Lecture 3 - Prostate kV/kV Image Matching + Rotational Translations
1/39
Earn XP
Description and Tags
ONCOL 306 - Imaging. University of Alberta
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
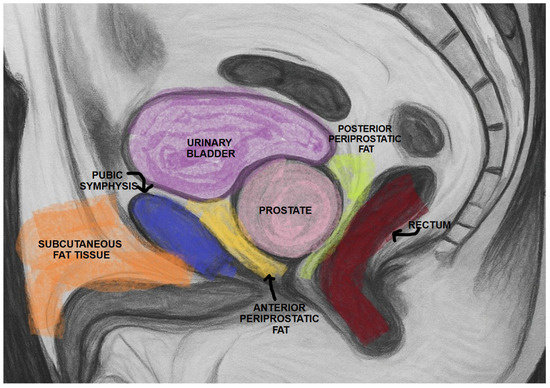
what is the best bony primary match structure of the prostate
the pubic symphysis
lies directly anterior to the prostate

On CTs, sometimes we can see white spots on the prostate. what pathology are these?
these are typically calcifications
what is the most important soft-tissue matching area on transverse CT for prostate patients?
prostate-rectal interface
how does rectal anatomy affect prostate position
width
ant/post rectal length
rectal width does not significantly affect prostate position but increased ant/post rectal length will shift prostate anteriorly
when should a patient be taken off the bed to manage rectal issues?
if rectal gas or stool is present, the patient may need to pass gas or empty rectum before imaging
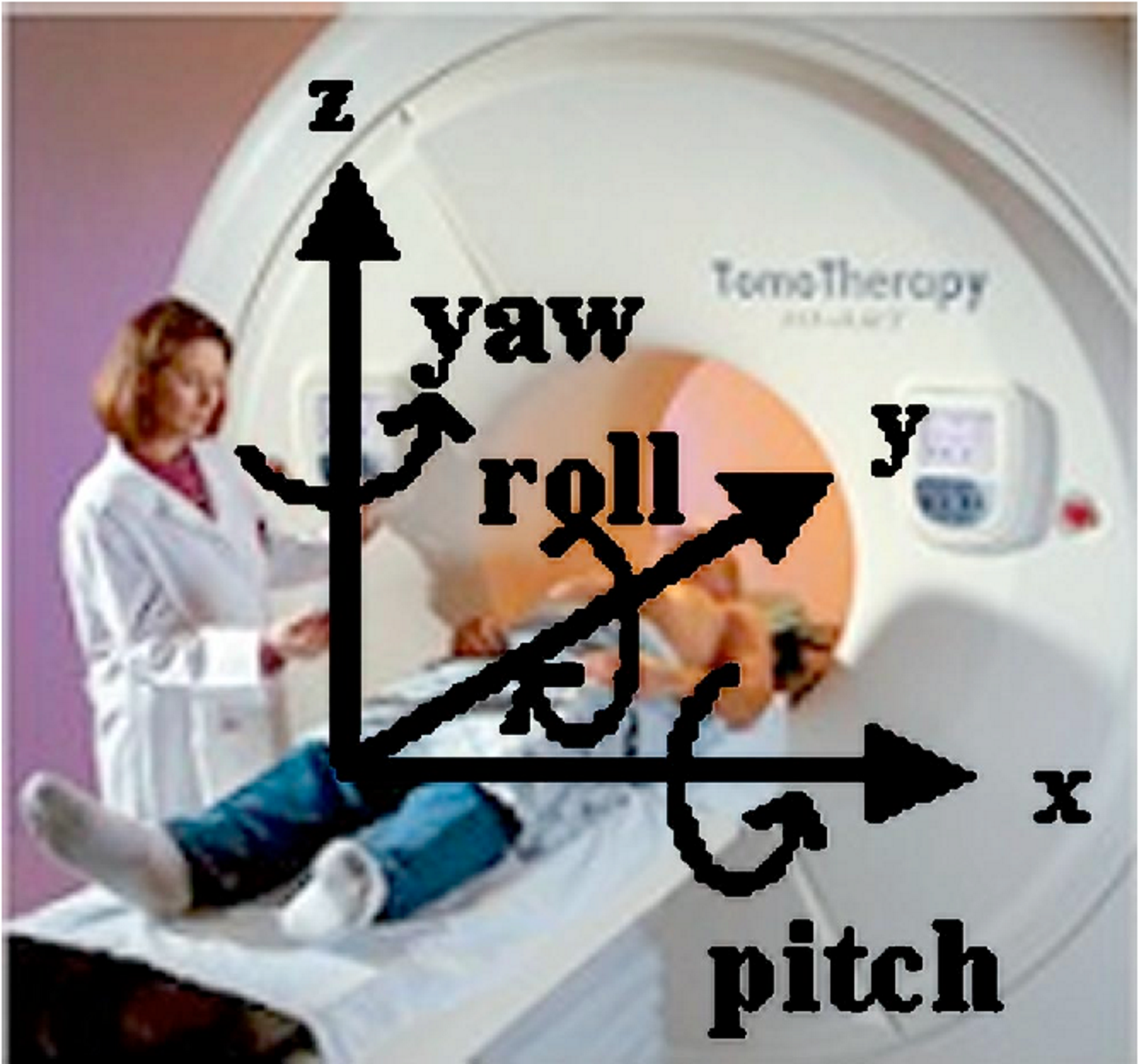
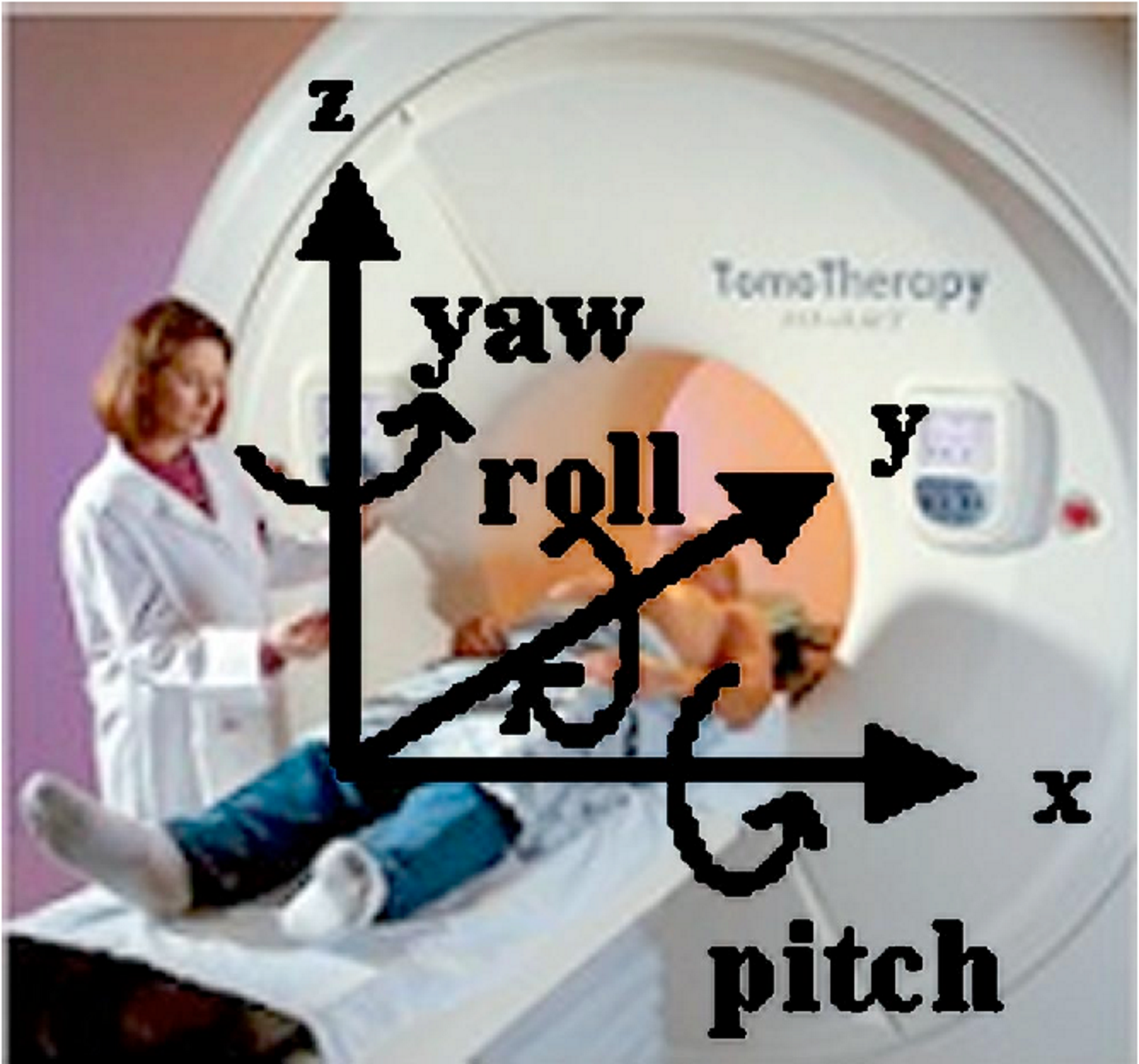
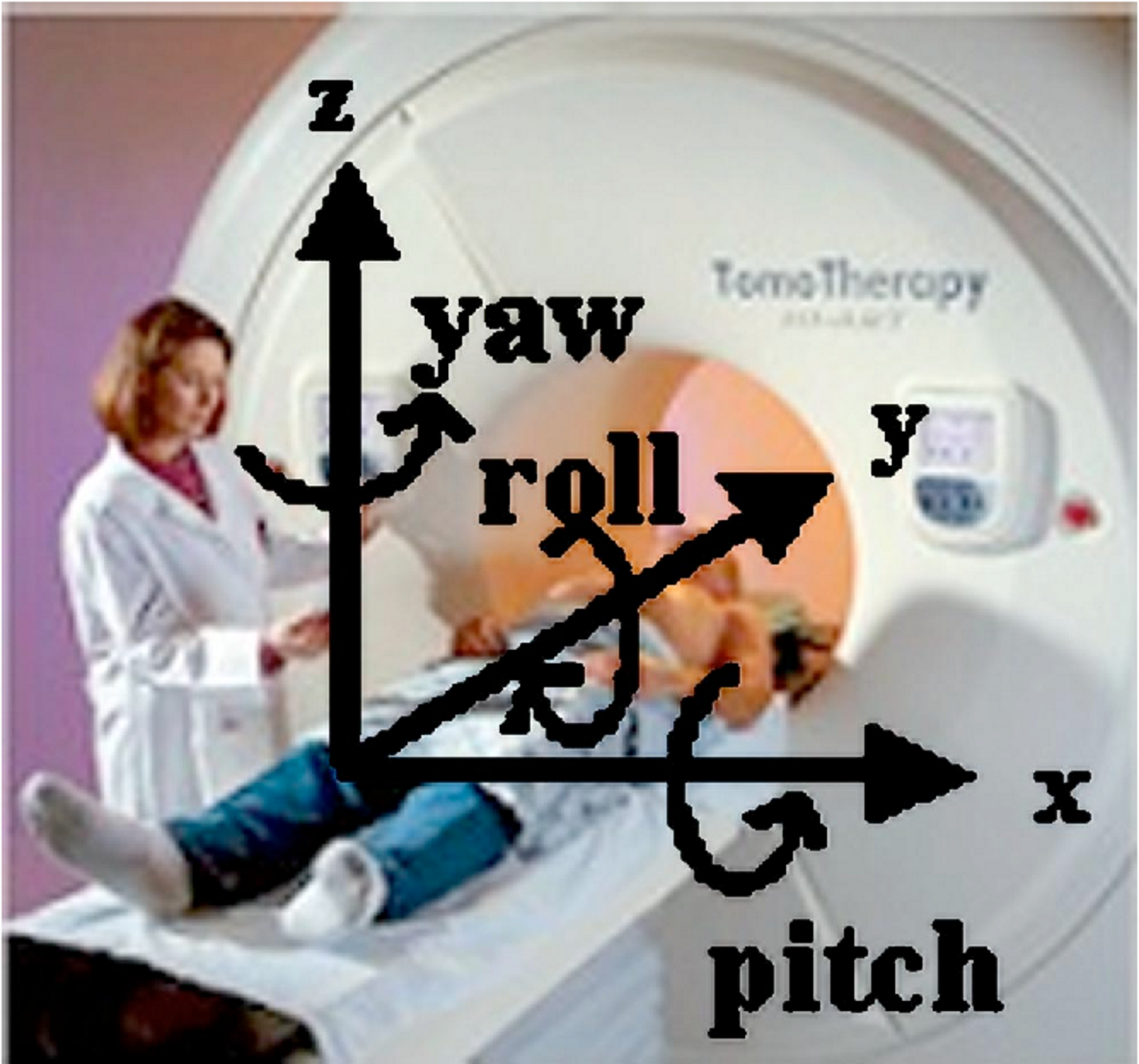
on a CT, if one femoral head appears more anterior than the other, what rotational movement is indicated?
a roll
what method is used if the patient’s tattoos are not aligned with isocenter?
the patient is being treated with a shift method: align to tattoos first, then apply couch shifts to isocenter
why is the isocenter placed more superior in prostate in high risk patients?
to include nodal volumes in PTV
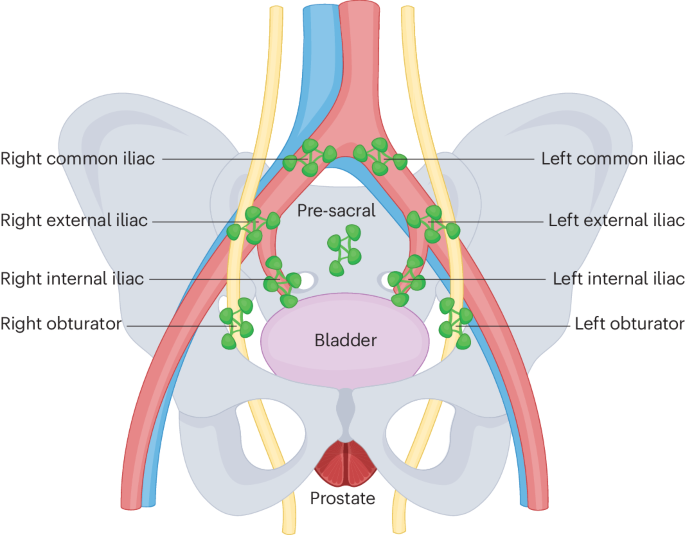
what three structures are included in the PTV for high-risk prostate patients?
prostate, seminal vesicles, and pelvic lymph nodes

On a MV right lateral image, what bony anatomy can be used to assist with the match
the pubic symphysis and the sacrum
why are the femoral heads not reliable for prostate matching?
they do not correlate well with prostate position

what are primary and secondary match structures on AP imaging?
primary: pubic symphysis or pelvic brim
secondary: obturator foramen or iliac crests

what rotational translation could be suggested with a mismatched obturator foramen?
A roll rotation: one hip is higher than the other
why is glute relaxation important for prostate set-up
tension cen introduce rotation or positioning error
patients may need to lift and relax
what can kV/kV imaging be matched to?
bony anatomy only
what adjustments are made during the A/P image match
left/right and sup/inf
what adjustments are made during the lat image match
ant/post
why can’t rotational errors be corrected with couch shifts?
couch shifts correct translational movements (x,y,z) not rotation
what is the consequence of an uncorrected roll in high-risk prostate cancer patients?
part of the PTV (especially nodal volumes) may fall outside the treated area, increasing rectal dose
what rotational error does a sup/inf mismatch on A/P suggest?
a pitch issue
during patient set-up, the lateral tattoos align but the anterior tattoo is inf of laser. what has occurred?
there is most likely a bladder filling issue
what characterizes a yaw rotational error?
Obvious hip asymmetry (rotation around the z-axis)
requires repositioning the patient.
why must superior anatomy be included in matching for high-risk prostate patients
because nodal volumes extend superiorly beyond the prostate
what is the most primary match structure for prostate on lateral imaging?
sacrum is used typically as pubic symphysis is often blurry
if pubic symphysis is sharply defined you an use that
what two structures should not be used as primary match structures for prostate?
iliac crests and femoral heads
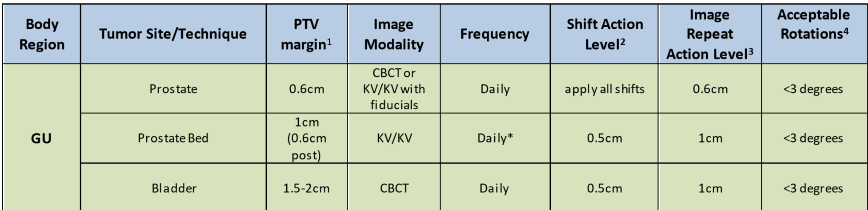
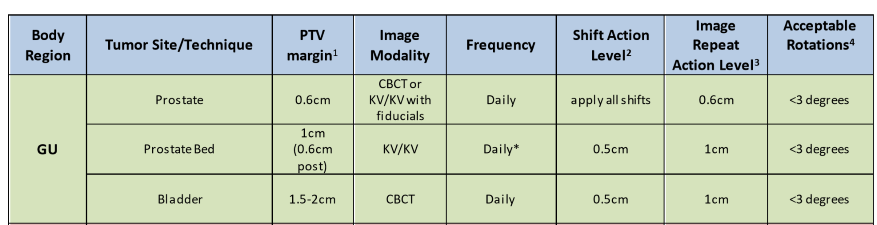
what is the prostate bed shift action level
half of the PTV margin (1 cm) = 5 mm
if shift is larger than 5 mm, apply shift
if below, we don’t need to apply
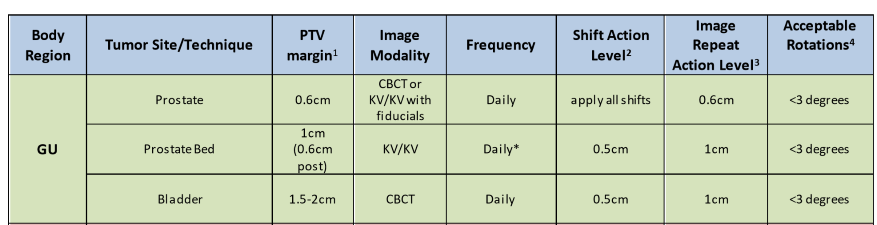
when can shifts be applied without repeat imaging for prostate bed?
when all shifts are below 1 cm (image repeat action level)
what should be assessed during the initial global image review prior to image matching
symmetry, bone alignment, rotations, and pathologies (fractures, zippers, and buttons)
why must bladder and bowel prep issues be addressed before matching?
A full rectum or empty bladder can significantly displace the prostate, making matching unreliable.
What is the recommended three step matching sequence for prostate imaging?
global assessment
AP match (sup/inf, left/right)
Lateral match (ant/post)
What is the goal of the global assessment before image matching?
Assess symmetry, rotations, bony alignment, and obvious positioning errors.
What structures are useful for assessing symmetry during global assessment?
Obturator foramen, pelvic inlet, iliac crests, femoral heads.
What common artifacts or issues should be ruled out during global assessment?
Zippers, buttons, foreign objects, fractures, or hardware.
why can the pubic symphysis be unreliable on lateral imaging?
it can appear blurry and difficut to visualize clearly
What indicates a roll error on a/p imaging
Pelvic inlet or obturator foramen not lining up; one hip higher than the other.
Can translational couch shifts correct roll, pitch, or yaw?
No—rotational errors require patient repositioning.
What is the dosimetric consequence of uncorrected roll in high-risk prostate?
PTV (especially nodes) may be missed and rectal dose may increase.
Why are skin tattoos not always reliable?
External alignment does not always reflect internal anatomy.
What indicates an acceptable final match despite minor discrepancies?
Iliac crests level, no clear rotation, AP and lateral matches aligned.
When is repeat imaging required for prostate patients?
When any shift exceeds 1 cm.