In class lab worksheets+, 2nd tri/placenta, Ovary Path
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
119 Terms
Homogeneous equal sized lobes with a central cord attachment. Chief complaint is vasa previa or post partum hemorrhage from retained products.
Bilobed

One or more multiple accessory lobes connected to the main part of the placenta. Chief complaint is a velamentous or eccentric cord, vessels connecting 2 segments can rupture during delivery or post partum hemorrhage when a lobe is left in
Succenturiate

Occurs when the chorionic plate is smaller than the basal plate. Umbilical cord can insert anywhere it is central or eccentric. Chief complaint is placental abruption and hemorrhage
Circumvallate
Smooth and homogeneous. There is central or eccentric cord insertion with no obvious complications
Normal placenta
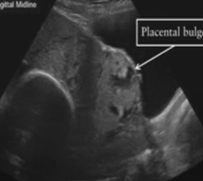
Swiss cheese appearance. Penetration of the chorionic villi through all uterine layers. Bulging of the placenta, vascular lacunae and no distinguishable myometrium layer. Cord is central or eccentric. Chief complaint is pt will need hysterectomy
Percreta
When the placenta embeds into the muscular wall of the uterus with a central or eccentric cord insertion. Chief complaint is preterm labor or possible hysterectomy
Increta
The chorionic villi is attached to the myometrium without muscular invasion. Cord is central or eccentric. Chief complain is pt may need a D&C
Accreta

Normal finding of anechoic regions with no blood flow detected. Can be irregular shape. Chief complaint is IUGR
Placental lakes
Occurs on the fetal surface of the placenta. Rare well circumscribed, oval anechoic masses originating from remnants of allantois or umbilical vesicle. They are simple in nature but may cause IUGR
Placental cysts

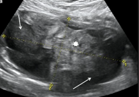
Hydrosalpinx USA
Dilated tubes near ampulla with pointed beak near isthmus, Colicky pain, Sausage appearance of tortuous tubes with anechoic fluid, cogwheel sign
Hydrosalpinx Clinical S/S
Asymptomatic, Pelvic fullness/discomfort, Low grade fever, colicky pain in reproductive women, common with PID
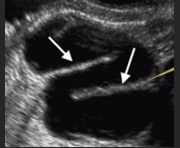
Hydrosaplinx
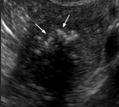
Pyosalpinx USA
Complex mass like distention, poor transmission, internal low-level echoes within a sausage appearance, tortuous tubes
Pyosalpinx Clinical S/S:
Asymptomatic
May have pelvic fullness/discomfort, leukocytosis, low grade fever within reproductive women, common w/PID

Pyosalpinx
Tubal-ovarian abscess USA
Complex adnexal mass difficult to differentiate pelvic structures, multiloculated, later stages of PID, usually unilateral
Tubal-ovarian abscess Clinical S/S:
Pelvic fullness/discomfort, low grade fever within reproductive women, common w/PID
Tubal-ovarian abscess
Paraovarian cyst USA
Simple cyst with thin deformable wall not surrounded by ovarian tissue, can be large enough to extend to Abd.
Paraovarian cyst Clinical S/S:
Asymptomatic: non functional, pelvic pain in any age but from REPRO-PERIMENO, common
Paraovarian cyst
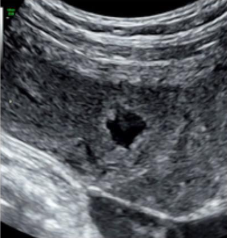
Endometritis USA
Enlarges UT, irregular endo, air in endo, fluid in posterior cul de sac
Endometritis Clinical S/S:
Dysmenorrhea, leokocytosis, menorrhagia, fever, associated w/C-section, abortion, IUD perforation, ROC and Bx, common in reproductive women

Endometritis
PID USA:
Difficult to distinguish borders, Most likely bilat, Review USA for hydrosalpinx, pyosalpinx and TOA often associated with PID, Beads on a string sign, Cog wheel signs, adhesions
PID S/S:
Pelvic pain and tenderness, vaginal discharge, fever, dyspareunia, caused from STD, abortion, IUD, and trauma, common in reproductive women
PID (Acute: Stage 1-endometritis Stage 2- salpingitis Stage 3- TOA Stage 4- peritonitis Chronic- adhesions)
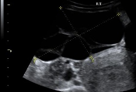
Peritoneal inclusion cyst USA
Multiloculated cyst in adnexa with clear delineation of normal ovary, spoke wheel, spider web
Peritoneal inclusion cyst Clinical S/S:
Pelvic pain or pelvic mass, Hx includes abdominal surgery or trauma, Rare but occurs in reproductive women

Peritoneal inclusion cyst
Fallopian tube carcinoma USA:
Complex mass adjacent to ovary - hydrosalpinx, sausage like cysts w/papillary projections
Fallopian tube carcinoma S/S:
Discharge, AUB, increased CA-125, associated with chronic salpingitis, nulliparity, BRCA gene, rare but occurs in premenopausal/Menopausal women
Fallopian tube carcinoma
Serous cystadenoma is the ______ most common benign tumor of ovary
2nd
Serous cystadenoma USA
Unilocular or multilocular cyst with THIN septations, can be bilat, NO PAP projections, smaller in size, no color flow
Serous cystadenoma Clinical S/S:
Pelvic pain and pressure, any age can get it
Serous cystadenoma (epithelial)
Mucinous cystadenoma USA:
Larger than serous cystadenoma, usually unilateral simple cyst, may have thin walled locules low level echoes from mucin, thin septations
Mucinous Cystadenoma Clinical S/S:
Pelvic pain and pressure, pseudomyxoma peritonei (mucin), common in reproductive/perimenopausal women
Dermoid is them most common ___________ tumor of the ovary
Benign
Dermoid USA
Complex solid mass, no central vascularity, thick irregular borders, “tip of iceberg” “Dermoid mesh”
Dermoid/Cystic Teratoma Clinical S/S:
Asymptomatic, slow growing, pelvic pain and fullness, increase AFP and hCG, may contain vb brine, teeth, hair, fat, palpable mass
Mucinous Cystadenoma (epithelial tumor)
Dermoid/Cystic Teratoma
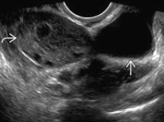
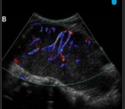
PCOS USA:
Bilateral enlarged ovaries, 15+ follicles per ovary, “string of pearls”
PCOS Clinical S/S:
Irregular menses, infertility - anovulation, obesity, endocrine disorder/imbalance, stein-Leventhal, androgen secreting/virilization (hirsutism, amenorrhea, increase testosterone, common with reproductive women

PCOS
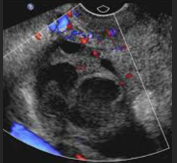
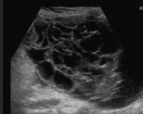
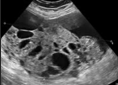
Theca Lutein cysts USA:
Bilat, multilocular cyst, grape-like clusters, no normal ovarian parenchyma
Theca Lutein cyst Clinical S/S:
Hyperemesis, elevated hCG, abdominal bloating, increases risk for torsion, associated with ovarian hyperstimulation or trophoblastic disease, common in reproductive women
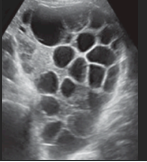
Theca Lutein Cyst
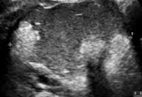
Fibroma USA:
Large, hypoechoic dense mass, usually unilateral, ascites and pleural effusion (Meig’s syndrome)
Fibroma Clinical S/S:
Asymptomatic, pelvic pain and fullness, NO estrogen, associated with Meig’s syndrome, contain fibrous tissue, Rare but occur in meno/post menopausal women
Fibroma (Sex cord stromal)
Thecoma USA:
Hypoechoic soldi mass, unilateral, may contain calcifications and shadowing may be lobular, rare but occurs in meno/postmeno
Thecoma Clinical S/S:
Asymptomatic, PMB, Pelvic pain and fullness, Estrogen producing, Contains only thecal cells

Thecoma (Sex cord stromal)
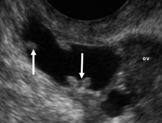
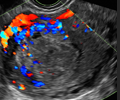
Ovarian Torsion USA
Hypoechoic enlarged unilateral ovary, ovarian mass present, absent Doppler flow in ovary - use power doppler, WHIRLPOOL sign, FF in cul de sac, most common on RIGHT
Ovarian torsion Clinical S/S:
Sudden onset adnexal pain, N/V, fever, common in reproductive women
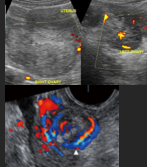
Ovarian torsion
Granulosa Cell Tumor USA:
Unilateral, complex, hetero solid/cystic, multiloculated complex, large >10cm, internal necrosis
Granulosa Cell Tumor S/S:
Malignant potential, estrogen excess, can develop to endometrial carcinoma, rare but occurs in peri/post menopausal women
Granulosa Cell Tumor (Sex cord stromal)
Brenners Tumor USA:
Small, well-defined, hypoechoic solid ovarian mass, calcification, unilateral, related to Meigs syndrome
Brenners Tumor Clinical S/S:
Asymptomatic, pelvic pain and fullness, NO estrogen, rare but occurs in post menopausal women
Brenner’s tumor (Transitional Cell Tumor)
Follicular Cyst USA:
Anechoic, smooth borders, posterior enhancement, uni or bilateral
Follicular Cyst Clinical S/S:
Asymptomatic, regress spontaneously, occurs at any age
Most common adnexal mass:
Follicular cyst

Follicular cyst
Most common adnexal mass in pregancy
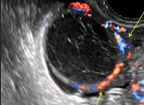
Corpus luteal cyst
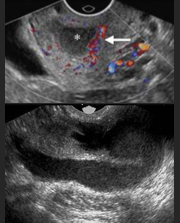
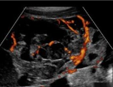
Corpus luteal cyst USA
Anechoic may contain debris, smooth borders, posterior enhancement, unilateral, ring of fire
Corpus luteal cyst Clinical S/S:
Asymptomatic, regress spontaneously, mass secretes progesterone, common in reproductive women
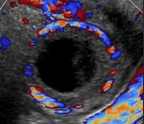
Corpus luteal cyst
Hemorrhagic cyst USA:
Fluid levels “Lacy”, round well defined, posterior enhancement, thin or thick septations, FF in posterior cul-de-sac
Hemorrhagic cyst Clinical S/S:
Pain unilateral, resolves spontaneously, common in reproductive/perimenopausal women
Hemorrhagic cyst
Mucinous/Serous cystadenocarcinoma USA:
Ill-defined, multilocular complex mass, papillary projections, mural nodules, thick septations, increased vascular in septations, ascites
Mucinous/Serous cystadenocarcinoma clinical S/S:
Palpable mass, increased CA-125, unexplained wt loss, pseudomyxoma peritonei (mucin), ascites, pelvic pain, associated w/torsion, prolonged estrogen exposure, rare in peri to postmenopausal women
Most common malignancy of ovaries
Serous cystadenocarcinoma
Mucinous/Serous Cystadenocarcinoma
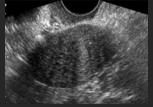
Dysgerminoma USA:
Solid, homogeneous mass w/irregular borders, areas or necrosis, rapid growth, lymph adenopathy, vascularity, usually unilateral
Dysgerminoma clinical S/S:
Asymptomatic, pelvic pain, palpable pelvic mass, elevated AFP, increase LDH, hCG, CA-125, amenorrhea, precocious puberty, rare, occurs in Pre-pub/early reproductive
Dysgerminoma (Germ cell)
Krukenberg Tumor USA:
Large predominantly solid adnexal mass, moth-eaten sign, usually bilateral, ascites
Most common METS from stomach to ovary:
Krukenberg Tumor
Krukenberg Tumor Clinical S/S:
Hx breast Ca, GI Tract Ca, Pelvic lymphadenopathy, rare in peri-post menopausal women

Krukenberg Tumor
Endometroid/Clear Cell Carcinoma USA:
Mimics endometrioma, solid component, heterogeneous, Mullerian duct origin, bilateral
Endometroid/Clear cell Carcinoma Clinical S/S:
Associated w/Lynch Syndrome, Endometriosis, endometrial carcinoma, increases w/thromboembolism, clear cell bilateral

Endometroid/Clear Cell Carcinoma (epithelial)
Most common malignancy of Ovary
Serous Cystadenocarcinoma
Yolk Sac Tumor/Endodermal Sinus Tumor USA:
Variable USA, associated with teratoma, increased vascularity w/echogenic foci
Yolk Sac Tumor Clinical S/S:
Increased AFP, pelvic fullness, poor prognosis - rapid growth, rare but occurs in prepuberty/adolescents
Yolk Sac Tumor/Endodermal Sinus Tumor
Choriocarcinoma (germ cell)
Choriocarcinoma USA:
Unilateral, rapid growing, variable USA, large, aggressive, rare but occurs in prepuberty/reproductive women
Sertoli-Leydig Cell Tumor/Androblastoma USA:
Benign or malignant, can occur in testicles, unilateral
Sertoli-Leydig Cell Tumor Clinical S/S:
Androgen secreting/virilization (hirsutism, deepening voice, amenorrhea, increased testosterone)

Sertoli-Leydig Cell Tumor/Androblastoma (Sex cord tumor)
Choriocarcinoma Clinical S/S:
Increased hCG, occur from trophoblastic cells, post ectpoic, precociuous puberty, Mets to Lungs