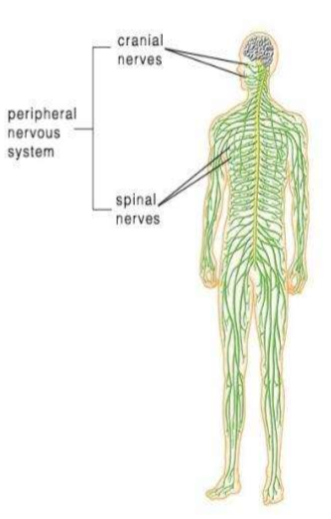
Peripheral Nervous System
Consists of the nerves that branch out from the CNS and connect it to other body parts, also includes the cranial nerves.
Somatic Nervous System
(Conscious activities) Skin, skeletal system
Autonomic Nervous System
(Unconscious activities); heart, viscera, glands
Peripheral Nervous System Explained
The spinal nerves comes out of the spine, and the cranial nerves come out of the brain directly. There are 12 pairs of cranial nerves. They are numbered with Roman numerals.
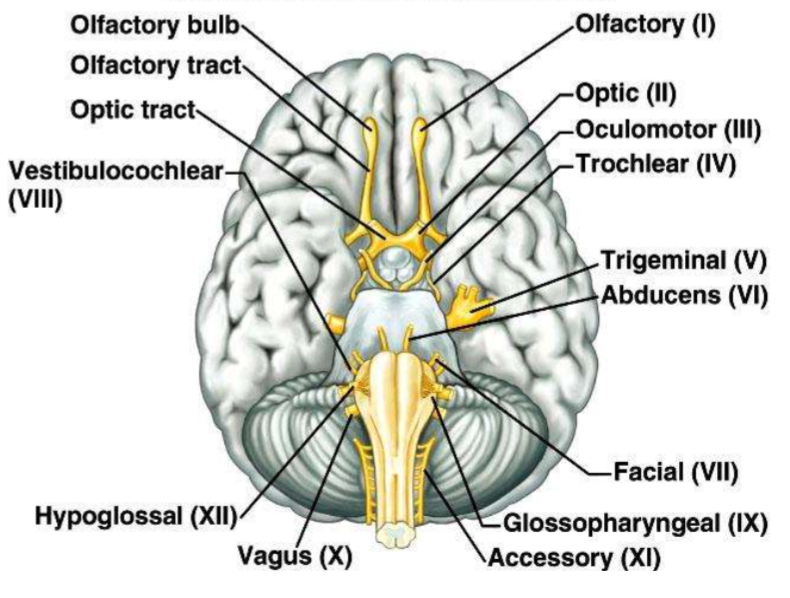
12 Pairs of Cranial Nerves
1.Olfactory (1) 2. Optic (II) 3. Oculomotor (III) 4. Trochlear (IV) 5. Trigeminal (V) 6. Abducens (VI) 7. Facial (VII) 8. Glossopharyngeal (IX) 9. Accessory (XI) 10. Vagus (X) 11. Hypoglossal (XII) 12. Vestibulocochlear (VIII)
*Be able to label this
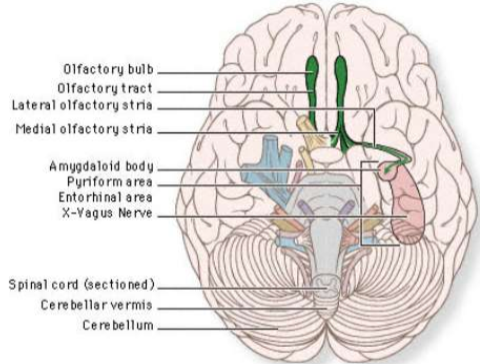
Olfactory (I)
Transmit the sense of smell. Outside of the CNS they are called olfactory nerves, and inside of the CNS they are called the olfactory tract.
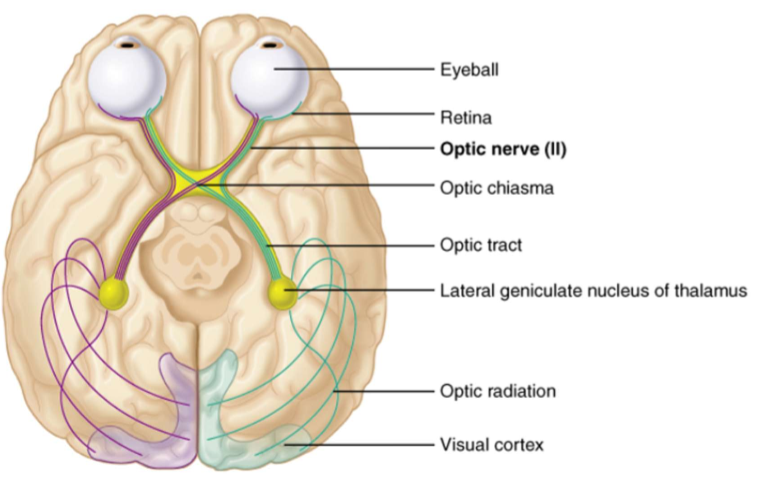
Optic Nerve (II)
Transmits information from the eye’s retina.
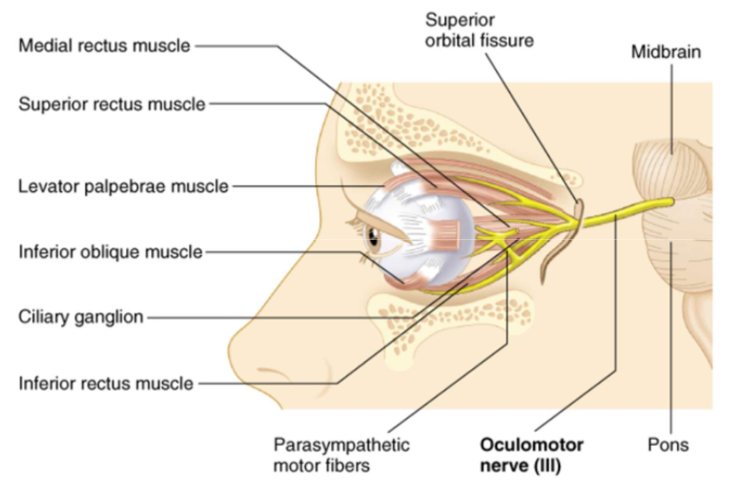
Oculomotor Nerve (III)
This controls most of the extrinsic muscles that move the eyeball; superior, medial, and inferior rectus muscles.
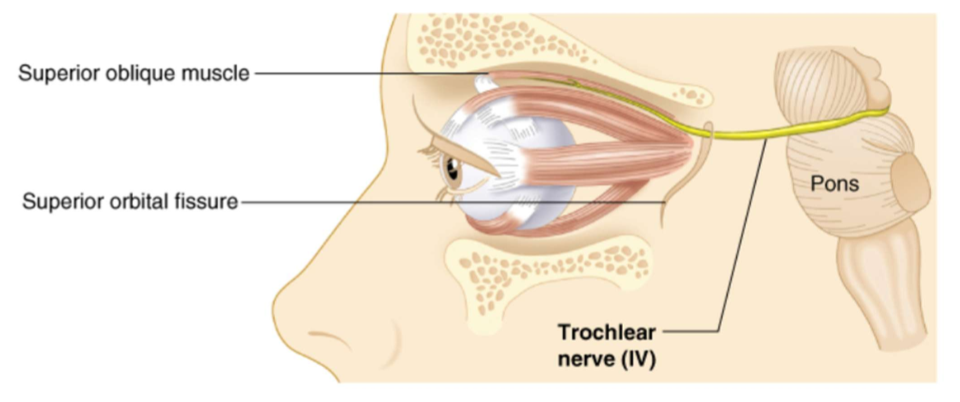
Trochlear Nerve (IV)
Innervates the extrinsic oblique eye muscle.
Trigeminal Nerve (V)
This is the main sensory nerve of the face. It has a large branch that passes through the foramen ovale of the skull. It has three parts.
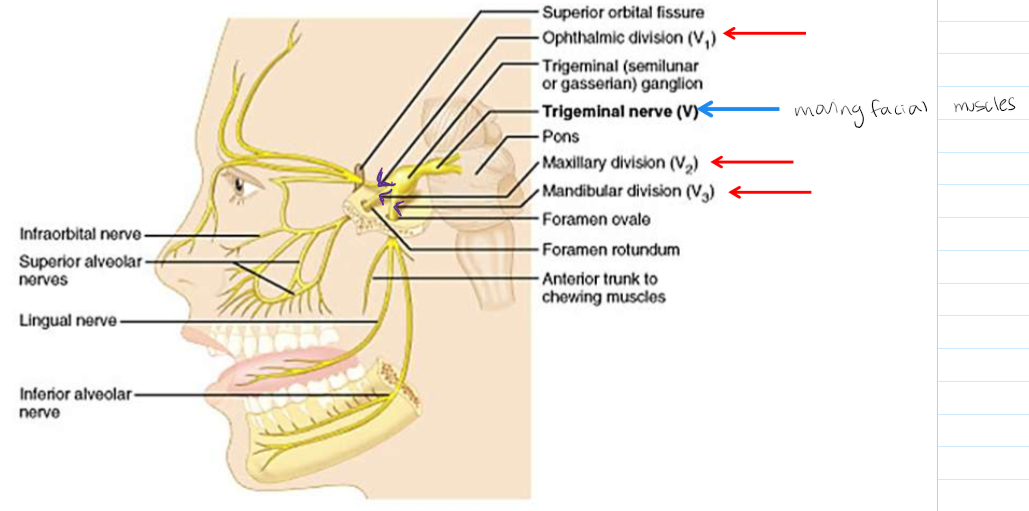
Three branches of Trigeminal Nerve
Ophthalmic (V1) branch, Maxillary (V2) branch, Mandibular (V3) branch.
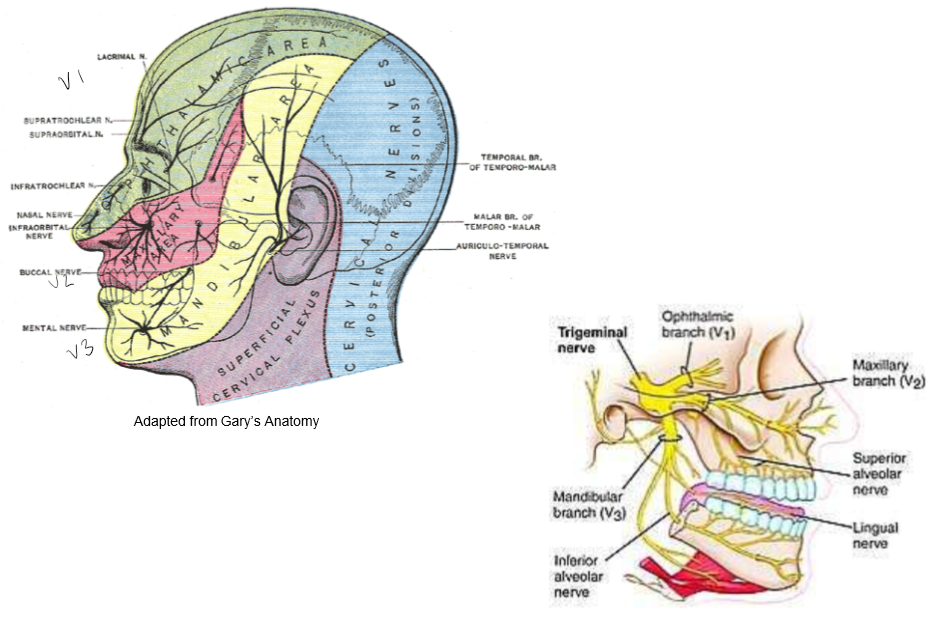
Ophthalmic (V1) Branch
A) carries sensory information from scalp, forehead, the upper eyelid, the
conjunctiva and cornea of the eye
B) the nose, the nasal mucosa, the frontal sinuses
C) parts of the meninges (the dura and blood vessels). Top of the face.
Maxillary (V2) Branch
A) carries sensory information from the lower eyelid, cheek, and upper lip, the upper teeth and gums
B) the nasal mucosa, the palate and roof of the pharynx, the maxillary, ethmoid and sphenoid sinuses, and parts of the meninges. Middle of the face