637 Outcome Measures & Examination
1/36
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
When would you modify exercise based on changes in HR, systolic BP, and diastolic BP?
If HR drops or does not increase incrementally in response to exercise = abnormal (EXCEPT w/ BB), modify
If systolic BP drops below baseline during exercise or >20 mmHg during position changes = abnormal, modify
If diastolic BP increases >10 mmHg = modify
What are BP recommendations by ACSM for testing and physical activity?
0-1 risk factor for adverse cardiac event, asymptomatic, and BP <180/110 mmHg = no additional testing for light to moderate activity (60% VO2 max)
Multiple CVD risk factors and BP > 180/110 mmHg = need no additional testing before light or very light activity (<40% VO2 max); need additional testing before moderate activity (60% VO2 max)
Pts dx w/ CVD (ischemia, stroke, HF) = require exercise testing before moderate and vigorous activity, should occur at cardiac rehabilitation (>60% VO2 max)
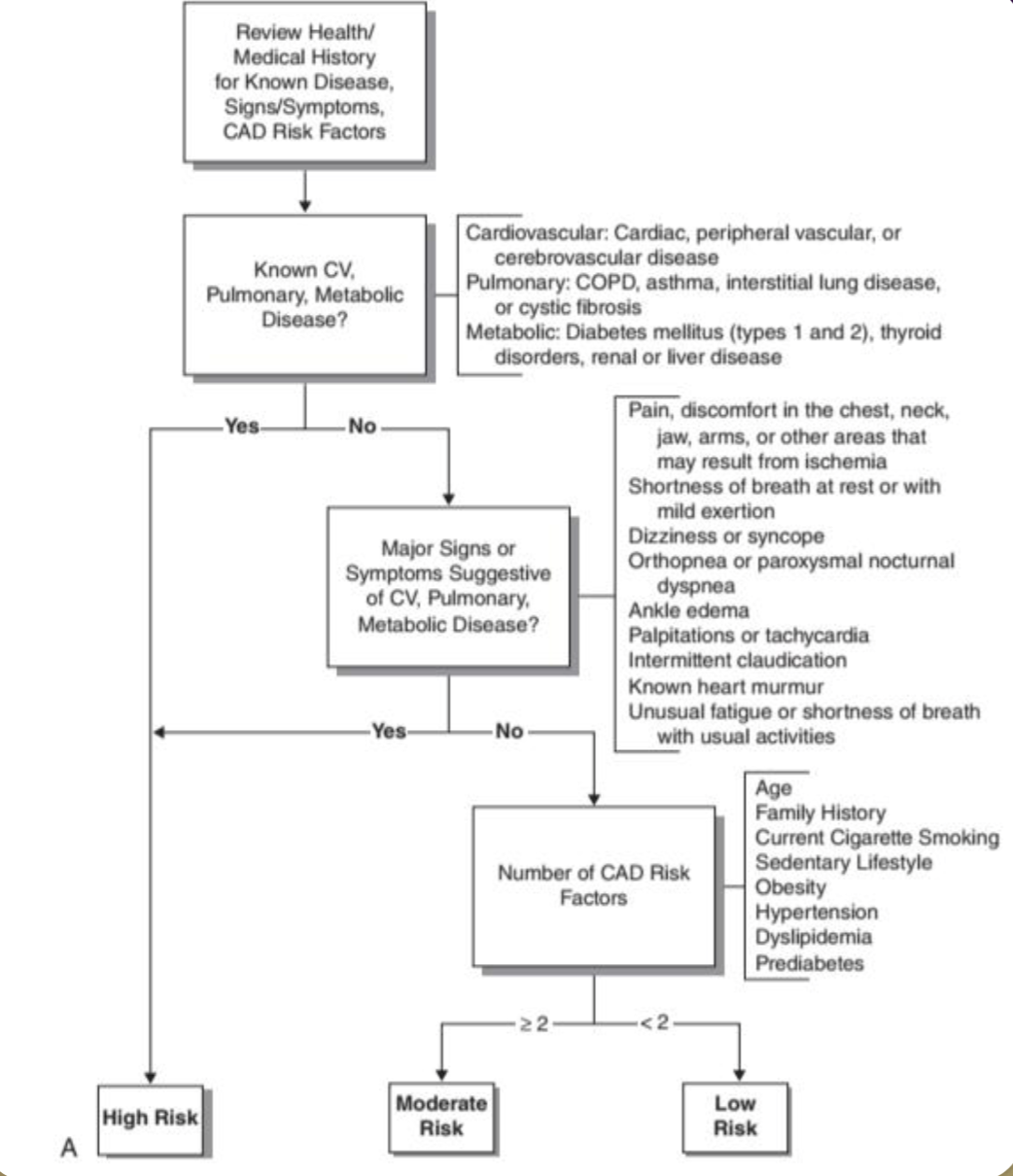
What is ACSM’s pre-screening for exercise testing criteria for high risk, moderate risk, and low risk?
After reviewing health/medical hx for known dx, sxs, CAD RF:
Known CV, pulmonary, metabolic disease
Yes → High risk
No → Major sxs suggestive of CV, pulmonary, metabolic disease?
Yes → High risk
No → Number of CAD RF?
2 or more = moderate risk
<2 = low risk
If a patient has a PMH of CV, pulmonary, metabolic disease what is their ACSM pre-screening risk level for exercise testing?
High risk automatically
What are ACSM guidelines for test selection?
Low risk - asymptomatic, 1 or more RF
Mod & vig ex - not rec
Submax & max - not rec
Moderate risk - asymptomatic, 2 or more RF
Mod ex - not rec, vig ex - rec
Submax - not rec, max - rec
High risk - symptomatic, or known cardiac, pulmonary, or metabolic disease
Mod & vig ex - rec
Submax & max - rec
What is the goal of VO2peak/max testing?
Get VO2peak as close to VO2max as possible
What is the difference between VO2 max and VO2 peak?
VO2 max = sum value O2 consumption w/ all muscles working maximally
Most exercise tests only use arms or legs
Exercises can also work extremities in diff ways & yielding diff muscle mass engagement (cycling vs walking)
Requires maximal exercise testing while a metabolic evaluation is performed to ensure physiologic capacity is reached and max HR
Also called maximal aerobic power = maximal rate of aerobic glycolysis (aerobic capacity speaks more accurately
VO2 peak = sum value O2 consumption during a given exercise
This value can be diff during diff exercises as diff masses of muscles are being used EX:
Leg work > arm work
Treadmill walking/running > cycle ergometer
The more muscle groups involved during an exercise the closer VO2 peak gets to VO2 max = goal
How does Garmin measure relative VO2 max?
Uses body weight
Most predictive outside & running
Not entirely accurate but good for trends
VO2max from a smartwatch or fitness tracker = RELATIVE VO2max
How much O2 you can use per kg of body weight in 1 min
*What do the different values of ABI represent? When is immediate medical attention required?
0.9-1.10 = normal
0.5-0.9 = PAD (can be asymptomatic)
<0.5 = critical limb ischemia
<0.2 = severe ischemia, need immediate medical attention
When should an ABI be done? How is it taken?
Pt has multiple RF for CVD
Pt in supine
Locate brachial A. on UE and dorsalis pedis/posterior tibial artery on LE
Take average of 3 systolic BP of UE and LE
Average of BP LE is divided by average of BP UE
What is the gold standard test for COPD?
FEV1/FVC
What are PFTs and CT scans used for? What should it be combined with? What is a graded exercise stress test used for?
PFTs and CT scans can define COPD severity, NOT a good measure of fx, only lung capacity
Combine w/ muscle strength, joint mobility, balance, etc.
Graded exercise stress test used for exercise prescription, can diagnose CAD
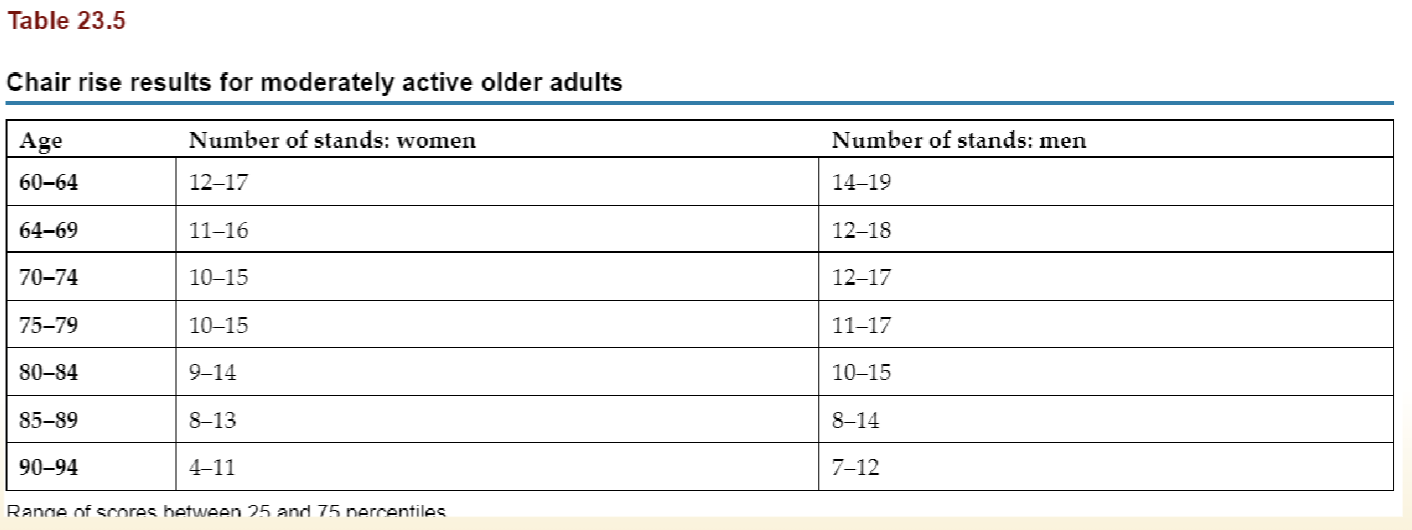
What are the chair rise tests?
Measures LE strength and endurance
30s chair rise test - CAN USE ARMS, chair 17” in height, PT counts # of STS in 30s
5x STS test - CANNOT USE ARMS, chair 16-17”, length of time it takes a pt to perform 5 STS, incomplete is a failure
What is the seated step test?
Chair is 18” tall w/ 6” step or bar placed in front of the pt
Pt alternates which foot they place on the step in front of them to a 60bpm pace
1. Pt alternates for 3 min, PT records HR
2. Higher bar of 12” for 3 more min (or fatigue), PT records HR
3. Higher bar of 18” for 3 more min (or fatigue), PT records HR
4. Sam bar for 18” w/ alt UE flexion to 90* for 3 min (or fatigue), PT records HR
Test is correlated w/ thigh muscle mass & peak torque
What is the 2 minute step test?
Pt standing and alternates lifting LE to a height midway btwn opposite patella and iliac crest
PT counts # of times RLE reaches appropriate height
65x or less places pts in high risk category
Can be used in place of 6MWT for endurance and functional capacity
What is the 6 minute walk test? What distances lead to increased mortality? Minimum distance needed for pre-transplant? What distances lead to shorter hospital stays?
Equipment: 100’ hall or 50’ intervals, timer, chair, vital monitor
Pt should wear comfortable clothes, shoes, and use an AD if needed and should have not exercised vigorously 2hrs before the test
Test parameters should be reviewed w/ pt prior to starting as well as the need to report adverse sxs
PT should provide neutral encouragement about 1x/min as well as provide update on remaining time
All rest breaths, vitals, and total distance should be documented
Distances less than 985’ related to increased mortality; >1000’ pre-transplant leads to shorter ICU stays; >750’ leads to shorter hospital stays
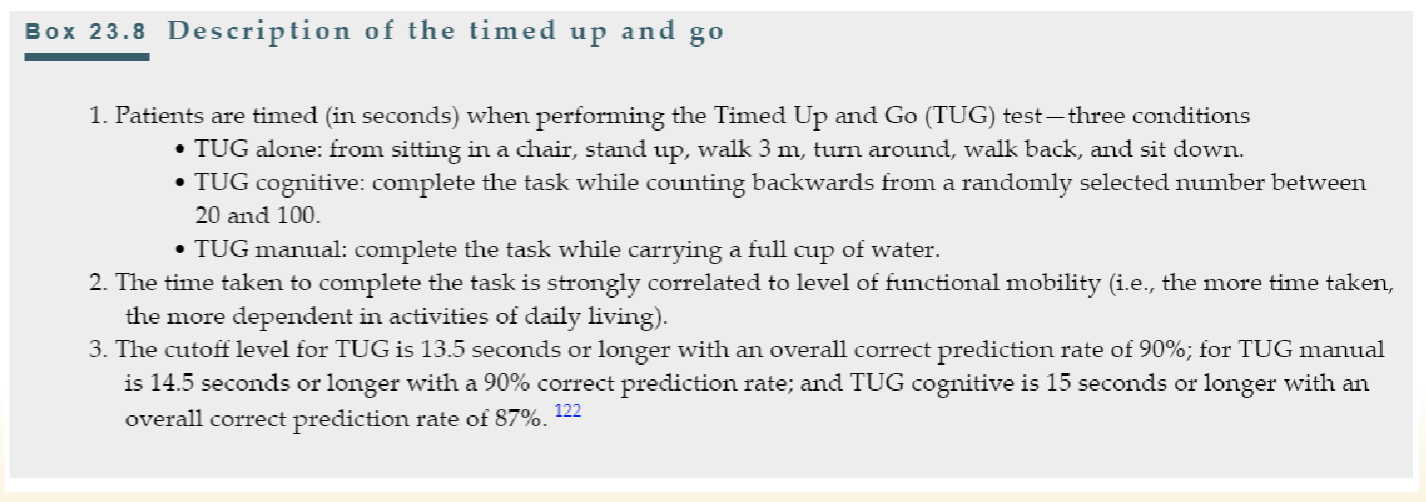
What is the timed up and go test?
Slower speed is associated w/ increased risk of MI, CHF, and mortality (>20s)
MCID is 3.4
What is the gait speed test?
Equipment: 6m straight path, obstacle free (1m for acceleration and deceleration)
PT starts timer after 1st meter and ends at 5th meter (speed divided by 4m to get m/s speed)
MCID is 0.1 m/s
*How do functional tasks relate to gait speed?
1.5 mph <2 METs = self care
2.0 mph 2.5 METs = household activities
2.5 mph 3.0 METs = carry groceries, light yard work
3.0 mph 3.5 METs = climb several flights of stairs
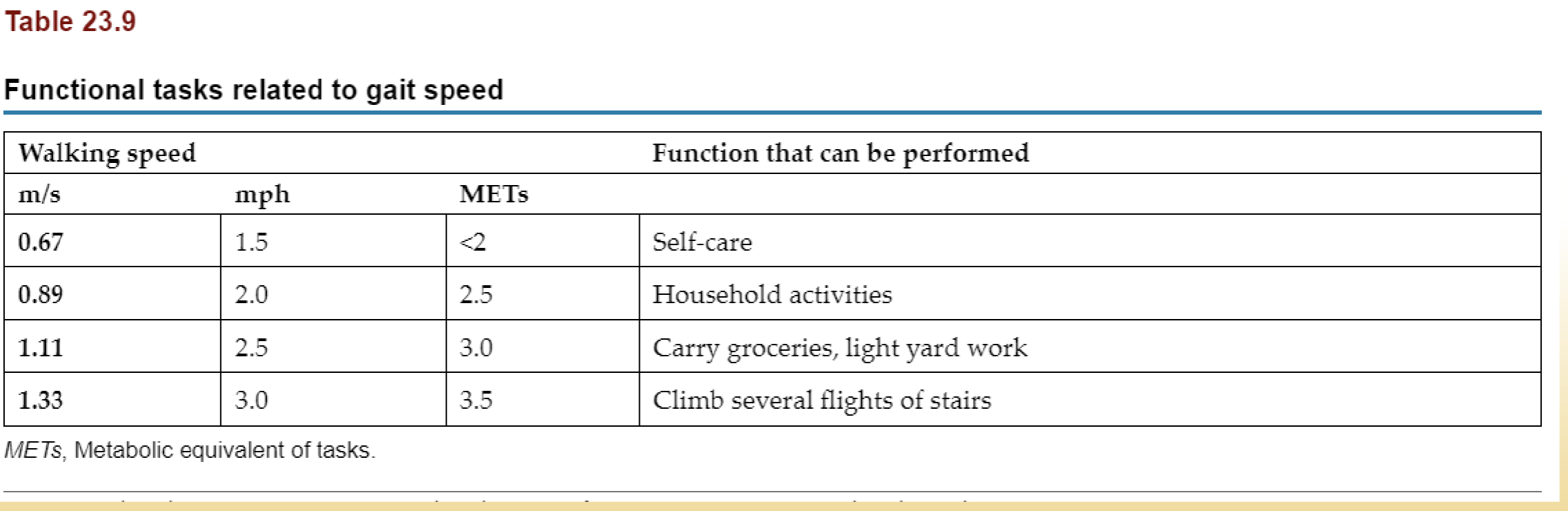
*What walking speed is required for self care, household activities, carrying groceries, light yard work, and climbing several flights of stairs?
1.5 mph for self care
2.0 mph household activities
2.5 mph for carrying groceries and light yard work
3.0 mph for climbing several flights of stairs
What is the short physical performance battery predictive of? What score is predictive of mortality? What does it comprise of?
Predictive of functional decline and hospitalization
<10 = predictive of mortality
Composed of static balance tests, 4MWT, 5xSTS
How do the balance tests progressed? Standard balance test used?
Progressed from narrow BOS, semi tandem, tandem for 10s each
BERG balance
What kind of outcome measure test can be used in the ICU to assess mobility?
Perme Intensive Unit Care Mobility Score
Measures pt’s mobility in ICU when ability to complete the FIM is limited, helps determine discharge status
15 item w/ scores 0-32, the higher the score, the fewer the mobility barriers
7 categories: mental status, potential mobility barriers, transfers, gait endurance, bed mobility, and functional strength
What does a high score on the Perme ICU scale mean?
better; fewer mobility barriers
What does the seattle angina questionnaire measure?
How impactful or limiting chest pain is on ADLs
*What are some of the standardized tools to screen for depression, what do they measure, and what settings can they be used in?
Centers for Epidemiologic Studies Depression Scale (CES-D)
Depression sx across 20 activities
Psychological Risk Factor Survey (PRFS)
Depression, anxiety, anger/hostility, social isolation, emotional guardedness
Beck-Depression Inventory-2
Measures depression severity
Patient Health Questionnaire (PHQ-9)
Activity interest, feelings of depression, sleeping disturbance, energy levels, eating habits, concentration, and thoughts of suicide
Hospital Anxiety and Depression Scale (HADS)
Detects presence and severity of mood disorder, anxiety, and depression
Name all the parts of an evaluation of a patient with a CV/P condition.
Examination
Evaluation
Diagnosis
Prognosis
Intervention
Outcomes
Reexamination
*What are clinical and nonclinical factors that affect patient outcomes?
Clinical factors
Principal diagnosis, severity
Acute clinical stability
Comorbidity, severity
Physical functional status
Age, sex
Nonclinical factors
Health-related QoL
Cultural, ethnic, and socioeconomic attributes, beliefs, and behaviors
Patient attitudes and preferences
Psychologic, cognitive, and psychosocial functioning
*What are clinical and nonclinical factors that affect diversity of patient outcomes?
Clinical factors
Severity of principal diagnosis
Acute clinical stability
Comorbidity, severity
Physical functional status
Complications, iatrogenic illness
Survival
Nonclinical factors
Health-related QoL
Resource utilization
Costs of care
Satisfaction
What are some questions you can ask a patient regarding activities?
Do you have enough energy for everyday life?
Are you able to accept your bodily appearance?
Do you have enough money to meet your needs?
How available to you is the information that you need in your day-to-day life?
To what extent do you have the opportunity for leisure activities?
Besides patient participation, what else can structure and function limit?
O2 transport
What are key needs for a PT to assess?
Determining health and possible complications
Identify risk factors
Work collaboratively with the multidisciplinary team
Provide education and lots of it
Increased risk factors requires increased monitoring and possible referrals for additional medical procedures/recommendations
Provide necessary and appropriate interventions with adjustments needed
Medications and coordination with therapy and/or exercise
Why are diagnoses or problems made for CV/P conditions? What factors may impair O2 transport? What factors threaten O2 transport? Intervention goals?
Primarily made to describe O2 transport deficiency, participation, and activity restrictions due to structure and function limitations
Impair O2T
Functional limitations and physiological limitations
Threaten O2T
1-2 hr turning cycle to improve O2 of pts w/ poor mobility through increased ventilation and circulation
Factors that improve or worsen O2T: CV/P pathophysiology, restricted mobility, recumbency, extrinsic & intrinsic factors
Restricted mobility & recumbency: over utilized intervention that has widespread negative impacts on O2T
Intervention goals
3 categories: short, long, preventative
Delay or reduce need for invasive care
What are questions that you would consider when diagnosing limitations in O2 transport?
What factors contribute to which steps in the pathway?
What factors threaten O2 transport?
What is the magnitude of the factors and what is the priority?
How can PT help change/limit/improve O2T and how can PT modify interventions?
How does monitoring need to change pending factors involved
With factors & priorities determined, what interventions will be used and what is POC?
What is the intervention goal for CV/P conditions?
The demand for O2 does NOT exceed available normal supply
What are interventions that increase VO2 and metabolic demand?
Mobilization & exercise
Positioning
Arousal/anxiety/pain
Breathing control
Coughing
Postural drainage & manual techniques
Suctioning
ROM
What are the short-term, long-term, and preventative goals of intervention?
Short term
Avoid worsening condition
Correct dysfunction
Empower client to improve
Long term
Enhance efficiency
Reduce need for medications/drugs
Preventative
Prevent multisystem complications
Maximize O2T and aerobic activity
Reduce impact of lifestyle conditions